
Abstract
Background
Low back pain is a very common symptom frequently characterized as a biopsychosocial problem. This study aims to investigate the effectiveness of education to keep the abdomen relaxed versus contracted during Pilates exercises in patients with primary chronic low back pain.
Methods
Two-group randomised controlled trial with allocation of parallel groups and intention-to-treat-analysis. This study will be conducted in Lavras, MG, Brazil. A total of 152 participants will be randomised into two groups that will be treated with Pilates exercises for 12 weeks (twice a week for 60 minutes). Recruitment began in May 2022. The control group will receive guidance on the specific activation of the center of strength (the powerhouse), while the experimental group will receive guidance to perform the exercises in a relaxed and smooth way. Primary outcomes will be pain intensity (Numeric Pain Rating Scale) and disability (Rolland-Morris Questionnaire) 12 weeks post randomisation. Secondary outcomes will be global improvement (Perception of Global Effect Scale) and specific functionality (Patient-specific Functional Scale). The outcomes will be analyzed using repeated-measure linear mixed models. The assessors were not considered blinded because the participants were not blinded, and outcomes were self-reported.
Discussion
The findings of this study will help in clinical decision-making concerning the need to demand abdominal contraction during the exercises, understanding if it’s a fundamental component for the effectiveness of the Pilates method for this population.
Trial registration
This trial was prospectively registered in the Clinical Trials (NCT05336500) in April 2022.
Similar content being viewed by others

Background
Low back pain is a very common symptom and the causes of its onset and its specific sources of nociception are rarely identified [1]. It is characterized often as a biopsychosocial problem associated with the experience of pain and disability, covering a range of factors that include biophysical, psychological, and social dimensions. Low back pain impairs social function and participation, in addition to personal financial prosperity, since additional costs are associated with chronic conditions [2]. There is a need to reduce unnecessary and even harmful health care, and most importantly, to promote an active lifestyle and adopting healthier habits [3].
The Pilates method is an important component in the treatment of primary chronic low back pain [4,5,6]. Hayden et al. (2021) conducted a systematic review evaluating the impact of exercise treatment on pain and functional limitations in adults with chronic nonspecific low back pain. They emphasized Pilates as one of several effective methods when compared to no treatment, placebo or usual care [7]. In patients with chronic low back pain, the beneficial effects of Pilates have been observed within 12 weeks, mainly in reducing pain and improving function. Sessions are recommended to last around 60 minutes, with a frequency of two and three times a week, supervised by certified physical therapists [8]. It is important that the exercises include isometric strengthening, global stretching, breathing, and proper positioning of the spine, promoting greater body awareness [9].
Pilates is an effective exercise method for rehabilitation of musculoskeletal disorders, as its principles are based on the activation of local muscles [10]. Specifically in chronic low back pain, clinical trials conducted using exercise protocols based on the principles of the method demonstrate its effectiveness [11,12,13,14,15]. In this sense, motor control of the lumbar spine and maintenance of adequate body posture during the execution of each Pilates exercise is relevant [16].
The real importance of activating muscles such as transversus abdominis and multifidus in chronic musculoskeletal pain conditions is still debatable [17, 18]. Contrary to the fact that muscular components of the trunk influence body stabilization, voluntary activation of the abdominal bracing can limit movements and increase mechanical stress, resulting in greater energy consumption [18, 19]. In patients with chronic low back pain, the transversus abdominis muscle appears to show no delay during activation [17]. Furthermore, multifidus activity can be modified independently of abdominal bracing activation [18]. Individuals with chronic low back pain exhibit higher global trunk muscle activity (multifidus, erector spinae, external oblique, and rectus abdominus )[20]. Interestingly, symptomatic individuals have increased erector spinae muscle activity (longissimus, iliocostalis, and multifidus) during the performance of functional tasks, contradicting the idea of stimulating the muscle activity [21]. Interestingly, patients with chronic low back pain have increased erector spinae muscle activity (longissimus, iliocostalis, and multifidus) during the performance of functional tasks, contradicting the idea of stimulating the muscle activity on these patients [21].
Consequently, a question arises about the need to encourage abdominal muscles contraction instead of relaxation during the performance of Pilates method exercises for the treatment of chronic low back pain. Therefore, the primary objective of this study is to investigate the effectiveness of education to keep the abdomen relaxed compared to contracted during Pilates exercises in reducing pain and disability in patients with primary chronic low back pain 12 weeks after randomisation.
