
Abstract
Background
This meta-analysis aimed to determine the bone union rate of bone defects treated with the different autologous bone graft techniques.
Methods
The PubMed and the Cochrane Library databases were searched using the terms: ‘fracture’ AND (‘bone loss’ OR ‘defect’ OR ‘defects’) AND ‘bone graft’, restricted to English language, to human species, and to a publication period from January 1999 to November 2014. Data were extracted by one of the reviewers and then checked by the second. A quality of evidence score and a methodology score were used. Heterogeneity was assessed. A random effects model approach was used to combine estimates.
Results
Out of 376 selected studies only 34 met the inclusion criteria. The summary pooled union rate was 91 % (95 % CI: 87–95 %) while union rate after additional procedures raised to 98 % (95 % CI 96–99 %). No association between union rate and bone defect size was found. (Univariable regression model: vascularized: P = 0.677; non-vascularized: 0.202. Multivariable regression model: vascularized: P = 0.381; non-vascularized: P = 0.226). Vascularized graft was associated with a lower risk of infection after surgery when compared to non-vascularized graft (95 % CI 0.03 to 0.23, p < 0.001).
Conclusion
The results of this meta-analysis demonstrate the effectiveness of autologous graft for bone defects. Furthermore, from the available clinical evidence bone defect size does not seem to have an impact on bone union when treated with autologous bone graft techniques.
Similar content being viewed by others


Background
Conventional autologous bone graft has become the most widely used treatment for bone defects over time. Several factors contributed to its widespread application: it is easy to obtain, it combines osteogenic, osteoinductive and osteoconductive properties, it does not raise immune response or transmit infectious diseases [1, 2]. Furthermore, autologous bone graft can be harvested in a variety of forms and sizes from different donor sites [1, 2].
Selection of the autologous graft type in the treatment of bone defects has been mostly based on defect size: several authors do not recommend the use of the non-vascularized graft in defects larger than 5 cm [1–3]. The more technical demanding vascularized bone graft method is considered the best choice for larger size defects [2, 3]. However, in recent years, advances in graft harvesting technique [4] and in wound environment recovery using the polymethylmethacrylate (PMMA) induced membrane technique [5], renewed the interest in the use of the non-vascularized autologous bone graft. Infection also plays a role in graft selection and a 2-stage approach with delayed grafting is sometimes necessary [6].
The primary objective of this meta-analysis is to determine the bone union rate of post-traumatic bone defects treated with the different autologous bone graft techniques. The secondary objective is to determine the rate of infection after this treatment.
Methods
Data collection and extraction
Prior to doing the electronic search, a written protocol was established according to guidelines for systematic reviews (AMSTAR, MOOSE and PRISMA) [7–9]. An electronic search was conducted in Medline restricted to English language, to human species, and to a publication period from January 1999 to November 2014. The search terms and Boolean operators used were: ‘fracture’ AND (‘bone loss’ OR ‘defect’ OR ‘defects’) AND ‘bone graft’. Additionally an electronic search was done in the Cochrane Library with the terms: fracture AND bone loss AND defect OR defects AND bone graft.
Two reviewers (MA, AA) independently scrutinized the list of titles of all the retrieved citations and, if necessary, the abstracts to determine usefulness of the article. The final selection was based on the full text version of the potentially relevant articles that were assessed independently by the reviewers. All references cited in these elected studies were manually searched along with the “related articles” researches in PubMed engine for additional relevant studies. Papers published by the same research group and studying the same factors were checked for duplicate data. Where duplication occured the less detailed paper was discarded.
We included only original reports that presented the results of at least ten cases of bone defects secondary to open fractures, post-traumatic nonunion or infected bone resection. The exclusion criteria were: bone defects after tumor resection; bone defects after reduction and fixation of closed metaphyseal fracture of long bones; studies with more than 25 % of the defect not located in long bones (forearm, humerus, femur or tibia); studies with more than 25 % of the defects treated with osteoconductive biomaterials in addition to the bone graft; cases with the use of osteoinductive factors in the graft; studies mostly about bone defects in children and studies that did not report the information about healing after treatment. When the information of each patient in a study was presented in the text and/or tables, cases that met the exclusion criteria were removed and the remaining patients were enrolled in the analysis.
