
Abstract
Background
Carpal tunnel syndrome (CTS) is the most common peripheral neuropathy. Moreover, carpal tunnel release (CTR) surgery generally has excellent results. The present study aimed to investigate the predictors of clinical outcomes and satisfaction in patients with CTR.
Methods
In this observational prospective cohort study, 152 patients with open carpal tunnel release surgery were investigated. Complete clinical examinations were performed and recorded before the surgery, two weeks after the surgery and 6 months after the surgery. The Boston Carpal Tunnel Questionnaire (BCTQ) were assessed on admission and at last follow-up visits to evaluate clinical outcomes. Patients’ satisfaction was determined by a 10-point verbal descriptor nominal scale (1 = very poor, 5 = fair and 10 = excellent) and recorded during the last follow -up visits.
Results
Among 152 patients who were investigated, there were 118 (77.6%) females and 34 (22.36%) males. Overall, surgery improved the outcomes based on Symptom Severity Scale (SSS) and Functional Status Scale (FSS) (P < 0.05). Most of the considered variables did not show significant effects on clinical outcomes and patients’ satisfaction. However, duration of symptoms and electrophysiological severity were the predictors of the change score in SSS(P < 0.05). As well as, age was the only predictor of the change score in FSS (P < 0.05). Finally, according to the linear regression model, the pre-operative grip strength and age were the independent predictors of post-operative satisfaction (P < 0.05).
Conclusions
Results of the present study revealed that there was a significant improvement in clinical outcomes after CTS surgery. Stronger pre-operative grip strength and younger age were independent predictors of higher post-operative satisfaction. These results can be used in pre-operative counseling and management of post-operative expectations.
Similar content being viewed by others


Background
Carpal tunnel syndrome (CTS) is the most common peripheral neuropathy[ [1]. Its prevalence reported between 1 to 16% in the general adult population [2, 3].
CTS is characterized by numbness or tingling in the sensory distribution of the median nerve. In some cases, CTS can be accompanied by pain and/or weakness of the thenar muscles which could affect thumb abduction and opposition [4].
Indicators of the disease are varied and include a combination of symptoms (e.g., paresthesia, tingling, and numbness), signs (e.g. Durkan’s sign, Phalen’s sign and Tinel’s sign) and electrophysical studies [1, 5, 6]. CTR is effective in most cases.
A limited number of studies have highlighted the predictors of patients’ outcomes and their satisfaction following CTR [3,4,5, 7]
Identifying preoperative predictors of clinical outcomes and post-operative satisfaction provides more information for surgical planning and preoperative consultation [5]. The present study had two aims. The primary purpose of this study was to identify predictors of clinical outcomes after CTR. The secondary objective of this study was to evaluate patients’ satisfaction and correlated predictors following CTR.
Methods
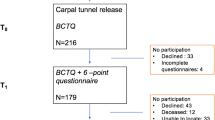
This prospective study was conducted in 2018. A sample of 152 patients with carpal tunnel syndrome who referred to the Imam Reza hospital, Kermanshah, Iran between April 2015 and April 2017, were included. Inclusion criteria were: age over 18 years, disease duration of at least 6 months and failure in medical treatment. Patients with a history of previous wrist surgery or trauma and those with diabetic neuropathy and cases with bilateral CTS were excluded. Moreover, 5 patients (3.03%) left the follow up and 8 subjects (4.84%) did not complete pre/postoperative forms [Fig. 1].

Flowchart of the study population
The present study was approved by the Scientific Research Board of the Kermanshah University of Medical Sciences. Informed written consent was obtained from all patients before enrolment.
Meticulous clinical examinations including specific provocative tests of the hand (Phalen’s sign, Tinel’s signs, and Durkan’s tests), the Semmes–Weinstein monofilament test, and grip strength test were performed.
We performed the Semmes–Weinstein monofilament test at the most prominent finger for each patient. Results were recorded by a 5-point scale as follows: 1- normal (2.83 monofilaments), 2-diminished light touch (3.61), 3- diminished protective sensation (4.31), 4- loss of protective sensation (4.56), and 5-untestable sensation (6.65) [8]. Grip strength test was conducted using a Jamar dynamometer (Sammons Preston, Bolingbrook, Illinois) [3].
Electrophysiological tests were conducted pre-operatively for each patient. Sensory nerve action potential (SNAP) (in μv), the peak latency of SNAP (in ms), the peak amplitude of compound muscle action potential (in mV), and conduction velocity of the SNAP (in m/s) were recorded. According to the American Association of Electrodiagnostic Medicine criteria [8] patients were categorized into three groups (mild, moderate and severe).