Methods and design
Design and setting
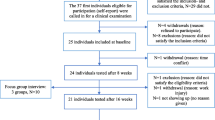
The protocol was written according to the SPIRIT statement (Fig. 1), increasing its transparency and completeness [22]. The findings will be reported following the CONSORT statement [23] and the TIDieR checklist [24]. This study is a research protocol for a two-group randomised controlled trial with parallel-group allocation and intention-to-treat analysis (Fig. 2). The study will be conducted in Lavras, MG (Brazil).

Content for the schedule of enrolment, interventions, and assessments (SPIRIT 2013)

Study flowchart
Recruitment and participants
We will screen patients of both sexes with primary chronic low back pain with symptoms for at least 12 weeks and who have not had an episode of worsening pain in the last 6 weeks (Table 1). Initially, participants will be evaluated by a physical therapist who is blinded to the allocation of intervention groups, confirming their eligibility according to the inclusion and exclusion criteria (Table 2). This screening will involve the survey of a brief history and the application of a questionnaire related to disability, as it characterizes one of the inclusion criteria. Eligible patients will be informed about the objectives and procedures of the study. They will be informed that there are two active interventions, but it is not yet known which one is superior. Eligible patients that agree to participate in the study will sign a print informed consent form before enrollment. The study started in May 2022, and the recruitment rate is 10 patients per month on average.
Treatment allocation and randomisation
Initially, a random sequence in blocks will be generated through a computer program by a researcher not involved in data collection. The random codes for treatment will be placed in opaque, sealed envelopes and sequentially numbered, thus assuring the secret allocation of individuals to the study groups. After the initial assessment, inclusion in the study, and baseline data collection, a researcher will open the envelopes and refer the participant to the physical therapist responsible for the respective group of allocation. The patient will start treatment in the same week, with groups of up to 6 patients for each treatment.
Intervention
Patients included in the study will be randomised to receive Pilates method exercises associated with education to keep the abdomen relaxed (KAR) or contracted (KAC). A certified physiotherapist in the Pilates method with at least 10 years of clinical practice has trained two other physiotherapists, both certified in the Pilates method (100 hours of training), for the exercise protocol. The training performed for the exercise protocol of both physiotherapists was the same. The training for the instruction type used in each intervention group was carried out individually. In addition, a pilot study was performed with 16 volunteers for 3 months.
Pilates method is characterized by exercises that involve the body and mind [25]. Its principles include 1. Centralization, based on the activation of the core or powerhouse muscles (transversus abdominis, diaphragm, obliques, multifidus, and pelvic floor) during exercises, as they are involved in the stabilization of the lumbopelvic complex; 2. Concentration, focusing attention on proper exercise performance; 3. Control, the exercise is performed with concentration, movement, and posture control; 4. Precision, which refers to paying attention to the quality of the exercise technique; 5. Breathing, the exercises are performed in the rhythm of breathing, promoting the activation of the deep muscles of the trunk; and 6. Flow: smoothness during exercise [26,27,28].
Based on validated protocol by Brito da Silva et al. (2018), nine exercises will be proposed: Spine stretch, The spine twist, The hundred, The one leg circle, The plank, Leg pull front, Swimming, Rocking, and Swan (Additional file 1: Appendix 1) [29]. All exercises will be performed in a single series, with 10 repetitions, previously demonstrated by the physical therapist. Aiming that the protocol can be executed in any circumstances, equipment and materials will not be used. The exercises will always be performed in groups of a maximum of six patients, however the progression in each exercise will be individualized. The sessions will last 60 minutes, twice a week until the 12 weeks are completed, without prescription of home exercises. Sessions will be conducted in different environments and without any contact between therapists and participants.
In the KAC group (control), patients will receive instructions about breathing and its performance along with muscle action. Patients will receive verbal instructions about the performance of each exercise. During execution, postures will be corrected as needed. All patients in the KAC group will be instructed about the performance of exercises based on specific activation of the musculature (transversus abdominis, diaphragm, obliques, multifidus, and pelvic floor). This characterizes the contraction of the center of strength (core or powerhouse), conceptualized by stabilization depth and activation of abdominal bracing. During the execution of the exercises, the patients will receive stimuli through verbal commands, which will be continuously reinforced, so that the contraction of the muscles is performed throughout the protocol. In the KAR group (experimental), patients will be instructed to perform the exercises in a relaxed and smooth way, keeping only breathing and concentration during their execution. Also, at no time will the participants be instructed to perform abdominal muscle contraction or activation of the center of strength.