Included studies were classified according the Oxford Centre for Evidence-Based Medicine system and a modified version of the Coleman methodology score [10] (Additional file 1). Data was extracted by one of the reviewers and then checked by the second. Disagreements were solved via discussion and consensus between the two reviewers. The following definitions were used for data extraction: primary union described as bone union achieved after bone grafting, secondary union as bone union achieved with a further surgery after the bone graft. Of note, a graft fracture was considered a union related complication only when the original study classified it in this manner, and cases with union before lost of follow up were considered as treated. Treatment failures were viewed as the loss of the graft in the postoperative period that required debridement and a new graft, the absence of bone union during follow-up or a new bone defect treatment (bone transport, amputation, etc.). Preoperative infection refers to the presence of infection (active or quiescent) or absence of it when bone defect treatment was implemented. Postoperative infection was infection reported as a complication after bone graft procedure. We considered that PMMA was used as an adjuvant in bone defect treatment (induced membrane technique) only when authors reported its use for this purpose.
Assessment of publication bias
Susceptibility of the systematic review to publication bias was formally assessed with the Egger test [11].
Quantitative data synthesis
To stabilize variance, the bone union proportions were subject to a Freeman-Tukey arcsine square root transformation and back-transformed according to Miller after quantitative data synthesis [12, 13]. With the normalized data, heterogeneity was assessed using both Cochran’s Q test and the inconsistency measure I2 suggested by Higgins [14]. A cut-off of P < 0.10 was used to indicate heterogeneity. Values of I2 equal to 25 %, 50 % and 75 % denoted a low, moderate and high degree of statistical heterogeneity. As data from a series of studies that had been performed independently are thought to be not functionally equivalent, a random effects model approach was used to combine estimates. Confidence intervals within studies were achieved using the exact binomial method. To perform a sub-group analysis, the studies were divided according to graft vascularization in two major categories: non-vascularized bone graft or vascularized bone graft. Analyses were performed using STATA (version 13.0) and Comprehensive Meta-analysis (version 2.0).
Results
Selection of studies
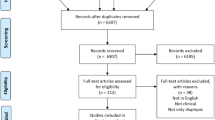
The Medline search resulted in 338 citations and after the abstract review 21 were considered as potentially eligible and all of them had the full version reviewed. References of these articles were manually screened and also the related citations tool resulting in further 38 potentially eligible articles, totaling 59 papers to review. The Cochrane Library search did not result in additional studies. After the full version review, 34 studies met the inclusion/exclusion criteria (Fig. 1) (Additional file 2). In seven of the 34 studies some cases were excluded from the analysis (Additional file 3). A total of 749 patients with 750 bone defects were included in this meta-analysis.

Flowchart of literature review
Concerning study characteristics, one was a randomized controlled trial, one was a prospective case series, three were retrospective comparative case series and 29 were retrospective case series (Table 1). Only Pelissier et al. [15] was a comparison between vascularized and non vascularized bone graft. The studies achieved 37.1 points (21 to 72) out of 100 in the quality assessment tool. The inter rater agreement in regards to the quality assessment between the reviewers was considerably high (ICC = 0.78; 95 % CI 0.75 to 0.94).
Publication bias
The shape of the funnel plot revealed evidence of asymmetry for both primary and secondary union (Fig. 2). The Egger’s test showed evidence of publication bias (p < 0.001 for primary union and p < 0.001 for secondary union).

Funnel plot comparing proportion versus the standard error of proportion for the outcome of (a) primary union and (b) secondary union. The assessment of the Egger test was coupled with an informal visual inspection of the funnel plot where circles represent studies included in the meta-analysis. The solid vertical line indicates no union in terms of proportion. The outer dashed line indicate the triangular region within which 95 % of studies are expected to lie in absence of both bias and heterogeneity (random effect pooled proportion ± 1.96 × standard error of pooled proportion). Asymmetry about the pooled proportion line is consistent with the presence of publication bias
Bone union rate
Primary bone union was documented in 33 studies [15–47] (Q = 87.53, df = 32, P <0.001; I2 = 63.4 %) and secondary bone union was documented in 34 studies [15–48] (Q = 38.65, df = 33, P =0.23; I2 = 14.6 %). Union rates as primary ranged between 48 % and 100 % across eligible studies. Using random-effects weights, the summary (pooled) union rate was 91 % (95 % CI: 87–95 %). Union rates as secondary ranged between 81 % and 100 % across eligible studies. Using random-effects weights, the summary (pooled) union rate was 98 % (95 % CI 96–99 %).
For comparison of vascularized versus non-vascularized graft the study from Toh et al. [18] and the study from Muramatsu et al. [20] were omitted as they used a mixed technique. The study of Pelissier et al. [15] included patients treated either with vascularized or non-vascularized graft, thus this publication contributed to both groups in the sub-group analysis (Table 2).