The Boston Carpal Tunnel Questionnaire (BCTQ) were assessed at intake and last follow -up visits to evaluate clinical outcomes.
Boston Carpal Tunnel Questionnaire (BCTQ) scores were recorded at preoperative visits and six-month post-operative visits. The BCTQ [6] is a disease-specific tool that can be used to assess symptom severity, functional status, and clinical outcome of patients with CTS. BCTQ is comprised of two separate parts: a symptom severity scale (SSS) and a functional status scale (FSS). The first part comprises 11 questions (Q1 ~ Q11) concerning the severity of pain, tingling, numbness, and weakness. The functional status scale has 8 questions of activities of daily tasks. Each item scoring from 1 to 5 in the ascending order making a total score of 55 for SSS (with 11 being the best and 55 being the worst) and 40 for the FSS (with eight being the best and 40 being the worst). Mean Boston score for symptom severity and mean Boston score for functional status were obtained by dividing the total SSS by11 and total FSS by 8. BCTQ was translated into the Persian language and it was validated. All patients were managed with the minimal invasive open technique for carpal tunnel release under local anesthesia.
Age, sex, hand dominancy, smoking, symptoms duration, body mass index (BMI), the Semmes–Weinstein monofilament test, grip strength, electrophysiological severity, scores of the Boston Carpal Tunnel Questionnaire, presence of positive physical examination signs (Phalen’s sign, Tinel’s signs and Durkan’s tests), presence of thenar atrophy and EMG abnormalities (fibrillations, positive sharp waves or fasciculations) were selected as probable predictors of clinical outcomes and patients’ satisfaction.
Patients’ satisfaction was determined by a 10-point verbal descriptor nominal scale (1 = very poor, 5 = fair, 10 = excellent) and recorded, at last, follow -up visits.
Statistical analysis
Data analysis was performed with SPSS 21 (SPSS Inc. Chicago, Illinois). The mean and standard deviation of quantitative variables were calculated. The normality of quantitative variables was checked by the Kolmogorov -Smirnov test. The Wilcoxon test was used to compare preoperative SSS and FSS with 6- month postoperative SSS and FSS. Because the variables of pre-operative SSS, pre-operative FSS, Satisfaction, as well as change scores in SSS and FSS were non-normal, we used nonparametric tests such as Mann-Whitney-U test, Kruskal Wallis, and Spearman correlation test for checking the relationship between mentioned variables with other variables and those that were significant entered into the linear regression model. It is notable, because dependent variables (pre-operative SSS, pre-operative FSS, Satisfaction, change score in SSS, and change score in FSS) were non-normal we take their logarithm (Ln) before doing regression tests. Significant level < 0.05 considered as the significant level. P values < 0.05 considered as the significant level.
Results
There were 118 (77.6%) females and 34 (22.36%) males. The mean age was 50.50 ± 7.24 years. Sixteen (10.5%) patients had CTS symptoms for less than 1 year, 123(80.9%) patients had symptoms for a period of 1 to 4 years, and 13(8.6%) of our patients were symptomatic for more than 4 years. In 69.7% of patients (106 individuals), the dominant hand was involved. [Table 1].
Predictors of pre-operative BCTQ (SSS & FSS)
The results of univariate analyses showed that the pre- operative SSS was related to age, duration of symptoms, electrophysiological severity, and the presence of thenar muscle atrophy(P < 0.05) [Table 2]. As well as, age, duration of symptoms, and the presence of thenar muscle atrophy were related to the pre-operative FSS (P < 0.05) [Table 2]. According to the linear regression model, duration of symptoms and electrophysiological severity were the independent predictors of preoperative SSS. The model predicted 63% of the variance of pre-operative SSS [Table 3]. Meanwhile, linear regression model showed the age, duration of symptoms, and the presence of thenar muscle atrophy as the predictors of pre-operative FSS [Table 4].
Predictors of change scores in SSS and FSS
Overall, the result of the present study revealed that the surgery improved outcomes [Table 5]. Most variables did not have strong predictive power in clinical outcomes [Table 2]. However, duration of symptoms and electrophysiological severity were predictors of the change score in SSS (P < 0.05) [Table 6]. Moreover, age was the only predictor of change scores in FSS(P < 0.05) [Table 7].
