
Abstract
Objectives
To investigate how body height and trajectories of height from infancy through childhood and adolescence were associated with spinal pain in pre- and late adolescence.
Methods
This prospective study included 43,765 individuals born into The Danish National Birth Cohort (DNBC) from 1996 to 2003. DNBC-data were linked with health and social data identified from Statistics Denmark registers. Spinal pain was self-reported in both the 11-year- and 18-year follow-up of DNBC and classified according to severity. Body height was measured from birth and onwards and further modelled as distinct developmental height trajectories by using latent growth curve modelling. Associations were estimated by using multinomial logistic regression models.
Results
Taller body height in childhood and adolescence was associated with approximately 20% increased likelihood of spinal pain in pre- and late adolescence among girls compared to their peers in the normal height group. For boys, taller body height was associated with spinal pain by late adolescence only. Spinal pain in pre-adolescence almost doubled the likelihood of spinal pain in late adolescence regardless of body height at age 18. Height trajectories confirmed the relationship for girls with the tall individuals being most likely to have spinal pain in both pre- and late adolescence.
Conclusion
Tall body height during childhood and adolescence predisposes to spinal pain among girls in both pre-and late adolescence, and among boys in late adolescence. Body height is a contributing factor to the pathogenesis of spinal pain in adolescence; however, the mechanisms may be related to growth velocity, but for now uncertain.
Similar content being viewed by others

Introduction
Spinal disorders constitute an enormous global burden with adverse societal and personal consequences [1], and low back and neck pain has been documented as leading causes of disabilities globally [2]. Evidence suggests spinal pain to have its onset already in childhood and the prevalence to reach adult levels around age 18 [3,4,5,6,7]. In addition, pediatric onset of spinal pain has been suggested to predict spinal pain in later life, and thus, spinal pain can be a long-term experience [3]. Etiology of spinal pain may be found in a complex interplay between psychosocial, environmental, and biological components. Psychosocial and environmental factors such as depressive symptoms [8, 9], stress and poor general well-being [10], as well as living in socioeconomically disadvantaged families [11] have been suggested as potential risk factors for the development of spinal pain in young people. However, there is little evidence to suggest that biological and genetical factors in terms of body height and growth during childhood and adolescence are associated with back pain in adolescents [12, 13].
Body height is hardly modifiable and mainly influenced by environmental factors and genetic predispositions [14,15,16,17]. Despite limited possibilities for intervention, body height and growth patterns are important aspects in the understanding of the interplay and impact of risk factors predisposing to spinal pain already in adolescence and identification of particularly vulnerable subgroups may guide personalized prevention.
Therefore, the overall aim of this study was to investigate how body height from birth up to adolescence were associated with spinal pain in pre-adolescence and late adolescence. Specifically, we aimed to first investigate body height at different ages from birth through childhood to adolescence in relation to spinal pain in pre-adolescence (11–12 years of age) and subsequently to spinal pain in late adolescence (18 years of age). Furthermore, we investigated developmental patterns of height and related these distinct height trajectories to spinal pain in 11-12-year-olds and 18-year-olds, respectively.
Methods
Study population
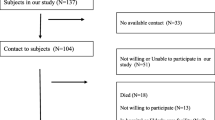
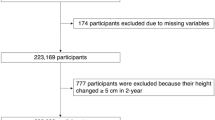
This longitudinal study applied data from The Danish National Birth Cohort (DNBC), nested within the nationwide population of Denmark. In brief, DNBC is a population-based cohort including 98,825 children born between 1996 and 2003, followed from birth and through childhood and young adulthood. DNBC is described in detail elsewhere (www.dnbc.dk) [18]. The overall study population consisted of 43,765 individuals 11–12 years of age that participated in the 11-year follow-up of DNBC (DNBC-11) and who had at least one height measure reported from birth to age 11. Selection mechanisms are depicted in the flow chart in Fig. 1. Since the study included height exposures at different ages as well as spinal pain outcomes in both pre-adolescence and late adolescence, we defined specific analysis samples according to the respective analyses to obtain the highest power for each analysis (see Fig. 1).

Flow chart of the study population and additional analysis samples
DNBC-data was linked to Danish national registers through the unique personal identification number assigned to all persons with a permanent residence in Denmark [19]. All registries applied were available and processed at Statistics Denmark, and all data were pseudonymized. Approval of the study was obtained from the Danish Data Protection Agency through the joint notification of The Faculty of Health and Medical Sciences at The University of Copenhagen (SUND-2017-09) and the DNBC Steering Committee (2017-23).
