
Abstract
Background
Musculoskeletal pains (MSPs) in sport are cause of poor performances and loss of competition in athletes. The present study aimed at determining the prevalence of MSPs with regard to sport disciplines and athletic status.
Methods
A cross-sectional study was conducted among 320 Senegalese professional and amateur athletes practicing football, basketball, rugby, tennis, athletics, and wrestling. Rates of MSPs in the past year (MSPs-12) and week (MSPs-7d) were assessed using standard questionnaires.
Results
Overall proportions of MSPs-12 and MSPs-7d were 70 and 74.2%, respectively. MSPs-12 were more frequently reported on shoulders (40.6%), neck (37.1%) and hips/thigh (34.4%), while MSPs-7d were predominant on hips/thigh (29.5%), shoulders (25.7%), and upper back (17.2%). Proportions of MSPs-12 and MSPs-7d varied significantly by sport disciplines, with highest values among basketball players. Again, highest MSPs-12 proportions on shoulders (29.7%, P = 0.02), wrists/hands (34.6%, P = 0.001), (40.2%, P = 0.0002), and knees (38.8%, P = 0.002) were seen among basketball players. High proportions of MSPs-7d were seen on shoulders (29.6%, P = 0.04) for tennis players, wrists/hands (29.4%, P = 0.03) for basketball and football players, and hips/thigh (38.8%, P < 0.00001) for basketball players. Football players had reduced risk of MSPs-12 by 75% on lower back (OR = 0.25; 95% CI. 0.10—0.63; P = 0.003) and by 72% on knees (OR = 0.28; 95% CI. 0.08—0. 95; P = 0.04). In contrast, tennis players were more at risk of MSPs-12 on shoulders (OR = 3.14; 95% CI. 1.14–8.68; P = 0.02), wrists/hands (OR = 5.18; 95% CI.1.40–11.13; P = 0.01), and hips/thigh (OR = 2.90; 95% CI. 1.1–8.38; P = 0.04). Professionals were protected from MSPs-12 on neck pain with a significant reduction of risk by 61% (OR = 0.39, 95% CI. 0.21–0.75, P = 0.03).
Conclusion
MSPs are a reality among athletes and their risk is modulated by sport disciplines, athletic status and gender.
Similar content being viewed by others


Background
Sport in competitions and its challenges are a catalysts of economic development in developing countries [1]. In amateur and professional athletes, training during preparation is essential for national/international competitions. This training also allows for assessing performances, profiling athletic talent, identifying ability to compete, and identifying weakness and factors determining performances [2].
Athletes, during performance optimization phase, face challenges that expose them to musculoskeletal pains (MSPs) which are sometimes associated with injury. MSP is frequently observed in athletes and is often cause of poor biomechanical performances and even loss of competition. It can also lead to significant recovery periods requiring physiotherapy or surgery [3, 4]. MSPs are a common problem and important warning signals of overuse injury in athletes [5, 6].
MSPs are diagnosed on several body parts of athletes including joints, ligaments, tendons, nerves, muscles, and structures that support limbs, neck and back. Causes of MSPs in athletes are multiple with diverse origin such as repetition of same movement, awkward posture, and host related genetic factors [7,8,9]. In sports medicine, primary and secondary prevention of MSPs and injuries are particularly challenging in sports medicine constitutes one of the most worrying health problems in athletic world because of their high economic costs, withdrawal of athletes from training and competition, and impaired performances [10, 11]. It is known that physical activity and sport may contribute to prevent MSPs via triggering endorphins production which will result in reduction in inflammation and pain [12,13,14]. Also, previous studies showed that moderate physical exercises were associated with sustained muscular activity and improved function of joints associated [15].
MSPs in athletes are persistent reality in various disciplines such as wrestling [16], handball [17], rugby [18], soccer [19], tennis, track and field [20], and basket-ball [21], and are cause of disability [6, 21,22,23] and vary by athletic status [24]. In sub-Saharan Africa there is lack of studies on MSPs in various sport disciplines according to athletic status. This preliminary study was therefore conducted to determine the prevalence of MPSs and associated factors in Senegalese athletes with varying athletic status and different disciplines.
Methods
Study design and participants
This was a cross-sectional prospective and analytical study conducted for four months (January-April 2021) in Dakar, Senegal. Participants were recruited at professional and amateur clubs, and were participating regularly to national and international competitions of different sport disciplines (football, basket-ball, rugby, tennis, athletics, and traditional wrestling).. These disciplines were chosen given their great popularity in Senegal. We excluded athletes recovering from musculoskeletal trauma, and under rehabilitation or physiotherapy interventions.
