
Abstract
Background
Previous neck-specific patient-reported outcome measures (PROMs) have tended to measure both symptoms and disability. This multi-staged study developed and evaluated a neck-specific PROM focusing on functional disability.
Methods
This study integrated findings from systematic reviews on neck-specific outcome measures, patient interviews, qualitative studies on neck disability, and iterative item testing to develop a 10-item measure of neck-related disability (ND10). Content validity was assessed by classifying items using the International Classification of Functioning, Disability and Health (ICF) and perspective linking. Patients (n = 78) with neck pain completed cognitive interviews, exploring items of the Neck Disability Index (NDI) and ND10, and completed structured questions related to literacy and relevance. Test–retest reliability and internal consistency were evaluated using intraclass correlation coefficients, Bland Altman graphs, and Cronbach’s alpha. Concurrent convergent validity was evaluated by comparing the ND10 to the NDI, Single Assessment Numeric Evaluation (SANE), and Disabilities of the Arm, Shoulder and Hand (DASH). Known group validity was determined by comparing ND10 scores from patients, who rated their neck as more or less than 1/2 of “normal” on the SANE, using t-tests.
Results
The ND10 requires respondents to make rational judgements about their neck-related body function and disability. It has high internal consistency (0.94) and re-test reliability (0.87; SEM = 3.2/100; MDC = 7.5); and no re-test bias (mean re-test difference of 0.6). It followed expected correlation patterns, being highly correlated with related multi-item PROMs (r = 0.85–0.91), and moderately correlated to the single-item SANE. More patients agreed that the ND10 was easily readable than did so for the NDI (84% vs 68%; p < 0.05). All the PROMs distinguished the patients who perceived themselves as being abnormal/normal defined by a dichotomized SANE (p < 0.01).
Conclusion
The ND10 is reliable and valid for measuring neck-related functional disability. Longitudinal and cross-cultural translation studies are needed to support future use.
Similar content being viewed by others

Introduction
Neck pain is one of the most common musculoskeletal disorders with one third of all adults experiencing it during the course of one year, and 70% doing so over the course of their lifetime [1]. The severity of disability can range from minor to severely debilitating and the natural history is characterized by episodic reoccurrence [2, 3]. Radiologic [4] or physiologic measures [5] rarely explain neck pain. As a result, accurate measurement of symptom severity and functional disability is essential to targeting treatment and evaluating treatment outcomes. Systematic reviews indicate that baseline pain and disability are the most potent prognostic indicators of future pain and disability outcomes [6, 7].
Musculoskeletal health outcome measures are commonly used to evaluate symptoms, disability, and quality of life, and how this change following an intervention. Neck disorders can cause pain [8, 9]; and disturbances in joint motion [10, 11], sensory function [12,13,14,15], proprioception [16, 17], motor function [18,19,20], coordination [5, 21], posture [22, 23], and balance [23, 24]. These can lead to functional disability [2, 25, 26], participation restrictions [27], reduced work capacity [28,29,30], and lower quality of life [31, 32]. There are a variety of impairment and disability measures that have been designed to assess these different constructs [23, 33,34,35,36,37,38]. A survey of international practice patterns of clinicians with respect to assessing the outcomes for patients with neck pain indicated that the Numeric Pain Rating Scale (NPR) (a single item on pain [37]), the Neck Disability Index (NDI), and the Disabilities of the Arm, Shoulder and Hand (DASH) (developed for upper extremity [39]) are the patient-reported outcome measures (PROMs) most commonly used by clinicians [40].
The two primary features of musculoskeletal conditions, including neck disorders, are pain and disability. Content validity of PROMs requires a clear conceptual foundation with a defined construct [41, 42]. Increasingly, there have been moves to define conceptual frameworks for identification of core constructs as a preliminary step to improving measurement in the field of musculoskeletal disability. A recent international consensus panel [43] identified 6 core domains for whiplash-associated disorders: Physical Functioning, Perceived Recovery, Work and Social Functioning, Psychological Functioning, Quality of Life, and Pain. Many existing measures have not adequately defined a single construct, but rather sample across multiple constructs or domains within a global construct or health condition. A recent international outcome measure core set consensus panel for whiplash disorders concluded that “the content validity of these PROMs has yet to be established… and until this is undertaken, it is not possible to recommend 1 PROM over the other” [35]. Commonly, PROMs for musculoskeletal conditions include items on pain and function and compute total scores—as if these items reflect a single construct. Combining symptoms and disability in a single score from PROMs may not be justifiable on psychometric rounds since these may not represent a single construct. Furthermore, combining different scores together may undermine clinical reasoning or research hypothesis testing since being able to differentiate the impact of interventions on specific constructs is critical to problem-solving and hypothesis testing. Where adequate content validity is not present, measures do not provide accurate information about what aspect of patient status is changing over time [44]. Content validity is a prerequisite to other psychometric properties like factor validity and unidimensionality [45]. Finally, consensus panels have verified that pain and disability are separate constructs that are important core outcomes in health conditions causing neck pain [43].
A variety of PROMs have been previously established. The most of commonly used is the NDI developed by Vernon and Mior [46]. It was constructed based on 5 items adapted from the Oswestry Low Back Pain Index (OLBPI) and an additional 5 new items [46]. The developer published a summary paper in 2008 summarizing a 17-year history with the NDI [47], reflecting its position as the earliest and most commonly used neck-specific PROM. Systematic reviews of the measurement properties of the NDI concluded that there was a deep pool of evidence supporting the NDI as being reliable and responsive, but found validity concerns about the factor structure, and relevance given the number of items left missing in certain populations [33, 48]. Although the NDI is used as if it provides interval-level scaling, Rasch analyses indicate that is not achievable with the original measure [49,50,51]. Further, there are substantial differences between the 2 proposed Rasch-based scoring version and the original [52]. A variety of neck-related PROMs have been developed subsequently. An overview of neck-related PROMs [48] found that more limited research on the other neck-related measures: Northwick Park Neck Pain Questionnaire (20 items), Copenhagen Neck Functional Disability Scale (15 items), Neck Bournemouth Questionnaire (7 items), and Neck Pain and Disability scale (20 items).