Height measures
Length at birth was retrieved from the Danish Medical Birth Registry [20]. The remaining height measures at age 1, 7, 11 and 18 were obtained from DNBC data collections. Height data were carefully cleaned for errors before any further data management and height measures within the range of -5 to 5 standard deviations (SD) were accepted [21]. Height at age 1 was mother-reported in the 18-months follow-up of DNBC and based on the registrations made by the general practitioner in ‘The Child’s Book’ in connection with routine preventive health visits scheduled at 5 and 12 months. We exclusively allowed inclusion of measurements reported between 11 and 13 months. Height at age 7, 11 and 18 were accepted if reported within the given year, and were further categorized into three percentile groups, calculated by sex. The group of normal height consisted of the 20th to 80th percentile, low height was defined as < 20th percentile, and the > 80th percentile was defined as tall height.
For latent growth curve modeling (LGCM), we modelled height z-scores to enable comparisons across age and sex. Z-scores were calculated using the Zanthro package in STATA with standardization according to the WHO-reference and included age in months [22].
Spinal pain
DNBC-11 included self-reported information on frequency and intensity of neck pain, mid back pain and low back pain. The questions were adopted from The Young Spine Questionnaire (YSQ) designed and validated to measure neck, mid back and low back pain in 9–11 year-olds [23]. Children were asked to report their pain frequency and intensity ranging from 0 to 6 based on the Faces Pain Scale-Revised (FPS-r)) [23, 24]. For each spinal region we combined pain frequency and intensity and trichotomized into no pain, moderate pain, or severe pain (Supplementary File 1). For all spinal regions, severe pain was defined as pain of 4 or more on FPS-r and occurring at least ‘once in a while’, and no pain was defined as pain up to 2 on FPS-r occurring ‘once in a while’ or ‘once or twice’. Moderate pain covered the remaining combinations. Subsequently, the main outcome of interest Spinal pain was constructed as a composite measure including all spinal regions categorized according to severity. The applied definition is directly adapted from our previous work and documented in detail elsewhere [11]. Information on spinal pain at age 18 was obtained from DNBC-18, which included a similar frequency scale as DNBC-11, however, the intensity scale ranged from 0 to 10 according to the Numeric Pain Rating Scale (NRS). Since no valid method exists to transfer NRS to FPS-r for adolescents, we based the definition of spinal pain in DNBC-18 on a study on elderly people in nursing homes [25], supported by several sensitivity analyses testing the different combinations of intensity and frequency of spinal pain. The applied measures of spinal pain in pre- and late adolescence are illustrated in Supplementary File 1.
Covariates
Potential confounders were selected a priori, and identified using the methods of causal diagrams (Depicted in Supplementary File 2) [26]. Information on sex was derived from DNBC-11. Parity (nulliparous/parous) and gestational age (term/preterm) were obtained from The Danish Medical Birth Registry [20]. Educational level was obtained from The Danish Population’s Education Register [19], and operationalized as the highest ongoing or completed education of the parents attained at childbirth and was categorized into three groups according to the International Standard Classification of Education (ISCED) 2011: low (ISCED 0–2), medium (ISCED 3–4) and high (ISCED 5–8) [27]. Equivalized household income at the year before childbirth was based on disposable household income extracted from The Income Statistics Register [28]. We divided disposable household income by an equivalence factor corresponding to the modified OECD scale [29]. Equivalized household income was further categorized into quartiles by year relative to all mothers giving birth in the given year. Finally, we created an indicator of pubertal maturation (i.e., having reached pubertal growth spurt) (yes/no) at time of completion of DNBC-11. A Tanner stage of 2 or more for girls and Genital stage of 4 or more for boys indicated that the pubertal growth spurt was reached [30].
Statistical analyses
Statistical analyses were performed in STATA V. 16.1. To estimate all associations between body height and spinal pain, we used multinomial logistic regression models to calculate crude and adjusted relative risk ratios (RRR) and corresponding 95% confidence intervals (CI) (see Supplementary File 3 for interpretation). Children with no spinal pain were considered the reference outcome in all analyses, and dependency between siblings in the sample was taken into account by applying a robust standard error estimator [31]. We tested and identified sex-differences between sex and height at the different ages by evaluating first-order interactions using Wald-tests, hence, included the interaction between sex and height in each model and further adjusted for the main effects of the identified potential confounders.