Sampling
The minimum sample size was computed using the Lorentz’s formula: N = p (1-p) z2/d2, where N is the minimum sample size; p (= 94%) is the prevalence in the last one year of low back pain reported among athletes by Farahbakhsh et al. [23]; z is statistic for the desired confidence level (z = 1.96 for confidence at 95%) and d the accepted margin of error (d = 0.05). Thus, the minimal sample size found was 87 participants. Finally, a total of 320 athletes was included.
Ethics
Aims and objectives of the study were first explained to administration staff of athlete clubs and coaches. After obtaining administrative authorization, the study was explained to athletes. An informed and signed consent was obtained from each athlete willing to participate in the study, and they were free to withdraw from study at any time. The study was approved by ethics committee of Cheikh Anta Diop University of Dakar, Senegal (015/2021/CER/UCAD), and conducted as per recommendations of the Declaration of Helsinki revised in 1989.
Data collection
A structured questionnaire was administered to each participant to socio-demographic and anthropometric data (age, gender, history of injuries), and socio-professional information (discipline, number of training session/ week).
Anthropometric parameters
Height was measured using a rod graduated to the nearest centimeter while weight was measured using an electronic scale Tanita BC-532 (Tokyo, Japan). Body mass index (BMI) was determined using Quetelet's formula: BMI (Kg.m−2) = Weight (kg) / height2 (m2).
Musculoskeletal pains
A modified Nordic questionnaire [24] adapted to athletes was used to determine MSPs prevalence. This questionnaire focuses on occurrence of MSPs on nine body regions (neck, shoulders, elbows, wrists/hands, upper back, lower back, hips/thighs, knees, ankles/feet) during last 12 months or 7 days after a competition or training session. For each body region.
Parameters evaluated were:
-
Presence or absence of aches, pains or discomfort during the last 12 months and / or the last seven days,
-
Bad performance due to joint pains,
-
Absenteeism during training sessions or competitions during the last 12 months and/or the last seven days owing to pain on at least one body region,
-
History of trauma one at least one body region during training sessions or competitions.
Therefore:
-
A year/12-month MSPs (MSPs-12) was considered present if self-reported ache, pain or discomfort on above mentioned body regions during the last 12 months was reported.
-
A week/7-day MSPs (MSPs-7d) was defined as seven-day prevalence of MSPs.
-
Pain reported on a former injuries regions was not considered as MSPs.
Statistical analysis
Quantitative and qualitative variables were expressed as means ± standard deviation and percentage (%) respectively. Unpaired Student's t-test was used to compare unpaired quantitative variables. Normality of data was evaluated using Kolmogorov–Smirnov test. The Pearson’s chi-square (χ2) test was performed to compare unpaired proportions. Logistic regression models were performed to identify factors associated with MSPs. The association between MSP and independent variables was quantified through computing crude and adjusted odd ratio (cOR and aOR), confidence interval at 95% (95%CI), and level of significance. Statistical analyses were conducted using StatView 5.0 (SAS Institute, Inc., Chicago, USA) software. Statistical significance was set at P < 0.05.
Results
The majority of athletes included in the study were males (69.7%). Football and basket-ball were predominant sport disciplines with proportion of 28.1 and 25%, respectively. More than half participants (64.1%) were amateurs. According to gender, the proportion of males was higher than that of females in all sport disciplines (P < 0.0001). On average, females were older than their male counterparts (P < 0.0001). Anthropometric parameters including height and weight were higher in males compared to females (P < 0.0001) (Table 1). According to athletic status, amateur athletes of the study were more (P < 0.0001) into basketball (51.2%), soccer (54.4%), rugby (100%), tennis (100%). On the staturo-ponderal plan, the amateurs were more (P = 0.03) height, on the other hand the number of training of the professionals was higher than (P < 0.0001) that of the amateurs.
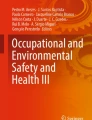
Proportions of MSPs-12 and MSPs-7d by sport disciplines, athletic status, and gender are illustrated on Fig. 1. Overall proportion of MSPs-12 and MSPs-7d was 70% (95%CI. 64.8–74.8%) and 32.8% (95%CI. 27.9–38.1%), respectively. Also, proportions of MSPs-12 and MSPs-7d were higher in males and professional athletes. For instance, proportion of MSPs-12 was 67.9% in males compared to 31.2% in females (Fig. 1). However, no statistically significant difference was found in MSPs-12 and MSPs-7d proportions with respect to gender and athletic status.

