
Abstract
Background
Neck pain, with or without radiculopathy, can have significant negative effects on physical and mental wellbeing. Mental health symptoms are known to worsen prognosis across a range of musculoskeletal conditions. Understanding the association between mental health symptoms and health outcomes in this population has not been established. Our aim was to systematically review the association between psychosocial factors and/or mental health symptoms on health outcomes in adults with neck pain, with or without radiculopathy.
Methods
A systematic review of published and unpublished literature databases was completed. Studies reporting mental health symptoms and health outcomes in adults with neck pain with or without radiculopathy were included. Due to significant clinical heterogeneity, a narrative synthesis was completed. Each outcome was assessed using GRADE.
Results
Twenty-three studies were included (N = 21,968 participants). Sixteen studies assessed neck pain only (N = 17,604 participants); seven studies assessed neck pain with radiculopathy (N = 4,364 participants). Depressive symptoms were associated with poorer health outcomes in people with neck pain and neck pain with radiculopathy. These findings were from seven low-quality studies, and an additional six studies reported no association. Low-quality evidence reported that distress and anxiety symptoms were associated with poorer health outcomes in people with neck pain and radiculopathy and very low-quality evidence showed this in people with neck pain only. Stress and higher job strain were negatively associated with poorer health outcomes measured by the presence of pain in two studies of very low quality.
Conclusions
Across a small number of highly heterogenous, low quality studies mental health symptoms are negatively associated with health outcomes in people with neck pain with radiculopathy and neck pain without radiculopathy. Clinicians should continue to utilise robust clinical reasoning when assessing the complex factors impacting a person’s presentation with neck pain with or without radiculopathy.
PROSPERO registration number
CRD42020169497.
Similar content being viewed by others


Background
Cervical spine pain with or without radiculopathy (CSp ± R) has a significant negative impact on people’s physical and mental health. It is an enormous burden for individuals, families and societies [1, 2]. The reported incidence of cervical spine radiculopathy (CSR) is between 0.83 and 1.79 per 1000 person-years, and prevalence ranges from 1.2 to 5.8 per 1000 [3]. The one-year incidence of cervical spine pain ranges between 10% and 21% [4, 5]. The global prevalence of cervical spine pain and years lived with disability has each increased by 19% over the last 10 years [6].
The association between psychological and/or mental health symptoms and LBP is well-established with low back pain [7, 8]. It is recognised that these symptoms are negatively associated with health outcomes and quality of life [7, 8]. Psychosocial factors encompass a wide range of cognitions, emotions, behaviours and family and workplace influences [9]. Mental health symptoms or conditions are an extension of such factors. Stress, anxiety, depression and negative coping behaviours negatively impact prognosis with musculoskeletal conditions such as low back pain [10], work related neck pain [11], knee osteoarthritis [12], carpal tunnel syndrome [13] and shoulder pain [14]. Psychosocial factors and/or mental health symptoms should be considered as part of a clinical reasoning framework to positively affect health outcomes and support prognosis [15]. The extent to which these factors may impact acute or persistent CSp ± R across global locations has not yet been synthesised in a systematic review study design.
Establishing the associative factors between psychosocial factors and/or mental health symptoms and health outcomes will enhance our understanding of these complex interactions. Furthermore, it should enhance clinicians’ assessment and management plans [16, 17]. To the authors’ knowledge, no systematic review has examined this association. Consequently, we report a systematic review assessing the association between psychosocial factors and/or mental health symptoms to health outcomes in adults with CSp ± R.
Methods
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) database (Reference: CRD42020169497). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [18] was followed. The review protocol has been previously published [19].
Search strategy
A systematic search of the electronic databases EMBASE, CINAHL and MEDLINE (PubMed) from inception to 31st April 2021 was completed by one reviewer (NS) under the supervision of a second (MM). The search was updated by the lead reviewer (MM) from 31st April 2021 to 1st September 2022. The PubMed search strategy is presented in Appendix 1. Unpublished (grey) literature search and trial registry was searched (e.g., WHO.It, ZETOC, British library higher education thesis deposits). All included studies underwent reference checking.
Eligibility criteria
Studies were included if they met the following criteria:
-
a.
A sample that included adults aged 18 years and over with CSp ± R. Following the International Association of the Study of Pain [20] and The Bone and Joint Decade 2000–2010 Task Force on Neck Pain [21] cervical spine pain definitions. We defined neck pain as cervical spine pain perceived anywhere in the posterior neck region to the first thoracic spinous process. Furthermore, a pragmatic approach was undertaken, and studies with probable or definite cervical spine radiculopathy diagnoses were adapted from IASP and North American Spine Society were eligible for inclusion [20, 22, 23] (Supplementary file 1).
-
b.
