
Abstract
Background
Extensive muscle atrophy is a common occurrence in orthopaedics patients who are bedridden or immobilized. The incidence is higher in intensive care unit (ICU) inpatients. There is still controversy about how to use neuromuscular electrical stimulation (NMES) in ICU patients. We aim to compare the effectiveness and safety of NMES to prevent muscle atrophy in intensive care unit (ICU) patients without nerve injury.
Methods
ICU patients without central and peripheral nerve injury were randomized into experimental group I (Exp I: active and passive activity training (APAT) + NMES treatment on the gastrocnemius and tibialis anterior muscle), experimental group II (Exp II: APAT + NMES treatment on gastrocnemius alone), and control group (Ctl: APAT alone). Changes in the strength of gastrocnemius, the ankle range of motion, and the muscle cross-section area of the lower leg were evaluated before and after the intervention. Also, changes in prothrombin time, lactic acid, and C-reactive protein were monitored during the treatment.
Results
The gastrocnemius muscle strength, ankle joint range of motion, and cross-sectional muscle area of the lower leg in the three groups showed a downward trend, indicating that the overall trend of muscle atrophy in ICU patients was irreversible. The decrease in gastrocnemius muscle strength in Exp I and Exp II was smaller than that in the control group (P < 0.05), but there was no difference between Exp I and Exp II. The decrease in active ankle range of motion and cross-sectional area of the lower leg Exp I and Exp II was smaller than that in the control group (P < 0.05), and the decrease in Exp I was smaller than that of Exp II (all P < 0.05). The curative effect in Exp I was better than in Exp II. There were no significant differences in the dynamic changes of prothrombin time, lactic acid, and C-reactive protein during the three groups (P > 0.05).
Conclusion
In addition to early exercise training, NMES should be applied to prevent muscle atrophy for patients without nerve injury in ICU. Also, simultaneous NMES treatment on agonist/antagonist muscle can enhance the effect of preventing muscle atrophy.
Trial registration
This study was prospectively registered in China Clinical Trial Registry (www.chictr.org.cn) on 16/05/2020 as ChiCTR2000032950.
Similar content being viewed by others


Background
Extensive muscle atrophy is a common occurrence in patients who are bedridden or immobilized [1, 2], while the degree of muscle atrophy is positively correlated with the time spent in bed [1]. Also, the incidence is higher in intensive care unit (ICU) inpatients. Disturbance of consciousness, mechanical ventilation, use of glucocorticoids, insufficient nutritional intake, and so on are some of the factors that can reduce muscle protein synthesis and promote muscle protein decomposition in ICU patients. Also, some ICU patients developed intensive care unit-acquired weakness (ICU-AW) [3, 4]. Surveys have shown that the incidence of muscular atrophy in intensive care patients receiving mechanical ventilation is as high as 60% [5, 6]. In addition, muscle atrophy has been closely associated with a prolonged hospital stay, increased duration of mechanical ventilation, and increased mortality [7, 8]. Also, studies have reported that muscle atrophy develops rapidly during the first week of stay in the ICU [1, 9, 10]; thus, early and effective intervention is very important.
Among early interventions, Neuromuscular Electrical Stimulation (NMES) has been commonly used to prevent muscle atrophy in ICU patients by improving their muscle strength and maintaining muscle mass [11, 12]. Yet, whether NMES should be used for conscious ICU bedridden patients who can independently move remains debatable. Some scholars advocate that NMES should not be used when the patient’s consciousness level is improved, and the patient can carry out autonomous activities [13], while other studies suggested that early active contraction combined with NMES can more alleviate muscle strength loss and atrophy through different modes of muscle activation [14]. Moreover, some studies have shown a dose-response relationship between NMES treatment intensity and NMES effectiveness [15], i.e., the non-physiological high stimulation intensity and disordered recruitment of motor units caused by NMES may lead to rapid muscle fatigue and muscle injury [16,17,18]. On the other hand, when the agonist and antagonist muscles are stimulated, the muscle fibers contract synchronously, reducing fatigue [19]. Still, it remains unclear whether simultaneous stimulation of the agonist and antagonist muscle can better prevent muscle atrophy.