The assessment of treatment fidelity will be performed by in vivo observations as well as video recording during the pilot study and along the trial. Therefore, both groups will be monitored, ensuring adequate adherence to the treatment that will be performed as planned.
Characteristics of participants
Baseline characteristics will include sociodemographic information, symptoms duration, number of pain areas, family history of low back pain, magnetic resonance imaging (MRI) performed, chronicity risk (Örebro Musculoskeletal Pain Questionnaire [OMPQ]), history of Pilates method practice, and life stress events (Table 3). Baseline characteristics (e.g. history of Pilates method practice) may be analyzed as potential predictors or moderators of outcomes.
Outcome measures
Co-primary outcomes will be pain intensity (Numerical Pain Scale) and disability (Roland-Morris Disability Questionnaire) related to primary chronic low back pain assessed 12 weeks after randomisation, obtained through self-report. Secondary outcomes will be global improvement (Perception of Global Effect Scale) and specific functionality (Patient-specific Functional Scale) assessed 12 weeks after randomisation (Table 4).
Blinding
It was not possible to blind the participants and the treating clinicians. The assessors were not considered blinded because the participants were not blinded, and outcomes were self-reported. However, to guarantee that the treatment expectation was evenly balanced between the groups and decrease measurement bias, the participants will not know the study hypothesis, and the assessors will not know the participant’s intervention group. The statistician will be blinded to the group allocation.
Statistical analysis
The analysis of the data obtained during the research will be carried out by a statistical professional who will have access to the coded data and were based on intention-to-treat principles. Missing data will be assumed to be missing completely at random. Multiple imputation will be used to account for these missing data [34]. Missing values in outcome variables will be estimated using multiple imputation by chained equations after 50 replicated imputed data sets. Variables included in the multiple imputation process will include (1) group factor, (2) time factor, and (3) the respective outcome variable. Descriptive statistics will be used to present the characteristics of participants in the two treatment groups. Two-sided P values of less than 0.05 will be considered to indicate statistical evidence of significance. The outcomes pain intensity and disability will be analyzed using repeated-measure linear mixed models (participants and time as random factors) that included all the scores that will be reported after randomisation with the baseline scores and treatment clusters as covariates. Adjusted mean differences will be tested at 12 weeks after randomisation. Multiple comparisons will be performed using the Tukey test with P values adjusted using the Holm procedure. The baseline variables will be evaluated as predictors and moderators of treatment effects including terms and interaction models. Effect sizes for primary and secondary outcomes will be calculated as Cohen’s d from estimated marginal means and standard error estimates from the primary adjusted analysis. Effect sizes will be interpreted according to Cohen’s criteria (small ≤0.2; moderate = 0.5; large ≥0.8) [35]. All analyses will be performed using the RStudio version 0.99.486.
Sample size estimation
The sample size required for this study will be 152 (76 per group) to detect a mean difference of 4.0 points for disability measured by RMDQ and 1.0 for pain intensity measured by NPRS between the two intervention arms, assuming a standard deviation of 4.9 for disability and 2.0 for pain, with an alpha of 5%, power of 80% and a possible loss to follow-up of 15 % [36,37,38].
Discussion
The results of this study will contribute to the understanding of the effectiveness of education to keep the abdomen relaxed versus contracted during Pilates method exercises in the treatment of primary chronic low back pain. Pilates is commonly used as an effective treatment for low back pain [39]. In Brazil, the Pilates method is widely disseminated, including practitioners of different profiles and age groups. It is used by physiotherapists for the prevention, recovery, and maintaining the overall functioning of the body.
There are no comparisons between these different strategies during the practice of Pilates method exercises – education based on a contraction versus relaxation of the abdomen. In this sense, aiming to understand the value of each component and increase the effect size of Pilates treatment, the result of a randomised controlled clinical trial of high methodological quality will help physical therapists in the clinical decision-making process.
There will be no objective measure of abdominal muscles activation in our study. However, regardless of whether the participant is able to activate the muscles as requested by the physiotherapist, the instruction for contracting the abdominal itself is an instruction for protecting the lower back during the exercises as opposed to the experimental group.
The sample size of this study will be sufficient to detect the relevant effects of different protocols conducted with a low risk of bias. Increasing the relevance of the study, the exercise protocol will be designed to reproduce the same format in which they would be conducted in the clinical practice by a certified physical therapist. The conclusions of this study may contribute to the existing literature for the treatment of patients with primary chronic low back pain with Pilates.