Predictors of post-operative satisfaction
At first, we assessed the relationship between post-operative satisfaction and suggested variables. The variables of age and preoperative grip strength were correlated with the patients’ satisfaction (P < 0.05) [Table 3]. In the next step, we conducted a linear regression model. Interestingly, the result of the regression model showed the preoperative grip strength as the powerful predictor of post-operative satisfaction (B = 0.026, P < 0.001). However, the model did not show such a strong predictive power for age (B = − 0.003, P = 0.043). Overall, the model predicted 73% of the variance of post-operative satisfaction [Table 8].
Critical complications such as tendon, muscle or nerve damages were not observed in the study.
Discussions
Carpal tunnel syndrome is the most common peripheral neuropathy [9]. Carpal releasing surgery proved to be effective in many cases, although reported success varies. The incidence of CTS is increasing as 11% of females and 3.5% of males, with increasing life expectancy [10].
Open release of the carpal tunnel, introduced by Phalen et al. (1950) is the standard treatment for the CTS [11]. According to a recent review of a long-term follow-up after CTS surgery, clinical success reported between 75 and 90% [1]. In spite of the considerable improvement in patients’ symptoms, their satisfaction with releasing surgery is still unpredictable. In the present study, we have evaluated the predictors of clinical outcomes and satisfaction of patients with CTR.
The Boston carpal tunnel syndrome questionnaire is a disease-specific measure [6]. The sensitivity of the Boston CTS Questionnaire for detecting a change after carpal tunnel surgery has been demonstrated [6]. Gay et al. found that the BCTQ is more sensitive to changes in clinical stats of patients than the electrophysiological findings, clinical examination or other generic questionnaires such as the Short-Form 36 and Disabilities of the Arm, Shoulder, and Hand questionnaire [12].
Some factors have been suggested as outcome predictors of carpal releasing surgery including age, gender, smoking, occupation, underlying disease, duration of symptoms, and preoperative muscle weakness or atrophy [7, 8] However, in this study, most variables did not have a strong predictive value on patients’ outcomes. In our study, patients with severe electrophysiological findings had higher postoperative FSS score. This finding suggests that early diagnosis and treatment of carpal tunnel syndrome could improve clinical outcomes.
Moreover, our results did not demonstrate a relationship between clinical outcomes and the duration of symptoms. Eisenhardt et al. reported a recovery period of 16 days in patients whose symptoms lasted less than 1 year compared to 25 days of recovery in patients with duration of symptoms more than 1 year [13]. They found that the duration of paresthesia did not have a significant effect on the outcome of CTR [13].
Grip strength can be decreased by CTS significantly which can lead to losing productivity at work and daily activities [14]. This study concluded that patients with a weaker preoperative grip strength had lower satisfaction following a CTR. Brown et al. reported that patients with reduced grip strength require longer postoperative duration to recover the grip strength and the recovery is also incomplete. They have suggested that this may be due to progressive median nerve damage in long-standing CTS [11]. Levine et al. reported that patients’ satisfaction had a moderate correlation with the improvement of the functional status score and highly with changes in the symptom severity scale score and a moderate correlation with the change of the functional status score [6].
The relationship between age and patients’ satisfaction after CTR is not well documented. Results of our study revealed a correlation between age and post-operative satisfaction. Hansen and Larsen [15] reported that patients over 65 years old had less favorable results on the BCTQ after CTR. They concluded that age may have an adverse effect on nerve regeneration. Atroshi et al. found that age was a significant predictor of patient dissatisfaction [16].
Strength and limitations
This study has shown to be powerful in three main areas: First, a large sample of patients, second, organized and detailed data on symptoms and third, a systemized physical examination.
This study had limitations. We measured patients’ satisfaction only at 6 months after CTS surgery. However, studies with longer follow-up periods showed that the persistence of positive effects had no further improvement beyond 6 months [4, 17, 18].
Furthermore, there was a substantial drop-out rate among patients between the intake and the follow-up at 6 months.
Conclusions: Results of the present study revealed that there was a significant improvement in clinical outcomes after CTS surgery. Stronger pre-operative grip strength and younger age were independent predictors of higher post-operative satisfaction. These results can be used in pre-operative counseling and management of post-operative expectations.
Availability of data and materials
All data are available from the corresponding author upon reasonable request.
Abbreviations
- BCTQ:
-
Boston Carpal Tunnel Questionnaire
- CTR:
-
Carpal Tunnel Release
- CTS:
-
Carpal Tunnel Syndrome
- CTS:
-
Symptom Severity Scale
- FSS:
-
Functional Status Scale
References
Louie D, Earp B, Blazar P. Long-term outcomes of carpal tunnel release: a critical review of the literature. Hand (New York, NY). 2012;7(3):242–6.
