
Abstract
Background
Concomitant lateral meniscal (LM) injuries are common in acute anterior cruciate ligament (ACL) ruptures. However, the effect of addressing these injuries with various treatment methods during primary ACL reconstruction (ACLR) on patient-reported outcomes (PROs) is unknown. Therefore, the purpose of this study was to compare postoperative Knee injury and Osteoarthritis Outcome Score (KOOS) at 2-, 5-, and 10-years after isolated primary ACLR to primary ACLR with various treatment methods to address concomitant LM injury.
Methods
This study was based on data from the Swedish National Knee Ligament Registry. Patients ≥ 15 years with data on postoperative KOOS who underwent primary ACLR between the years 2005 and 2018 were included in this study. The study population was divided into five groups: 1) Isolated ACLR, 2) ACLR + LM repair, 3) ACLR + LM resection, 4) ACLR + LM injury left in situ, and 5) ACLR + LM repair + LM resection. Patients with concomitant medial meniscal or other surgically treated ligament injuries were excluded.
Results
Of 31,819 included patients, 24% had LM injury. After post hoc comparisons, significantly lower scores were found for the KOOS Symptoms subscale in ACLR + LM repair group compared to isolated ACLR (76.0 vs 78.3, p = 0.0097) and ACLR + LM injury left in situ groups (76.0 vs 78.3, p = 0.041) at 2-year follow-up. However, at 10-year follow-up, no differences were found between ACLR + LM repair and isolated ACLR, but ACLR + LM resection resulted in significantly lower KOOS Symptoms scores compared to isolated ACLR (80.4 vs 82.3, p = 0.041).
Conclusion
The results of this study suggest that LM injury during ACLR is associated with lower KOOS scores, particularly in the Symptoms subscale, at short- and long-term follow-up. However, this finding falls below minimal clinical important difference and therefore may not be clinically relevant.
Level of Evidence
III.
Similar content being viewed by others


Introduction
Concomitant, traumatic lateral meniscal (LM) tears are frequently found in patients with acute anterior cruciate ligament (ACL) injuries [1, 2], and have been associated with increased knee instability, risk of cartilaginous defects, and later development of osteoarthritis [1, 3,4,5,6,7]. Meniscal tears in the setting of ACL reconstruction (ACLR) can be treated operatively with repair or partial meniscectomy or nonoperatively depending on patients’ intended future knee function and the type of the tear [8]. Studies have reported decreased long term risk of osteoarthritis development as well as increased activity levels and quality of life scores when patients are treated with meniscal repair instead of partial meniscal resection [1, 9,10,11,12,13,14]. However, as meniscal repair has been associated with more extensive postoperative rehabilitation [15] and higher revision risk than partial meniscectomy [13, 16], partial meniscal resection or non-operative treatment may be necessary in irreparable meniscal injuries or in patients wishing for faster return to sport [3, 17].
Research has variable results when comparing short-term subjective knee outcomes in patients undergoing medial or LM repair versus partial meniscal resection in the setting of ACLR [18,19,20]. At 6 months to 1 year postoperatively, patients undergoing concomitant meniscal resection with ACLR have reported comparable subjective knee function to isolated ACLR [18]. Yet, patients undergoing meniscal repair with ACLR reported slightly worse subjective knee function in the same postoperative time periods [18]. However, at 2-year follow-up, studies report that clinical outcomes of concomitant meniscal repair with ACLR are more comparable to isolated ACLR than are outcomes of ACLR with meniscal resection [19, 20]. It is unclear what effect the treatment of meniscal pathology, particularly LM injury, in the setting of ACLR has on mid- to long-term patient-reported outcomes (PROs) of subjective knee function. Previous studies have reported that concomitant LM injury in the setting of ACLR places a patient at higher risk of persistent knee laxity and thus, higher risk of subsequent injuries [21, 22]. However, subjective knee function outcomes following ACLR with concomitant LM treatment are less studied. Thus, an increased understanding of the outcomes of several treatment methods of LM injury in the setting of primary ACLR would improve preoperative planning, postoperative outcomes, and patient education. As such, the aim of this study was to compare the effect of primary isolated ACLR versus primary ACLR with concomitant LM injury (addressed with repair, resection, a combination of repair and resection, or left in situ) on the Knee injury and Osteoarthritis Outcome Score (KOOS) at 2-, 5-, and 10-years postoperatively.