Assessed psychosocial factors or mental health symptoms as an exposure. Studies must have investigated one or more psychosocial or mental health symptoms (or conditions). Psychosocial factors may have included: cognitive (e.g., neuropsychological functioning), affective (e.g., distress, mood), behavioural (e.g., coping strategies), vocational (e.g., job satisfaction, self-perceived work ability) or interpersonal processes (e.g., social support) [24]. Mental health symptoms and conditions such as depressive symptoms, clinical depression, anxiety, perceived stress, personality, psychotic, traumatic and eating disorders were also considered. Self-reported, objective, standardised questionnaires (e.g., Beck Depression Index, Karasek’s Job Control Questionnaire, GHQ-12) and psychosocial factors or mental health symptoms assessed using dichotomous data (“yes/no”) were also considered. Studies were also eligible if the study population compared different severities of mental health symptoms, conditions or psychosocial factors related to an outcome.
-
c.
Published in English language and were either case-control, cross-sectional or cohort study design.
No restriction on publication date was applied. Studies were excluded if they were animal or cadaveric studies, commentaries, editorials, single case studies, reports or laboratory data, books or book chapters, letters, conference posters or proceedings or study protocols. Furthermore, we excluded studies whose participants’ CSp ± R resulted from an upper motor neuron lesion, fracture, radiculitis, myelopathy, post-surgery, whiplash-associated disorder, systemic pathology or metabolic diseases such as diabetes.
Study identification
We uploaded the search strategy results into the Rayann systematic review online platform (https://www.rayyan.ai). Two reviewers (MM, TS) independently reviewed, checked titles and abstracts and documented decisions on study eligibility. All potentially eligible full-text papers were independently reviewed by the same two reviewers to determine final inclusion. A third reviewer (MT) was available to review any disagreements; this was not required.
Data extraction
Data extraction forms were designed by the lead reviewer (MM). This form was reviewed and agreed upon by all reviewers. Two reviewers (MM, JT) independently extracted data from included studies. The same two reviewers discussed the data extracted and reached a consensus through discussion. Data extracted included lead author and date of publication; study design; study demographics (country, sample size, age range or mean gender ratio); definition of exposure; report of the comparator; outcome measure description; risk estimates (risk ratios, hazard ratios, odds ratio and mean differences including 95% confidence intervals (CI)) where available.
Methodological quality
Two reviewers (MM, TS) independently assessed the quality of each included study using a Newcastle-Ottawa Quality Scale (NOS) assessment quality appraisal tool [25]. The NOS checklist assesses the quality of studies across three domains: selection of the studies groups, comparability of the groups and control for confounding factors and exposure. The two reviewers discussed NOS quality appraisal scores and, through discussion, reached a consensus. The certainty of the evidence was assessed as very low, low, moderate or high certainty using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) [26].
Synthesis
Two reviewers (MM, TS) assessed all included analyses from a clinical (e.g., diagnosis, variability in population characteristics) and study methodology perspective to determine the suitability of meta-analysis. Both reviewers agreed on the existence of significant clinical heterogeneity, questioning the appropriateness of meta-analysis. Data were, therefore, narratively analysed by patient populations and clinical diagnoses.
Results
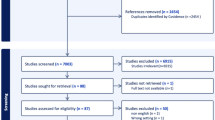
The results of the search strategy are presented in Fig. 1. A total of 6732 studies were identified and screened. Of these 6450 were excluded from the title and abstract. Of the remaining 282 full-text studies reviewed, 259 were excluded. Twenty-three studies met the inclusion criteria and were included in the review [2, 27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48].

PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases, registers and other sources. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: https://doi.org/10.1136/bmj.n71
Study characteristics—population and location
A total of 21,968 participants were recruited across the 23 included studies. There were 17,604 participants with non-specific neck pain and 4364 participants with CSR. Sixteen studies included neck pain populations, five were cohort study designs [27, 29, 34, 43, 46] and 11 were cross-sectional in study design [2, 28, 32, 35,36,37, 39, 41, 42, 45, 47]. Of the seven studies that included CSR populations, five were observational [30, 31, 38, 44, 48] and two were secondary analyses of healthcare records [33, 40]. The characteristics of the included studies are presented in Table 1 (summary study characteristics). A full table of study characteristics can be accessed in Supplementary File 2.
Seven studies included participants with CSR recruited from elective spinal surgery waiting lists. The CSR diagnosis was made using imaging associated with a neurological deficit on clinical examination [30, 31, 33, 38, 40, 44, 48]. Despite contacting the corresponding authors for further information, no further details were obtained.
Nine studies measured depressive symptoms [2, 29, 32, 33, 38, 40, 43, 45, 48]. Five studies measured anxiety symptoms [27, 32, 40, 43, 48] and three studies measured job-strain and stress [34, 35, 46]. Three studies used the psychological components of SF-36 [30, 39, 47]. Two studies used the psychological components of SF-12 [31, 35]. One study measured kinesiophobia [28] and one study measured catastrophising [41]. Three studies used more than one mental health symptom measurement [32, 35, 43]. A summary of the mental health symptoms and tools to measure the severity of mental health conditions across the 23 included studies are presented in Table 1.
