
Abstract
Background
Several interventions are established for treating patellofemoral instability in adults. Fewer exist for pediatric patients without damaging the epiphysis. The Ali Krogius (AK) method is currently still being used. Most studies are not current and report varying results in small patient population. The aim of this study is to determine the long-term results of the AK method.
Methods
In this monocentric, retrospective study design, 33 knees in 33 patients who received the AK procedure for recurrent patellar dislocation were assessed. The average age was 20.8 years (range 6–40). The following functional scores were assessed: Kujala Score, Lysholm Score and Tegner Score. Subgroup analysis was done for patients ≤16 years of age. Available preoperative imaging was assessed for known risk factors.
Results
After an average follow-up of 7.8 years (Range 59–145 months), a total of 8 (24%) knees suffered a redislocation postoperatively. Seven of the eight dislocations occurred in patients ≤ 16 years of age. One knee (3%) was revised due to persistent pain. The median score was 86 points for the Kujala score and 90 for the Lysholm score. The median in the Tegner score was level 6. Clinically, the patellar glide was lateralized in 7 knees (21%) and an apprehension sign was triggered in 8 knees (24%).
Conclusions
Including the present study, the existing literature indicates a redislocation rate between 24 and 41% following AK. It should thus be regarded as obsolete even though it protects the epiphysis. Surgical interventions such as medial patellofemoral ligament reconstruction with femoral drilling distal to the epiphysis should be preferred.
Trial registration
Retrospectively registered: S-302/2016.
Level of evidence
III
Similar content being viewed by others


Background
Patellar dislocation is common in children and adolescents. The incidence is reported to be around 43 per 100,000 in patients younger than 16 years of age [1]. The etiology is diverse. Two forms can be distinguished. The chronic patellar instability due to a congenital malformation of the patellar stabilizers and the chronic, secondary patellar instability after traumatic patellar dislocation [2]. The first etiology is significantly more common and occurs more frequently in female patients [3]. Several anatomical and functional factors contribute to the recurrent dislocations. These include trochlear dysplasia, patella alta, lateral patellar tilt, increased tibial extra-torsion, increased femoral anteversion, vastus medialis hypoplasia, subtalar joint pronation or valgus deformity of the lower limb [4]. A variety of different surgical treatment options exist depending on the severity and etiology. The goal is proximal and/or distal realignments to achieve a stable patella [5].
The Elmslie-Trillat procedure is indicated in patellofemoral instability related to a pathological Tuberositas-Tibiae-Trochlea-Groove-Index (TTTG-Index) and involves medialization of the ligamentum patellae with the corresponding part of the tibial tubercule [6]. Trochleoplasty is an invasive procedure to deepen the trochlear groove indicated in patients with patellar instability due to a “C” or “D” and in some cases “B” trochlea according to Dejour [7]. The Roux–Goldthwait procedure was initially described by Roux in 1888 and then modifed by Goldthwait in 1895 as hemi-patellar transfer for the treatment of recurrent patellar dislocation [8]. The Ali Krogius (AK) procedure was first described in 1904 for the treatment of patellofemoral instability [9]. A strip of the medial retinaculum, pedicled proximally into the vastus medialis, is sewn into the lateral retinaculum This results in a proximal active and passive medialization restraint of the patella. The AK procedure is a purely soft tissue operation and offers the advantage of protecting open growth plates. Unfortunately, studies from the 1980s report a rather high rate of dislocation [10, 11]. The procedure is still practiced in many institutions and is mentioned as a standard procedure in book references for orthopaedic surgery. Current studies do not exist. The aim of the present study is to report results of the Ali Krogius procedure in a considerable number of patients with a long-term follow-up in order to provide a current statement and recommendation regarding its use.
Methods
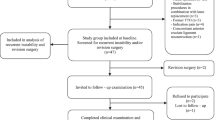
The present retrospective monocentric cohort study investigates all patients with recurrent patellar dislocation (3 or more instances of patellar dislocation) treated with the AK surgical method in one university hospital between January 1, 2004 and December 31, 2011. During this period, 93 knees in 81 patients received the procedure and were included. Patients with an underlying neurological disease or congenital syndromes (32 patients) that predispose to patellar dislocation were excluded in order to provide a more reliable conclusion. Patients who received other procedures (i.e. Roux–Goldthwait / Galeazzi / femoral or tibial osteotomies) in combination with AK were also omitted (11 patients). As a result, 54 knees were excluded from the study. A total of 39 knees in 38 patients remained in the cohort. Five patients were lost to follow-up. Thirty-three knees in thirty-three patients (70% female, 30% male) were therefore included in the final cohort. The patients’ age at the time of surgery ranged from 6 to 40 years, with an average age of 20.8 years. Age distribution is demonstrated in Fig. 1. Seventeen of the thirty-three examined knees belonged to patients who were 16 years old or younger at the time of surgery.