Prevalence of MSPs according to gender and Athletic status. MSPs-12: prevalence of musculoskeletal pains during the 12 last months; MSPs-7d: prevalence of musculoskeletal pains during the seven last days
MSPs-12 was more frequently reported on shoulders (40.6% [95%CI.34.4–47.2%]), followed by neck (37.1% [95%CI.31.0–43.5%]), and hips/thigh (34.4% [95%CI.28.5–40.8%]) (Fig. 2). MSPs-7d were more frequent on hips/thigh (29.5% [95%CI.21.6–38.8%]), followed by shoulders (25.7% [95%CI.18.3–34.8%]), and upper back (17.2% [95%CI.11.1–25.5%]).

Prevalence of MSPs according to body regions. MSPs-12: prevalence of musculoskeletal pains during the 12 last months; MSPs-7d: prevalence of musculoskeletal pains during the seven last days
Proportions of MSPs-12 and MSPs-7d were significantly highest in basketball players with values of 29.5 and 30.5%, respectively. No statistically significant difference of MSPs-12 and MSPs-7d proportion was noted between athletic status (Table 2). Upon stratifying analysis by body regions, we observed that proportion of MSPs-12 was still highest in basketball players on shoulders (29.7%, P = 0.02), wrists/hands (34.6%, P = 0.001), (40.2%, P = 0.0002), and knees (38.8%, P = 0.002). In contrast, proportion of MSPs-12 was higher in tennis players on shoulders (36.4%, P = 0.002) (Table 2). Results were a bit contrasted for MSPs-7d, with higher proportions found on shoulders (29.6%, P = 0.04) for tennis players, wrists/hands (29.4%, P = 0.03) for basketball and football players, and hips/thigh (38.8%, P < 0.00001) for basketball players.
Multivariate analysis, presented in Table 3, showed a significant reduction of MSPs-12 risk by 66% in football players compared to athletics (OR = 0.34; 95% CI. 0.14—0.83; P = 0.01). Again, football players had reduced risk of MSPs-12 on lower back (OR = 0.25; 95% CI. 0.10—0.63; P = 0.003) and on knees (OR = 0.28; 95% CI. 0.08—0. 95; P = 0.04), compared to those practicing athletics. In contrast, tennis players were more at risk of MSPs-12 on shoulders (OR = 3.14; 95% CI. 1.14–8.68; P = 0.02), wrists/hands (OR = 5.18; 95% CI.1.40–11.13; P = 0.01), and hips/thigh (OR = 2.90; 95% CI. 1.1–8.38; P = 0.04). Professional athletes were protected from MSPs-12 on neck pain, with a significant risk reduction by 61% (OR = 0.39, 95% CI. 0.21–0.75, P = 0.03).
Tennis players had a threefold higher overall risk of MSPs-7d (OR = 3.20; 95% CI. 1.20–8.54; P = 0.02) compared to those practicing athletics. Irrespective of body region, wrestlers had a ~ fourfold higher risk of MSPs-7d in wrist/hand (OR = 3.60; 95% CI. 1.87–7.58; P = 0.01) and ~ sixfold higher on shoulders (OR = 5.93; 95% CI. 1.16–11.58; P = 0.03), compared to those practicing athletics.
Depending on athletic status among amateurs, odds of MSPs-12 on lower back were more than two times higher (OR = 2.43; 95% CI. 1.10–5.39; P = 0.02) in males when compared to their female counterparts. Then, compared to track and field athletes, footballers were protected from MSPs-12 on lower back (OR = 0.10; 95% CI. 0.01–0.96; P = 0.04) and knees (OR = 0.20; 95% CI. 0.05–0.94; P = 0.04), whereas tennis players had a high risk of MSPs-7d on wrists/hands (OR = 9.45; 95% CI. 1.20–12.16; P = 0.003). Risk of MSPs-7d lower back was significantly reduced by 89% in footballers (OR = 0.11; 95% CI 0.01–0.96; P = 0.04) compared to those practicing athletics.
Among professional athletes, the odds of MSPs-12 on hips/thigh region were four times higher (OR = 4.20; 95% CI. 1.18–9.47; P = 0.02) in basketball players, but footballers were protected by 83% from MSPs on lower back (OR = 0.17; 95% CI. 0.04–0.74; P = 0.01), compared with athletic runners.
Discussion
This study was designed to evaluate the prevalence of MSPs among Senegalese athletes according to sport disciplines and athletic status.