Methods
This registry cohort study was performed in accordance with the Declaration of Helsinki, and approved by the Regional Ethical Board in Stockholm, Sweden (2011/337–31/3), and the Swedish Ethical Review Authority (2022–00913-01). Strengthening the Reporting of Observational Studies in Epidemiology guidelines were used to present this study [23].
This observational cohort study included data obtained from the SNKLR, in which 90% of all ACLR performed annually in Sweden are reported. The SNKLR is a national database that was established in January 2005 and uses a web-based protocol consisting of two parts: a surgeon reported section and a patient reported section [24]. While demographical (sex, age, date of injury, activity at time of injury) and surgical data (surgery type, graft type, concomitant injuries, previous surgery) are reported by the surgeon, patients are asked to fill out the web-based questionnaires regarding to knee function (KOOS, EQ-5D) preoperatively and at 1-, 2-,5 and 10-year follow-ups. Revision surgeries and reoperations for other reasons are registered separately and subsequently correlated with primary ACL surgeries. Furthermore, the participation in the registry is optional and patients are given option to request exclusion if research participation would not be desired. More detailed description of the registry can be found in previous literature [25].
Study population and data collection
Patients aged ≥ 15 years who underwent primary ACLR between 2005 and 2018 and completed postoperative KOOS questionnaires were included in this study. Exclusion criteria were any prior knee surgery, concomitant fracture, concomitant medial meniscal injury, concomitant posterior cruciate ligament injury, or neurovascular injury. Also, patients undergoing double bundle ACLR and patients receiving surgical treatment for concomitant collateral ligament injury were excluded.
The study population was divided into five different groups to determine the effect of different treatments of LM injury in the setting of ACL reconstruction: 1) Isolated ACLR (patients undergoing isolated ACLR without concomitant LM injury or procedure), 2) ACLR + LM repair (patients undergoing ACLR with concomitant LM repair), 3) ACLR + LM resection (patients undergoing ACLR with concomitant LM resection), 4) ACLR + LM injury left in situ (patients undergoing ACLR with nonoperatively treated concomitant LM injury), and 5) ACLR + LM repair + LM resection (patients undergoing ACLR with concomitant LM repair + LM resection).
Patient data (sex, age, body mass index [BMI]), injury (activity at time of injury, concomitant injury) and surgical characteristics (graft type, time from injury to surgery) were extracted from the registry. The activity at the time of injury was divided into six groups: 1) pivoting sport (American football, rugby, basketball, dancing, floorball, gymnastics, handball, ice hockey/bandy, martial arts, racket sports, soccer, volleyball, wrestling); 2) non-pivoting sport (cross-country skiing, cycling, horseback riding, motocross/endure, skateboarding, snowboarding, and surfing/wakeboarding); 3) alpine/skiing; 4) other physical activity (other recreational sport, exercise, trampoline); 5) traffic related; and 6) other (other outdoor activity and work).
Outcome measures
The main outcome of interest for this study was the patient-reported postoperative KOOS at 2-, 5-, and 10-years after the primary ACLR. The KOOS consists of 5 subscales (Pain, Other Symptoms, Function in Sport and Recreation [Sport/Rec], Knee-Related Quality of Life [QoL], and Activities of Daily Living [ADL], including questions related to knee function. Patients are asked whether they have any pain, other symptoms including restricted range of motion or mechanical symptoms, difficulties with performing physical activities and activities of daily living or whether they have needed to make any life changes due to their current knee status. All the questions are ranged from 0 to 4 on 5-point Likert Scale, and each subscale is scaled from 0 to 100, where the latter indicates the best outcome [26]. Even though the KOOS was originally created to assess patients with knee osteoarthritis, it has also been later used in other orthopaedic knee conditions, including ACLR, to assess outcomes following a specific treatment approach [26, 27].