Construct clarity is important in outcome evaluation. International consensus has concluded that functional disability is an important construct for assessing outcomes in neck-related health problems [43]. However, the wording of many of the current neck PROM items suggests that they measure neck-related pain interference–how much neck pain interferes with function. Pain interference and disability are related but different constructs. It may be problematic when PROMs conflate pain and function or do not specify what they are measuring is pain interference. This construct ambiguity might explain why some factor analyses studies indicate that the NDI contains 2 factors [53,54,55,56]. This is further supported by qualitative studies of experts and patients who suggest that the NDI measures more than physical functioning [44]. Since physical functioning is 1 of the core constructs agreed upon by an international panel [43], a measure that focuses solely on function/disability for people with neck conditions is needed. A recent review of disability measures for whiplash concluded that “the content validity of these PROMs has yet to be established…, and until this is undertaken, it is not possible to recommend 1 PROM over the other for inclusion in (core outcome measure sets)” [35].
Although there are several PROMs used for patients with neck pain, there is no measure that limits its focus to functional disability. Some neck-related PROMs measure symptoms, functional disability, pain interference, and/or quality of life [48]. Surveys [40, 57] suggest that the DASH is frequently used to measure the upper extremity-related components of neck pain which are not covered by the NDI, despite the fact that the DASH was not developed for this purpose. The importance of the upper extremity in neck-related functional disability was emphasized by qualitative studies which found that this was an important component of neck symptoms and disability from the patient perspective [27]. Lab-based studies have demonstrated altered upper extremity neuromuscular functioning in people with neck pain [21], which confirms the importance of considering upper extremity functioning in neck conditions.
The lack of sufficient involvement of patients with neck pain in developing some of the early neck-specific PROMs may have contributed to important gaps in the scope of symptoms or disability included on the NDI. Content validity requires that during development and validation the relevance of items be assessed with respect to the target population [41]. When PROMs fail to address important elements or the full scope of a construct, then content validity is inadequate, regardless of whether the measure demonstrates adequate quantitative psychometric properties.
Therefore, the purpose of this paper is to report the development and validation of a PROM that is designed to measure neck-related disability in patients with neck pain/disorders. Specific objectives are to describe the development process, content validity, readability, potential for floor/ceiling effects, test–retest reliability, and construct validity.
Methods
Scale conceptual definition
The Neck Disability 10 (ND10) was developed based on analyzing gaps in current neck PROMs using qualitative studies with patients living with neck pain and quantitative studies on neck disability. Guiding principles were developed to avoid problems identified in previous PROMs that measure the construct of neck-related disability:
-
1)
The items should focus on the single construct of neck-related disability.
-
2)
Valid legacy constructs of neck-related disability from prior PROMs could be retained if they were confirmed by patients as being relevant and re-worded for clarity as needed.
-
3)
New salient items from patient-based qualitative or quantitative studies were added to the item pool to address gaps in current PROMs.
-
4)
Health literacy, potential for translation across groups/cultures, and cognitive burden were considered in item bank refinement and decisions on format.
The ND10
After iterative item selection with patients and experts, mapping legacy, and new items in the item pool, and pilot testing of items, the final version of the ND10 is presented as Supplementary File 1. The ND10 is a 10-item scale that measures neck-related disability. Each item is scored on a scale from zero (no difficulty) to 5 (unable to do at all). The scale is scored calculating a percentage out of 100 (if no missing items, then total score can be multiplied by 2). If items are missing, the total score is calculated as a percentage to range from 0–100 points. The rationale for remediated legacy items and new items from the iterative consultative steps to refine the item bank to the final set of items is summarized in Table 1.
Comparison study measures
The Neck Disability Index (NDI)
The NDI is a 10-item PROM that assesses neck-related pain interference with function [33, 46, 48]. It was expected to be concordant with the ND10 based on specificity to neck disorders. Two Rasch-based versions of the NDI exist and show systematic differences from the traditional ordinal NDI [52]. The NDI-5 is a Rasch-based, 5-item version of the NDI [50] developed to focus on the subset of NDI items that address function and provide interval-level scaling and was selected as most comparable in the intended construct: neck-related disability. NDI-5 scores can be represented two ways: as a raw score and using the Rasch-based transformation that provides interval-level scaling.
The Quick Disabilities of the Arm, Shoulder and Hand (QDASH)
The QDASH is an 11-item measure of upper extremity symptoms and disability. It was selected as a comparator as it has been shown to be salient to people with neck disorders [58], since patients report that neck pain and/or upper extremity movement affects their neck pain [27]. Since upper extremity items were one of the gap areas identified in qualitative research [27], it was seen as important to consider this construct.
The Single Assessment Numeric Evaluation (SANE) for neck
The SANE is a single global item [61], first reported for use to evaluate function in patients with knee problems, and subsequently applied to a variety of health conditions and body areas [36, 62]. The patient responds to “how would you rate your (body area) today as a percentage of normal (0% to 100% scale with 100% being normal)”. It has been validated for multiple musculoskeletal conditions [61, 63,64,65,66,67]. Based on previous studies we expected a moderate relationship between the ND10 and the SANE [62, 63].
Patient recruitment
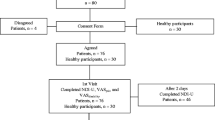
Patients with neck pain were recruited through physiotherapy clinics. Exclusion criteria included lack of ability to complete questionnaires in English. The study was approved by the Hamilton Integrated Research Ethics Board and all respondents provided informed consent.
Data collection
Respondents completed the full version of the ND10, DASH, and the NDI on a single occasion. For the test–retest data, the respondents were asked to complete the ND10 for a second test occasion and return the survey within 14 days. The SANE was also completed on the second test occasion. The NDI-5 and NDI-5 T were extracted from the full NDI, and the Rasch scoring applied [50]. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. A talk-aloud approach cognitive interview with follow-up probes approach was used to explore respondents’ perceptions of individual items [68] in 15 patients.