Age distributions of the study population
A clinical examination was carried out with an average duration of 94 months (Range 59–145 months). Relevant examination parameters such as the Zohlen sign (patellar grind test), apprehension sign and J-sign were performed. Range of motion (ROM) of the knee was reported [12]. Scores relevant to patellofemoral instability, pain and function which have been tested for validity and reliability in the literature were assessed [13, 14]. These included the Kujala Anterior knee pain scale, Lysholm Score, IKDC-2000, Knee Injury and Osteoarthritis Outcome Score (KOOS) and Tegner activity Score [15,16,17,18,19]. A subgroup analysis was done in patients aged ≤16 years and those older. Postoperative redislocations and revisions were reported. Preoperative radiological evaluation of available radiographs and Magnetic Resonance Imaging (MRI) was done in patients when available. The Caton-Deschamps index was used to evaluate patella alta (Caton-Deschamps Index > 1,2) [20]. High-grade trochlear dysplasia was defined as Dejour types B, C, and D [21].
Data acquisition and analysis were performed in compliance with protocols approved by the Ethical Committee of the corresponding medical faculty (S-302/2016). The study was registered in the German Register of Clinical Studies and was conducted in accordance with the Declaration of Helsinki. All Patients gave informed written consent to participate in the study.
Descriptive statistics were used to report frequencies and means for the cohort and subgroups. A 2-tailed t-test was performed to compare data. Statistical analysis was performed using SPSS version 26. P-value < 0.05 was considered statistically significant.
Surgical method
The procedure was performed under general anesthesia. The patient was placed supine on the operating table. A tourniquet was applied to the thigh, the leg exsanguinated, and the cuff inflated to 250 mmHg.
A skin incision running along the middle of the patella is made reaching the tibial tuberosity. The medial and lateral retinaculum are first exposed. The medial retinaculum is split lengthways approximately 1 cm medial to the patella and 2–3 cm proximal to the tibial tuberosity in order to prepare a proximally pedicled capsular retinaculum strip approximately 1 cm wide, depending on the degree of the desired correction. Care is taken to ensure that the retinaculum strip is sufficiently stalked into the vastus medialis muscles to ensure that the proximal medialization is as uniform as possible. This capsule-retinacular strip is then thread-reinforced distally and, with slight tension, repositioned laterally under the quadriceps tendon and anchored to the lateral retinaculum margins. The medial retinaculum is now adapted by means of a single button suture and with constant monitoring of the patellar path. The degree of medialization can be increased at any time by overlapping suturing of the medial retinaculum margins. The method is demonstrated in Figs. 2 and 3.

Intraoperative demonstration of the Ali Krogius method. A: Undermining the Quadriceps. B: Pedunculated retinaculum strip. C: Lateralization of the retinacular strip. D: Fixed, medialized patella after the Ali Krogius procedure

Illustration of the Ali Krogius surgical method
All patients received regular physiotherapy postoperatively. A 2-week duration of partial weightbearing with approximately 20 kg was instructed initially instructed. This was followed by a 2-week duration of gradual build up to full weightbearing. The flexion of the operated knee joint did not exceed 90 ° degrees for 6 weeks. A rigid frame brace was worn for a total of 3 months postoperatively with the above-mentioned flexion restriction for the first 6 weeks. Cycling and swimming were allowed 6 weeks postoperatively, jogging after 12 weeks and full fitness after muscle strengthening 6 months postoperatively.
Results
The preoperative radiological examination was possible in 26 of 33 knees. Fifteen of twenty-six knees (58%) had a Caton-Deschamps index > 1.2 and thus a patella alta. A patella tilt angle > 5 ° was measured in 19 of 26 knees (73%). MRI revealed a type A trochlea in 12 patients, type B in 2 patients, type C in 2 patients and type D in 6 patients.