In sensitivity analyses, we applied height as a continuous variable in 5 cm intervals after first testing for linearity. Secondly, we performed analyses using neck, mid, and low back pain as separate outcomes. Thirdly, in a sub-analysis of height at age 11 and spinal pain in pre-adolescence, we accounted for pubertal maturation. Lastly, to evaluate the extent to which the results may have been affected by selection forces, we conducted a loss-to-follow-up analysis and subsequently applied inverse probability weighting (IPW) to account for potential selection bias as to handle potential bias arising from exclusion of missing data [32, 33]. Predictor variables in IPW corresponded those included in the loss-to-follow-up analysis.
Identification and analysis of height trajectories
LGCM was used to estimate developmental height patterns from childbirth through childhood to adolescence and their relation to spinal pain in adolescence. The analysis was conducted as a two-step process, first by estimating height trajectories with height included as z-scores as a function of age [34]. A priori, we had decided to look at the different height trajectories separately for boys and girls, however, we observed a striking similarity between the two trajectory models, and decided, also supported by a likelihood ratio test, that the modelling of the trajectories should not be separated by sex. The height trajectories were subsequently included as an interaction term between height and sex as described above. Secondly, multinomial logistic regression models were used to calculate associations with spinal pain in pre- and late adolescence [34]. The association was further analyzed separately for each spinal region in a sensitivity analysis. Supplementary File 4 includes detailed description of LGCM.
Results
The tallest individuals differed from their shorter peers by being more likely to be born to term and from families of higher socioeconomic status (Table 1). On average, boys were of taller height from birth to age 7 (Supplementary File 5). At 11 years, mean height of girls and boys approached equal levels. However, from age 11 to age 18 boys grew more and reached significant taller height than girls. Prevalence of severe spinal pain in pre-adolescence was 12% and 21% in late adolescence with the highest prevelance among girls (Supplementary File 6).
Loss-to-follow-up analyses revealed that the study participants were more often girls, from families of higher socioeconomic status, had non-smoking mothers during pregnancy, and from urban areas compared to those lost to follow-up. This was slightly more significant among those with further follow-up in late adolescence (Supplementary File 7). Nonetheless, applying IPW to account for selection both into the cohort and from attrition had no essential impact on the estimates in any of the analyses included in this study (data not shown).
Association between body height and adolescence spinal pain
Results from adjusted regression analyses showed that among girls, tall body height during childhood and adolescence was directly associated with moderate and severe spinal pain in pre-adolescence as well as late adolescence (Table 2). The tallest group at age 11 had an increased likelihood of severe spinal pain in pre-adolescence of 26% (RRR: 1.26, 95% CI: 1.11–1.43) relative to no pain and compared to their peers in the normal height group, whereas those in lowest height group were less likely to have spinal pain. The same pattern was observed for height at age 7 and spinal pain in pre-adolescence, and for height at age 11 in relation to spinal pain in late adolescence (Table 2). This dose-response trend was confirmed in sensitivity analyses analyzing height as a continuous variable (Supplementary File 8). Among boys, no definite associations were observed in pre-adolescence. Nevertheless, for boys we observed both tall height at age 11 (RRR: 1.44, 95% CI: 1.19–1.75) and at age 18 (RRR: 1.24, 95% CI: 1.06–1.46) to be associated with spinal pain in late adolescence (Table 2), as did we observe a tendency of a dose-response effect for boys. Additional adjustment for pubertal maturation had no effect on the estimates for boys; however, it weakened the estimates for girls (Supplementary File 9). The prevailing spinal pain regions were the mid and low back for girls, whereas no consistent pattern was observed for boys (data not shown).
Additionally, we observed that having reported spinal pain already in pre-adolescence seemed to approximately double (and for some even more) the likelihood of severe spinal pain in late adolescence independently of height at age 18 for both sexes (Supplementary File 10). For boys, the likelihood of severe spinal pain in late adolescence relative to no pain increased stepwise with increasing height at age 18 regardless of spinal pain status in pre-adolescence, which was not the case for girls. The findings were supported by Wald-tests.