In this study, we explored whether NMES treatment should be added to ICU patients without neurological impairment who can carry out active activities in bed. We compared the efficacy of NMSE treatment when simultaneously stimulating agonist and antagonist muscles. In addition, the safety of early NMES intervention was analyzed and discussed.
Methods
Study design
This study was a randomized parallel controlled trial and approved by the Ethics Committee of Shanghai Sixth People’s Hospital (2020–076) and registered in the China Clinical Trial Registry (ChiCTR2000032950) on 16/05/2020. All patients signed the informed consent form. All methods were performed in accordance with the Declaration of Helsinki. Furthermore, the trial was reported based on the Guidelines for Consolidated Standards of Reporting Trials (CONSORT 2010).
Subjects
Patients admitted to the emergency ICU of our hospital from December 2020 to June 2021 were included in the study. Inclusion criteria were: (1) patients who were conscious; (2) with no central and peripheral nervous system injury; (3) no acute exacerbation; (4) expected to be treated in ICU for more than 1 week, and training could be completed on at least one side of the lower limbs. Exclusion criteria were the following: patients in a coma, inability to cooperate with treatment, original limb function defect or neuromuscular disease, other defects, wound or external fixation of the treatment area, patients with sarcopenia (calf circumference < 34 cm for men and < 33 cm for women, and grip strength < 28 kg for men and < 18 kg for women) [20], and other contraindications of NMES, such as high fever, cardiac pacemaker implantation, severe arrhythmia, etc.
The changes in the muscle strength of the gastrocnemius measured by dynamometer before and after 1 week of bed rest were selected as the main outcome, then based on the mean ± standard deviation (20.69 ± 5.24, 18.45 ± 5.13) the effect value was calculated by GPower3.1(University of Düsseldorf, Germany) as 0.43. The sample size was calculated as 57 cases (α = 0.05, 1-β = 0.8). Therefore, taking into account the 15% loss rate, the proposed sample is 65 cases.
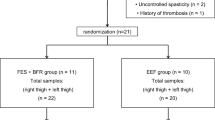
The patients who met the trial criteria were randomly assigned to three groups using the block randomization method with a block size of eleven: Experimental group I (n = 21), Experimental group II (n = 22) and Control group (n = 22) (Fig. 1). To control the potential selection bias, the random allocation sequence was generated by a person who was not involved in the enrollment or screening of participants. The enrolled patients, the evaluators and the statistical analysis specialist were blinded to group assignment.

Flow diagram of the study
Interventions
Experimental group I (Exp I): patients received active and passive activity training (APAT) on the lower limbs + NMES on the gastrocnemius and tibialis anterior muscles; experimental group II (Exp II): patients received APAT on lower limbs + NMES on gastrocnemius alone; control group (Ctl): patients received APAT on the lower limbs. The initial time of intervention was the 2nd or 3rd day after admission to the ICU ward. The end time of intervention was the day of transfer out of ICU or the day before.
Active and passive activity training
Patients were placed in a supine position. The same therapist passively moved the patient’s bilateral ankles, knees, and hips to the maximum range of motion for 5–10 minutes and then instructed the patient to perform active dorsiflexion, plantar flexion, inversion and eversion of ankles, active extension and flexion of knees, active flexion of hips, and abduction and adduction to the maximum range of motion. The training lasted 15 to 20 minutes and was performed twice per day for at least 7 days until the patient was released from the ICU. If one side of the patient’s lower limb needed to be immobilized due to illness, only the healthy side of the lower limb was trained.
NMES treatment
Patients were placed in a supine position. The patient’s calfskin was exposed, and then two self-adhesive electrodes (6 cm × 9 cm) were placed on the motor point of the target muscle (the skin area with the lowest stimulation threshold when stimulating the muscle)(Fig. 2). The adhesive area was marked with a marking pen to allow stimulation in the same position every day. The electrode plate was connected with a neuromuscular electrical stimulator (QT-22 T, ITO, Japan). Based on the recommendations of the physiotherapy techniques textbook, for mild to moderate disuse myatrophy, the parameters are set as follows: pulsed current and a biphasic, asymmetrical, balanced rectangular waveform [21, 22], frequency of 30 Hz(the frequency that feels comfortable to the human body [23]), wave width of 300 μs(consistent with the time value for stimulating the motor nerve [24]), on/off ratio of 1:4, adjusting the current intensity according to the patient’s feelings, 20 min/time, twice a day for at least 7 days until the patient was released from the ICU. Effective muscle stimulation is defined as palpable and visible muscle contraction. The same therapist performed the treatment.