Statistical analyses
The SAS System for Windows software (version 9.4, SAS Institute, North Carolina, USA) was used to perform the statistical analyses. Count (n) and proportion (%) were used to present categorical variables, while mean with standard deviation (SD) and median with minimum and maximum were used to present continuous and ordinal variable, respectively. For comparisons between groups, including post-hoc analysis, the Kruskal–Wallis test was used for continuous variables, while for pairwise comparisons between groups either the Fisher’s non-parametric permutation test or the Mann–Whitney U-test was used for continuous variables due to non-parametric data. Logistic regression analysis was used for adjusting for the concomitant cartilaginous injuries, considering their previously reported influence on postoperative outcomes [28]. All significance tests were conducted at the 5% significance level.
Results
Baseline characteristics
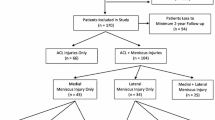
Table 1 presents baseline characteristics. The majority of patients in the study underwent isolated ACLR (24,144). Of the patients with concomitant LM injury, more patients underwent ACLR + LM resection (n = 5,152) compared to ACLR + LM repair (n = 1,099) or ACLR + LM injury left in situ (n = 1,342) (Fig. 1). Lateral meniscal injuries were treated with combined treatment (ACLR + LM repair + LM resection) in the smallest population of patients (n = 82).

Flow Chart on Patient Enrollment
ACLR = anterior cruciate ligament reconstruction; LM = lateral meniscus
Postoperative KOOS by Lateral Meniscal Status 2 years after ACLR
Table 2 shows KOOS results at 2-year follow-up across LM treatment methods. The overall 2-year follow-up data was available for 29,378 patients (92.3%). No significant differences were found between isolated ACLR or the four LM treatment methods for four of five (4/5) KOOS subscales: Sports/Rec, Pain, ADL, and QoL. Significant difference was seen for the KOOS Symptoms subscale (p = 0.0067). When post hoc comparisons were performed across LM status for the KOOS Symptom subscale, ACLR + LM repair (76.0 ± 18.3) resulted in significantly lower KOOS Symptoms scores compared to isolated ACLR (78.3 ± 17.9, p = 0.0097) and ACLR + LM injury left in situ (78.3 ± 17.4, p = 0.041). All other post-hoc comparisons were statistically insignificant (Table 3).
Postoperative KOOS by Lateral Meniscal Status 5 years after ACLR
Table 4 shows KOOS results at 5-year follow-up across LM treatment methods. The overall 5-year follow-up data was available for 22,291 patients (70.1%). No significant differences were found between isolated ACLR or the four LM treatment methods for four of five (4/5) KOOS subscales: Sports/Rec, Pain, ADL, and QoL. Significant difference was seen for the KOOS Symptoms subscale (p = 0.018). However, when post hoc comparisons were performed across LM status for the KOOS Symptoms subscale, not pairwise comparisons were found to be statistically significant (Table 5).
Postoperative KOOS by Lateral Meniscal Status 10 years after ACLR
Table 6 shows KOOS results at 10-year follow-up across LM treatment methods. The overall 10-year follow-up data was available for 11,092 patients (34.9%). No significant differences were found between isolated ACLR or the four LM treatment methods for four of five (4/5) KOOS subscales: Sports/Rec, Pain, ADL, and QoL. Significant difference was seen for the KOOS Symptoms subscale (p = 0.0095). When post hoc comparisons were performed across LM status for the KOOS Symptoms subscale, ACLR + LM resection (80.4 ± 18.0) had significantly lower scores than isolated ACLR (82.3 ± 17.6, p = 0.041). All other post hoc comparisons were statistically insignificant (Table 7).
Discussion
The main findings of this study were that type of LM intervention in the setting of primary ACLR statistically affected postoperative KOOS scores. However, the difference found in the KOOS subscales falls below minimal clinical important difference (MCID) [29].