Analyses
Content validity
Content validity was integrated in the development process and informed revisions of the items. New items were derived from the published qualitative and quantitative literature on the experience of neck disability, including a specific qualitative study designed to assess the experience of neck pain and its contributors [27]. Iterative feedback was obtained from people living with neck pain and measurement experts to revise the items to ensure clarity. Structured content analysis of the final version of the ND10 was performed using 3 methods. The content of the ND10 was compared to other neck-related PROMs that have been reported in the literature. Secondly, the International Classification of Functioning Disability and Health (ICF) linking procedures were used to code item content according to established linking rules [41, 69, 70] to specific ICF codes. ICF linking provides a mechanism to communicate content in a common international language and is particularly salient to measures of disability. Item linking was performed by 2 raters, using updated rules that include perspective and response options. Item Perspective Classification (IPC) was used to classify the nature of the decisions made in responding to individual items [71]. A two-level IPC was used which focuses on whether it was a rational or emotional judgement; and if the question addressed psychological, social, biological, or inorganic issues/content.
Scale distributions and floor/ceiling
Box plots were used to examine the distribution of scores for individual items and subscales. We adopted the commonly used 15% threshold for patients achieving the highest and lowest score to define a ceiling and floor effect (i.e., scores of 0–10 and 90–100).
Reliability and Agreement
The following statistics were calculated:
-
a)
Internal consistency
-
b)
Reliability: intraclass correlation coefficients (ICC) (2,1) [72]
-
c)
Agreement: Bland and Altman graphs to determine potential bias (mean difference across test occasions) and limits of agreement [73, 74]
-
d)
Standard error of measurement and minimal detectable change (90% confidence)
Construct validity
The following hypotheses were constructed to assess construct validity. The expected relationships were then assessed using Pearson correlations.
-
1.
The ND10 should demonstrate high correlation (i.e., convergent validity indicated by r > 0.75) with the NDI, NDI-5, and DASH, given conceptual concordance and prior research demonstrating correlations between the NDI and DASH.
-
2.
The SANE would correlate moderately with the ND10, given that it is the single item rating of “normality” and expected to be less directly related to the construct in a multi-item neck disability measure.
-
3.
The people who see themselves as less than 50% “normal” on the SANE will have higher ND10 scores (discriminative, known-groups validity).
Patients’ preferences
Patients’ preferences were addressed by questions completed immediately after completing the NDI and ND10 (random order). Patients were questioned about the clarity and relevance of the two questionnaires.
Results
The ND10 was developed as a 10-item functional scale for patients with disorders of the neck. The final version is presented with scoring instructions as Supplementary File 1. Characteristics of participants in the validation studies are listed in Table 2 and indicate a 75/25 female imbalance in gender distribution.
Content validity
Item content comparison of neck-related PROMs indicate some common functional items across six neck-related PROMs (e.g., personal care, driving, lifting, sleep, and work) ask how neck pain influences function rather than purely rating functional difficulty/ability (Table 3). Some of the PROMs have more emphasis on physical symptoms like motion or paresthesia, or mental symptoms like anxiety or depression. Other PROMs include other constructs like social functioning, medication use, or attitudes about the future.
ICF/IPF codes and item content validity coding for the ND10 are presented in Table 1. IPF codes indicated that 100% of the items involved rational decision; 5 (half) of the items focused on the biological domain; 3 psychological; 1 social; and 1 on inorganic content. The ICF linking revealed that all ND10 items were linked to unique ICF codes: 2 of the items linked to body functions (sleeping, concentration), while the remaining 8 items were linked to disability codes. Disability items mapped to changing body position, self-care, and major life areas; with the level of precision varying across items.
Mixed methods assessment of ND10 and NDI by patients
Of the 78 patients completing both the NDI and the ND10, a greater number strongly agree that the ND10 was easy to read when compared to the NDI (84% versus 68%; p < 0.05). There was strong or moderate agreement that both measures were “easy to read”, 94% for the NDI and 98% for the ND10. Similar numbers strongly agreed that the NDI and ND10 contain relevant content (48% versus 45%); with overall rating of item relevance being higher for the ND10 (90%) versus the NDI (84%) (p < 0.05). More people found the ND10 easy to answer in comparison to the NDI: 72% versus 66% strongly agreed (NS), and 96% versus 86% agreed (p < 0.05). Some respondents reported that response options did not make sense to them—this was reported by 8% for the NDI and 4% for the ND10. Neither questionnaire was seen as providing undue burden to patients since 82% of respondents reported that the NDI was the right length, and 14% said it was too short. Similarly, 74% reported that the ND10 was the right length and 18% said it was too short.
A substantial number of patients (43% for the NDI and 48% the ND10) reported that these measures did not ask enough about the impact of their neck pain on their life.
Cognitive interview findings
The specific comments raised by respondents are listed in Supplementary File 2. Several themes arose in these comments. Respondents identified multiple issues that were important to them, but that were not covered on the questionnaires. Many respondents noted that specific impairments, such as movement or strength, were not being assessed. These concerns about the need to consider other constructs reflect that this study focused on evaluating specific functional PROMs—and were not taken as problems with the PROMs themselves.
Similarly, many respondents noted that specific types of pain or sensory disturbance were not assessed by one or both measures. Several respondents noted the importance of numbness/tingling, and that these symptoms were bothersome, but not painful. Another domain that respondents noted as being absent was social function. Things like intimacy, relationships, finances, etc. were relevant impacts that were not addressed by either the NDI or ND10. For the ND10 these would be outside the defined construct of functional disability, but important considerations for quality of life. Interestingly these items do appear on some of the other PROMs in Table 3, but this was deemed problematic in terms of construct clarity and unidimensionality.
Many respondents noted that their disability issues had changed over time, and that this may have affected how they calibrated items. Reducing or replacing recreation or work activities to avoid pain were cited as examples. Some relayed that they experienced deterioration in status after their initial recovery, and these temporal changes made it challenging to answer questions, or to have confidence that PROMs adequately reflect their experience with neck pain. Many respondents noted that the items did not reflect the complexity of their neck problem.