Neuromuscular electrical stimulation treatment. a NMES on the gastrocnemius and tibialis anterior muscles in experimental group I . b NMES on gastrocnemius alone in experimental group II
Primary outcome measures
Muscle strength of the gastrocnemius
The muscle strength of ankle plantar flexion (gastrocnemius) was measured with a dynamometer (OE-210, ITO, Japan) at baseline and at the same time (8: 00 ~ 9: 00 am) before transferring the patient out of the ICU. The patient was placed in the supine position; the hip and knee joints were in the extension position, and the ankle joints were in the neutral position. The therapist fixed the knee joints with one hand and placed the dynamometer on the proximal end of the metatarsal bone in the sole resisting the plantarflexion force with the other hand. Patients were instructed to perform plantar flexion of the ankle to maximum isometric contraction during the test (Fig. 3a). A one-minute rest was given between two consecutive tests, and the measurements were repeated 3 times; data were averaged. Only the lower extremities that received the therapeutic intervention were assessed, and for patients who received the intervention in both lower extremities, the results were averaged and recorded. The assessment was completed by the same therapist who was blinded to the grouping.

Measure the strength of gastrocnemius muscle (a) and Active joint range of motion of ankle joint (b)
CT evaluation of muscle cross-sectional area
Patients underwent CT plain scan on the lower leg of the treatment side when entering the ICU and then again before leaving the ICU. Before scanning, the non-metallic marker was placed at 10 cm below the tibial tubercle. CT images of the lower leg were obtained by the plain scan with CT (SOMATOM Force, SIEMENS, Germany). The muscle boundary of the target section was semi-automatically marked by ImageJ (Fig. 4) [25], after which the muscle cross-sectional area (CSA) was automatically calculated. After obtaining the data before and after treatment, the value before treatment was defined as 100%, and then the change rate of the value after treatment was calculated. CT scanning, labeling, and recording of CSA data were performed and averaged bilaterally by the same radiology operator who was blinded to grouping.

Lower leg CT plain scan and muscle area marking. a CT cross-section image of the lower leg (10 cm below the tibial tubercle). b Muscle boundary was marked with ImageJ; the cross-sectional area of the muscle was automatically calculated
Active joint range of motion of ankle joint
The active range of motion (AROM) of the ankle was measured at baseline and then again before the patient was released from the ICU. The patient was placed in the supine position. The knee joint was straight or slightly flexed, the ankle was in the neutral position; the intersection point of the fibula longitudinal axis and the outer edge of the foot was the axis, the line parallel to the fibula longitudinal axis was the fixed arm, and the line parallel to the fifth metatarsal longitudinal axis was the moving arm. Then ankle active dorsiflexion and plantarflexion angles were measured by goniometer (IL-1, Changzhou Zhongquan Medical Rehabilitation Equipment Co., Ltd., China) before and after treatment (Fig. 3b). AROM = plantar flexion angle + dorsiflexion angle. Each patient was measured twice, and data were averaged. The same therapist who performed the muscle strength assessment completed the measurements.
Secondary outcome measures
Safety of NMES treatment
The changes in C-reactive protein (CRP), prothrombin time (PT), and lactic acid were monitored on days 1, 3, 5, and 7 during the treatment using an automatic CRP analyzer (PA-990, Lifotronic Shenzhen Pumen Technology Co., Ltd., China), automatic coagulation analyzer (CS5100, Sysmex Co., Ltd., Japan), and automatic blood gas analyzer (GEM Premier 3500, Instrumentation Laboratory, USA). The operator of biochemical testing was blinded to the grouping.