When analyzing the primary bone union, significant intra-group heterogeneity was observed (Vascularized: Q = 37.07, df = 18, P < 0.01; I2 = 51.4 %; Non-vascularized: Q = 47.48, df = 12, P < 0.001; I2 = 74.7 %). However, there was no statistical difference between the two groups (P = 0.372) supporting the pooling of all studies into one pooled measure. Using random-effects weights, the summary (pooled) union rate was 93 % (95 % CI: 89–97 %) for the vascularized group and 89 % (95 % CI: 79–97 %) for the non-vascularized group (Fig. 3a).

Forest plot of bone union (% of union rates) in patients with vascularized and non-vascularized bone graft (random effects model). a Primary union b Secondary union
Meta-regression was performed to investigate potential sources of heterogeneity within study for primary bone union. The main factor investigated was bone defect size additionally adjusted for age and proportion of female patients. Both univariable and multivariable meta-regression did not show any association of union rate and bone defect size (Univariable: vascularized: P = 0.677; non-vascularized: 0.202. Multivariable: vascularized: P = 0.381; non-vascularized: P = 0.226).
When analyzing the secondary bone union, no significant intra-group heterogeneity was observed (Vascularized: Q = 18.22, df = 19, P = 0.508; I2 = 0.0 %; Non-vascularized: Q = 15.20, df = 12, P = 0.231; I2 = 21.0 %), neither difference between groups was noted (P = 0.106). Using random-effects weights, the summary (pooled) secondary union rate was 98 % (95 % CI: 97–100 %) for the vascularized group and 96 % (95 % CI: 91–99 %) for the non-vascularized group (Fig. 3b).
Infection pre and post-treatment
Infection status of the cases was reported pre- and post-operative in 22 studies [16, 18, 19, 21, 23, 24, 26, 27, 29–33, 35, 36, 40, 41, 43–47]. The pooled estimate of mean effect size showed about 6-fold decrease of infection after treatment compared with pre-operative situation (OR = 0.17 (95 % CI 0.08 to 0.36), p < 0.001; Q = 58.6, p < 0.001, df = 21, I2 = 64.2 %). Therefore, a subgroup analysis was performed. A significant decrease of post-treatment infection was observed among the vascularized graft group (n = 12; OR = 0.08 (95 % CI 0.03 to 0.23), p < 0.001) but not in the non-vascularized group (n = 10; OR = 0.43 (95 % CI 0.15 to 1.22), p = 0.114). Moreover, a statistical difference between the two groups was found (Q = 4.350; P = 0.037) (Fig. 4).

Forest plot of the odds ratio of bone infection before and after bone graft treatment stratified by type of graft (vascularized and non-vascularized)
As heterogeneity in the subgroup analysis may be due to the presence of outlying studies, a sensitivity analysis was conducted excluding the studies that presented the highest OR (Jones et al. [27], Ristiniemi et al. [29] and Niu et al. [41]). After these studies were excluded a moderate degree of heterogeneity (I2 = 63.7 %) was found. In the sensitivity analysis there was no statistical difference between the two techniques (Q = 1.146; P = 0.284) and the non-vascularized group also showed a statistically significant decrease of post-operative infection (n = 7; OR = 0.207 (95 % CI 0.06–0.77)).
Additionally, investigation of heterogeneity was performed by means of meta-regression including age, percentage of females and months of delay from injury to treatment. No variables showed a significant association with the risk of post-treatment infection.
Discussion
Bone union
The primary bone union rate expected for the bone graft techniques is 91 %. In some circumstances, additional procedures such as the change of a broken implant, compression in the nonunion site or cancellous graft in nonunion areas at bone ends, may be necessary and they raised the union rate to 98 % in published studies (Additional file 4) [15, 17–23, 25–31, 33–35, 39, 41, 42, 46–48].
Defect size as a guide to select graft
Only few studies presented a description of the method used to define and measure the bone defect [27, 29, 31, 46]. Small defects that might have been susceptible to spontaneous regeneration were present in some studies. They were treated not only with non-vascularized graft but also with vascularized bone graft.
Studies about vascularized bone grafts have been performed on larger bone defects but association of union rate and bone defect size wasn’t found between the vascularized and non-vascularized grafts. Limitations of this conclusion include also a potential selection bias: some recent studies about non-vascularized graft were excluded because of the addition of growth factor or biomaterial to the graft. Despite the limitation of this study, our data suggests that selection of graft technique shall not be guided only by defect size. Patient expectations, surgeon experience, soft tissue condition and a trained staff to perform microsurgery are elements that must be carefully judged before making a decision on the graft to be used.