Trial registration in a clinical trials database
This study was prospectively registered in the Clinical Trials (Registration number: NCT05336500) and approved by the Human Research Ethics Committee (Plataforma Brasil CAAE 25669519.4.0000.5116). Recruitment begins in May 2022 and is expected to continue until March 2023.
Availability of data and materials
All data measured and/or manipulated during the study will be available by the corresponding author on reasonable request. Patients will be accompanied by the physiotherapist responsible for their treatment. All possible adverse effects or events during the intervention will be recorded daily. An auxiliary researcher will act as data coordinator at baseline and during reassessments, being responsible for all the processes involved until the end of the research (completion of tables and data processing). All documents will be stored in a safe place, being accessible only to the researchers involved. Electronic data will be protected on a computer with a restricted password and access, and only authorized researchers will be able to handle them. All names or personally identifiable information will be encoded. The statistician who will do the final analysis will receive the coded data.
Change history
13 February 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12891-023-06224-0
Abbreviations
- CAPES:
-
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior
- FAPERJ:
-
Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro
- KAC:
-
Education to keep the abdomen contracted
- KAR:
-
Education to keep the abdomen relaxed
- NPS:
-
Numerical Pain Scale
- OMPQ:
-
Örebro Musculoskeletal Pain Questionnaire
- PGES:
-
Perception of Global Effect Scale
- PSFS:
-
Patient-specific functional scale
- RMDQ:
-
Roland-Morris Disability Questionnaire
References
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. Lancet Publishing Group. 2017;389:736–47.
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. Lancet Publishing Group. 2018;391:2356–67.
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391:2368–83.
Hasanpour-Dehkordi A, Dehghani A, Solati K. A comparison of the effects of Pilates and McKenzie training on pain and general health in men with chronic low back pain: a randomized trial. Indian J Palliat Care. 2017;23:36–40. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28216860.
Mostagi FQRC, Dias JM, Pereira LM, Obara K, Mazuquin BF, Silva MF, et al. Pilates versus general exercise effectiveness on pain and functionality in non-specific chronic low back pain subjects. J Bodyw Mov Ther. 2015;19:636–45.
Wajswelner H, Metcalf B, Bennell K. Clinical pilates versus general exercise for chronic low back pain: randomized trial. Med Sci Sports Exerc. 2012;44:1197–205. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22246216.
Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021;9. Available from: https://pubmed.ncbi.nlm.nih.gov/34580864/.
Eliks M, Zgorzalewicz-Stachowiak M, Zeńczak-Praga K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: state of the art. Postgrad Med J. 2019;95:41–5.
de Macedo CSG, Debiagi PC, de Andrade FM. The Isostretching effect in the muscle strength of gluteus maximus, abdominal and the trunk extensor, incapacity and pain in patients with low back pain. Fisioter Mov. 2010;23:113–20.
Lee K. The relationship of trunk muscle activation and core stability: a biomechanical analysis of Pilates-based stabilization exercise. Int J Environ Res Public Health. 2021;18. Available from: https://pubmed.ncbi.nlm.nih.gov/34886530/.
Batıbay S, Külcü DG, Kaleoğlu Ö, Mesci N. Effect of Pilates mat exercise and home exercise programs on pain, functional level, and core muscle thickness in women with chronic low back pain. J Orthop Sci. 2021;26:979–85. Available from: https://pubmed.ncbi.nlm.nih.gov/33386201/.
de Oliveira NTB, Ricci NA, dos Santos Franco YR, Salvador EMES, Almeida ICB, Cabral CMN. Effectiveness of the Pilates method versus aerobic exercises in the treatment of older adults with chronic low back pain: a randomized controlled trial protocol. BMC Musculoskelet Disord. 2019;20. Available from: https://pubmed.ncbi.nlm.nih.gov/31122227/.
Cruz-Díaz D, Romeu M, Velasco-González C, Martínez-Amat A, Hita-Contreras F. The effectiveness of 12 weeks of Pilates intervention on disability, pain and kinesiophobia in patients with chronic low back pain: a randomized controlled trial. Clin Rehabil. 2018;32:1249–57. Available from: https://pubmed.ncbi.nlm.nih.gov/29651872/.