Statistical analysis
SPSS 23.0 (SPSS, IBM, USA) was used to complete data entry and statistical analysis. Enumeration data were expressed as frequency, and measurement data were expressed as mean ± standard deviation (\(\overline{\mathrm{x}}\) ± SD). The chi-square test was used to compare enumeration data. When the measurement data were in accordance with the normality test and homogeneity of variance test, the F test was used, on the contrary, the rank-sum test was used. The comparison among the three groups was conducted by repeated measurement data analysis of variance, and the LSD method was used to compare between groups (whether the intervention was implemented or not) and within groups (different time points). A two-sided test was applied, and P-value < 0.05 was considered statistically significant.
Results
General information
A total of 65 patients were recruited; 3 patients were lost due to early discharge (Exp II 1 case and Ctl 2 cases), and 2 patients were lost due to aggravation of the disease (1 case both in Exp I and Exp II). Finally, 60 patients participated in the study, all of whom belonged to the Per Protocol Set (PPS), including 51 males and 9 females. No adverse events were reported. Most of the patients had pelvic and spinal fractures (72.8%), and the average ICU stay was 13.35 days. The general information about the patients is shown in Table 1. There was no significant difference in the general information among the three groups (all P > 0.05).
For ICU patients, the severity of critical illness, duration of ICU stay, the duration of mechanical ventilation, the duration of sedation and corticosteroid therapy were risk factors for ICU-acquired muscle weakness [3]. In this study, the proportion of patients with those risk factors was not high, and there was no statistical difference among the three groups.
Primary outcome measures
Comparison of gastrocnemius muscle strength
Compared with before treatment, the gastrocnemius muscle strength of the three groups decreased to different degrees (all P < 0.05). The muscle strength of Exp I and Exp II was higher than that of the Ctl (Exp I vs Ctl, d = 2.60, 95%CI:1.13 ~ 4.07, P < 0.05; Exp II vs Ctl, d = 2.60, 95%CI:1.24 ~ 3.96, P < 0.05), but there was no significant difference between Exp I and Exp II (d = 0.00, 95%CI:-1.45 ~ 1.45, P > 0.05) (Fig. 5).

Comparison of gastrocnemius muscle strength before and after treatment. a Decrease of gastrocnemius muscle strength before and after treatment in the three groups. b Gastrocnemius muscle strength gap before and after treatment among the three groups. Exp I: experimental group I, Exp II: experimental group II, Ctl: control group; Bef: before treatment, Aft: after treatment; * P < 0.05 between each group before and after treatment; # P < 0.05 vs. control group
Comparison of ankle AROM
Compared with before treatment, the AROM of ankle joints in three groups decreased to different degrees (all P < 0.05). The gap analysis between groups showed that after treatment, the decrease of AROM of the ankle joint in Exp I and Exp II was smaller than that in Ctl(Exp I vs Ctl, d = 7.90, 95%CI:4.437 ~ 11.36, P < 0.05; Exp II vs Ctl, d = 3.97, 95%CI: 0.43 ~ 7.50, P < 0.01), and there was a significant difference between Exp I and Exp II (d = 3.93, 95%CI: 1.19 ~ 6.67, P < 0.05) (Fig. 6).

Comparison of AROM of ankle joint before and after treatment. a AROM of ankle joint before and after treatment among three groups. b Comparison of ankle AROM gap before and after treatment in three groups. Exp I: experimental group I, Exp II: experimental group II, Ctl: control group; Bef: before treatment, Aft: after treatment; * P < 0.05 between each group before and after treatment; # P < 0.05 vs. control group; & P < 0.05 between the Exp I and the Exp II
Comparison of muscle CSA
Compared with before treatment, muscle CSA in three groups decreased in different ranges (all P < 0.05). The comparative analysis between groups showed that after treatment, the decrease of muscle CSA in the leg of Exp I and Exp II was smaller than that of the Clt (Exp I vs Ctl, d = 8.93, 95%CI:6.20 ~ 11.66, P < 0.01; Exp II vs Ctl, d = 4.54, 95%CI: 1.38 ~ 7.70, P < 0.05), and there was a significant difference between Exp I and Exp II (d = 4.39, 95%CI: 1.50 ~ 7.28, P < 0.05) (Fig. 7).