Association between distinct height trajectories and spinal pain in adolescence
We identified five distinct height trajectories from childbirth to age 11 (Fig. 2a), as well as from childbirth to age 18 (Fig. 2b). We found girls with a height trajectory characterized by height above the mean to be 27% (RRR: 1.27, 95% CI: 1.14–1.41) more likely to have severe spinal pain in pre-adolescence and 23% (RRR: 1.23, 95% CI: 1.11–1.37) in late adolescence compared with their peers in the normal height trajectory (Table 3). Mid and low back pain were the prevailing pain regions (data not shown). Analyses of height trajectories showed no significant associations with spinal pain for boys, and we observed no tendencies of certain time periods of excessive growth that impacted on spinal pain.

Latent growth curve modelling was used to derive distinct body height trajectories from 0 to 11 years (A) and from 0 to 18 years (B) of individuals in The Danish National Birth Cohort. The figures display the class-specific estimated average height (z-scores) for age with 95% confidence intervals. The normal height groups in both figures were characterized as having a birth length above the mean, which was expected since z-scores were made according to the WHO-reference and Scandinavian newborns are generally longer at birth
Discussion
To our knowledge, this is the first large-scale birth cohort study including several prospectively collected height measures during childhood and adolescence as well as spinal pain in both pre-and late adolescence. We demonstrated that being tall during childhood and adolescence predisposed to spinal pain in pre-adolescence and late adolescence among girls, and tall height at age 11 and 18 predisposed to severe spinal pain among boys in late adolescence. Further, the presence of spinal pain in pre-adolescence predisposed to spinal pain in late adolescence regardless of height at age 18. Height trajectories were confirmative of tall girls being more likely to have spinal pain.
The existing literature is contradictive according to the association between height and musculoskeletal pain including back pain [35]. Our findings illustrated tall body height to be associated with spinal pain in adolescence with onset in pre-adolescence for girls and later for boys. Hebert et al. found that pubertal development and increase in height were potentially risk factors for spinal pain in 10-12-year-olds with no indication of interaction with sex [36]. In line with our findings in late adolescence, Hershkovich et al. investigated boys and girls separately and found height to be positively associated with low back pain among 17-year-old (i.e., late adolescence) girls and boys [13]. During adolescence pubertal maturation (i.e., the pubertal growth spurt and changes in hormone levels) occurs earlier in girls than in boys [7, 15, 30], and affects very differently between sexes and within individuals [15, 37]. In addition, changes in hormone levels are demonstrated to impact on pain perception [37,38,39]. Pubertal maturation has previously been related to back pain in adolescents [36, 40], and therefore the earlier onset of spinal pain in girls could potentially correspond the time of puberty [4], since the majority of individuals in DNBC-11 were 11 years of age. In contrast to our expectations, adjusting for pubertal maturation had no impact for boys.
Another mechanism that may explain the findings is related to growth velocity of the spine, which is around the time of pre-adolescence accelerating faster than the lower extremities. This leads to increasing height and change in body composition, which have previously been suggested to impact on back pain in adolescence [7, 41]. The back muscle strengths and the connective tissue do not develop as fast as the spine grows during adolescence, and these are important for the maintenance of the strengths of the body stature [12, 42]. Growth spurt initiates around age 10–12 in girls, whereas boys grow significant more than girls between age 11 and 18 and development of spinal pain due to height may thus be later for boys than girls [12], as also indicated in our study.
Taller stature has been associated with higher socioeconomic status and better health [43,44,45], whereas spinal pain seems associated with lower socioeconomic status [11]. Since taller stature was still related to spinal pain in our study also subsequent to socioeconomic adjustment, it indicated that the identified association between tall stature and spinal pain is not likely to be explained by social confounding.
Strengths and limitations
The prospective nature of this large-scale study with access to the unique database of DNBC facilitated examination of an array of height factors from childbirth through childhood and adolescence as well as spinal pain in pre- and late adolescence. The design ensured temporality between distinct height measures and spinal pain in pre- and late adolescence. Additionally, LGCM allowed modeling of distinct height trajectories with unstructured covariance matrix i.e., height measures did not need to be reported neither at the same time or with the same interval for each individual and only one height measure per individual was required, which strengthened statistical power [34].
Some limitations to this work need to be addressed. Some of the height measures in the DNBC were either maternally reported or reported by the individual itself, which is prone to misclassification in relation to timing and accuracy. We believe, however, that misclassification of height was a minor issue since it was not assumed to be related to the reporting of spinal pain [46]. In addition, information on birth length was retrieved from The Danish Medical Birth Register, and even though the register in general holds high validity, the practical measurement of the newborn may be imprecise.