The main specific concern raised about the items that did fit within the construct of disability was about response options. There were multiple respondents who found the response options on the NDI difficult to understand, not descriptive of their status, or to contain conflicting options. Conversely, while this complaint did not occur on the ND10, a few respondents noted that the response options were less defined which made it difficult for them to calibrate. This reflects the different approaches on the two measures. The NDI has detailed response options that are often double-barreled or not mutually exclusive, whereas the ND10 has simple anchors that are used for all items, but there is no clarification of how to define “a little” or “moderate”. This contrast was noted by patients.
Item distributions and floor/ceiling effects
There were no ceiling effects for either the ND10, NDI, QDASH, or NDI-5 as none of the patients scored 90 or higher on any of the measures. There were minor concerns about floor effects as the percentage in the bottom 10% was 8%, 18%, 11%, and 23%, respectively. The NDI and NDI-5 exceeded the floor threshold set at 15%. The box plots reflect a similar mean score estimation across the different instruments, with wide confidence intervals excepting the Rasch-transformed version of the NDI-5 (Fig. 1).

Score Distributions for studied PROMs (/100)
Reliability/agreement
The internal consistency of the ND10 was 0.93. The ICC for re-test reliability was 0.87 (95% CI 0.76 – 0.93). The Bland and Altman plot indicated minimal bias between test and re-test of the ND10 (0.6 mean difference) with Limits of Agreement (18.6 to—17.4). See Additional file 3: Supplemental Figure A for the Bland and Altman graphs. The SEM was 3.2 and the MDC90 was 7.5.
Construct validity
Correlations followed constructed hypotheses in that the ND10 was strongly correlated with other measures of neck and arm pain and disability (NDI, NDI-5, DASH) and moderately related to the SANE (Table 4).
The constructed hypothesis was supported indicating that the ND10 and the other measures were highly discriminative between patients who rated themselves as more or less than 50% of normal (Table 5).
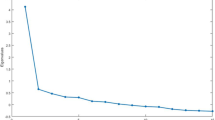
Structural validity (factor analysis)
All items loaded on one factor explaining 65% of the variance with a clear demarcation of one factor in the SCREE plot (Fig. 2).

ND10 scree plot
Discussion
This study provides evidence that the ND10 can provide understandable, relevant, reliable, structurally sound, and discriminative scores representing neck-related disability. While there are multiple PROMs that could be used for people with neck pain, the uniqueness of the ND10 is that it was developed to solely focus on neck-related functional disability, whereas other commonly used measures combine symptoms, pain interference, and other constructs within a single scale. We used iterative quantitative and qualitative work to establish the content validity and usability of the ND10. Content validity analyses was studied using item comparison, classification in ICF and perspective, patient questionnaires and cognitive interviews; and these findings were triangulated during development. The conceptual clarity of the construct being measured, and its constituent items may be the most critical aspect of ND10 development, and is an aspect most sparsely attended to in development of many other neck-related PROMs. COSMIN (COnsensus-based Standards for the selection of health Measurement Instruments) has recently provided more detail highlighting the importance of rigor in content validity [45] and development of item content coding and cognitive interviewing methods provides enhanced methodological support [41].
Although the other PROMs used in the study performed well from a quantitative psychometric view, concerns about content validity of the other neck-related PROMs were apparent in the lack of clear construct definition since items crossed multiple domains and often focused more on pain interference than function. From a health literacy perspective, the readability and relevancy were better than the NDI, and the preference of patients were favourable. Thus, the ND10 may be preferable for clinicians or researchers who wish to distinguish construct of function and pain as recommended by core outcome recommendations [75]. It may also be easier for patients to complete—this is important given the extent to which health literacy is a problem in many clinical contexts. With the move towards identifying core sets of constructs to be measured in musculoskeletal research and practice, the importance of separating pain and disability in separate constructs has become clearer [75,76,77]. Overall, the ND10’s psychometric properties were better than other neck-related PROMs in terms of establishing a clear conceptual construct and focusing in functional (dis)ability. It was better than the NDI in terms of patient relevance and health literacy and in avoiding floor effects. The ND10 was similar to the NDI and DASH in terms of its convergent association with other measures and ability to discriminate between known groups. Preliminary factor analysis, based on one sample, supported that the ND10 is unidimensional, which has been problematic in other neck-related PROMs including the NDI [33].
An outcome measure which focuses distinctly on disability can be important where it is the focus of a specific treatment or a specific discipline, e.g., rehabilitation. For example, in patients with chronic pain, treatment programs often target improved function without an expectation of substantial improvements in pain [78]. The development of the ND10 was not to diminish the importance of pain as an outcome measure. Conversely, we think that a brief functional neck-specific measure, like the ND10, allows space in patient contact time for a more thorough multi-dimensional pain assessment using a valid pain-specific outcome measure.
Our findings suggest that some of the limitations in previous measures that we hoped to address were successfully mitigated in our new outcome measure. Our prior work indicated the importance of the upper extremity [27, 58] in neck disorders, concerns about high rates of missingness items due to relevancy issues for some items [79], and the importance of considering health literacy during development. Our qualitative interviews indicated the most consistent concern with the NDI was a lack of clarity in the response options. The previous neck PROMs compared at a content level in Table 3 have response options that are longer, have a great cognitive burden, and are sometimes double-barreled or not mutually exclusive. These issues were commonly noted by patients as reasons that it was difficult to calibrate their responses to the NDI in our cognitive interviews. We designed the ND10 to be very simple and brief (118 words on ND10 versus 783 on ND1). Health literacy and cognitive burden are partially related to the number and complexity of words, but also to the format in which information is presented. Therefore, our use of a consistent response options and icons to represent direction were used to improve health literacy. A few of the respondents noted that the ND10 response options being brief meant that they were more open to interpretation. This is inevitable given the choices made for a streamlined format.