In the 33 knees that received AK, 8 knees (24.2%) suffered a redislocation. The patients’ age at the time of dislocation was ≤16 years in 7 of the 8 cases. Stratified according to patient age, the patient group aged 16 years or younger therefore has a significantly higher rate of dislocation of 41% (Fig. 4) than those over 16 years of age (6%). Preoperative imaging was available for 5 of the 8 redislocated knees. Two patients (40%) had a patella alta. A high grade trochelar dysplasia (Type B and D) was detected in two patients (40%). The remaining patients had a mild grade trochlear dysplasia (Type A). Despite redislocations, these patients showed good to very good clinical results. The median Kujala score was 81%, the Lysholm score 82%, the IKDC-2000 86%, the KOOS score 90% and the Tegner score a median of 5.

Redislocations after Ali Krogius procedure according to patients’ age
On physical examination on follow-up, knee flexion range had a median of 140 ° (range 110 °-150 °) and extension range of 5 ° (Range 0 ° -20 °). In comparison, the non-operated knees showed a flexion range of 140 ° (range 120 ° -150 °) and extension range of 5 ° (range 0 ° -20 °). When comparing the ROM of the operated and non-operated knee joints using the T-test, there were no significant differences in flexion (P = 0.45) and extension (P = 0.34). The J-sign was positive in 3 knees. One of these knees was dislocated postoperatively. The apprehension sign could be triggered in 8 of the 33 knees. In 3 of these knees, the patella redislocated postoperatively. Of all patients, 13 (39%) had a valgus deformity, 3 (9%) a varus deformity and 17 (51.5%) a straight leg axis. In addition, 7 (21%) had a lateralized patellar glide and 26 (79%) had a centered patellar glide.
The postoperative scores showed good to very good results (Fig. 5). The median was 86% in the Kujala score, 90% in the Lysholm score, 88% in the IKDC 2000, 93% in the KOOS score and 6 in the Tegner score. Eleven patients (33.3%) achieved a very good result in the Lysholm score, 13 (39.4%) patients a good result, 8 patients (24.2%) a sufficient result and 1 patient (3%) a bad result. In the IKDC-2000, 30 patients (91%) reported results in the range of the reference values and 3 patients (9%) reported results below the reference values [22]. In the Tegner activity score, both men and women had a median of 6.

Results of the score on follow-up
Subgroup analysis were performed considering patients age of ≤ 16 years and > 16 years indicating approximate time of closed physis. The available preoperative values of both subgroups are displayed in Table 1. Statistical comparison of the available values revealed no significant differences. Regarding the follow-up assessment, a mean of 5.3 showed a significantly higher value in the Tegner Score (P = 0.03) for those over 16 years. The Kujala score (P = 0.097), Lysholm score (P = 0.15), IKDC 2000 score (P = 0.089) and KOOS score (P = 0.085) showed higher scores among those aged 16 years or younger (Fig. 6), but statistical comparison was not significant.

Subgroup analysis of patients according to age group
Discussion
There are many different conservative and surgical procedures that address different predisposing risk factors for the treatment of recurrent patellar dislocation. No gold standard exists for the surgical treatment. Many of the procedures that have become established in recent years, such as Elmslie’s tuberosity medialization or trochleaplasty, are bone-invasive and are contraindicated in young patients due to open growth plates [23, 24]. Medial-based soft-tissue stabilization procedures are the focus in this pediatric population. A method for which there are only a few studies with varying results in the medical literature is the AK procedure performed as described in the methods section.
In the present study, a total of 33 knee joints received the AK procedure. In comparison with other studies, the number of knees operated on is roughly as large as that of published studies with 24–34 operated knee joints and smaller than 2 other studies with 73 and 49 operated knee joints (Table 2) ([9, 11, 25,26,27,28]. The average age of the operated patients was 20.78 (range 6–40), which is consistent with other studies on the AK method and also other epidemiological studies in which an average age of 20–22 years is reported [9, 25, 28,29,30,31]. The follow-up period in the present study was more than twice as long as that in the studies by Petrick and Tischer and Bauer et al. selected follow-up period of 2.8 years and slightly longer than that of Rebmann et al. and Jalovaara et al. with follow-up durations of 6.5 and 7 years, respectively [9, 11, 25, 27, 28]. To date, no study has been published on the results of the AK method with a follow-up period longer than 7.7 years.
When comparing the ROM of the operated and non-operated knee joints using the T-test, no significant differences in the ROM were found in this study. 13 (39%) patients had a valgus deformity. The proportion of patients who also have a genu valgum with recurrent patellar dislocation is therefore significantly smaller compared to the 77% described in a cross-sectional study [31]. Whether the valgus deformity is predisposing to a recurrent patellar dislocation cannot be definitively proven based on these figures. No comparative values regarding the clinical parameters such as J-sign and apprehension sign exist.