We were able to adjust for several confounders, however, the complex etiology of spinal pain including social, psychological, and biological risk factors did challenge comprehensive inclusion of confounders, and it is possible that unmeasured variables may have confounded the observed associations. For example, BMI can impact timing of pubertal maturation i.e., early overweight might result in the earlier growth spurt [47] and at the same time BMI in itself can affect the development of spinal pain [13, 48]. We did not adjust for BMI due to risk of overadjustment. Adjustment for BMI was found to have limited influence in another study [15].
Finally, as with all longitudinal birth cohort studies with long follow-up, selection into the cohort and from attrition are inevitable, and DNBC is not an exception. Compared to the source population, the participants constituted a selected sample being healthier and of higher socioeconomic position [49]. Nevertheless, methodological studies have documented the impact on effect estimates to be negligible [49, 50], and further accounting for selection by using inverse probability weighting revealed no essential changes to the findings [32, 33]. Therefore, we do not consider selection bias a major issue for the findings of this study, and thus the study population to be overall representative for individuals born in Denmark.
Conclusion
Tall body height during childhood and adolescence is associated with spinal pain in girls in both pre- and late adolescence, and for boys by late adolescence. In addition, having had spinal pain already in pre-adolescence is remarkably increasing the likelihood of spinal pain in late adolescence regardless of height. Thus, tall height is a contributing factor to the pathogenesis of spinal pain in adolescence, with timing and mechanisms potentially being related to growth velocity, but for now this remains uncertain. Despite body height being a hardly modifiable factor, the findings from this study may from a public health perspective be important for the wider understanding of the complex interplay between risk factors of spinal pain in adolescence and further to guide the identification of vulnerable subgroups that may benefit from targeted prevention.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to the data being stored and processed in the research machines of Statistics Denmark and only available for licensed institutions but are available from the corresponding author on reasonable request.
Abbreviations
- DNBC:
-
The Danish National Birth Cohort
- DNBC-11:
-
The 11-year follow-up of The Danish National Birth Cohort
- DNBC-18:
-
The 11-year follow-up of The Danish National Birth Cohort
- FPS-r:
-
The Faces Pain Scale - revised
- IPW:
-
Inverse probability weighting
- ISCED:
-
International Standard Classification of Education
- LGCM:
-
Latent Growth Curve Modeling
- NRS:
-
The Numeric Pain Rating Scale
- RRR:
-
Relative risk ratio
- SD:
-
Standard deviation
- Spinal pain:
-
Neck pain, mid back pain and/or low back pain
- YSQ:
-
The Young Spine Questionnaire
- 95% CI:
-
95% confidence intervals
References
Hurwitz EL, Randhawa K, Yu H, Côté P, Haldeman S. The global spine care initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J. 2018;27(6):796–801.
Kassebaum NA, Barber M, Bjertness RM, Hailu E, Knudsen A, Norheim AK, Skogen OF, Savic JC, Skirbekk M, Steiner V, Stovner TJ, Søreide LJ, Vollset K, Weiderpass SEE. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603–58.
Dunn KM, Hestbaek L, Cassidy JD. Low back pain across the life course. Best Pract Res Clin Rheumatol. 2013;27(5):591–600.
Jeffries LJ, Milanese SF, Grimmer-Somers KA. Epidemiology of adolescent spinal pain: a systematic overview of the research literature. Spine. 2007;32(23):2630–7.
Calvo-Munoz I, Gomez-Conesa A, Sanchez-Meca J. Prevalence of low back pain in children and adolescents: a meta-analysis. BMC Pediatr. 2013;13: 14.
MacDonald J, Stuart E, Rodenberg R. Musculoskeletal low back pain in school-aged children: a review. JAMA Pediatr. 2017;171(3):280–7.
Lardon A, Leboeuf-Yde C, Le Scanff C, Wedderkopp N. Is puberty a risk factor for back pain in the young? A systematic critical literature review. Chiropr Man Ther. 2014;22(1):27.
Diepenmaat AC, van der Wal MF, de Vet HC, Hirasing RA. Neck/shoulder, low back, and arm pain in relation to computer use, physical activity, stress, and depression among Dutch adolescents. Pediatrics. 2006;117(2):412–6.