Some ND10 items reflect important issues raised by patients in qualitative interviews and surveys [27, 58] that were not included on the NDI, e.g., lifting and carrying a heavy object, putting something on a high shelf, and overhead work. These items create different types of strain on the neck and represent common tasks of daily life. Other issues we encountered during development indicate that items may have a “shelf-life”. For example, the NDI which was developed more than 2 decades ago asks patients about difficulty reading a book. However, many people now primarily read electronic devices. Although the way people read has changed, the ability to read and communicate with text remains an important human function. Therefore, our rewording of a reading item was designed to be more inclusive of different ways that this function is performed. One of the problematic items due to high rates of missingness on the NDI item is the driving item [33, 56]. Driving tends to leave out specific segments of the population, e.g., in some countries women are not allowed to drive; lower income people may not be able to afford vehicles; age restrictions may limit who can drive; and people with comorbidities may have medical reasons for not being allowed to drive. Thus, the driving item inherently represents a form of selection bias. However, the ability to move around in society is an important human function, and many forms of transportation can be difficult for patients with neck disorders. Therefore, this item was included in a more inclusive format by using “drive or ride” and different modes of transportation as exemplars.
Patients did not indicate concerns about the burden of either the NDI or the ND10, and some felt these PROMs were too short. Patients in a qualitative study [27] and our cognitive interviews wanted PROMs to reflect the full scope of the problems they experience. Several patients commented that the measures did not tap into important impacts of their life. Some of these issues were outside of the target construct of functional disability. This indicates the importance of using multiple PROMs to reflect the different constructs important to patients, particularly when these have been defined by core sets [43]. For example, mental symptoms and social/emotional functioning are important but should be measured in separate well-validated PROMs specific to those constructs. Patients in this study may not have understood that typically we would be measuring a larger suite of PROMs within a clinical study or clinical interaction. CATWAD (Core Outcome Domain Set For Whiplash-Associated Disorders) distinguished pain, recovery, and functional disability as separate constructs [43]. Several issues raised by patients reflected recovery or other domains within quality of life. The Satisfaction and Recovery Index [59, 80] is an example of a measure designed to measure recovery following musculoskeletal trauma. Many of the issues that patients raised as missing constructs from the ND10 and NDI fell within the construct measured on The Satisfaction and Recovery Index (e.g., intimacy, life roles). Patient interviews conducted in this study confirm CATWAD findings about the importance of considering both functional disability status and perceived recovery.
We observed that some patients had unique concerns that they felt were important to communicate, but that were not represented on any of the PROMs evaluated. No outcome measure can capture all issues important to every patient. Patients wanted clinicians to understand the complexity of their neck pain. Listening to patients helped us recognize the importance of allowing space to express individual issues qualitatively when responding on an outcome measure. Therefore, we added an open text box to the ND10 where patients can communicate what they want others to know. Although this does not contribute to the score, it is potentially useful in clinical practice since one of the important consequences of implementing outcome measures should be better communication with patients.
The reliability of the ND10 of 0.87 was high, even though the re-test interval was relatively long for some participants (mean 8.5 days; range 4–25) and did not exclude people under treatment. We attribute this to the measure itself and the chronic nature of the patient’s neck disorder. A minimal detectable change of 7.5 points compares favorably with other PROMs. We speculate that test–retest reliability can be influenced by the re-test interval, the acuity of the condition, and the extent to which the construct being measured is stable and definable by patients. We anticipate that future studies that more rigorously assess whether patients have remained stable and use more consistent test–retest intervals might find an even higher reliability coefficient.
The development of a new PROM is justified when there are no PROMs for an important construct or there are serious flaws in existing PROMs. These rationales apply for the ND10 development since previous PROMs lack conceptual clarity, content validity, or failed to adequately incorporate patient perspectives. The ND10 addresses a core construct recommended by an international consensus as being important for patients with neck pain [43]. Despite all of these favourable findings, we recognize it can be difficult to transition to a new PROM. Although there are conceptual flaws with existing neck PROMs, their long-standing use—particularly with respect to the NDI—means that legacy measures have pools of comparative data and familiarity, which may make some people reluctant to change their current usage patterns.
Although this study reports the findings of a multi-stage process, there are limitations in our work. We did not provide the full suite of psychometric evidence. Important future investigations include fit to the Rasch model and responsiveness studies; as well as widespread cross-cultural translation. Although we found excellent reliability and factor structure, the sample sizes were relatively small for these analyses, and future studies in larger samples are needed for greater precision and confidence. A clear understanding of utility of any new PROMs only becomes apparent over time after it has been tested in multiple contexts and populations.
Conclusions
This study led to the development of a reliable and valid measurement PROM, the ND10, designed specifically for assessing neck-related functional disability. Overall, the findings are supportive of the content validity and suggest strong clinical measurement properties. The ND10 is provided by open access from the developer/copyright owner (J MacDermid: jmacderm@uwo.ca at https://www.lawsonresearch.ca/hulc/outcome-measures) so that it is freely available for use where a simple measure of function is needed for patients with neck pain or disability. It should be used in combination with a pain scale and measures of other salient constructs to reflect multiple aspects of health outcomes and quality of life.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request. The data are not publicly available due to ethical and privacy restrictions.
Abbreviations
- CATWAD:
-
Core Outcome Domain Set for Whiplash-Associated Disorders
- COSMIN:
-
COnsensus-based Standards for the selection of health Measurement Instruments
- DASH:
-
Disabilities of the Arm, Shoulder and Hand
- ICC:
-
Intraclass correlation coefficients
- ICF:
-
International Classification of Functioning, Disability and Health
- IPC:
-
Item Perspective Classification
- ND10:
-
Neck Disability 10 (10-item measure of neck-related disability)
- NDI:
-
Neck Disability Index
- NPR:
-
Numeric Pain Rating Scale
- OLBPI:
-
Oswestry Low Back Pain Index
- PROMs:
-
Patient-reported outcome measures
- QDASH:
-
Quick Disabilities of the Arm, Shoulder and Hand
- SANE:
-
Single Assessment Numeric Evaluation
References
Croft PR, Lewis M, Papageorgiou AC, Thomas E, Jayson MIV, Macfarlane GJ, et al. Risk factors for neck pain: a longitudinal study in the general population. Pain. 2001;93:317–25.