At 2-year follow-up, KOOS values from this study are comparable with the literature, particularly for isolated ACLR, ACLR + LM repair, and ACLR + LM resection [19, 20, 30,31,32]. This supports the current study’s results and adds further information to the body of literature on functional knee recovery after ACLR. No significant differences were found between isolated ACLR or the four LM treatment methods in 4 of 5 subscales of the KOOS (Sports/Rec, Pain, ADL, QoL). ACLR + LM repair had significantly lower mean KOOS Symptoms scores than isolated ACLR and ACLR + LM injury left in situ for this follow-up timepoint. While some subjective knee scores may be slower to recover after ACLR with meniscal repair compared to isolated ACLR and ACLR with meniscal resection [18], numerous studies have shown the long term benefit of repairing meniscal lesions in the setting of ACLR, resulting in improved QoL and decreased risk of osteoarthritis development [30, 33,34,35]. Yet, in this study, mean KOOS Symptoms scores were significantly lower for the ACLR + LM repair group compared to isolated ACLR and ACLR + LM injury left in situ groups. It is possible that the nature of non-surgically treated LM tears in this study was different compared to surgically treated LM injuries. Tears left in situ in this study may have been partial or non-traumatic [17, 36], having less impact on postoperative course and thus managed without intervention. However, a 2016 study calculating patient acceptable symptom state (PASS) values for KOOS subscales of patients 1 to 5 years postoperatively after ACLR found PASS for KOOS Symptoms subscale to be 57.1 (sensitivity 78%, specificity 67%) [27, 37]. At 2-year follow up in this current study, mean KOOS Symptoms subscale scores in the isolated ACLR as well as ACLR with all concomitant LM treatment methods were greater than the PASS value of 57.1. Furthermore, a MCID value for KOOS Symptoms subscale has been calculated at the threshold of 15.7 for early follow-up after ACLR [29]. When examining the comparisons with statistically significance in this study, differences in mean values between isolated ACLR and ACLR + LM repair as well as ACLR + LM injury left in situ were 2.3, much lower than previously reported MCID for the subscale score. However, wide standard deviations exist, suggesting that larger differences may have been present between some patients in the various treatment groups. Thus, the question remains on the clinical meaningfulness of the statistical findings of KOOS Symptoms subscale scores in the current study, as it is uncertain whether the small statistical differences between isolated ACLR, ACLR + LM repair, and ACLR + LM injury left in situ correlate with any meaningful clinical difference [38, 39]. It is possible that statistical significance has been achieved primarily due to large sample size, while the absolute difference between the groups may not be clinically meaningful to the patient.
At 5-year follow-up, significant differences were found between isolated ACLR and the four LM treatment methods in in KOOS Symptoms subscale. However, post hoc comparisons (comparing CI) showed no statistically significant differences between the groups. Additionally, although no direct comparisons were made between follow-up time points, KOOS subscale outcomes appeared to be preserved between 2- and 5-year follow up for isolated ACLR and ACLR with all LM treatment methods, suggesting the sustainability of each treatment option in terms of KOOS outcomes overtime.
At 10-year follow-up, no significant differences were found between isolated ACLR or the four LM treatment methods in 4 of 5 subscales of the KOOS. However, post hoc comparisons revealed that mean KOOS Symptoms for ACLR + LM resection had significantly lower scores than isolated ACLR. The risk of osteoarthritis after both ACLR and partial meniscal resection is well established [14, 40, 41], and a recent meta-analysis reported that although the risk of osteoarthritis development after ACLR exists, concomitant partial meniscal resection increases that risk of osteoarthritis development [42]. It is possible that patients undergoing ACLR + LM resection developed more symptomatic arthritis than those with isolated ACLR, thus accounting for the significant difference in KOOS symptom subscale scores at 10-year follow-up. These differences may reflect the clinical importance of protecting the LM in the setting of ACLR, as the value of meniscal preservation on long term knee health is widely agreed upon [43,44,45,46]. However, with an absolute difference of less than 2 points between the Symptoms subscale scores between the two groups, it again is uncertain that this difference is associated with any clinically significance [38, 39, 47] Thus, more research is needed to determine PASS values as well as MCID values at 10-year follow-up in order to aid in better understanding differences in KOOS subscale scores overtime in patients undergoing ACLR.
The results of this study provide valuable information on postoperative KOOS after isolated ACLR and ACLR with various treatments of LM lesions at short-, mid-, and long-term follow-up points in a large sample size of patients. Although this is just one data point, surgeons can utilize this information on functional knee recovery when considering options to address LM injury in the setting ACLR and when educating patients on expectations in the pre- and postoperative periods.