Neck pain associative outcomes: depressive symptoms
Of the 16 studies with people with non-specific neck pain, there were positive and negative associations between mental health symptoms and health outcomes. Four studies reported a positive association [2, 32, 43], and one study reported a negative association [29] with depression. Using GRADE classifications, the overall strength of evidence was ‘low’, which is attributed to a high risk of bias.
Depressive symptoms measured through Hospital Anxiety and Depression Scale (HADS) was positively associated with the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire (r:0.245, p = 0.004) [43], Odds Ratio (OR): 3.46 (95% CI: 2.01–5.95) [45] and OR: 1.02 (95% CI: 0.98–1.06) [32]. When measured through the Center for Epidemiologic Studies Depression Scale (CES-D), depressive symptoms were positively associated with pain (Hazard Ratio (HR): 3.97, 95% CI: 1.81–8.72) [2]. Depressive symptoms measured by the Montgomery Asberg Depression Rating Scale were negatively associated with Neck Disability Index (NDI) (OR: 0.94, 95% CI: 0.86–1.03) [29].
Neck pain associative outcomes: anxiety symptoms
Anxiety symptoms were positively associated with poorer health outcomes in two studies [27, 32] and had no significance in one study [43]. The overall strength of evidence was ‘very low’ in the GRADE assessment which is attributed to a high risk of bias and imprecision.
Anxiety symptoms measured through the Nordic musculoskeletal questionnaire were more likely to be associated with sick leave (OR: 1.4, 95% CI: 0.9–2.1) [27]. Anxiety symptoms measured through HADS were more likely to be associated with the presence of pain (OR: 1.02, 95% CI: 0.98–1.05) [32]. Whereas in one study, anxiety symptoms measured through HADS had no statistical significance with DASH (r: 0.104, p = 0.220) [43].
Neck pain associative outcomes: Kinesiophobia
Kinesiophobia was associated with poorer health and the presence of pain (r: 0.566, P = < 0.05) in one study [28].
Neck pain associative outcomes: Catastrophising
Catastrophising, measured by the catastrophising pain scale, was positively associated with pain (OR: 1.03, 95% CI 0.97–1.09) in one study [41].
Neck pain associative outcomes: stress
Stress was positively associated with the presence of pain (OR: 0.32, 95% CI: 0.25–0.39) in one study [34].
Neck pain associative outcomes: job strain
A higher job strain was negatively associated with the presence of pain in the neck and shoulder in two studies (Relative Risk (RR): 1.79, 95% CI: 1.19–2.69) [46] and OR: 1.51 (95% CI: 0.88–2.59) [35]. This was rated as ‘low’ in the GRADE assessment, attributed to imprecision across the studies.
Neck pain associative outcomes: distress
Distress was positively associated with health outcomes in three studies [37, 39, 42] and negatively associated with health outcomes in two studies [36, 47]. The overall strength of evidence using the GRADE approach is ‘very low’, which is attributed to a high risk of bias and imprecision.
Psychological distress measures were positively associated with the presence of pain when measured by SF-36 (r2: 0.12, p < 0.01) [39] and Hopkins Check List-10 (OR: 2.32, 95% CI: 1.20–3.43) [42]. Similarly, this was positively associated with NDI (OR: 1.75, 95% CI 0.83–3.70) [37]. Two studies reported a negative association between distress and the presence of pain (OR: 0.88, 95% CI: 0.62–1.24) [36] and OR: -0.3, 95% CI -0.4-0.1 [47].
Cervical spine radiculopathy associative outcomes: depressive symptoms
Of the seven studies with CSR populations, there were both positive and negative associations between depressive symptoms and health outcomes. Three studies reported a negative association [33, 40, 44], whereas one study reported a positive association [38]. The overall strength of evidence using the GRADE approach was ‘very low’, this is attributed to a high risk of bias and imprecision.
Depressive symptoms were positively associated with NDI when measured through the Zung Self-Reporting Scale (NDI with depression 42.8 (High) (SD: 19.9) vs. 20.9 (SD: 15.9), p < 0.0001) [38]. Three studies reported negative associations (OR: 0.71, p < 0.001) [44], regression coefficient 0.25 (95% CI: -0.01-0.50) [40] and risk of depression not being significant (p = 0.3) [33].
Cervical spine radiculopathy associative outcomes: distress
There were two studies that reported a positive association between SF-36 (p < 0.05) [30] and SF-12 (p = 0.04) [31] and NDI. Whereas one study reported distress being negatively associated with NDI (r2 = 0.80, p = 0.0005) [44]. The overall strength of evidence using the GRADE approach was ‘very low’. This is attributed to a high risk of bias and imprecision.