Comparison of muscle CSA of the lower leg before and after treatment. a Decrease of muscle CSA of the lower leg before and after treatment among three groups. b Comparison of muscle CSA gap before and after treatment in three groups. Exp I: experimental group I, Exp II: experimental group II, Ctl: control group; Bef: before treatment, Aft: after treatment; CSA: cross-sectional area; * P < 0.05 between each group before and after treatment; # P < 0.05 vs. Ctl; & P < 0.05 between Exp I and the Exp II
Secondary outcome - safety parameters
There was no statistically significant difference in CRP, lactic acid, and PT among the three groups on the 1st, 3rd, 5th, and 7th days of treatment (Fig. 8).

Comparison of the changes of CRP (a), lactic acid (b), and PT (c) in the three groups during treatment. Exp I: experimental group I, Exp II: experimental group II, Ctl: control group
Discussion
Using NMES to prevent muscle atrophy in ICU patients is still controversial [11, 16,17,18,19]. Our results showed that even with exercise therapy and NMES treatment, patients without nerve injury in ICU still developed muscle atrophy. Yet, stimulating antagonistic muscles simultaneously with NMES provided a better curative effect that when stimulating a group of muscles alone.
Myogenic weakness occurs in ICU patients due to systemic inflammatory response, stress, heavy drug use, and reduced stress load [26]. Comprehensive treatment is generally adopted, including nutritional support, blood sugar control, and rehabilitation treatment [27,28,29]. During the rehabilitation treatment, active and passive exercise training for patients is generally considered. Most scholars [30] have approved NMES treatment for patients with nerve injury or inability to move; yet, it is still controversial whether NMES should be added to patients with no nerve injury, consciousness, and active bed exercise. Some scholars advocate that when the level of consciousness of patients is improved, NMES is no longer needed when voluntary activities can be carried out [13]; however, there is still a lack of evidence-based medical support for whether NMES can increase the therapeutic effect of active and passive movement.
This study showed that despite the early APAT intervention, the patients still had a significant decline in muscle strength, while the patients who received NMES intervention in combination with APAT had a relatively small decline in muscle strength (P < 0.05), which is consistent with results reported by Akar et al. [31] It is believed that NMES may promote muscle activity that cannot be stimulated by exercise. We suspect that the possible mechanism is that the recruitment of motor units in NMES is just the opposite of active muscle contraction and that larger myocytes with lower axonal input impedance are more likely to be excited, and large motor units are more likely to be recruited [32]. It appears that electrically evoked muscle action produces more force than active contraction [33]. Therefore, for awake patients in ICU, early APAT combined with NMES can have a greater effect on muscular atrophy.
Some studies have reported contrary views on using NMES to prevent muscular atrophy. Some recommended stimulating quadriceps femoris only [34, 35], while others suggested stimulating multiple muscles [13] or agonist/antagonist muscle alone [36]. The present study showed that NMES single muscle group stimulation promoted slow ankle ROM loss (which is consistent with Shamsi et al [37]) and lowered extremity muscle atrophy (which is consistent with Dirks et al [38]); still, this effect was higher when a combination therapy (NMES agonist/antagonist muscle) was used. A possible reason for this result is that the simultaneous stimulation of the agonist/antagonist muscle can generate and transmit the resistance across the ankle joint through the tendon, forming the centrifugal activity of the muscle, which is the protective element of joint stability or resistance to articular cartilage stress [39]. Westing et al [40] found that the muscle torque produced by electrically stimulated eccentric contraction was 21 to 24% greater than that produced by eccentric autonomic contraction. Other studies have shown that eccentric contraction may slow the onset of muscle fatigue by increasing muscle torque [41]. In addition, other studies have also found that the co-contraction of the agonist/antagonist muscle may produce higher loads, and the co-activation of the agonist/antagonist muscle can significantly increase the tension of the Achilles tendon that can further effectively stretch the ankle joint [42, 43]. Therefore, the simultaneous stimulation of the agonist/antagonist muscle can improve the joint’s ROM. However, the specific mechanism needs to be verified by further experimental studies.
When NMES is used in ICU patients, its safety and possible side effects should also be considered. Common side effects are skin burns, muscle soreness, increased lactic acid, etc. Most of the side effects are caused by improper setting of treatment parameters or poor skin and muscle function of patients. Yet, in this study, no obvious skin burns and muscle soreness were observed. In addition, the rapid changes in inflammatory factors and coagulation function in patients after trauma can reflect the progress of the disease [44, 45]. Therefore, this study monitored the changes in CRP and PT in patients during NMES treatment; the results showed that NMES intervention had no significant effect on patients’ inflammatory status and coagulation function. Therefore, NMES is considered relatively safe for severe post-traumatic patients.