Lastly, the study has several limitations. Despite the large sample size and long-term follow-up, this cohort study from a registry of patients is a limitation as it includes patients undergoing operations at various centers with differing surgical techniques, rehabilitation guidelines, and quality of rehabilitation. Additionally, the follow-up data was limited, specifically at the 10-year follow-up timepoint leading to possible limitations when comparing the outcomes between the different treatment groups. In this study, only the KOOS was used to assess knee function after ACLR. Although widely used to assess knee function in patients after ACLR, the KOOS may not address all important functional limitation related to ACLR [48,49,50] and therefore, the KOOS may not fully capture all the important functional limitations related to ACLR. Also, no data was available on indications for choice of LM treatment, thus, it is unclear why some of the tears were decided to be repaired, resected, or treated nonoperatively. No data regarding the type or location of LM tear, and proportion of LM resected, were available either leading to some limitations as differing severities of LM injury as well as surgeon expertise, training, and clinical decision-making may affect the outcomes. Lastly, the presence of other injuries in addition to LM injuries, such as cartilaginous and other non-surgically treated ligament injuries, as well as possible revision surgeries during the follow-up period, may have influenced the postoperative outcomes.
Conclusion
The results of this study suggest that LM injury during ACLR is associated with lower KOOS scores, particularly in the Symptoms subscale, at short- and long-term follow-up. However, this finding falls below MCID and therefore may not be clinically relevant [29].
Availability of data and materials
The dataset analyzed during the current study are available from the corresponding author on reasonable request.
References
Kopf S, Beaufils P, Hirschmann MT, Rotigliano N, Ollivier M, Pereira H, Verdonk R, Darabos N, Ntagiopoulos P, Dejour D, et al. Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1177–94.
Sayampanathan AA, Howe BK. Bin Abd Razak HR, Chi CH, Tan AH. Epidemiology of surgically managed anterior cruciate ligament ruptures in a sports surgery practice. J Orthop Surg (Hong Kong). 2017;25(1):2309499016684289.
D'Ambrosi R, Meena A, Raj A, Ursino N, Mangiavini L, Herbort M, Fink C. In elite athletes with meniscal injuries, always repair the lateral, think about the medial! A systematic review. Knee Surg Sports Traumatol Arthrosc. 2023;31(6):2500–10.
Rönnblad E, Barenius B, Stålman A, Eriksson K. Failed meniscal repair increases the risk for osteoarthritis and poor knee function at an average of 9 years follow-up. Knee Surg Sports Traumatol Arthrosc. 2022;30(1):192–9.
Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB. Knee osteoarthritis risk is increased 4–6 fold after knee injury - a systematic review and meta-analysis. Br J Sports Med. 2019;53(23):1454–63.
Hoshino Y, Miyaji N, Nishida K, Nishizawa Y, Araki D, Kanzaki N, Kakutani K, Matsushita T, Kuroda R. The concomitant lateral meniscus injury increased the pivot shift in the anterior cruciate ligament-injured knee. Knee Surg Sports Traumatol Arthrosc. 2019;27(2):646–51.
Mouton C, Magosch A, Pape D, Hoffmann A, Nührenbörger C, Seil R. Ramp lesions of the medial meniscus are associated with a higher grade of dynamic rotatory laxity in ACL-injured patients in comparison to patients with an isolated injury. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1023–8.
Shelbourne KD, Heinrich J. The long-term evaluation of lateral meniscus tears left in situ at the time of anterior cruciate ligament reconstruction. Arthroscopy. 2004;20(4):346–51.
Magnussen RA, Mansour AA, Carey JL, Spindler KP. Meniscus status at anterior cruciate ligament reconstruction associated with radiographic signs of osteoarthritis at 5- to 10-year follow-up: a systematic review. J Knee Surg. 2009;22(4):347–57.
Persson F, Turkiewicz A, Bergkvist D, Neuman P, Englund M. The risk of symptomatic knee osteoarthritis after arthroscopic meniscus repair vs partial meniscectomy vs the general population. Osteoarthritis Cartilage. 2018;26(2):195–201.
Lutz C, Dalmay F, Ehkirch FP, Cucurulo T, Laporte C, Le Henaff G, Potel JF, Pujol N, Rochcongar G, Salledechou E, et al. Meniscectomy versus meniscal repair: 10 years radiological and clinical results in vertical lesions in stable knee. Orthop Traumatol Surg Res. 2015;101(8 Suppl):S327-331.