Overall prevalence rates of MSPs-12 and MSPs-7d were 70 and 32.8%, respectively. There are few studies assessing MSPs on all the nine body regions in different sports, most of them being focalized on one or two body regions [25,26,27,28,29]. These findings are not consistent with those reported by Oliveira et al. [28] respective values of 54.2 and 43.5% among Brazilian adolescent amateurs practicing multiple sport disciplines (i.e., basketball, handball, judo, swimming, volleyball). Other studies reported higher values in Germany (MSPs-12 = 81.1%, MSPs-7d = 49%) and Norway (MSPs-7d = 84%) [25, 30]. A recent study by Owoeye et al. [28] reported MSPs-12 estimate of 26% in apparently healthy collegiate practicing soccer and basketball. Moreover, Goes et al. [29] found a prevalence of pain on joints (tendinopathy) of 30.3% in elite athletes from five disciplines (rugby, soccer, combat sports, handball, and water polo).
Pain was more frequently found in males compared to females, and this is not consistent with findings from earlier reports [25, 30]. Higher rates of pain in female athletes would be related to their earlier maturity associated with hormonal discrimination [31]. Also, anatomical features in females could be additional risk factors of of pains [31]. In addition, as reported by Shan et al. [32] that males have a higher pain threshold than females could also justify higher rates of MSPs in females.
We reported higher rates of MSPs-12 on shoulders and hips/thigh regardless of sport discipline. Such results were reported previously in Brazil [27] in adolescents amateur athletes (basketball, handball, judo, swimming, volleyball) where authors found MSPs-12 and MSPs-7d rates on shoulders of 43.5 and 54.2%, respectively. These values are higher than 21.4% for MSPs-7d and 38.8% for MSPs-12 reported by Mohseni-Bandpei et al. [33] in Iranian athletes (swimming, rowing, wrestling, basketball, volleyball, and handball). Our findings contrast with those from several studies where MSPs-12 were predominantly seen on neck [25, 30, 34] and lower back [21, 25, 28].
Likewise, our prevalence of shoulders pain is superior to that of highlighted in an epidemiological cross-sectional study carried out among 613 Iranian overhead sports athletes in different collegiate sport fields ( swimming, rowing, wrestling, basketball, volleyball, and handball) where Mohseni-Bandpei et al. [33] reported MSPs-7d and MSPs-12 of 21.4, and 38.8% respectively. It should be noted that shoulder pain is a major performance limiting factor in aerobic and anaerobic sports requiring repeated overhead movements placed heavy loads on the dominant shoulder. In Canada, Harmath et al. [35] found MSPs-7d prevalence of 41.9% on shoulder during a study on shoulder pain and performance limitation in competitive tennis players. For some authors, joint changes in athletes are cause of acute adaptations of bones and muscles, which lead to negative impact on the range of motion of shoulders, while associated internal rotation deficits would increase the risks of shoulder pain [27, 36,37,38,39]. According to the anatomical justification, shoulder pain and injuries would be due to this internal rotation deficit, commonly kwon as ‘’glenohumeral internal rotation deficit’’ which have been recognized as joint adaptations to the practice of sports activities [39, 40]. Moreover, it is known that sport practice can lead to capsular stiffness and limit internal rotation of the glenohumeral, and thus, increase the risk of chronic pains or injuries on shoulders [37, 41].
Prevalence of MSPs varied significantly by sport disciplines, with higher values in basketball, football and tennis. Analyzing back pains in German elite athletes, Fett et al. [25] found similar results to those in the present study. Football and basketball are team sports and contact with high physiological and biomechanics demands. Both disciplines demand high level of aerobic and anaerobic capacities along with integration of physical characteristics. Frequent jumping, landing and changes in direction make up much of physical load of competitive games, which therefore, expose players to high level of eccentric muscle contractions and joints solicitations [42, 43]. Again, the intermittent aspect of basket-ball, football and tennis implies postural deviations and sudden changes in speed which are common to these three sports; and well considered as an important key factor on occurrence of pains and injuries on observed body regions [44,45,46]. Additional reasons of more frequent pains in basketball could be specific anthropometric demands such as height and weight which impact positively performances and increase the risk of pain and injuries [47, 48].
According to body articulations, MSPs were more frequent on shoulders, wrists/hands, hips/thigh, knees in basketball, and on elbows, shoulders in tennis. In tennis players, high prevalence of pain was found on shoulders and elbows which is in line with previous studies. Sport disciplines such as tennis, also termed as intermittent sport disciplines, imply repeated overhead motions that place important loads on dominant shoulder, and then, result in pain on this body region [49, 50]. Besides, pain on elbow is the most common cause of lateral sided in tennis, and 50% of tennis players will get an episode of follow-up-requiring pain of elbows during their career [51, 52].