Bae JY, Kim JK, Yoon JO, Kim JH, Ho BC. Preoperative predictors of patient satisfaction after carpal tunnel release. Orthop Traumatol Surg Res. 2018;104(6):907–9.
Beck JD, Brothers JG, Maloney PJ, Deegan JH, Tang X, Klena JC. Predicting the outcome of revision carpal tunnel release. J Hand Surg. 2012;37(2):282–7.
Carmona L, Faucett J, Blanc PD, Yelin E. Predictors of rate of return to work after surgery for carpal tunnel syndrome. Arthritis Care Res. 1998;11(4):298–305.
Dyer G, Lozano-Calderon S, Gannon C, Baratz M, Ring D. Predictors of acute carpal tunnel syndrome associated with fracture of the distal radius. J Hand Surg. 2008;33(8):1309–13.
Levine DW, Simmons BP, Koris MJ, Daltroy LH, Hohl GG, Fossel AH, et al. A self-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. J Bone Joint Surg Am. 1993;75(11):1585–92.
Werner RA, Gell N, Franzblau A, Armstrong TJ. Prolonged median sensory latency as a predictor of future carpal tunnel syndrome. Muscle Nerve. 2001;24(11):1462–7.
Chen AC, Wu MH, Cheng CY, Chan YS. Outcomes and satisfaction with endoscopic carpal tunnel releases and the predictors - a retrospective cohort study. Open Orthop J. 2016;10:757–64.
Lo JK, Finestone HM, Gilbert K. Prospective evaluation of the clinical prediction of electrodiagnostic results in carpal tunnel syndrome. PM R. 2009;1(7):612–9.
Visser LH, Ngo Q, Groeneweg SJ, Brekelmans G. Long term effect of local corticosteroid injection for carpal tunnel syndrome: a relation with electrodiagnostic severity. Clin Neurophysiol. 2012;123(4):838–41.
Brown RA, Gelberman RH, Seiler JG 3rd, Abrahamsson SO, Weiland AJ, Urbaniak JR, et al. Carpal tunnel release. A prospective, randomized assessment of open and endoscopic methods. J Bone Joint Surg Am. 1993;75(9):1265–75.
Gay RE, Amadio PC, Johnson JC. Comparative responsiveness of the disabilities of the arm, shoulder, and hand, the carpal tunnel questionnaire, and the SF-36 to clinical change after carpal tunnel release. J Hand Surg. 2003;28(2):250–4.
Eisenhardt SU, Mathonia C, Stark GB, Horch RE, Bannasch H. Retrospective analysis of 242 patients whose carpal tunnels were released using a one-port endoscopic procedure: superior results of early intervention. J Plast Surg Hand Surg. 2010;44(6):311–7.
Edgell SE, McCabe SJ, Breidenbach WC, LaJoie AS, Abell TD. Predicting the outcome of carpal tunnel release. J Hand Surg. 2003;28(2):255–61.
Hansen TB, Larsen K. Age is an important predictor of short-term outcome in endoscopic carpal tunnel release. J Hand Surg Eur Vol. 2009;34(5):660–4.
Atroshi I, Johnsson R, Ornstein E. Patient satisfaction and return to work after endoscopic carpal tunnel surgery. J Hand Surg. 1998;23(1):58–65.
Zwolinska J, Kwolek A. Factors determining the effectiveness of conservative treatment in patients with carpal tunnel syndrome. Int J Occup Med Environ Health. 2019;32(2):197–215.
Louie DL, Earp BE, Collins JE, Losina E, Katz JN, Black EM, et al. Outcomes of open carpal tunnel release at a minimum of ten years. J Bone Joint Surg Am. 2013;95(12):1067–73.
Acknowledgments
We appreciate the Clinical Research Development Center of Taleghani and Imam Ali Hospital for their wise advice.
Funding
There was no external source of funding.
Author information
Authors and Affiliations
Contributions
EA and SRB had the idea for this study. EA and PR participated in outlining the concept and design. HH and AA did the data acquisition. EA and AA did the statistical analysis and wrote the first draft of the manuscript. EA, SRB, HH, and AA revised the final manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study received ethics approval by the Kermanshah University of Medical Science Ethics Committee. Written consent to participate was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Alimohammadi, E., Bagheri, S.R., Hadidi, H. et al. Carpal tunnel surgery: predictors of clinical outcomes and patients’ satisfaction. BMC Musculoskelet Disord 21, 51 (2020). https://doi.org/10.1186/s12891-020-3082-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-020-3082-2