Weber J, Koch M, Angele P, Zellner J. The role of meniscal repair for prevention of early onset of osteoarthritis. J Exp Orthop. 2018;5(1):10.
Paxton ES, Stock MV, Brophy RH. Meniscal repair versus partial meniscectomy: a systematic review comparing reoperation rates and clinical outcomes. Arthroscopy. 2011;27(9):1275–88.
Stein T, Mehling AP, Welsch F, von Eisenhart-Rothe R, Jäger A. Long-term outcome after arthroscopic meniscal repair versus arthroscopic partial meniscectomy for traumatic meniscal tears. Am J Sports Med. 2010;38(8):1542–8.
Cavanaugh JT, Killian SE. Rehabilitation following meniscal repair. Curr Rev Musculoskelet Med. 2012;5(1):46–58.
Shieh A, Bastrom T, Roocroft J, Edmonds EW, Pennock AT. Meniscus tear patterns in relation to skeletal immaturity: children versus adolescents. Am J Sports Med. 2013;41(12):2779–83.
Beaufils P, Becker R, Kopf S, Englund M, Verdonk R, Ollivier M, Seil R. Surgical Management of Degenerative Meniscus Lesions: The 2016 ESSKA Meniscus Consensus. Joints. 2017;5(2):59–69.
Svantesson E, Cristiani R, Hamrin Senorski E, Forssblad M, Samuelsson K, Stålman A. Meniscal repair results in inferior short-term outcomes compared with meniscal resection: a cohort study of 6398 patients with primary anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2018;26(8):2251–8.
Phillips M, Rönnblad E, Lopez-Rengstig L, Svantesson E, Stålman A, Eriksson K, Ayeni OR, Samuelsson K. Meniscus repair with simultaneous ACL reconstruction demonstrated similar clinical outcomes as isolated ACL repair: a result not seen with meniscus resection. Knee Surg Sports Traumatol Arthrosc. 2018;26(8):2270–7.
LaPrade CM, Dornan GJ, Granan LP, LaPrade RF, Engebretsen L. Outcomes After Anterior Cruciate Ligament Reconstruction Using the Norwegian Knee Ligament Registry of 4691 Patients: How Does Meniscal Repair or Resection Affect Short-term Outcomes? Am J Sports Med. 2015;43(7):1591–7.
Grassi A, Dal Fabbro G, Di Paolo S, Stefanelli F, Macchiarola L, Lucidi GA, Zaffagnini S. Medial and lateral meniscus have a different role in kinematics of the ACL-deficient knee: a systematic review. JISAKOS. 2019;4(5):233–41.
Musahl V, Rahnemai-Azar AA, Costello J, Arner JW, Fu FH, Hoshino Y, Lopomo N, Samuelsson K, Irrgang JJ. The Influence of Meniscal and Anterolateral Capsular Injury on Knee Laxity in Patients With Anterior Cruciate Ligament Injuries. Am J Sports Med. 2016;44(12):3126–31.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–9.
Björnsson H, Andernord D, Desai N, Norrby O, Forssblad M, Petzold M, Karlsson J, Samuelsson K. No difference in revision rates between single- and double-bundle anterior cruciate ligament reconstruction: a comparative study of 16,791 patients from the Swedish national knee ligament register. Arthroscopy. 2015;31(4):659–64.
Kvist J, Kartus J, Karlsson J, Forssblad M. Results from the Swedish national anterior cruciate ligament register. Arthroscopy. 2014;30(7):803–10.
Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. 2003;1:64.
Svantesson E, Hamrin Senorski E, Webster KE, Karlsson J, Diermeier T, Rothrauff BB, Meredith SJ, Rauer T, Irrgang JJ, Spindler KP, et al. Clinical outcomes after anterior cruciate ligament injury: panther symposium ACL injury clinical outcomes consensus group. Knee Surg Sports Traumatol Arthrosc. 2020;28(8):2415–34.