Infection pre- post-treatment
The pooled estimate of mean effect size showed a decrease of infection after treatment compared with the pre-operative situation. However, these findings should be interpreted with caution due to the presence of a moderate degree of statistical heterogeneity. According to the results of this meta-analysis, vascularized graft showed a significant decrease of post-treatment infection. Again, this conclusion is limited. Infection definition varies between the included studies and several different surgical techniques were used. Although we cannot give evidence to support this recommendation, most of the studies suggest a two step reconstruction as the standard approach to manage infected bone defects: an extensive debridement, followed by antibiotic treatment before graft surgery [16, 21, 26, 29, 31, 32, 36, 40, 43, 44]. Furthermore, some of the studies use PMMA as a local antibiotic delivery and/or due to its ability to induce a biological membrane at the defect site [21, 29, 32–34, 36].
Overall completeness and applicability of evidence
The included studies provide the most complete information available concerning union rates after autologous graft for bone defects; however, different factors may have added to the heterogeneity of the pooled results, such as different treatment techniques, different sample sizes reflecting different levels of experience, incomplete information about complications. Additionally, information regarding surgical steps was limited in several studies. Finally, data concerning potential confounding factors, such as patients selection criteria, soft tissue treatment and definition of complications were also incomplete.
Quality of the evidence
The overall quality of the included studies is poor. Most of them are nonrandomized observational studies with serious limitations. There was evidence of publication bias for primary and secondary bone union, with higher union rates in bigger studies. Overall sample size allows obtaining several statistically significant results. However, the level of evidence of these findings is low or very low due to the heterogeneity of the pooled data and the risk of bias caused by the studies’ design.
Conclusion
This study states the effectiveness of autologous graft for bone defects. Overall union rate was 91 % while union rate after additional procedures raised to 98 % in published studies. Available clinical evidence does not show a direct relation between bone defect size and bone union rate when autologous bone graft techniques were applied. Therefore, bone defect size should not be the only factor used when choosing between vascularized or non vascularized bone graft. Finally, pooled analysis stated that in the presence of infection, vascularized graft has a lower risk of post-surgery infection. Well-designed randomized, controlled trials are needed to raise the low level of evidence for those conclusions.
Abbreviations
- PMMA:
-
Polymethylmethacrylate
References
Myeroff C, Archdeacon M. Autogenous bone graft: donor sites and techniques. J Bone Joint Surg Am. 2011;93:2227–36.
Ashman O, Phillips AM. Treatment of non-unions with bone defects: Which option and why? Injury. 2013;44(1):S43–5.
Mauffrey C, Barlow BT, Smith W. Management of segmental bone defects. J Am Acad Orthop Surg. 2015;23(3):143–53.
Cox G, Jones E, McGonagle D, et al. Reamer-irrigator-aspirator indications and clinical results: A systematic review. Int Orthop. 2011;35(7):951–6.
Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin N Am. 2010;41(1):27–37.
Egol KA, Nauth A, Lee M, et al. Bone Grafting: Sourcing, Timing, Strategies, and Alternatives. J Orthop Trauma. 2015;29(12):S10–4.
Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–12.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann Intern Med. 2009;151(4):W65–94.
Coleman BD, Khan KM, Maffulli N, Victorian Institute of Sport Tendon Study Group, et al. Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Scand J Med Sci Sports. 2000;10(1):2–11.
Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Freeman MF, Tukey JW. Transformations related to the angular and the square root. Ann Math Stat. 1954;21:607–11.
Miller JJ. The inverse of the Freeman-Tukey double arcsine transformation. Am Statistic. 1978;32(4):138.
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Pelissier P, Boireau P, Martin D, et al. Bone reconstruction of the lower extremity: complications and outcomes. Plast Reconstr Surg. 2003;111(7):2223–9.
Ring D, Jupiter JB, Quintero J, et al. Atrophic ununited diaphyseal fractures of the humerus with a bony defect: treatment by wave-plate osteosynthesis. J Bone Joint Surg Br. 2000;82(6):867–71.
Tu YK, Yen CY, Yeh WL, et al. Reconstruction of posttraumatic long bone defect with free vascularized bone graft: good outcome in 48 patients with 6 years’ follow-up. Acta Orthop Scand. 2001;72(4):359–64.
Toh S, Tsubo K, Nishikawa S, et al. Ipsilateral pedicle vascularized fibula grafts for reconstruction of tibial defects and non-unions. J Reconstr Microsurg. 2001;17(7):487–96.