This study has a few limitations. Firstly, the sample size is relatively small. Secondly, because the purpose of this study is to evaluate the efficacy of early NMES intervention, the duration of NMES intervention is relatively short. Thus, our data need to be further verified in large sample size studies with a longer follow-up. In addition, most of the patients in this study are severe trauma patients; therefore, the findings may not apply to patients with ICU-AW due to severe cardiopulmonary and neurologic diseases.
Conclusion
Although the overall trend of muscle atrophy cannot be reversed in ICU patients without nerve injury, the combination of exercise and NMES can significantly slow down its development. In addition to APAT, NMES should be used to prevent muscle atrophy in the early stage, and the agonist/antagonist muscle should be simultaneously stimulated to enhance the effect of preventing muscle atrophy. It is relatively safe to perform NMES in the early phase of recovery.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to the privacy concern of participants but are available from the corresponding author upon reasonable request.
Abbreviations
- NMES:
-
Neuromuscular Electrical Stimulation
- ICU:
-
Intensive Care Unit
- Exp I:
-
Experimental Group I
- Exp II:
-
Experimental Group II
- Ctl:
-
Control Group
- APAT:
-
Active and passive activity training
- ICU-AW:
-
Intensive care unit-acquired weakness
- CSA:
-
Cross-sectional area
- AROM:
-
Active range of motion
- CRP:
-
C-reactive protein
- PT:
-
Prothrombin time
- PPS:
-
Per Protocol Set
References
Wall BT, Dirks ML, van Loon LJC. Skeletal muscle atrophy during short-term disuse: implications for age-related sarcopenia. Ageing Res Rev. 2013;12(4):898–906.
Memme JM, Slavin M, Moradi N, Hood DA. Mitochondrial bioenergetics and turnover during chronic muscle disuse. Int J Mol Sci. 2021;22(10):5179.
Vanhorebeek I, Latronico N, Van den Berghe G. ICU-acquired weakness. Intensive Care Med. 2020;46(4):637–53.
Tortuyaux R, Davion JB, Jourdain M. Intensive care unit-acquired weakness: questions the clinician should ask. Rev Neurol (Paris). 2022;178(1–2):84–92.
Sousa AS, Guerra RS, Fonseca I, Pichel F, Amaral TF. Sarcopenia among hospitalized patients - a cross-sectional study. Clin Nutr. 2015;34(6):1239–44.
Sheean PM, Peterson SJ, Gomez Perez S, Troy KL, Patel A, Sclamberg JS, et al. The prevalence of sarcopenia in patients with respiratory failure classified as normally nourished using computed tomography and subjective global assessment. JPEN J Parenter Enteral Nutr. 2014;38(7):873–9.
Sharshar T, Bastuji-Garin S, Stevens RD, Durand MC, Malissin I, Rodriguez P, et al. Presence and severity of intensive care unit-acquired paresis at time of awakening are associated with increased intensive care unit and hospital mortality. Crit Care Med. 2009;37(12):3047–53.
Garnacho-Montero J, Madrazo-Osuna J, Garcia-Garmendia JL, Ortiz-Leyba C, Jimenez-Jimenez FJ, Barrero-Almodovar A, et al. Critical illness polyneuropathy: risk factors and clinical consequences. A cohort study in septic patients. Intensive Care Med. 2001;27(8):1288–96.
Monk DN, Plank LD, Franch-Arcas G, Finn PJ, Streat SJ, Hill GL. Sequential changes in the metabolic response in critically injured patients during the first 25 days after blunt trauma. Ann Surg. 1996;223(4):395–405.
Plank LD, Connolly AB, Hill GL. Sequential changes in the metabolic response in severely septic patients during the first 23 days after the onset of peritonitis. Ann Surg. 1998;228(2):146–58.
Zayed Y, Kheiri B, Barbarawi M, Chahine A, Rashdan L, Chintalapati S, et al. Effects of neuromuscular electrical stimulation in critically ill patients: a systematic review and meta-analysis of randomized controlled trials. Aust Crit Care. 2020;33(2):203–10.