Cervical spine radiculopathy associative outcomes. Anxiety symptoms
In one study, anxiety symptoms were positively associated with NDI in CSR populations (OR: 0.63, p = 0.006) [48]. All associative outcomes data are populated in Table 2.
Quality assessment. Neck pain populations
Five cohort studies included patients with non-specific neck pain as their exposure [27, 29, 34, 43, 46]. These studies scored between five and seven out of nine on the NOS. All studies met the ‘representativeness of exposed cohort’ and ‘adequate follow-up’. All five studies did not complete the ‘assessment of outcome’ item.
Eleven studies were cross-sectional in study design. Scores ranged from five to seven out of nine on the NOS. All studies met the ‘representativeness of exposed cohort’ and ‘adequate follow-up’. All studies did not meet the ‘assessment of outcome’ item. Three studies completed a secondary analysis of data [36, 37, 45]. These studies scored six to seven out of a possible nine. All studies did not meet the ‘demonstration that outcome of interest was not present at the start of study’ item and ‘assessment of outcome’. The overall strength of evidence measured through GRADE is populated in Table 3. The quality assessment tables are populated in Table 4.
Quality assessment. Cervical spine radiculopathy populations
Five cohort studies included patients with CSR as their exposure population [30, 31, 38, 44, 48]. These studies scored between six and seven out of a possible nine on NOS. All studies met the ‘representativeness of exposed cohort’ and ‘adequate follow-up’. All five studies did not complete the ‘assessment of outcome’ item. Two studies with a CSR study population were retrospective secondary data analyses where each study scored five [33] and seven [40], respectively. The overall strength of evidence measured through GRADE is populated in Table 3. The quality assessment tables are populated in Table 4.
Discussion
This is the first systematic review investigating the association of mental health symptoms and conditions with health outcomes in adults with CSp ± R. Our results indicate that depressive symptoms were associated with poorer health outcomes in seven studies classified as with ‘low quality’, four studies with CSR populations and three studies with non-specific neck pain populations. There was no association with depressive symptoms health outcomes in six studies (four studies with CSR populations and two studies with non-specific neck pain populations) with very low quality. Distress and anxiety symptoms were associated with poorer health outcomes in CSR populations and non-specific neck pain in two studies with ‘very low-level’ quality. Stress and higher job strain was negatively associated with poorer health outcomes measured by the presence of pain in two studies with very low quality sampling non-specific neck pain populations. Stress and higher job strain symptoms were not reported in our included studies that sampled CSR populations.
At the time of conducting this research, there was no universal agreement on CSR diagnosis [3, 49]. Therefore, a pragmatic approach was undertaken, and studies with probable or definite CSR diagnoses were adapted from IASP and North American Spine Society [20, 22, 23] (Supplementary file 1). The diagnostic criteria for CSR varied between each included study. Included studies used a combination of subjectively reported symptoms, clinical assessment testing associated with imaging findings assessed by a physician, and/or sensory and motor electrophysiological testing. In line with our protocol [19], the included patients with CSR would have a ‘definite’ CSR diagnosis. All participants with CSR were on an orthopaedic surgery waiting list, which may question the external validity to alternative healthcare settings such as primary care.
It is acknowledged that a recent international e-Delphi study has been published [50] with an agreement on CSR classification criteria. The 12 physiotherapists who participated in the e-Delphi reached a consensus of radicular pain with arm pain worse than neck pain and paraesthesia or numbness and/or weakness and/or altered reflex and MRI confirmed nerve root compression compatible with clinical findings [50]. Future research should now be conducted to test the reliability and determine which tools can be used to assess these criteria [50]. Strengthening these CSR diagnostic criteria should facilitate standardisation of assessment criteria across multiple health care professionals globally and enhance pooling of results and conclusions regarding this disabling condition.
Our results indicate that depressive symptoms were associated with poorer health outcomes in seven studies classified as ‘low quality’. Of these, four studies were with CSR populations and three studies with non-specific neck pain populations. There was no association with depressive symptoms health outcomes in six studies of very-low quality (four studies with CSR populations and two studies with non-specific neck pain populations). The mixed association between depressive symptoms and health outcomes across CSR and non-specific neck pain populations may be attributed to a difference in the assessment tools used to measure depressive symptoms.
Although each assessment tool has appropriate psychometric properties to measure mental health symptoms, the mode of delivery to collect these data may influence responses [64, 65]. For example, previous literature suggests people may rate their health and well-being, more favourable in telephone interviews compared to self-reported paper-based questionnaire [64, 65]. Furthermore, it is not clear whether the included studies assessing CSR and non-specific neck pain populations compared participant’s scores to the general population’s normative values or by using cut-off scores to indicate different levels of clinically relevant distress, anxiety and/or depressive symptoms [66]. These two points may provide some reasoning for the mixed association findings reported between nonspecific neck pain and CSR populations.