The prevalence of MSPs-12 was higher in amateurs compared to that seen in professionals. This finding does not support that reported by Hoskins et al. [53] who found higher prevalence of lower back pain in Australian semi-elite athletes compared to their elite counterparts. This result could also be related to training techniques given fact that physical and psychological demands of professional athletes during competitions are thought to be higher than those of amateurs.
Multivariate logistic regression analysis revealed significant association between risk of MSP in body regions and some athletes’ characteristics (athletic status, gender, and sport discipline). Regardless of athletic status, overall risk of MSPs on shoulders, wrist/hands, and hips/thigh was higher in tennis players compared to those practicing athletics. Tennis players had higher risk of MSPs irrespective of body regions. This variability in MSPs risk is likely due to existing correlation between hyperflexion motion and incidence joints pains in athletes. Furthermore, there is a strong relationship between flexion and excessive stretching of certain musculoskeletal joints and occurrence of pain or discomfort. Thus, stress-related mechanical pressure on non-contractile tissue are sufficient to stimulate musculoskeletal pain receptors according to intermittent or continuous flexion on some joints as those of the lumbar spine [7]. To all justification, we could associate the glenohumeral internal rotation deficit on shoulders as additional explanation of this result [37, 39,40,41].
It is well known that MSPs incidence, prevalence, causes and risks are strongly dependent on sport modality [29, 44, 54,55,56]. Biomechanical and physiological demands of the musculoskeletal system following the increase in training loads, techniques in relation to athletic status in some sports disciplines before chronic adaptations could to be the main cause of pain reported within the week or in a year. Zemková et al. [57] identified that fatigue of the trunk muscles, induced by excessive loading of musculoskeletal system, is one of main sources of pain in athletes. To this regard, some studies on pain in sports have highlighted that factors, such as high training volume, repetitive motions, high physical loads, repetitive mechanical strain and extreme body(spine) positions, might be responsible for variation in risk of pain and injuries on body regions [7, 25, 58]. Nevertheless, athletes practicing discipline such as basketball, tennis and wrestling face important biomechanical, physiological demands, morphological requirements, and more positional solicitations of some joint regions of during training sessions and competitions, that can reduce or increase the risk of MSPs.
Conclusion
In conclusion, this study pointed out high prevalence of MSPs-12 and MSPs-7d in athletes. Depending on body region, prevalence of MSPs varied significantly by sport disciplines, gender, and athletic status. Also, these three variables were associated either with decreased or increased risk of MSPs on a specific body region specific of athletes, especially in tennis and football players. The occurrence of MSPs impacted negatively performances of athletes and their health via increased exposure to injuries. There is urgent need to prevent MSPs in sub-Saharan African athletes to optimize their biomechanical performances and guarantee their wellbeing.
Limitations
Comparability of findings from this study is limited given that prevalence of MSPs varies according to questionnaire used, most studies use self-report questionnaires with a special characterization of pain and perception. In addition, small sample sizes for some disciplines could constitute a bias. Further studies on sub-Saharan athletes should take into account age, weekly training volume, quality of life and sleep, which are important factors involved in occurrence of MSPs.
Availability of data and materials
Data can be shared upon contact with the correspondence author.
References
Acquah-sam E. Developing sports for economic growth and development in developing countries. ESJ. 2021;172–216. https://doi.org/10.19044/esj.2021.v17n15p172.
Bangsbo J, Mohr M, Poulsen AH, Pérez-Gómez J, Krustrup P. Training and testing the elite athlete. J Exerc Sci Fit. 2006;4:1–14.
Kerr ZY, Cortes N, Ambegaonkar JP, Caswell AM, Prebble M, Romm K, et al. The Epidemiology of injuries in Middle School Football, 2015–2017: the advancing healthcare initiatives for underserved students project. Am J Sports Med. 2019;47(4):933–41.
Kiliç Ö, Aoki H, Goedhart E, Hägglund M, Kerkhoffs GMMJ, Kuijer PPFM, et al. Severe musculoskeletal time-loss injuries and symptoms of common mental disorders in professional soccer: a longitudinal analysis of 12-month follow-up data. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):946–54.
Ball JR, Harris CB, Lee J, Vives MJ. Lumbar spine injuries in sports: review of the literature and current treatment recommendations. Sport Med. 2019;5(1):26.