Mirzoev TM. Skeletal muscle recovery from disuse atrophy: protein turnover signaling and strategies for accelerating muscle regrowth. Int J Mol Sci. 2020;21(21):7940.
Hirose T, Shiozaki T, Shimizu K, Mouri T, Noguchi K, Ohnishi M, et al. The effect of electrical muscle stimulation on the prevention of disuse muscle atrophy in patients with consciousness disturbance in the intensive care unit. J Crit Care. 2013;28(4):536.e1–7.
Paillard T. Combined application of neuromuscular electrical stimulation and voluntary muscular contractions. Sports Med. 2008;38(2):161–77.
Maffiuletti NA, Gondin J, Place N, Stevens-Lapsley J, Vivodtzev I, Minetto MA. Clinical use of neuromuscular electrical stimulation for neuromuscular rehabilitation: what are we overlooking? Arch Phys Med Rehabil. 2018;99(4):806–12.
Bigland-Ritchie B, Jones DA, Woods JJ. Excitation frequency and muscle fatigue: electrical responses during human voluntary and stimulated contractions. Exp Neurol. 1979;64(2):414–27.
Gregory CM, Bickel CS. Recruitment patterns in human skeletal muscle during electrical stimulation. Phys Ther. 2005;85(4):358–64.
Foure A, Nosaka K, Wegrzyk J, Duhamel G, Le Troter A, Boudinet H, et al. Time course of central and peripheral alterations after isometric neuromuscular electrical stimulation-induced muscle damage. PLoS One. 2014;9(9):e107298.
Kim SJ, Fairchild MD, Iarkov Yarkov A, Abbas JJ, Jung R. Adaptive control of movement for neuromuscular stimulation-assisted therapy in a rodent model. IEEE Trans Biomed Eng. 2009;56(2):452–61.
Chen LK, Woo J, Assantachai P, et al. Asian working Group for Sarcopenia: 2019 consensus update on Sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020 Mar;21(3):300–307.e2.
Kho ME, Truong AD, Zanni JM, et al. Neuromuscular electrical stimulation in mechanically ventilated patients: a randomized, sham-controlled pilot trial with blinded outcome assessment. J Crit Care. 2015 Feb;30(1):32–9.
Baker LL, Bowman BR, McNeal DR. Effects of waveform on comfort during neuromuscular electrical stimulation. Clin Orthop Relat Res. 1988 Aug;233:75–85.
Bowman BR, Baker LL. Effects of waveform parameters on comfort during transcutaneous neuromuscular electrical stimulation. Ann Biomed Eng. 1985;13(1):59–74.
Prentice WE. Therapeutic modalities in rehabilitation. 4th ed; 2011.
Teigen LM, Kuchnia AJ, Nagel E, et al. Impact of software selection and ImageJ tutorial corrigendum on skeletal muscle measures at the third lumbar vertebra on computed tomography scans in clinical populations. JPEN J Parenter Enteral Nutr. 2018;42(5):933–41.
Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, et al. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310(15):1591–600.
Casaer MP, Langouche L, Coudyzer W, Vanbeckevoort D, De Dobbelaer B, Guiza FG, et al. Impact of early parenteral nutrition on muscle and adipose tissue compartments during critical illness. Crit Care Med. 2013;41(10):2298–309.
Yosef-Brauner O, Adi N, Ben Shahar T, Yehezkel E, Carmeli E. Effect of physical therapy on muscle strength, respiratory muscles and functional parameters in patients with intensive care unit-acquired weakness. Clin Respir J. 2015;9(1):1–6.
Patel BK, Pohlman AS, Hall JB, Kress JP. Impact of early mobilization on glycemic control and ICU-acquired weakness in critically ill patients who are mechanically ventilated. Chest. 2014;146(3):583–9.
Carson RG, Buick AR. Neuromuscular electrical stimulation-promoted plasticity of the human brain. J Physiol. 2021;599(9):2375–99.
Akar O, Gunay E, Sarinc Ulasli S, Ulasli AM, Kacar E, Sariaydin M, et al. Efficacy of neuromuscular electrical stimulation in patients with COPD followed in intensive care unit. Clin Respir J. 2017;11(6):743–50.