Kaarre J, Simonson R, Ris V, Snaebjörnsson T, Irrgang JJ, Musahl V, Samuelsson K, Hamrin Senorski E: When ACL reconstruction does not help: risk factors associated with not achieving the minimal important change for the KOOS Sport/Rec and QoL. Br J Sports Med 2023:bjsports-2022–106191.
Beletsky A, Naami E, Lu Y, Polce EM, Chahla J, Okoroha KR, Bush-Joseph C, Bach B, Yanke A, Forsythe B, et al. The Minimally Clinically Important Difference and Substantial Clinical Benefit in Anterior Cruciate Ligament Reconstruction: A Time-to-Achievement Analysis. Orthopedics. 2021;44(5):299–305.
Westermann RW, Wright RW, Spindler KP, Huston LJ, Wolf BR. Meniscal repair with concurrent anterior cruciate ligament reconstruction: operative success and patient outcomes at 6-year follow-up. Am J Sports Med. 2014;42(9):2184–92.
Wright RW, Huston LJ, Haas AK, Allen CR, Anderson AF, Cooper DE, DeBerardino TM, Dunn WR, Lantz BBA, Mann B, et al. Predictors of Patient-Reported Outcomes at 2 Years After Revision Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2019;47(10):2394–401.
Cristiani R, Parling A, Forssblad M, Edman G, Engström B, Stålman A. Meniscus Repair Does Not Result in an Inferior Short-term Outcome Compared With Meniscus Resection: An Analysis of 5,378 Patients With Primary Anterior Cruciate Ligament Reconstruction. Arthroscopy. 2020;36(4):1145–53.
Yang YP, Ma X, An H, Liu XP, An N, Ao YF. Meniscus repair with simultaneous anterior cruciate ligament reconstruction: Clinical outcomes, failure rates and subsequent processing. Chin J Traumatol. 2022;25(1):37–44.
Barber FA, Click SD. Meniscus repair rehabilitation with concurrent anterior cruciate reconstruction. Arthroscopy. 1997;13(4):433–7.
Nepple JJ, Dunn WR, Wright RW. Meniscal repair outcomes at greater than five years: a systematic literature review and meta-analysis. J Bone Joint Surg Am. 2012;94(24):2222–7.
Zemanovic JR, McAllister DR, Hame SL. Nonoperative treatment of partial-thickness meniscal tears identified during anterior cruciate ligament reconstruction. Orthopedics. 2004;27(7):755–8.
Muller B, Yabroudi MA, Lynch A, Lai CL, van Dijk CN, Fu FH, Irrgang JJ. Defining Thresholds for the Patient Acceptable Symptom State for the IKDC Subjective Knee Form and KOOS for Patients Who Underwent ACL Reconstruction. Am J Sports Med. 2016;44(11):2820–6.
Roos EM, Toksvig-Larsen S. Knee injury and Osteoarthritis Outcome Score (KOOS) - validation and comparison to the WOMAC in total knee replacement. Health Qual Life Outcomes. 2003;1:17.
Roos EM, Boyle E, Frobell RB, Lohmander LS, Ingelsrud LH. It is good to feel better, but better to feel good: whether a patient finds treatment ‘successful’ or not depends on the questions researchers ask. Br J Sports Med. 2019;53(23):1474.
Cinque ME, Dornan GJ, Chahla J, Moatshe G, LaPrade RF. High Rates of Osteoarthritis Develop After Anterior Cruciate Ligament Surgery: An Analysis of 4108 Patients. Am J Sports Med. 2017;46(8):2011–9.
Karia M, Ghaly Y, Al-Hadithy N, Mordecai S, Gupte C. Current concepts in the techniques, indications and outcomes of meniscal repairs. Eur J Orthop Surg Traumatol. 2019;29(3):509–20.
Claes S, Hermie L, Verdonk R, Bellemans J, Verdonk P. Is osteoarthritis an inevitable consequence of anterior cruciate ligament reconstruction? A meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):1967–76.
Wright RW, Huston LJ, Haas AK, Nwosu SK, Allen CR, Anderson AF, Cooper DE, DeBerardino TM, Dunn WR, Lantz BBA, et al. Meniscal Repair in the Setting of Revision Anterior Cruciate Ligament Reconstruction: Results From the MARS Cohort. Am J Sports Med. 2020;48(12):2978–85.