Côté P, Cassidy JD, Carroll LJ, Kristman V. The annual incidence and course of neck pain in the general population: a population-based cohort study. Pain. 2004;112:267–73.
Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24:783–92.
Rudy SS, Poulos A, Owen L, Batters A, Kieliszek K, Willox J, et al. The correlation of radiographic findings and patient symptomatology in cervical degenerative joint disease: a cross-sectional study. Chiropr Man Ther. 2015;23:9.
MacDermid JC, Gross AR, Galea V, McLaughlin LM, Parkinson WL, Woodhouse LJ, et al. Developing biologically-based assessment tools for physical therapy management of neck pain. J Orthop Sports Phys Ther. 2009;39(5):388–99.
Walton DM, Pretty J, MacDermid JC, Teasell RW. Risk factors for persistent problems following whiplash injury: results of a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2009;39(5):334–50.
Walton DM, MacDermid JC, Giorgianni AA, Mascarenhas J, West SCSC, Zammit CACA. Risk factors for persistent problems following acute whiplash injury: update of a systematic review and meta-analysis. J Orthop Sport Phys Ther. 2013;43:31–43.
Sterling M, Pedler A. A neuropathic pain component is common in acute whiplash and associated with a more complex clinical presentation. Man Ther. 2009;14:173–9.
Kamper SJ, Rebbeck TJ, Maher CG, McAuley JH, Sterling M. Course and prognostic factors of whiplash: a systematic review and meta-analysis. Pain. 2008;138(3):617–62.
Prushansky T, Dvir Z. Cervical motion testing: methodology and clinical implications. J Manipulative Physiol Ther. 2008;31:503–8.
Ernst MJ, Crawford RJ, Schelldorfer S, Rausch-Osthoff A-K, Barbero M, Kool J, et al. Extension and flexion in the upper cervical spine in neck pain patients. Man Ther. 2015;20:547–52.
Chien A, Sterling M. Sensory hypoaesthesia is a feature of chronic whiplash but not chronic idiopathic neck pain. Man Ther. 2010;15:48–53.
Hübscher M, Moloney N, Leaver A, Rebbeck T, McAuley JH, Refshauge KM. Relationship between quantitative sensory testing and pain or disability in people with spinal pain - a systematic review and meta-analysis. Pain. 2013;154:1497–504.
Sterling M. Testing for sensory hypersensitivity or central hyperexcitability associated with cervical spine pain. J Manipulative Physiol Ther. 2008;31:534–9.
Uddin Z, MacDermid JC, Galea V, Gross AR, Pierrynowski MR. The current perception threshold test differentiates categories of mechanical neck disorder. J Orthop Sport Phys Ther. 2014;44:532–40.
Knox JJ, Beilstein DJ, Charles SD, Aarseth GA, Rayar S, Treleaven J, et al. Changes in head and neck position have a greater effect on elbow joint position sense in people with whiplash-associated disorders. Clin J Pain. 2006;22:512–8.
de Vries J, Ischebeck BK, Voogt LP, van der Geest JN, Janssen M, Frens MA, et al. Joint position sense error in people with neck pain: a systematic review. Man Ther. 2015;20(6):736–44.
Falla D, Jull G, Rainoldi A, Merletti R. Neck flexor muscle fatigue is side specific in patients with unilateral neck pain. Eur J Pain. 2004;8:71–7.
Jull G, Kristjansson E, Dall’Alba P. Impairment in the cervical flexors: a comparison of whiplash and insidious onset neck pain patients. Man Ther. 2004;9:89–94.
O’Leary S, Jull G, Kim M, Vicenzino B. Cranio-cervical flexor muscle impairment at maximal, moderate, and low loads is a feature of neck pain. Man Ther. 2007;12:34–9.
Galea V, Pierrynowski M, MacDermid J, Gross A. Upper limb neuromuscular strategies are altered in patients with mechanical neck disorders compared with asymptomatic volunteers. Crit Rev Phys Rehabil Med. 2012;24:69–84.
Silva AG, Punt TD, Sharples P, Vilas-Boas JP, Johnson MI. Head posture and neck pain of chronic nontraumatic origin: a comparison between patients and pain-free persons. Arch Phys Med Rehabil. 2009;90:669–74.
Humphreys BK. Cervical outcome measures: testing for postural stability and balance. J Manipulative Physiol Ther. 2008;31:540–6.
Silva AG, Cruz AL. Standing balance in patients with whiplash-associated neck pain and idiopathic neck pain when compared with asymptomatic participants: A systematic review. Physiother Theory Pract. 2012;29(1):1–18.
Hoy D, March L, Woolf A, Blyth F, Brooks P, Smith E, et al. The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1309–15.
Carroll LJ, Hogg-Johnson S, van der Velde G, Haldeman S, Holm LW, Carragee EJ, The Burden and Determinants of Neck Pain in the General Population, et al. Results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manipulative Physiol Ther. 2009;32:S83-92.
MacDermid JC, Walton DM, Bobos P, Lomotan M, Carlesso L. A qualitative description of chronic neck pain has implications for outcome assessment and classification. Open Orthop J. 2016;10:746–56.
Côté P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, The Burden and Determinants of Neck Pain in Workers, et al. Results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manipulative Physiol Ther. 2009;32:S70-86.
Buckle PW, Jason DJ. The nature of work-related neck and upper limb musculoskeletal disorders. Appl Ergon. 2002;33(3):207–17.
Côté P, Kristman V, Vidmar M, Van Eerd D, Hogg-Johnson S, Beaton D, The Prevalence and Incidence of Work Absenteeism Involving Neck Pain, et al. A Cohort of Ontario lost-time claimants. J Manipulative Physiol Ther. 2009;32:S219-26.
Carlesso LC, Walton DM, MacDermid JC. Reflecting on whiplash associated disorder through a QoL lens: an option to advance practice and research. Disabil Rehabil. 2012;34:1131–9.