Myrtveit SM, Sivertsen B, Skogen JC, Frostholm L, Stormark KM, Hysing M. Adolescent neck and shoulder pain–the association with depression, physical activity, screen-based activities, and use of health care services. J Adolesc Health. 2014;55(3):366–72.
Stallknecht SE, Strandberg-Larsen K, Hestbaek L, Nybo Andersen A. Spinal pain and co-occurrence with stress and general well-being among young adolescents: a study within the Danish National Birth Cohort. Eur J Pediatrics. 2017;176(6):807–14.
Joergensen AC, Hestbaek L, Andersen PK, Nybo Andersen AM. Epidemiology of spinal pain in children: a study within the Danish National Birth Cohort. Eur J Pediatrics. 2019;178(5):695–706. https://doi.org/10.1007/s00431-019-03326-7.
Jones GT, Macfarlane GJ. Epidemiology of low back pain in children and adolescents. Arch Dis Child. 2005;90(3):312–6.
Hershkovich O, Friedlander A, Gordon B, Arzi H, Derazne E, Tzur D, et al. Associations of body mass index and body height with low back pain in 829,791 adolescents. Am J Epidemiol. 2013;178(4):603–9.
Jelenkovic A, Sund R, Hur YM, Yokoyama Y, Hjelmborg JB, Möller S, et al. Genetic and environmental influences on height from infancy to early adulthood: an individual-based pooled analysis of 45 twin cohorts. Sci Rep. 2016;6(1):1–13.
Heuch I, Heuch I, Hagen K, Zwart JA. Association between body height and chronic low back pain: a follow-up in the Nord-Trøndelag Health Study. BMJ Open. 2015;5(6):e006983-e.
Xu L, Nicholson P, Wang Q, Alén M, Cheng S. Bone and muscle development during puberty in girls: a seven-year longitudinal study. J Bone Miner Res. 2009;24(10):1693–8.
Gualdi-Russo E, Toselli S, Masotti S, Marzouk D, Sundquist K, Sundquist J. Health, growth and psychosocial adaptation of immigrant children. Eur J Pub Health. 2014;24 Suppl 1(suppl 1):16–25.
Olsen J, Meder I. Better health for mother and child - the Danish National Birth Cohort (DNBC), its structure, history and aims. Nor Epidemiol. 2014;24(1–2):37–8.
Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7 Suppl):91–4.
Bliddal M, Broe A, Pottegard A, Olsen J, Langhoff-Roos J. The Danish medical birth register. Eur J Epidemiol. 2018;33(1):27–36.
Freedman DS, Lawman HG, Skinner AC, McGuire LC, Allison DB, Ogden CL. Validity of the WHO cutoffs for biologically implausible values of weight, height, and BMI in children and adolescents in NHANES from 1999 through 2012. Am J Clin Nutr. 2015;102(5):1000–6.
Vidmar SI, Cole TJ, Pan H. Standardizing anthropometric measures in children and adolescents with functions for egen: update. Stata J. 2013;13(2):366–78.
Lauridsen HH, Hestbaek L. Development of the young spine questionnaire. BMC Musculoskelet Disord. 2013;14: 185.
Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B. The faces pain scale-revised: toward a common metric in pediatric pain measurement. Pain. 2001;93(2):173–83.
Jones KR, Vojir CP, Hutt E, Fink R. Determining mild, moderate, and severe pain equivalency across pain-intensity tools in nursing home residents. J Rehabil Res Dev. 2007;44(2):305–14.
Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology. 1999;10(1):37–48.
ISCED. International Standard Classification of Education ISCED 2011. Montreal: UNESCO Institute for Statistics; 2012.
Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–5.
OECD. OECD Project on Income Distribution and Poverty. What are the equivalence scales? : Organization for Economic Cooperation and Development. Available from: http://www.oecd.org/eco/growth/OECD-Note-EquivalenceScales.pdf. Cited 2018 19 September.
Aksglaede L, Olsen LW, Sørensen TIA, Juul A. Forty years trends in timing of pubertal growth spurt in 157,000 Danish school children. PLoS One. 2008;3(7):e2728-e.
Vach W. Regression models as a tool in medical statistics. Boca Raton: Chapman and Hall/CRC; 2013.
Seaman SR, White IR. Review of inverse probability weighting for dealing with missing data. Stat Methods Med Res. 2013;22(3):278–95.
Molenberghs G, Fitzmaurice G, Kenward MG, Tsiatis A, Verbeke G. Handbook of Missing Data Methodology. 1st edition. Chapman and Hall/CRC; 2014. https://doi.org/10.1201/b17622.