Yabe Y, Hagiwara Y, Sekiguchi T, Momma H, Tsuchiya M, Kanazawa K, et al. High prevalence of low back pain among young basketball players with lower extremity pain: a cross-sectional study. BMC Sport Sci Med Rehabil. 2020;12:40.
Howell DW. Musculoskeletal profile and incidence of musculoskeletal injuries in lightweight women rowers. Am J Sports Med. 1984;12(4):278–82.
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021.
Salles JI, Lopes LR, Eugenia M, Duarte L, Morrissey D, Martins MB, et al. increases the risk of tendinopathy in volleyball athletes : a case control study. BMC Med Genet. 2018;19(1):119.
Lisman PJ, de la Motte SJ, Gribbin TC, Jaffin DP, Murphy K, Deuster PA. A systematic review of the association between physical fitness and musculoskeletal injury risk: part 1-cardiorespiratory endurance. J strength Cond Res. 2017;31(6):1744–57.
Zaremski JL, Diamond MC, Aagesen A, Casey E, Davis B, Ellen M, et al. Musculoskeletal and sports medicine physical medicine and rehabilitation curriculum guidelines. PM R. 2017;9:1244–67.
Harber VJ, Sutton JR. Endorphins and exercise. Sports Med. 1984;1(2):154–71.
Schwarz L, Kindermann W. Changes in beta-endorphin levels in response to aerobic and anaerobic exercise. Sports Med. 1992;13(1):25–36.
Scheef L, Jankowski J, Daamen M, Weyer G, Klingenberg M, Renner J, et al. An fMRI study on the acute effects of exercise on pain processing in trained athletes. Pain. 2012;153(8):1702–14.
Morken T, Magerøy N, Moen BE. Physical activity is associated with a low prevalence of musculoskeletal disorders in the Royal Norwegian Navy: a cross sectional study. BMC Musculoskelet Disord. 2007;8(1):56.
Baranto A. Back pain and MRI changes in the thoraco-lumbar spine of top athletes in four different sports : a 15-year follow-up study Back pain and MRI changes in the thoraco-lumbar spine of top athletes in four different sports : a 15-year follow-up study. Knee Surg Sports Traumatol Arthrosc. 2009;17:1125–34.
Tunås P, Nilstad A, Myklebust G. Low back pain in female elite football and handball players compared with an active control group. Knee Surgery Sport Traumatol Arthrosc. 2014;23:2540–7.
Iwamoto J, Abe H, Tsukimura Y, Wakano K. Relationship between radiographic abnormalities of lumbar spine and incidence of low back pain in high school rugby players: a prospective study. Scand J Med Sci Sports. 2005;15(3):163–8.
Brynhildsen J, Lennartsson H, Klemetz M, Dahlquist P, Hedin B, Hammar M. Oral contraceptive use among female elite athletes and age-matched controls and its relation to low back pain. Acta Obstet Gynecol Scand. 1997;76(9):873–8.
Lively MW. Prevalence of pre-existing recurrent low back pain in college athletes. W V Med J. 2002;98(5):202–4.
Cristina S, Borges DC, Valadão S, Rayanne P, Azevedo VD, Márcia R, et al. Musculoskeletal disorders in basketball players and associated factors : a systematic review protocol with meta- analysis [version 1; peer review : awaiting peer review ]. F1000Research. 2021;10:557.
Trompeter K, Fett D, Platen P. Prevalence of back pain in sports: a systematic review of the literature. Sports Med. 2017;47(6):1183–207.
Farahbakhsh F, Rostami M, Noormohammadpour P, Mehraki Zade A, Hassanmirazaei B, Faghih Jouibari M, et al. Prevalence of low back pain among athletes: a systematic review. J Back Musculoskelet Rehabil. 2018;31(5):901–16.
Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–7.
Fett D, Trompeter K, Platen P. Back pain in elite sports: a cross-sectional study on 1114 athletes. PLoS ONE. 2017;12(6): e0180130.
Villavicencio AT, Burneikiene S, Hernández TD, Thramann J. Back and neck pain in triathletes. J Neurosurg Spine. 2007;7:408–13. https://doi.org/10.3171/foc.2006.21.4.8.
de Oliveira VMA, Pitangui ACR, Gomes MRA, da Silva HA, Dos PMHP, de Araújo RC. Shoulder pain in adolescent athletes: prevalence, associated factors and its influence on upper limb function. Brazilian J Phys Ther. 2017;21(2):107–13.