Nolet PS, Côté P, Kristman VL, Rezai M, Carroll LJ, Cassidy JD. Is neck pain associated with worse health-related quality of life 6 months later? A population-based cohort study. Spine J. 2015;15:675–84.
MacDermid JC, Walton DM, Avery S, Blanchard A, Etruw E, McAlpine C, et al. Measurement properties of the neck disability index: a systematic review. J Orthop Sports Phys Ther. 2009;39:400–17.
Pietrobon R, Coeytaux RR, Carey TS, Richardson WJ, DeVellis RF. Standard scales for measurement of functional outcome for cervical pain or dysfunction: a systematic review. Spine (Phila Pa 1976). 2002;27:515–22.
Griffin AR, Leaver AM, Arora M, Walton DM, Peek A, Bandong AN, et al. Clinimetric properties of self-reported disability scales for whiplash: a systematic review for the whiplash core outcome Set (CATWAD). Clin J Pain. 2021;37:766–87.
Bobos P, MacDermid J, Nazari G, Furtado R. Psychometric properties of the global rating of change scales in patients with neck disorders: a systematic review with meta-analysis and meta-regression. BMJ Open. 2019;9(11):e033909.
Modarresi S, Lukacs MJ, Ghodrati M, Salim S, MacDermid JC, Walton DM. A systematic review and synthesis of psychometric properties of the numeric pain rating scale and the visual analog scale for use in people with neck pain. Clin J Pain. 2022;38:132–48.
McGee S, Sipos T, Allin T, Chen C, Greco A, Bobos P, et al. Systematic review of the measurement properties of performance-based functional tests in patients with neck disorders. BMJ Open. 2019;9(11):e031242.
Beaton DE, Katz JN, Fossel AH, Wright JG, Tarasuk V, Bombardier C. Measuring the whole or the parts? J Hand Ther. 2001;14(2):128–46.
MacDermid JC, Walton DM, Côté P, Santaguida PL, Gross A, Carlesso L. Use of outcome measures in managing neck pain: an international multidisciplinary survey. Open Orthop J. 2013;7:506–20.
MacDermid JC. ICF Linking and cognitive interviewing are complementary methods for optimizing content validity of outcome measures: an integrated methods review. Front Rehabil Sci. 2021;2:702596.
Manchaiah V, Granberg S, Grover V, Saunders GH, Ann HD. Content validity and readability of patient-reported questionnaire instruments of hearing disability. Int J Audiol. 2019;58:565–75.
Chen K, Andersen T, Carroll L, Connelly L, Côté P, Curatolo M, et al. Recommendations for core outcome domain set for whiplash-associated disorders (CATWAD). Clin J Pain. 2019;35:727–36.
Ailliet L, Knol DL, Rubinstein SM, De Vet HCW, Van Tulder MW, Terwee CB. Definition of the construct to be measured is a prerequisite for the assessment of validity. the Neck Disability Index as an example. J Clin Epidemiol. 2013;66:775–82.
Terwee CB, Prinsen CAC, Chiarotto A, Westerman MJ, Patrick DL, Alonso J, et al. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual Life Res. 2018;27:1159–70.
Vernon H, Mior S. The neck disability index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14:409–15.
Vernon H. The Neck Disability Index: state-of-the-art, 1991–2008. J Manipulative Physiol Ther. 2008;31(7):491–502.
Bobos P, MacDermid JC, Walton DM, Gross A, Santaguida PL. Patient-reported outcome measures used for neck disorders: an overview of systematic reviews. J Orthop Sports Phys Ther. 2018;48:775–88.
Hung M, Cheng C, Hon SD, Franklin JD, Lawrence BD, Neese A, et al. Challenging the norm: Further psychometric investigation of the neck disability index. Spine Journal. 2015;15(11):2440–5.
Walton DM, MacDermid JC. A brief 5-item version of the Neck Disability Index shows good psychometric properties. Health Qual Life Outcomes. 2013;11:108.
van der Velde G, Beaton D, Hogg-Johnston S, Hurwitz E, Tennant A. Rasch analysis provides new insights into the measurement properties of the neck disability index. Arthritis Rheum. 2009;61:544–51.
Lu Z, MacDermid JC, Nazari G. Agreement between original and Rasch-approved neck disability index. BMC Med Res Methodol. 2020;20:1–11.
Swanenburg J, Humphreys K, Langenfeld A, Brunner F, Wirth B. Validity and reliability of a German version of the Neck Disability Index (NDI-G). Man Ther. 2014;19:52–8.
Shaheen AAM, Omar MTA, Vernon H. Cross-cultural adaptation, reliability, and validity of the arabic version of neck disability index in patients with neck pain. Spine (Phila Pa 1976). 2013;38(10):E609-15.
Nakamaru K, Vernon H, Aizawa J, Koyama T, Nitta O. Crosscultural adaptation, reliability, and validity of the Japanese version of the Neck Disability Index. Spine (Phila Pa 1976). 2012;37(21):E1343-7.
Monticone M, Ferrante S, Vernon H, Rocca B, Dal Farra F, Foti C. Development of the Italian version of the neck disability index: Cross-cultural adaptation, factor analysis, reliability, validity, and sensitivity to change. Spine (Phila Pa 1976). 2012;37(17):E1038-44.
Kennedy CA, Beaton DE. A user’s survey of the clinical application and content validity of the DASH (Disabilities of the Arm, Shoulder and Hand) outcome measure. J Hand Ther. 2017;30:30–40.
Mehta S, MacDermid JC, Carlesso LC, McPhee C. Concurrent validation of the DASH and the QuickDASH in comparison to neck-specific scales in patients with neck pain. Spine (Phila Pa 1976). 2010;35:2150–6.
Walton DM, MacDermid JC, Pulickal M, Rollack A, Veitch J. Development and Initial Validation of the Satisfaction and Recovery Index (SRI) for measurement of recovery from musculoskeletal trauma. Open Orthop J. 2014;8:316–25.