Øiestad BE, Engebretsen L, Storheim K, Risberg MA. Knee osteoarthritis after anterior cruciate ligament injury: a systematic review. Am J Sports Med. 2009;37(7):1434–43.
Cohen M, Amaro JT, Ejnisman B, Carvalho RT, Nakano KK, Peccin MS, Teixeira R, Laurino CF, Abdalla RJ. Anterior cruciate ligament reconstruction after 10 to 15 years: association between meniscectomy and osteoarthrosis. Arthroscopy. 2007;23(6):629–34.
Shelbourne KD, Gray T. Results of anterior cruciate ligament reconstruction based on meniscus and articular cartilage status at the time of surgery. Five- to fifteen-year evaluations. Am J Sports Med. 2000;28(4):446–52.
Ehrich EW, Davies GM, Watson DJ, Bolognese JA, Seidenberg BC, Bellamy N. Minimal perceptible clinical improvement with the Western Ontario and McMaster Universities osteoarthritis index questionnaire and global assessments in patients with osteoarthritis. J Rheumatol. 2000;27(11):2635–41.
Svantesson E, Hamrin Senorski E, Webster KE, Karlsson J, Diermeier T, Rothrauff BB, Meredith SJ, Rauer T, Irrgang JJ, Spindler KP, et al. Clinical Outcomes After Anterior Cruciate Ligament Injury: Panther Symposium ACL Injury Clinical Outcomes Consensus Group. Orthopc Jf Sports Med. 2020;8(7):2325967120934751–2325967120934751.
Comins J, Brodersen J, Krogsgaard M, Beyer N. Rasch analysis of the Knee injury and Osteoarthritis Outcome Score (KOOS): a statistical re-evaluation. Scand J Med Sci Sports. 2008;18(3):336–45.
Piussi R, Simonson R, Högberg J, Thomeé R, Samuelsson K, Hamrin Senorski E. Psychological Patient-reported Outcomes Cannot Predict a Second Anterior Cruciate Ligament Injury in Patients who Return to Sports after an Anterior Cruciate Ligament Reconstruction. Int J Sports Phys Ther. 2022;17(7):1340–50.
Acknowledgements
The authors would like to thank statisticians Bengt Bengtsson from the Statistiska Konsultgruppen for help the statistical analyses.
Funding
Open access funding provided by University of Gothenburg.
Author information
Authors and Affiliations
Contributions
All listed authors have contributed substantially to this work: literature search, interpretation of the results, and initial manuscript preparation were performed by JK, ZJH, FP and JOW. EAG, EHS, VM, and KS assisted with study design, as well as editing and finalizing the manuscript. All authors have read and approved the final manuscript to be submitted and published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
According to the Swedish law (2008:35) no informed consent is required for national registries. Patients are provided with information about the registry and possibility to withdraw from participation at any time. This study was approved by the Regional Ethical Board in Stockholm, Sweden (2011/337–31/3), and the Swedish Ethical Review Authority (2022–00913-01) as well as performed in accordance with the Declaration of Helsinki. The Swedish National Knee Ligament Registry complies with the Swedish legislation related to data security and therefore, no informed consent is necessary for national databases in Sweden. Investigators had access only to unidentifiable patient data.
Consent for publication
Not applicable.
Competing interests
JK, ZJH, FP, JOW, and EAG have nothing to disclose. EHS is an associate editor of the Journal of Orthopaedic and Sports Physical Therapy (JOSPT). VM reports educational grants, consulting fees, and speaking fees from Smith & Nephew plc, educational grants from Arthrex and DePuy/Synthes, is a board member of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), and deputy editor-in-chief of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA). KS is a member of the Board of Directors in Getinge AB (publ.).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table s1.
Baseline characteristics of the included patients with 2-year follow-up data. Table s2. Baseline characteristics of the included patients with 5-year follow-up data. Table s3. Baseline characteristics of the included patients with 10-year follow-up data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kaarre, J., Herman, Z.J., Persson, F. et al. Differences in postoperative knee function based on concomitant treatment of lateral meniscal injury in the setting of primary ACL reconstruction. BMC Musculoskelet Disord 24, 737 (2023). https://doi.org/10.1186/s12891-023-06867-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06867-z