Miyamoto GC, Franco KFM, van Dongen JM, Franco YRDS, de Oliveira NTB, Amaral DDV, et al. Different doses of Pilates-based exercise therapy for chronic low back pain: a randomised controlled trial with economic evaluation. Br J Sports Med. 2018;52:859–68.
Mazloum V, Sahebozamani M, Barati A, Nakhaee N, Rabiei P. The effects of selective Pilates versus extension-based exercises on rehabilitation of low back pain. J Bodyw Mov Ther. 2018;22:999–1003. Available from: https://pubmed.ncbi.nlm.nih.gov/30368347/.
Gholamalishahi S, Backhaus I, Cilindro C, Masala D, la Torre G. Pilates-based exercise in the reduction of the low back pain: an overview of reviews. Eur Rev Med Pharmacol Sci. 2022;26:4557–63. Available from: https://pubmed.ncbi.nlm.nih.gov/35856344/.
Gubler D, Mannion AF, Schenk P, Gorelick M, Helbling D, Gerber H, et al. Ultrasound tissue doppler imaging reveals no delay in abdominal muscle feed-forward activity during rapid arm movements in patients with chronic low back pain. Spine. 2010;Phila Pa 1976(35):1506–13.
Coenen P, Campbell A, Kemp-Smith K, O’Sullivan P, Straker L. Abdominal bracing during lifting alters trunk muscle activity and body kinematics. Appl Ergon. 2017;63:91–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28502411.
Campbell A, Kemp-Smith K, O’Sullivan P, Straker L. Abdominal bracing increases ground reaction forces and reduces knee and hip flexion during landing. J Orthop Sports Phys Ther. 2016;46:286–92. Movement Science Media. Available from: http://www.jospt.org/doi/10.2519/jospt.2016.5774.
Ghamkhar L, Kahlaee AH. Trunk muscles activation pattern during walking in subjects with and without chronic low back pain: a systematic review. PM R. 2015;7:519–26. Available from: https://pubmed.ncbi.nlm.nih.gov/25633636/.
Lima M, Ferreira AS, Reis FJJ, Paes V, Meziat-Filho N. Chronic low back pain and back muscle activity during functional tasks. Gait Posture. 2018;61:250–6. Available from: https://doi.org/10.1016/j.gaitpost.2018.01.021.
Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-Jerić K et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158:200–7. Available at: https://www.acpjournals.org/doi/full/10.7326/0003-4819-158-3-201302050-00583?rfr_dat=cr_pub++0pubmed&url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org.
Altman DG, Schulz KF, Moher D, Egger M, Davidoff F, Elbourne D, et al. The revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern Med. 2001;134:663–94. Available from: https://pubmed.ncbi.nlm.nih.gov/11304107/.
Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014:348. Available from: https://pubmed.ncbi.nlm.nih.gov/24609605/.
Hoffman J, Gabel CP. The origins of Western mind–body exercise methods. Phys Ther Rev. 2015;20:315–24.
Latey P. The Pilates method: history and philosophy. J Bodyw Mov Ther. 2001;(5):275–82. Available from: http://www.idealibrary.com
Muscolino JE, Cipriani S. Pilates and the “powerhouse”. J Bodyw Mov Ther. 2016;8:15–24. Available from: https://doi.org/10.1016/S1360-8592(03)00057-3.
Wells C, Kolt GS, Bialocerkowski A. Defining pilates exercise: a systematic review. Complement Ther Med. 2012;20:253–62.
da Silva PHB, da Silva DF, da Oliveira JKS, de Oliveira FB. The effect of the Pilates method on the treatment of chronic low back pain: a clinical, randomized, controlled study. Brazilian J Pain. 2018;1:21–8.
Fuhro FF, Fagundes FRC, Manzoni ACT, Costa LOP, Cabral CMN. Örebro musculoskeletal pain screening questionnaire - short form and start Back screening tool: correlation and agreement analysis. Spine (Phila Pa 1976). 2016;41:E931–6.
Costa LOP, Maher CG, Latimer J, Ferreira PH, Ferreira ML, Pozzi GC, et al. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: which one is the best? Spine (Phila Pa 1976). 2008;33:2459–63. Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed8&NEWS=N&AN=2009254927.
Vigotsky AD, Tiwari SR, Griffith JW, Apkarian AV. What is the numerical nature of pain relief? Front Pain Res (Lausanne, Switzerland). 2021;2. Available from: https://pubmed.ncbi.nlm.nih.gov/35295426/.