At 24%, the rate of redislocations in the present study is lower than that of Bauer et al., Jalovaara et al. and Rebmann et al., who describe a rate of 36–42% and roughly comparable to that of Heisel et al., with a redislocation rate of 25% [9, 11, 25,26,27,28]. The revision rates after AK in the studies by Heisel et al. (12.5%), Jalovaara et al. (7%) and Bauer et al. (23.5%) are higher than in the present study (3%) [25, 27, 28].
In skeletally immature patients, a conservative therapy regimen is initially recommended if the first dislocation of the patella is uncomplicated. After exhaustion of conservative therapy and persistence of the symptoms in children with recurrent patellar dislocation, surgical treatment must be considered. This is especially the case if massive bone deformities or traumatic osteochondral injuries are involved [32]. In skeletally immature patients, bony transpositions should primarily be discouraged, and growth-respecting surgical stabilization techniques such as the AK procedure, preferred [23].
The identification of the medial patellofemoral ligament (MPFL) as the most important passive stabilizer in the extended knee has led to considerable progress in understanding patellar dislocation. Patients of growing age have more frequent injuries to the MPFL than adults with an injury rate of up to 99% following the first dislocation [33]. MPFL reconstruction yields a high success with excellent clinical results and low redislocation rates postoperatively (5–7%) [34,35,36]. A meta-analysis comparing MPFL reconstruction with other soft tissue realignment techniques in skeletally immature patients reported a statistically insignificant difference in instability rate, It was evident, however, that MPFL reconstruction had superior results [37]. Techniques using the adductor magnus tendon as a “sling” for the femoral fixation minimize risk to the distal femoral physis. However, the attachment site of the reconstruction on the femur nonanatomic and is too proximal, potentially resulting in a non-isometric graft, loss of knee motion, and extension of the graft as growth occurs [38]. Considering these risks, multiple physeal-sparing MPFL reconstruction techniques have emerged which aim to prevent injury to the physis and at the same time adequately augment the MPFL [39, 40]. These techniques produced good preliminary results, but more studies are required to establish them further.
Strengths and limitations
The validity of this study could have been enhanced by control groups and a prospective study design. One aspect worth mentioning is the size of the study population. Since the AK method is only rarely used, this number of cases is relatively high compared to other studies on the results of this surgical method. Only in the retrospective cohort studies by Jalovaara and Rebmann in the 1980s were similarly large case numbers examined. Moreover, the subgroup analysis assessed patients with a cut-off at 16 years of age as a comparison of adult and pediatric populations. However, this does not necessarily separate patients with and without epiphyseal closure.
In comparison with the other retrospective studies on the AK method, the average follow-up period of 94 months (7.8 years) is comparatively long. However, the range is quite large with 59–145 months. In addition, due to the long-time interval between the date of the operation and the follow-up examination, only 85% of the patients who had met the study criteria took part in the study. The remaining 15% could no longer be contacted due changing addresses or names. Their redislocation rates remain unknown. Since a period of several years was examined, the patients in the study collective were treated by different surgeons, which limits comparability. In follow-up studies, a prospective study design should be used in which pre- and postoperative score collection and imaging are compared over time to present the subjective and objective postoperative results more precisely. In the present study, a preoperative radiological assessment was unfortunately not possible for all patients.
Conclusions
Even if the protection of the growth plate speaks for the use of the AK procedure in skeletally immature patients, it must be described as obsolete due to the relatively high rate of redislocation. The present study retaliates an important message which is consistent with older existing studies in the medical literature. Other surgical interventions such as MPFL reconstruction with femoral drilling distal to the growth plate should thus be preferred.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
17 July 2022
Missing Open Access funding information has been added in the Funding Note.
Abbreviations
- AK:
-
Ali krogius
- MPFL:
-
Medial patellofemoral ligament
- TTTG-Index:
-
Tuberositas-Tibiae-Trochlea-Groove-Index
- ROM:
-
Range of motion
- KOOS:
-
Knee Injury and Osteoarthritis Outcome Score
- MRI:
-
Magnetic resonance imaging
- i.e.:
-
Id est
References
Nietosvaara Y, Aalto K, Kallio PE. Acute patellar dislocation in children: incidence and associated osteochondral fractures. J Pediatr Orthop. 1994;14(4):513–5.
Chotel F, Bérard J, Raux S. Patellar instability in children and adolescents. Orthop Traumatol Surg Res. 2014;100(1 Supplement):S125–37.