Tu YK, Tilling K, Sterne JAC, Gilthorpe MS. A critical evaluation of statistical approaches to examining the role of growth trajectories in the developmental origins of health and disease. Int J Epidemiol. 2013;42(5):1327–39.
Huguet A, Tougas ME, Hayden J, McGrath PJ, Stinson JN, Chambers CT. Systematic review with meta-analysis of childhood and adolescent risk and prognostic factors for musculoskeletal pain. Pain. 2016;157(12):2640–56.
Hebert JJ, Leboeuf-Yde C, Franz C, Lardon A, Hestbæk L, Manson N, et al. Pubertal development and growth are prospectively associated with spinal pain in young people (CHAMPS study-DK). Eur Spine J. 2019;28(7):1565–71.
Rhee H. Relationships between physical symptoms and pubertal development. J Pediatr Health care. 2005;19(2):95–103.
Wedderkopp N, Andersen LB, Froberg K, Leboeuf-Yde C. Back pain reporting in young girls appears to be puberty-related. BMC Musculoskelet Disord. 2005;6(1): 52.
Sundblad GMB, Saartok T, Engstrom LM. Prevalence and co-occurrence of self-rated pain and perceived health in school-children: age and gender differences. Eur J Pain. 2007;11(2):171–80.
Janssens KA, Rosmalen JG, Ormel J, Verhulst FC, Hunfeld JA, Mancl LA, et al. Pubertal status predicts back pain, overtiredness, and dizziness in American and Dutch adolescents. Pediatrics. 2011;128(3):553–9.
Perry M, Straker L, O’Sullivan P, Smith A, Hands B. Fitness, motor competence, and body composition are weakly associated with adolescent back pain. J Orthop Sports Phys Ther. 2009;39(6):439–49.
Takahashi I, Kikuchi SI, Sato K, Iwabuchi M. Effects of the mechanical load on forward bending motion of the trunk: comparison between patients with motion-induced intermittent low back pain and healthy subjects. Spine (Phila Pa 1976). 2007;32(2):E73–8.
Tyrrell J, Jones SE, Beaumont R, Astley CM, Lovell R, Yaghootkar H, et al. Height, body mass index, and socioeconomic status: mendelian randomisation study in UK Biobank. BMJ. 2016;352:i582-i.
Whitley E, Martin RM, Davey Smith G, Holly JMP, Gunnell D. The association of childhood height, leg length and other measures of skeletal growth with adult cardiovascular disease: the Boyd-Orr cohort. J Epidemiol Community Health. 2012;66(1):18–23.
Smith GD, Hart C, Upton M, Hole D, Gillis C, Watt G, et al. Height and risk of death among men and women: aetiological implications of associations with cardiorespiratory disease and cancer mortality. J Epidemiol Community Health. 2000;54(2):97–103.
Lash T, VanderWeele T, Rothman K. Measurement and measurement error. In: Zinner S, editor. Modern epidemiology. 4th ed. Mexico: Wolters Kluwer; 2021. p. 287–314.
Aksglaede L, Juul A, Olsen LW, Sørensen TIA. Age at puberty and the emerging obesity epidemic. PLoS One. 2009;4(12):e8450-e.
Heuch I, Heuch I, Hagen K, Zwart J-A. Body mass index as a risk factor for developing chronic low back pain: a follow-up in the Nord-Trøndelag Health Study. Spine. 2013;38(2):133–9.
Jacobsen T, Nohr E, Frydenberg M. Selection by socioeconomic factors into the Danish National Birth Cohort. Eur J Epidemiol. 2010;25(5):349–55.
Pizzi C, De Stavola B, Merletti F, Bellocco R, dos Santos Silva I, Pearce N, et al. Sample selection and validity of exposure-disease association estimates in cohort studies. J Epidemiol Commun Health. 2011;65(5):407–11.
Acknowledgements
The study was supported by The Danish Council for Independent Research (DFF-7016-00344) and the EUCAN-connect, a federated FAIR platform enabling large-scale analysis of high-value cohort data connecting Europe and Canada in personalized health project (European Commission, Grant Agreement No. 824989).