Nusbaum L, Natour J, Ferraz MB, Goldenberg J. Translation, adaptation and validation of the Roland-Morris questionnaire - Brazil Roland-Morris. Braz J Med Biol Res. 2001;34:203–10.
Sterne JAC, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:157–60. Available from: https://pubmed.ncbi.nlm.nih.gov/19564179/.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. New York: Routledge; 1988. Available from: https://www.taylorfrancis.com/books/mono/10.4324/9780203771587/statistical-power-analysis-behavioral-sciences-jacob-cohen.
Costa LOP, Maher CG, Latimer J, Hodges PW, Herbert RD, Refshauge KM, et al. Motor control exercise for chronic low back pain: a randomized placebo-controlled trial. Phys Ther. 2009;89:1275–86. Available from:https://pubmed.ncbi.nlm.nih.gov/19892856/.
Costa LOP, Maher CG, Latimer J, Ferreira PH, Pozzi GC, Ribeiro RN. Psychometric characteristics of the Brazilian-Portuguese versions of the Functional Rating Index and the Roland Morris Disability Questionnaire. Spine (Phila Pa 1976). 2007;32:1902–7. Available from: https://pubmed.ncbi.nlm.nih.gov/17762300/.
Garcia AN, Costa LDCM, Hancock MJ, de Souza FS, Gomes GVFDO, de Almeida MO, et al. McKenzie Method of Mechanical Diagnosis and Therapy was slightly more effective than placebo for pain, but not for disability, in patients with chronic non-specific low back pain: a randomised placebo controlled trial with short and longer term follow-up. Br J Sports Med. 2018;52:594–600. Available from: https://bjsm.bmj.com/content/52/9/594.
Cordeiro ALL, Oliveira APS, Cerqueira NS, Santos FAD, Oliveira AMS. Pilates method on pain in patients with low back pain: systematic review. Brazilian J Pain. 2022;5:265–71. Available from: http://brjp.org.br/article/doi/10.5935/2595-0118.20220038.
Acknowledgements
This study was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES), Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro – FAPERJ, and Fundação de Amparo à Pesquisa do Estado de Minas Gerais – FAPEMIG.
Funding
This study was supported by the Fundação Carlos Chagas Filho de Apoio à Pesquisa do Estado do Rio de Janeiro (FAPERJ, No. E-26/211.104/2021, No. E-26/210.239/2018, and No. E-26/201.357/2022), and Coordenação de Aperfeiçoamento de Pessoal (CAPES, Finance Code 001; No. 88881.708719/2022-01, and No. 88887.708718/2022-00).
Author information
Authors and Affiliations
Contributions
The authors have contributed substantially to this protocol and accept responsibility for the content of the manuscript. All authors have read and approved the manuscript. LCL: Conceptualization, Writing - original draft, Writing - review & editing, Supervision. MADN: Methodology, Investigation, Data curation. LFB: Methodology, Investigation, Data curation. LRC: Investigation (blinded evaluator), Data curation. ASF: Methodology, Data curation, Formal analysis, Writing - review & editing. NMF: Conceptualization, Writing - review & editing, Supervision, Project administration.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The approval was obtained from the Human Research Ethics Committee from Centro Universitário de Lavras (Plataforma Brasil CAAE 25669519.4.0000.5116, No. 3716573) and prospectively registered at https://www.clinicaltrials.gov/ (Registration number: NCT05336500).
Participation in the study will be voluntary and conditioned to the completion and signing of the print informed consent form by all individuals included, containing information about the objectives and procedures of the research. The non-compulsory participation will be informed, as well as the confidentiality of information about the participants will be guaranteed, ending the research only when the entire sample is collected.
Subjects will also be aware that regardless of the treatment group they will be allocated to, the intervention will consist of a physical therapy treatment considered effective for low back pain that does not present health risks.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: the authors corrected the three mentions of reference [22] in Table 4 from "Chan et al. 2013" to "Costa et al. 2008”. Furthermore, the missing "S" of the word "Specific" under Secondary outcomes in Table 1 was inserted.
Supplementary Information
Additional file 1: Appendix 1.
Exercise protocol based on the Pilates method.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lunkes, L.C., Dias Neto, M.A., Barra, L.F. et al. Education to keep the abdomen relaxed versus contracted during pilates in patients with chronic low back pain: study protocol for a randomised controlled trial. BMC Musculoskelet Disord 24, 49 (2023). https://doi.org/10.1186/s12891-023-06160-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06160-z