Solomonow M. External control of the neuromuscular system. IEEE Trans Biomed Eng. 1984;31(12):752–63.
Enoka RM. Muscle strength and its development. New perspectives. Sports Med. 1988;6(3):146–68.
Abu-Khaber HA, Abouelela AMZ, Abdelkarim EM. Effect of electrical muscle stimulation on prevention of ICU acquired muscle weakness and facilitating weaning from mechanical ventilation. Alexandria J Med. 2019;49(4):309–15.
Gruther W, Kainberger F, Fialka-Moser V, Paternostro-Sluga T, Quittan M, Spiss C, et al. Effects of neuromuscular electrical stimulation on muscle layer thickness of knee extensor muscles in intensive care unit patients: a pilot study. J Rehabil Med. 2010;42(6):593–7.
Abdellaoui A, Prefaut C, Gouzi F, Couillard A, Coisy-Quivy M, Hugon G, et al. Skeletal muscle effects of electrostimulation after COPD exacerbation: a pilot study. Eur Respir J. 2011;38(4):781–8.
Shamsi M, Vaisi-Raygani A, Rostami A, Mirzaei M. The effect of adding TENS to stretch on improvement of ankle range of motion in inactive patients in intensive care units: a pilot trial. BMC Sports Sci Med Rehabil. 2019;11:15.
Dirks ML, Hansen D, Van Assche A, Dendale P, Van Loon LJC. Neuromuscular electrical stimulation prevents muscle wasting in critically ill comatose patients. Clin Sci (Lond). 2015;128(6):357–65.
Solomonow M, Baratta R, D'Ambrosia R. The role of the hamstrings in the rehabilitation of the anterior cruciate ligament-deficient knee in athletes. Sports Med. 1989;7(1):42–8.
Westing SH, Seger JY, Thorstensson A. Effects of electrical stimulation on eccentric and concentric torque- velocity relationships during knee extension in man. Acta Physiol Scand. 1990;140(1):17–22.
Michaut A, Babault N, Pousson M. Specific effects of eccentric training on muscular fatigability. Int J Sports Med. 2004;25(4):278–83.
Sontag KH, Wand P, Cremer H, Mühlberg B. The proprioceptive activation of stretch tension in pretibial flexor muscles induced by stimulation of antagonistic muscle afferents. Arch Ital Biol. 1975;113(1):44–62.
Kim J, Moon JH, Kim J. Impedance control of human ankle joint with electrically stimulated antagonistic muscle co-contraction. IEEE Trans Neural Syst Rehabil Eng. 2021;29:1593–603.
Hillas G, Vassilakopoulos T, Plantza P, Rasidakis A, Bakakos P. C-reactive protein and procalcitonin as predictors of survival and septic shock in ventilator-associated pneumonia. Eur Respir J. 2010;35(4):805–11.
Walsh TS, Stanworth SJ, Prescott RJ, Lee RJ, Watson DM, Wyncoll D. Prevalence, management, and outcomes of critically ill patients with prothrombin time prolongation in United Kingdom intensive care units. Crit Care Med. 2010;38(10):1939–46.
Acknowledgments
We would like to thank Jianhong Deng and Yueqi Zhu of the Department of Radiology who assisted in the CT examination during the study. We are grateful to the doctors and nurses working in the ICU of our hospital for their cooperation in completing this study, and all patients who are willing to participate in the study.
Funding
This work was supported by Shanghai Municipal Health Commission (grant numbers 2015ZB0403). The sponsor played no role in the design, execution, analysis, and interpretation of data and preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
WB and JY wrote the original manuscript draft. JY, ZM and ML collected data. KC and YX contributed to analyzing the data. BY and YX designed the study, reviewed and edited the manuscript draft. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Shanghai Sixth People’s Hospital (2020–076) and registered in China Clinical Trial Registry (ChiCTR2000032950). All patients signed the informed consent form.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bao, W., Yang, J., Li, M. et al. Prevention of muscle atrophy in ICU patients without nerve injury by neuromuscular electrical stimulation: a randomized controlled study. BMC Musculoskelet Disord 23, 780 (2022). https://doi.org/10.1186/s12891-022-05739-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05739-2