Comparing this review’s results to other spinal pain populations may enhance our understanding of health outcomes and inform assessment and management strategies. Depressive symptoms or clinical depression are reported to have worse recovery and greater healthcare utilisation, but not pain or work-related outcomes in people with LBP [51]. However, healthcare utilisation was based on one study and depressive symptoms were based on six highly heterogeneous studies [51]. The differences between our reported findings may be attributed to the inclusion of acute episodes of low back pain (pain lasting less than one month), whereas the CSp ± R populations in this review were all persistent in presentation (lasting more than three months).
The symptoms related to CSR are likely to be underpinnings of neuropathic pain mechanisms compared to non-neuropathic mechanisms associated with nonspecific neck pain [67]. It is known that neuropathic pain is associated with more severe pain, higher workplace absenteeism, distress and higher medical costs [67, 68] compared to non-neuropathic pain which is comparable to our review’s findings. However, it is reported that the expectation of recovery for patients with CSR pending operative management, may reduce the psychological impact on health outcomes [63]. The mixed observations across CSR and non-specific neck pain populations may therefore explained by the complex contributing biopsychosocial factors impacting a health outcomes.
The interactions and mechanisms underpinning mental health symptoms, conditions and health outcomes in musculoskeletal pain populations are highly complex [52,53,54]. Clinical conditions such as spinal pain with or without radiculopathy will have complex interactions and influences that will be unique to each individual [17]. These factors include genetic [55], pathoanatomical [56] and psychological and lifestyle health factors [17, 57]. The complex interactions will influence pain perceptions, levels of distress and, subsequently, health outcomes [58, 59]. Enhancing our knowledge and understanding of mental health symptoms on health outcomes such as disability, function and pain can guide expectations and management strategies for clinicians and patients with CSp ± R. Healthcare providers should continue to assess mental health symptoms in a holistic assessment framework as part of a robust clinical reasoning process. The identification of patients potentially at risk of long-term disability and worse recovery can enhance patient-centred care pathways and may improve health outcomes [60].
We acknowledge limitations in our review. Included studies were written in the English language or those that could be translated. This may have resulted in a publication bias of our included studies by language. Health outcomes in our target populations can often have multidimensional and complex interactions [61, 62], which may be reflected in the variability of single measurement tools in the included studies. Future research should consider the multidimensional factors and develop core outcome measurements when evaluating health outcomes for this patient population.
Conclusions
This systematic review has reported variable associations between mental health symptoms and diagnosis with health outcomes in people with CSp ± R. Stress, depressive and anxiety symptoms are associated with poorer health outcomes in patients with CSp ± R. However, this is based on a small number of low-quality studies. The low quality can be attributed to wide-ranging diagnostic criteria and population sampling methods. Further research is indicated to standard diagnosis classification criteria for radiculopathy and developing core outcomes to further our understanding of this debilitating condition.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CES-D:
-
Center for epidemiologic studies depression scale
- CSp ± R:
-
Cervical spine pain with or without radiculopathy
- CSR:
-
Cervical spine radiculopathy
- DASH:
-
Disability of arm and shoulder
- GRADE:
-
Grading of recommendations, assessment, development and evaluations
- NDI:
-
Neck disability index
- NOS:
-
Newcastle Ottawa scale
- OR:
-
Odds ratio
- SF-36:
-
Short form 36
- SF-12:
-
Short form 12
References
Hurwitz EL, Randhawa K, Yu H, Côté P, Haldeman S. The Global Spine Care Initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J. 2018 Sep;27:796–801.
Carroll LJ, Cassidy JD, Cote P. Depression as a risk factor for onset of an episode of troublesome neck and low back pain. Pain. 2004;107(1–2):134–9.
Mansfield M, Smith T, Spahr N, Thacker M. Cervical spine radiculopathy epidemiology: a systematic review. Musculoskelet Care. 2020;18(4):555–67.
Hoy D, March L, Woolf A, Blyth F, Brooks P, Smith E, et al. The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1309–15.
Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24(6):783–92.
DALYs GBD, Collaborators H, Murray CJ, Barber RM, Foreman KJ, Abbasoglu Ozgoren A, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet. 2015;386(10009):2145–91.
Wertli MM, Burgstaller JM, Weiser S, Steurer J, Kofmehl R, Held U. Influence of catastrophizing on treatment outcome in patients with nonspecific low back pain: a systematic review. Spine (Phila Pa 1976). 2014;39(3):263–73.
Pinheiro MB, Ferreira ML, Refshauge K, Maher CG, Ordonana JR, Andrade TB, et al. Symptoms of depression as a prognostic factor for low back pain: a systematic review. Spine J. 2016;16(1):105–16.
Martikainen P, Bartley M, Lahelma E. Psychosocial determinants of health in social epidemiology. Int J Epidemiol. 2002;31(6):1091–3.