Owoeye OBA, Neme JR, Buchanan P, Esposito F, Breitbach AP. Absence of injury is not absence of pain: prevalence of preseason musculoskeletal pain and associated factors in Collegiate soccer and basketball student athletes. Int J Environ Res Public Health. 2022;19(15):9128. https://doi.org/10.3390/ijerph19159128.
Goes RA, Lopes LR, Rodrigues V, Cossich A, Almeida V, De MR, et al. Musculoskeletal injuries in athletes from five modalities: a cross-sectional study. BMC Musculoskelet Disord. 2020;21(1):122. https://doi.org/10.1186/s12891-020-3141-8.
Guddal MH, Stensland SØ, Johnsen MB. Physical activity level and sport participation in relation to musculoskeletal pain in a population-based study of adolescents the young-HUNT study. Orthop J Sports Med. 2017;5(1):2325967116685543.
Shehab DK, Al-Jarallah KF. Nonspecific low-back pain in Kuwaiti children and adolescents: associated factors. J Adolesc Health. 2005;36(1):32–5.
Shan Z, Deng G, Li J, Li Y, Zhang Y, Zhao Q. Correlational analysis of neck/shoulder pain and low back pain with the use of digital products, physical activity and psychological status among adolescents in Shanghai. PLoS ONE. 2013;8(10):e78109.
Mohseni-Bandpei MA, Keshavarz R, Minoonejhad H, Mohsenifar H, Shakeri H. Shoulder pain in Iranian elite athletes: the prevalence and risk factors. J Manipulative Physiol Ther. 2012;35(7):541–8.
Legault ÉP, Descarreaux M, Cantin V. Musculoskeletal symptoms in an adolescent athlete population: a comparative study. BMC Musculoskelet Disord. 2015;16:210.
Harmath D, Côté P. The one-week prevalence of overuse-related shoulder pain and activity limitation in competitive tennis players living in Toronto : a feasibility study. J Can Chiropr Assoc. 2022;66(1):33–42.
Guney H, Harput G, Colakoglu F, Baltaci G. The effect of Glenohumeral internal-rotation deficit on functional rotator-strength ratio in adolescent overhead athletes. J Sport Rehabil. 2016;25(1):52–7.
Astolfi MM, Struminger AH, Royer TD, Kaminski TW, Swanik CB. Adaptations of the shoulder to overhead throwing in youth athletes. J Athl Train. 2015;50(7):726–32.
Cools AM, Johansson FR, Borms D, Maenhout A. Prevention of shoulder injuries in overhead athletes: a science-based approach. Brazilian J Phys Ther. 2015;19(5):331–9.
Leonard J, Hutchinson MR. Shoulder injuries in skeletally immature throwers: review and current thoughts. Br J Sports Med. 2010;44(5):306–10.
Pocecco E, Ruedl G, Stankovic N, Sterkowicz S, Del Vecchio FB, Gutiérrez-García C, et al. Injuries in judo: a systematic literature review including suggestions for prevention. Br J Sports Med. 2013;47(18):1139–43.
Wilk KE, Macrina LC, Fleisig GS, Porterfield R, Simpson CD 2nd, Harker P, et al. Correlation of glenohumeral internal rotation deficit and total rotational motion to shoulder injuries in professional baseball pitchers. Am J Sports Med. 2011;39(2):329–35.
Jacoby L, Yi-Meng Y, Kocher MS. Hip problems and arthroscopy: adolescent hip as it relates to sports. Clin Sports Med. 2011;30(2):435–51.
van Beijsterveldt AMC, van de Port IGL, Krist MR, Schmikli SL, Stubbe JH, Frederiks JE, et al. Effectiveness of an injury prevention programme for adult male amateur soccer players: a cluster-randomised controlled trial. Br J Sports Med. 2012;46(16):1114–8.
Candela V, De CA, Giuseppe U, Salvatore G, Denaro V. Hip and Groin Pain in Soccer Players. Joints. 2021;7(4):182–7. https://doi.org/10.1055/s-0041-1730978.
Makino T, Kaito T, Sakai Y, Takenaka S, Yoshikawa H. Health-related quality of life and postural changes of spinal alignment in female adolescents associated with back pain in adolescent idiopathic scoliosis: a prospective cross-sectional study. Spine (Phila Pa 1976). 2019;44(14):833–40.
Kerbel YE, Smith CM, Prodromo JP, Nzeogu MI, Mulcahey MK. Epidemiology of hip and groin injuries in Collegiate athletes in the United States. Orthop J Sports Med. 2018;6(5):2325967118771676. https://doi.org/10.1177/2325967118771676.