Hsiao M, Owens BD, Burks R, Sturdivant RX, Cameron KL. Incidence of acute traumatic patellar dislocation among active-duty United States military service members. Am J Sports Med. 2010;38(10):1997–2004.
White BJ, Sherman OH. Patellofemoral instability. Bull NYU Hosp Jt Dis. 2009;67(1):22–9.
Hughston JC, Walsh WM. Proximal and distal reconstruction of the extensor mechanism for patellar subluxation. Clin Orthop Relat Res. 1979;144:36–42.
Rillmann P, Dutly A, Kieser C, Berbig R. Modified Elmslie-Trillat procedure for instability of the patella. Knee Surg Sports Traumatol Arthrosc. 1998;6(1):31–5.
Lippacher S, Dejour D, Elsharkawi M, Dornacher D, Ring C, Dreyhaupt J, et al. Observer agreement on the Dejour trochlear dysplasia classification: a comparison of true lateral radiographs and axial magnetic resonance images. Am J Sports Med. 2012;40(4):837–43.
Felli L, Capello AG, Lovisolo S, Chiarlone F, Alessio-Mazzola M. Goldthwait technique for patellar instability: surgery of the past or here to stay procedure? A systematic review of the literature. Musculoskelet Surg. 2019;103(2):107–13.
Petrick P, Tischer K. Results of the Ali Krogius treatment in so-called habitual patellar luxation. Beitr Orthop Traumatol. 1978;25(10):570–2.
Synder M, Grzegorzewski A, Witoński D. Surgical treatment for recurrent dislocation of the patella in children and adolescents. Chir Narzadow Ruchu Ortop Pol. 1996;61(5):459–62.
Rebmann K, Grasshoff H, Brendel U. Results of the surgical treatment of habitual and recurrent patella dislocation using Ali Krogius' method. Beitr Orthop Traumatol. 1989;36(12):571–5.
Lester JD, Watson JN, Hutchinson MR. Physical examination of the patellofemoral joint. Clin Sports Med. 2014;33(3):403–12.
Smith TO, Davies L, O'Driscoll ML, Donell ST. An evaluation of the clinical tests and outcome measures used to assess patellar instability. Knee. 2008;15(4):255–62.
Paxton EW, Fithian DC, Stone ML, Silva P. The reliability and validity of knee-specific and general health instruments in assessing acute patellar dislocation outcomes. Am J Sports Med. 2003;31(4):487–92.
Kujala UM, Jaakkola LH, Koskinen SK, Taimela S, Hurme M, Nelimarkka O. Scoring of patellofemoral disorders. Arthroscopy. 1993;9(2):159–63.
Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res. 1985;198:43–9.
Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR. The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med. 2009;37(5):890–7.
Higgins LD, Taylor MK, Park D, Ghodadra N, Marchant M, Pietrobon R, et al. Reliability and validity of the international knee documentation committee (IKDC) subjective knee form. Joint Bone Spine. 2007;74(6):594–9.
Roos EM, Lohmander LS. The knee injury and osteoarthritis outcome score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes. 2003;1:64.
Biedert RM, Tscholl PM. Patella Alta: a comprehensive review of current knowledge. Am J Orthop (Belle Mead NJ). 2017;46(6):290–300.
Colatruglio M, Flanigan DC, Harangody S, Duerr RA, Kaeding CC, Magnussen RA. Identifying patients with Patella Alta and/or severe trochlear dysplasia through the presence of patellar apprehension in higher degrees of flexion. Orthop J Sports Med. 2020;8(6):2325967120925486.
Anderson AF, Irrgang JJ, Kocher MS, Mann BJ, Harrast JJ. The international knee documentation committee subjective knee evaluation form: normative data. Am J Sports Med. 2006;34(1):128–35.
Baier C, Springorum HR, Beckmann J, Grifka J, Matussek J. Treatment of patellar instability in children and adolescents. Orthopade. 2011;40(10):868–70 872-864, 876.
Oestern S, Varoga D, Lippross S, Kaschwich M, Finn J, Buddrus B, et al. Patella dislocation. Unfallchirurg. 2011;114(4):345–58 quiz 359.
Bauer FC, Wredmark T, Isberg B. Krogius tenoplasty for recurrent dislocation of the patella. Failure associated with joint laxity. Acta Orthop Scand. 1984;55(3):267–9.
Cotta H. On the therapy of habitual patellar luxation. Arch Orthop Unfallchir. 1959;51:265–71.