Ramond A, Bouton C, Richard I, Roquelaure Y, Baufreton C, Legrand E, et al. Psychosocial risk factors for chronic low back pain in primary care–a systematic review. Fam Pract. 2011;28(1):12–21.
Shahidi B, Curran-Everett D, Maluf KS. Psychosocial, Physical, and neurophysiological risk factors for chronic Neck Pain: a prospective inception cohort study. J Pain. 2015;16(12):1288–99.
Stubbs B, Aluko Y, Myint PK, Smith TO. Prevalence of depressive symptoms and anxiety in osteoarthritis: a systematic review and meta-analysis. Age Ageing. 2016;45(2):228–35.
Harris-Adamson C, Eisen EC, Dale AM, Evanoff B, Hegmann KT, Thiese MS, et al. Personal and workplace psychosocial risk factors for carpal tunnel syndrome: a pooled study cohort: author response. Occup Environ Med. 2014;71(4):303–4.
Chester R, Jerosch-Herold C, Lewis J, Shepstone L. Psychological factors are associated with the outcome of physiotherapy for people with shoulder pain: a multicentre longitudinal cohort study. Br J Sports Med. 2018;52(4):269–75.
Edwards I, Jones M, Carr J, Braunack-Mayer A, Jensen GM. Clinical reasoning strategies in physical therapy. Phys Ther. 2004;84(4):312–30. discussion 31 – 5.
Mescouto K, Olson RE, Hodges PW, Setchell J. A critical review of the biopsychosocial model of low back pain care: time for a new approach? Disabil Rehabil. 2022;44(13):3270–84.
Green BN, Johnson CD, Haldeman S, Griffith E, Clay MB, Kane EJ, et al. A scoping review of biopsychosocial risk factors and co-morbidities for common spinal disorders. PLoS ONE. 2018;13(6):e0197987.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol (Engl Ed). 2021;74(9):790–9.
Mansfield M, Spahr N, Smith T, Stubbs B, Haig L, Thacker M. Association between psychosocial factors and mental health symptoms to cervical spine pain with or without radiculopathy on health outcomes: systematic review protocol. Pain Rep. 2021;6(1):e870.
IASP. Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Prepared by the International Association for the Study of Pain, Subcommittee on Taxonomy. Pain Suppl. 1986;3:1–226.
Haldeman S, Carroll L, Cassidy JD, Schubert J, Nygren A, Bone, et al. The bone and joint decade 2000–2010 Task Force on Neck Pain and its Associated Disorders: executive summary. Spine (Phila Pa 1976). 2008;33(4 Suppl):5–7.
Bono CM, Ghiselli G, Gilbert TJ, Kreiner DS, Reitman C, Summers JT, et al. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011;11(1):64–72.
Scholz J, Finnerup NB, Attal N, Aziz Q, Baron R, Bennett MI, et al. The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–9.
Upton J. Psychosocial factors. Encyclopedia of behavioral medicine Cham: Springer International Publishing. 2020:1795-7.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454):1490.
Alipour A, Ghaffari M, Shariati B, Jensen I, Vingard E. Four-year incidence of sick leave because of neck and shoulder pain and its association with work and lifestyle. Spine (Phila Pa 1976). 2009;34(4):413–8.
Beltran-Alacreu H, Lopez-de-Uralde-Villanueva I, Calvo-Lobo C, Fernandez-Carnero J, La Touche R. Clinical features of patients with chronic non-specific neck pain per disability level: A novel observational study. Rev Assoc Med Bras (1992). 2018;64(8):700-9.
Bohman T, Bottai M, Bjorklund M. Predictive models for short-term and long-term improvement in women under physiotherapy for chronic disabling neck pain: a longitudinal cohort study. BMJ Open. 2019;9(4):e024557.
Diebo BG, Tishelman JC, Horn S, Poorman GW, Jalai C, Segreto FA, et al. The impact of mental health on patient-reported outcomes in cervical radiculopathy or myelopathy surgery. J Clin Neurosci. 2018;54:102–8.
Divi SN, Goyal DKC, Mangan JJ, Galetta MS, Nicholson KJ, Fang T et al. Are Outcomes of Anterior Cervical Discectomy and Fusion Influenced by Presurgical Depression Symptoms on the Mental Component Score of the Short Form-12 Survey? Spine (Phila Pa 1976). 2020;45(3):201–7.
Elbinoune I, Amine B, Shyen S, Gueddari S, Abouqal R, Hajjaj-Hassouni N. Chronic neck pain and anxiety-depression: prevalence and associated risk factors. Pan Afr Med J. 2016;24:89.
Engquist M, Lofgren H, Oberg B, Holtz A, Peolsson A, Soderlund A, et al. Factors affecting the outcome of Surgical Versus Nonsurgical Treatment of Cervical Radiculopathy: a Randomized, controlled study. Spine (Phila Pa 1976). 2015;40(20):1553–63.