Walton DM, MacDermid JC, Taylor T, ICON. What does “recovery” mean to people with neck pain? Results of a descriptive thematic analysis. Open Orthop J. 2013;7:420–7.
Williams GN, Taylor DC, Gangel TJ, Uhorchak JM, Arciero RA. Comparison of the single assessment numeric evaluation method and the Lysholm score. Am J Sports Med. 1999;27(2):214-21. https://doi.org/10.1177/03635465990270021701.
Furtado R, MacDermid JC. Single Assessment Numeric Evaluation. J Physiother. 2019;65(2):111.
Nazari G, Bobos P, Lu S, MacDermid JC. Psychometric properties of the single assessment numeric evaluation in patients with lower extremity pathologies. A systematic review. Disabil Rehabil. 2021;43(15):2092–9.
Lu Z, MacDermid JC, Rosenbaum P. A narrative review and content analysis of functional and quality of life measures used to evaluate the outcome after TSA: an ICF linking application. BMC Musculoskelet Disord. 2020;21:1–11.
Saad MA, Kassam HF, Suriani RJ, Pan SD, Blaine TA, Kovacevic D. Performance of PROMIS Global-10 compared with legacy instruments in patients with shoulder arthritis. J Shoulder Elb Surg. 2018;27(12):2249–56.
Jones IA, Togashi R, Heckmann N, Vangsness CT. Minimal clinically important difference (MCID) for patient-reported shoulder outcomes. J Shoulder Elb Surg. 2020;29:1484–92.
Nazari G, MacDermid JC, Bobos P, Furtado R. Psychometric properties of the Single Assessment Numeric Evaluation (SANE) in patients with shoulder conditions. A systematic review. Physiotherapy (United Kingdom). 2020;109:33–42.
Willis GB. C H A P T E R 2: Cognitive Interviewing Revisited: A Useful Technique, in Theory? Methods for Testing and Evaluating Survey Questionnaires. Eds(s): Presser S, Rothgeb JM, Couper MP, Lessler JT, Martin E, Martin J, Singer E. Hoboken: Wiley; 2004. https://doi.org/10.1002/0471654728.
Cieza A, Geyh S, Chatterji S, Kostanjsek N, Üstün B, Stucki G. ICF linking rules: an update based on lessons learned. J Rehabil Med. 2005;37:212–8.
Cieza A, Fayed N, Bickenbach J, Prodinger B. Refinements of the ICF Linking Rules to strengthen their potential for establishing comparability of health information. Disabil Rehabil. 2019;41:574–83.
Rosa D, MacDermid J, Klubowicz D. A comparative performance analysis of the international classification of functioning, disability and health and the item-perspective classification framework for classifying the content of patient reported outcome measures. Health Qual Life Outcomes. 2021;19:132.
Shrout PE, Fleiss JL. Intraclass correlations: Uses in assessing rater reliability. Psychol Bull. 1979;86:420–8.
Martin Bland J, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;327:307–10.
Mantha S, Roizen MF, Fleisher LA, Thisted R, Foss J. Comparing methods of clinical measurement: reporting standards for bland and altman analysis. Anesth Analg. 2000;90:593–602.
Chen K, Andersen T, Carroll L, Connelly L, Côté P, Curatolo M, et al. Recommendations for core outcome domain set for whiplash associated disorders (CATWAD). Clin J Pain. 2019;35(9):727–36.
Dworkin RH, Turk DC, Revicki DA, Harding G, Coyne KS, Peirce-Sandner S, et al. Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain. 2009;144(1–2):35–42.
Goldhahn J, Beaton D, Ladd A, MacDermid J, Hoang-Kim A. Recommendation for measuring clinical outcome in distal radius fractures: a core set of domains for standardized reporting in clinical practice and research. Arch Orthop Trauma Surg. 2014;134(2):197–205.
Miller J, MacDermid J, Walton DM, Richardson J. ChrOnic pain self-ManagementMent support with pain science EducatioN and exerCisE (COMMENCE) for people withchronic pain and multiple comorbidities: a randomized controlled trial. Arch Phys Med Rehabil. 2020;101(5):750–612020.
Mousavi SJ, Parnianpour M, Montazeri A, Mehdian H, Karimi A, Abedi M, et al. Translation and validation study of the Iranian versions of the Neck Disability Index and the Neck Pain and Disability Scale. Spine (Phila Pa 1976). 2007;32:E825-31.
Walton DM, MacDermid JC, Nielson W. Recovery from acute injury: clinical, methodological and philosophical considerations. Disabil Rehabil. 2010;32:864–74.
Acknowledgements
Joy MacDermid was supported by a Canada Research Chair in Musculoskeletal Health Outcomes and Knowledge Translation and the Dr James Roth Chair in Musculoskeletal Measurement and Knowledge Translation. The authors thank Margaret Lomotan for assistance with the study and manuscript preparation.
Funding
The study was funded by the Canadian Institutes of Health Research (FRN: SCA-145102).
Author information
Authors and Affiliations
Contributions
Joy MacDermid developed the ND10, obtained ethics, developed the study protocol, analyzed data, and wrote the first manuscript draft. David Walton co-authored qualitative studies and systematic reviews on, provided input into item selection, reviewed data analysis, and manuscript versions. The author(s) read and approved the final manuscript.
Authors’ information
Not applicable.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Hamilton Integrated Research Ethics Board (Project #13–300). All respondents provided informed consent.
Consent for publication.
Not applicable.
Competing interests
Authors have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary File 1. ND10 with scoring instructions.
Additional file 2:
Supplementary File 2. Record of patient comments about specific questionnaires in cognitive interviews and actions taken.
Additional file 3:
Supplemental Figure A. Bland-Altman graph demonstrating the mean difference in test and retest scores (0.6) and the limits of agreement (18.6 to -17.4).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
MacDermid, J.C., Walton, D.M. Development and validation of the ND10 to measure neck-related functional disability. BMC Musculoskelet Disord 23, 605 (2022). https://doi.org/10.1186/s12891-022-05556-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05556-7