The Danish National Birth Cohort was established with a significant grant from the Danish National Research Foundation. Additional support was obtained from the Danish Regional Committees, the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Health Foundation and other minor grants. The DNBC Biobank has been supported by the Novo Nordisk Foundation and the Lundbeck Foundation. Follow-up of mothers and children have been supported by the Danish Medical Research Council (SSVF 0646, 271-08-0839/06-066023, O602-01042B, 0602-02738B), the Lundbeck Foundation (195/04, R100-A9193), The Innovation Fund Denmark 0603-00294B (09-067124), the Nordea Foundation (02-2013-2014), Aarhus Ideas (AU R9-A959-13-S804), University of Copenhagen Strategic Grant (IFSV 2012), and the Danish Council for Independent Research (DFF – 4183 − 00594 and DFF − 4183 − 00152).
We also like to thank Professor Cecilia Ramlau-Hansen and Nis Brix from Aarhus University for a fruitful discussion on the potential impact of puberty on spinal pain.
Funding
Open access funding provided by Royal Library, Copenhagen University Library The study was supported by The Danish Council for Independent Research (DFF-7016-00344) and the EUCAN-connect, a federated FAIR platform enabling large-scale analysis of high-value cohort data connecting Europe and Canada in personalized health project (European Commission, Grant Agreement No 824989).
Author information
Authors and Affiliations
Contributions
PhD Falch-Joergensen conceptualized and designed the study, contributed to methods development including operationalization of variables, carried out data management, analyses and interpretation of results, and drafted the manuscript. Prof Nybo Andersen designed the data collection instruments, conceptualized, and designed the study, and contributed to methods development including operationalization of variables, interpretation of results and critical revision of the manuscript.Prof Kragh Andersen and Prof Budtz-Jorgensen supervised the statistical methods and analyses and contributed to method development, interpretation of results and critical revision of the manuscript. Prof Hestbaek conceptualized and designed the study, contributed to methods development, interpretation of results and critical revision of the manuscript. PhD Strandberg-Larsen designed the data collection instruments, contributed to methods development, interpretation of results and critical revision of the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of this article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The procedures of this study are performed in accordance with the Declarations of Helsinki. Approval of the study was obtained from the Danish Data Protection Agency through the joint notification of The Faculty of Health and Medical Sciences at The University of Copenhagen (SUND-2017-09) and the DNBC Steering Committee (2017-23).
Written informed consent was collected from all study participants (maternally) before study participants were enrolled in the first data collection of The Danish National Birth Cohort, and again from study participants when they turned 18 years.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary File 1.
The combination of pain frequency and intensity of the overall measure of spinal pain from DNBC-11 and DNBC-18.
Additional file 2: Supplementary File 2.
Causal diagram of the assumed relationship between body height and spinal pain in adolescence.
Additional file 3:
Supplementary File 3. Interpretation of relative risk ratio in multinomial logistic regression models.
Additional file 4: Supplementary File 4.
Supplementary information on the method of latent growth curve modeling.
Additional file 5: Supplementary File 5
. Height characteristics of girls and boys at birth, age 1, 7, 11, and 18 (The Danish National Birth Cohort, 1996-2003).
Additional file 6: Supplementary File 6.
Prevalence of spinal pain in pre-adolescence and late adolescence.
Additional file 7: Supplementary File 7.
Characteristics of the 90,978 participants invited to participate in DNBC-11 and included in the baseline cohort according to follow-up status at age 11 and follow-up status at age 18.
Additional file 8: Supplementary File 8.
Adjusted relative risk ratio(RRR) of spinal pain at age 11-12 according to body height at age 7 and 11, respectively, as continuous variables in 5 cm intervals (The Danish National Birth Cohort, born 1996-2003).
Additional file 9: Supplementary File 9.
Adjusted relative risk ratio(RRR) of spinal pain at age 11-12 according to body height at age 11, additionally adjusted for puberty maturation at age 11 (The Danish National Birth Cohort, born 1996-2003,N = 30,683).
Additional file 10: Supplementary File 10.
Adjusted relative risk ratio(RRR) of spinal pain at age 18 according to body height at age 18 taking spinal pain status in pre-adolescents into account (The Danish National Birth Cohort, born 1996-2003, N = 25,868).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Falch-Joergensen, A.C., Andersen, P.K., Budtz-Jorgensen, E. et al. Body height and spinal pain in adolescence: a cohort study from the Danish National Birth Cohort. BMC Musculoskelet Disord 24, 958 (2023). https://doi.org/10.1186/s12891-023-07077-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-07077-3