Grimby-Ekman A, Andersson EM, Hagberg M. Analyzing musculoskeletal neck pain, measured as present pain and periods of pain, with three different regression models: a cohort study. BMC Musculoskelet Disord. 2009;10:73.
Hoe VC, Kelsall HL, Urquhart DM, Sim MR. Risk factors for musculoskeletal symptoms of the neck or shoulder alone or neck and shoulder among hospital nurses. Occup Environ Med. 2012;69(3):198–204.
Hill JC, Lewis M, Sim J, Hay EM, Dziedzic K. Predictors of poor outcome in patients with neck pain treated by physical therapy. Clin J Pain. 2007;23(8):683–90.
Hurwitz EL, Goldstein MS, Morgenstern H, Chiang LM. The impact of psychosocial factors on neck pain and disability outcomes among primary care patients: results from the UCLA Neck Pain Study. Disabil Rehabil. 2006;28(21):1319–29.
Kim EJ, Chotai S, Schneider BJ, Sivaganesan A, McGirt MJ, Devin CJ. Effect of Depression on patient-reported outcomes following cervical epidural steroid injection for degenerative spine disease. Pain Med. 2018;19(12):2371–6.
Lee KC, Chiu TT, Lam TH. The role of fear-avoidance beliefs in patients with neck pain: relationships with current and future disability and work capacity. Clin Rehabil. 2007;21(9):812–21.
MacDowall A, Skeppholm M, Lindhagen L, Robinson Y, Olerud C. Effects of preoperative mental distress versus surgical modality, arthroplasty, or fusion on long-term outcome in patients with cervical radiculopathy. J Neurosurg Spine. 2018;29(4):371–9.
Meisingset I, Stensdotter AK, Woodhouse A, Vasseljen O. Predictors for global perceived effect after physiotherapy in patients with neck pain: an observational study. Physiotherapy. 2018;104(4):400–7.
Myhre K, Roe C, Marchand GH, Keller A, Bautz-Holter E, Leivseth G, et al. Fear-avoidance beliefs associated with perceived psychological and social factors at work among patients with neck and back pain: a cross-sectional multicentre study. BMC Musculoskelet Disord. 2013;14:329.
McLean SM, Moffett JK, Sharp DM, Gardiner E. An investigation to determine the association between neck pain and upper limb disability for patients with non-specific neck pain: a secondary analysis. Man Ther. 2011;16(5):434–9.
Peolsson A, Vavruch L, Oberg B. Predictive factors for arm pain, neck pain, neck specific disability and health after anterior cervical decompression and fusion. Acta Neurochir (Wien). 2006;148(2):167–73. discussion 73.
Pico-Espinosa OJ, Cote P, Hogg-Johnson S, Jensen I, Axen I, Holm LW, et al. Trajectories of Pain Intensity over 1 year in adults with disabling Subacute or Chronic Neck Pain. Clin J Pain. 2019;35(8):678–85.
van den Heuvel SG, van der Beek AJ, Blatter BM, Hoogendoorn WE, Bongers PM. Psychosocial work characteristics in relation to neck and upper limb symptoms. Pain. 2005;114(1–2):47–53.
Rodriguez-Romero B, Perez-Valino C, Ageitos-Alonso B, Pertega-Diaz S. Prevalence and Associated factors for Musculoskeletal Pain and Disability among Spanish Music Conservatory Students. Med Probl Perform Art. 2016;31(4):193–200.
Wibault J, oberg B, Dedering A, Lofgren H, Zsigmond P, Persson L, et al. Individual factors associated with neck disability in patients with cervical radiculopathy scheduled for surgery: a study on physical impairments, psychosocial factors, and life style habits. Eur Spine J. 2014;23(3):599–605.
Thoomes EJ, van Geest S, van der Windt DA, Falla D, Verhagen AP, Koes BW, et al. Value of physical tests in diagnosing cervical radiculopathy: a systematic review. Spine J. 2018;18(1):179–89.
Lam KN, Rushton A, Thoomes E, Thoomes-de Graaf M, Heneghan NR, Falla D. Neck pain with radiculopathy: a systematic review of classification systems. Musculoskelet Sci Pract. 2021;54:102389.
Wong JJ, Tricco AC, Cote P, Liang CY, Lewis JA, Bouck Z, et al. Association between depressive symptoms or Depression and Health Outcomes for Low Back Pain: a systematic review and Meta-analysis. J Gen Intern Med. 2022;37(5):1233–46.
Colloca L, Ludman T, Bouhassira D, Baron R, Dickenson AH, Yarnitsky D, et al. Neuropathic pain. Nat Rev Dis Primers. 2017;3:17002.
de Koning EJ, Timmermans EJ, van Schoor NM, Stubbs B, van den Kommer TN, Dennison EM, et al. Within-person Pain Variability and Mental Health in older adults with osteoarthritis: an analysis across 6 european cohorts. J Pain. 2018;19(6):690–8.