Cui Y, Liu F, Bao D, Liu H, Zhang S, Gómez M-Á. Key anthropometric and physical determinants for different playing positions during national basketball association draft combine test. Front Psychol. 2019;10:2359.
Okonkwo CA, Okereke EC, Onuwa J, Ibikunle PO, Egwuonwu V, et al. Pattern of musculoskeletal injuries amongst male amateur basketball players in Anambra State. Nigeria Int J Sports Exerc Med. 2022;8:212. https://doi.org/10.23937/2469-5718/1510212.
Elliott B, Fleisig G, Nicholls R, Escamilia R. Technique effects on upper limb loading in the tennis serve. J Sci Med Sport. 2003;6(1):76–87.
Reid M, Elliott B, Alderson J. Shoulder joint loading in the high performance flat and kick tennis serves. Br J Sports Med. 2007;41(12):884–9.
Pluim BM, Fuller CW, Batt ME, Chase L, Hainline B, Miller S, et al. Consensus statement on epidemiological studies of medical conditions in tennis, April 2009. Clin J Sport Med. 2009;19(6):445–50. https://doi.org/10.1097/JSM.0b013e3181be35e5.
Keijsers R, de Vos R-J, Kuijer PPF, van den Bekerom MP, van der Woude H-J, Eygendaal D. Tennis elbow. Shoulder Elb. 2019;11(5):384–92.
Hoskins W, Pollard H, Daff C, Odell A, Garbutt P, McHardy A, et al. Low back pain status in elite and semi-elite Australian football codes: a cross-sectional survey of football (soccer), Australian rules, rugby league, rugby union and non-athletic controls. BMC Musculoskelet Disord. 2009;10:38.
Junge A, Langevoort G, Pipe A, Peytavin A, Wong F, Mountjoy M, et al. Injuries in team sport tournaments during the 2004 Olympic Games. Am J Sports Med. 2006;34(4):565–76.
Dönmez G, Korkusuz F, Özçakar L, Karanfil Y, Dursun E, Kudaş S, et al. Injuries among recreational football players: results of a prospective cohort study. Clin J Sport Med. 2018;28(3):249–54. https://doi.org/10.1097/JSM.0000000000000425.
Bromley SJ, Drew MK, Talpey S, McIntosh AS, Finch CF. A systematic review of prospective epidemiological research into injury and illness in Olympic combat sport. Br J Sports Med. 2018;52(1):8–16.
Zemková E, Kováčiková Z, Zapletalová L. Is there a relationship between workload and occurrence of back pain and back injuries in athletes? Front Physiol. 2020;11:894.
Belavý DL, Albracht K, Bruggemann G-P, Vergroesen PPA, van Dieën JH. Can Exercise Positively Influence the Intervertebral Disc? Sports Med. 2016;46(4):473–85.
Acknowledgements
Authors thank sports coaches (coaches and physical trainers) and administrative staff of amateur and professional clubs for the support. We also extend our acknowledgments to all athletes who accepted to participate in this study.
Funding
No
Author information
Authors and Affiliations
Contributions
Hassane Ahmet Malam Moussa collected data and interpreted results, Jerson Mekoulou Ndongo performed the data analysis, interpreted results and drafted the manuscript. Elysée Claude Bika Lele, Mbang Biang Wiliam, Ahmadou drafted the manuscript, Loick Pradel Foko Kojom, Caroline Dupré performed data analysis, proofread English language, and revised manuscript for important intellectual content. Wiliam Richard Guessogo, Peguy Brice Assomo-Ndemba drafted the manuscript; collected data. Clarisse Noel Ayina, Nathalie Barth, Jessica Guyot, Bienvenu Bongue critical revision of the manuscript for important intellectual. Abdoulaye SAMB, Abdoulaye BA and Mandengue Samuel Honoré supervised the study at all stages. All authors read and approved final version of paper before submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by ethics committee of Cheikh Anta Diop University of Dakar, Senegal (015/2021/CER/UCAD) in accordance with relevant guidelines of the declaration of Helsinki, informed and signed consent was obtained from all participants.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Malam Moussa Ahmet, H., Bika Lele, E.C., Guessogo, W.R. et al. Musculoskeletal pains among amateur and professional athletes of five disciplines in Senegal: a preliminary study. BMC Musculoskelet Disord 24, 210 (2023). https://doi.org/10.1186/s12891-023-06275-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06275-3