Heisel J, Aeckerle J, Mittelmeier H. Surgical treatment of chronic recurrent patella dislocations. Surgical procedure and results. Z Orthop Ihre Grenzgeb. 1983;121(5):571–7.
Jalovaara P, Seppänen-Lehmonen T, Lindholm RV. Krogius and roux-Goldthwait operations for recurrent patellar dislocation. Acta Orthop Belg. 1988;54(4):380–3.
Atkin DM, Fithian DC, Marangi KS, Stone ML, Dobson BE, Mendelsohn C. Characteristics of patients with primary acute lateral patellar dislocation and their recovery within the first 6 months of injury. Am J Sports Med. 2000;28(4):472–9.
Stefancin JJ, Parker RD. First-time traumatic patellar dislocation: a systematic review. Clin Orthop Relat Res. 2007;455:93–101.
Diederichs G, Scheffler S. MRI after patellar dislocation: assessment of risk factors and injury to the joint. Rofo. 2013;185(7):611–20.
Hinton RY, Sharma KM. Acute and recurrent patellar instability in the young athlete. Orthop Clin North Am. 2003;34(3):385–96.
Askenberger M, Arendt EA, Ekström W, Voss U, Finnbogason T, Janarv PM. Medial patellofemoral ligament injuries in children with first-time lateral patellar dislocations: a magnetic resonance imaging and arthroscopic study. Am J Sports Med. 2016;44(1):152–8.
Balcarek P, Rehn S, Howells NR, Eldridge JD, Kita K, Dejour D, et al. Results of medial patellofemoral ligament reconstruction compared with trochleoplasty plus individual extensor apparatus balancing in patellar instability caused by severe trochlear dysplasia: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2017;25(12):3869–77.
Boelch SP, Gurok A, Gilbert F, Weißenberger M, Rudert M, Barthel T, Reppenhagen S. Why compromise the patella? Five-year follow-up results of medial patellofemoral ligament reconstruction with soft tissue patellar fixation. Int Orthop. 2021;45(6):1493–500.
Lippacher S, Dreyhaupt J, Williams SR, Reichel H, Nelitz M. Reconstruction of the medial patellofemoral ligament: clinical outcomes and return to sports. Am J Sports Med. 2014;42(7):1661–8.
Wilkens OE, Hannink G, van de Groes SAW. Recurrent patellofemoral instability rates after MPFL reconstruction techniques are in the range of instability rates after other soft tissue realignment techniques. Knee Surg Sports Traumatol Arthrosc. 2020;28(6):1919–31.
Lind M, Enderlein D, Nielsen T, Christiansen SE, Faunø P. Clinical outcome after reconstruction of the medial patellofemoral ligament in paediatric patients with recurrent patella instability. Knee Surg Sports Traumatol Arthrosc. 2016;24(3):666–71.
Ladenhauf HN, Berkes MB, Green DW. Medial patellofemoral ligament reconstruction using hamstring autograft in children and adolescents. Arthrosc Tech. 2013;2(2):e151–4.
Liles J, Johnston T, Hu J, Riboh JC. Physeal-sparing medial patellofemoral ligament reconstruction with suture anchor for femoral graft fixation. Arthroscopy techniques. 2020;9(7):e889–95.
Acknowledgements
For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft within the funding programme “Open Access Publikationskosten” as well as by Heidelberg University.
Funding
The authors have not received specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
BY, SH, AB were responsible for the idea and conception of the study. AB, BY and FM planned the Study protocol. AB, SH and BY performed all operations mentioned in the study. FM and AJ were responsible for the organization of all clinical trials as well as data acquisition. AJ, JW and BY performed the clinical examination for all study participants. AJ, SH, FM and JW did the statistical analysis and interpreted the results. AJ, JW, SH, YB, FM and AB wrote and revised the Manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Data acquisition and analysis were performed in compliance with protocols approved by the Ethical Committee of Heidelberg University Hospital (Ethikkommission - Medizinische Fakultät Heidelberg). The study was registered in the local register of clinical studies and was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all patients/parents before inclusion in the study.
Consent for publication
Informed consent was obtained from all patients/parents before inclusion in the study and anonymous publication of the results.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bangert, Y., Mittelstrass, F., Weisshorn, J. et al. The Ali Krogius procedure for treatment of patellofemoral instability should be regarded as obsolete even in skeletally immature patients. BMC Musculoskelet Disord 23, 257 (2022). https://doi.org/10.1186/s12891-022-05200-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05200-4