Stubbs B, Koyanagi A, Thompson T, Veronese N, Carvalho AF, Solomi M, et al. The epidemiology of back pain and its relationship with depression, psychosis, anxiety, sleep disturbances, and stress sensitivity: data from 43 low- and middle-income countries. Gen Hosp Psychiatry. 2016;43:63–70.
Dario AB, Ferreira ML, Refshauge KM, Lima TS, Ordonana JR, Ferreira PH. The relationship between obesity, low back pain, and lumbar disc degeneration when genetics and the environment are considered: a systematic review of twin studies. Spine J. 2015;15(5):1106–17.
Blanpied PR, Gross AR, Elliott JM, Devaney LL, Clewley D, Walton DM, et al. Neck Pain: Revision 2017. J Orthop Sports Phys Ther. 2017;47(7):A1–A83.
Kirsch Micheletti J, Blafoss R, Sundstrup E, Bay H, Pastre CM, Andersen LL. Association between lifestyle and musculoskeletal pain: cross-sectional study among 10,000 adults from the general working population. BMC Musculoskelet Disord. 2019;20(1):609.
Martinez-Borba V, Ripoll-Server P, Yakobov E, Suso-Ribera C. Predicting the Physical and Mental Health Status of individuals with Chronic Musculoskeletal Pain from a Biopsychosocial Perspective: a Multivariate Approach. Clin J Pain. 2021;37(3):211–8.
Mody GM, Brooks PM. Improving musculoskeletal health: global issues. Best Pract Res Clin Rheumatol. 2012;26(2):237–49.
Ashworth J, Konstantinou K, Dunn KM. Prognostic factors in non-surgically treated sciatica: a systematic review. BMC Musculoskelet Disord. 2011;12:208.
Greenhalgh T, Papoutsi C. Studying complexity in health services research: desperately seeking an overdue paradigm shift. BMC Med. 2018;16(1):95.
Rusoja E, Haynie D, Sievers J, Mustafee N, Nelson F, Reynolds M, et al. Thinking about complexity in health: a systematic review of the key systems thinking and complexity ideas in health. J Eval Clin Pract. 2018;24(3):600–6.
Conradie M, Bester M, Crous L. Psychosocial factors associated with acute cervical radiculopathy. South African J Physiother. 2005;61. https://doi.org/10.4102/sajp.v61i1.166
Falla D, Peolsson A, Peterson G, et al. Perceived pain extent is associated with disability, depression and self-efficacy in individuals with whiplash-associated disorders. Eur J Pain. 2016;20:1490–501.
Simon GE, Revicki D, VonKorff M. Telephone assessment of depression severity. Journal of psychiatric research. 1993 Jul 1;27(3):247 – 52
Breeman S, Cotton S, Fielding S, Jones GT. Normative data for the hospital anxiety and depression scale. Qual Life Res. 2015 Feb;24:391–8.
Tampin B, Slater H, Briffa NK. Neuropathic pain components are common in patients with painful cervical radiculopathy, but not in patients with nonspecific neck-arm pain. The Clinical journal of pain. 2013 Oct 1;29(10):846 – 56.
Dworkin RH, Jensen MP, Gammaitoni AR, Olaleye DO, Galer BS. Symptom profiles differ in patients with neuropathic versus non-neuropathic pain. The journal of pain. 2007 Feb 1;8(2):118 – 26
Acknowledgements
Prof. Lesley Haig for the continued support throughout Michael Mansfield’s PhD programme.
Dr. Brendon Stubbs for his contribution to the review protocol.
School of Sport, Exercise and Rehabilitation Sciences at the University of Birmingham for supporting Michael Mansfield in completing his PhD programme of study.
Funding
Nil funding. This study forms part of Michael Mansfield’s PhD study programme.
Author information
Authors and Affiliations
Contributions
Michael Mansfield conceptualised the project with support from Mick Thacker, Stephanie Jong and Toby Smith.
Michael Mansfield designed the methodology. Toby Smith, Nicolas Spahr, Stephanie Jong, Joseph Taylor, Kirsty Bannister, and Mick Thacker supported the methodology.
Michael Mansfield administrated and managed the project.
Michael Mansfield lead the writing and original draft.
Michael Mansfield, Toby Smith, Nicolas Spahr, Stephanie Jong, Joseph Taylor, Kirsty Bannister, and Mick Thacker all reviewed the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable for this systematic review.
Consent for publication
Not applicable for this systematic review.
Competing interests
There are no conflicts or competing interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mansfield, M., Thacker, M., Taylor, J.L. et al. The association between psychosocial factors and mental health symptoms in cervical spine pain with or without radiculopathy on health outcomes: a systematic review. BMC Musculoskelet Disord 24, 235 (2023). https://doi.org/10.1186/s12891-023-06343-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06343-8