Heitmann C, Erdmann D, Levin LS. Treatment of segmental defects of the humerus with an osteoseptocutaneous fibular transplant. J Bone Joint Surg Am. 2002;84(12):2216–23.
Muramatsu K, Doi K, Ihara K, et al. Recalcitrant posttraumatic nonunion of the humerus: 23 patients reconstructed with vascularized bone graft. Acta Orthop Scand. 2003;74(1):95–7.
Yajima H, Kobata Y, Shigematsu K, et al. Vascularized fibular grafting in the treatment of methicillin-resistant Staphylococcus aureus osteomyelitis and infected nonunion. J Reconstr Microsurg. 2004;20(1):13–20.
Lee KS, Han SB, Baek JR. Free vascularized osteocutaneous fibular graft to the tibia in 51 consecutive cases. J Reconstr Microsurg. 2004;20(4):277–84.
Adani R, Delcroix L, Innocenti M, et al. Reconstruction of large posttraumatic skeletal defects of the forearm by vascularized free fibular graft. Microsurgery. 2004;24(6):423–9.
Ring D, Allende C, Jafarnia K, et al. Ununited diaphyseal forearm fractures with segmental defects: plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am. 2004;86(11):2440–5.
Yazar S, Lin CH, Wei FC. One-stage reconstruction of composite bone and soft-tissue defects in traumatic lower extremities. Plast Reconstr Surg. 2004;114(6):1457–66.
Safoury Y. Free vascularized fibula for the treatment of traumatic bone defects and nonunion of the forearm bones. J Hand Surg Br. 2005;30(1):67–72.
Jones AL, Bucholz RW, Bosse MJ, et al. Recombinant human BMP-2 and allograft compared with autogenous bone graft for reconstruction of diaphyseal tibial fractures with cortical defects. A randomized, controlled trial. J Bone Joint Surg Am. 2006;88(7):1431–41.
El-Sayed M, El-Hadidi M, El-Adl W. Free non-vascularised fibular graft for treatment of post-traumatic bone defects. Acta Orthop Belg. 2007;73(1):70–6.
Ristiniemi J, Lakovaara M, Flinkkilä T, et al. Staged method using antibiotic beads and subsequent autografting for large traumatic tibial bone loss: 22 of 23 fractures healed after 5-20 months. Acta Orthop. 2007;78(4):520–7.
Adani R, Delcroix L, Tarallo L, et al. Reconstruction of posttraumatic bone defects of the humerus with vascularized fibular graft. J Shoulder Elbow Surg. 2008;17(4):578–84.
Ryzewicz M, Morgan SJ, Linford E, et al. Central bone grafting for nonunion of fractures of the tibia: a retrospective series. J Bone Joint Surg Br. 2009;91(4):522–9.
Allende C, Mangupli M, Bagliardelli J, et al. Infected nonunions of long bones of the upper extremity: staged reconstruction using polymethylmethacrylate and bone graft impregnated with antibiotics. Chir Organi Mov. 2009;93(3):137–42.
Cavadas PC, Landín L, Ibáñez J, et al. Reconstruction of major traumatic segmental bone defects of the tibia with vascularized bone transfers. Plast Reconstr Surg. 2010;125(1):215–23.
McCall TA, Brokaw DS, Jelen BA, et al. Treatment of large segmental bone defects with reamer-irrigator-aspirator bone graft: technique and case series. Orthop Clin North Am. 2010;41(1):63–73.
Sun Y, Zhang C, Jin D, et al. Free vascularised fibular grafting in the treatment of large skeletal defects due to osteomyelitis. Int Orthop. 2010;34(3):425–30.
Apard T, Bigorre N, Cronier P, et al. Two-stage reconstruction of post-traumatic segmental tibia bone loss with nailing. Orthop Traumatol Surg Res. 2010;96(5):549–53.
Zhen P, Hu YY, Luo ZJ, et al. One-stage treatment and reconstruction of Gustilo Type III open tibial shaft fractures with a vascularized fibular osteoseptocutaneous flap graft. J Orthop Trauma. 2010;24(12):745–51.
Chai YM, Wang CY, Zeng BF, et al. Peroneal artery perforator chimeric flap for reconstruction of composite defects in extremities. Microsurgery. 2010;30(3):199–206.
Georgescu AV, Ignatiadis I, Ileana M, et al. Long-term results after muscle-rib flap transfer for reconstruction of composite limb defects. Microsurgery. 2011;31(3):218–22.
Chung DW, Han CS, Lee JH. Reconstruction of composite tibial defect with free flaps and ipsilateral vascularized fibular transposition. Microsurgery. 2011;31(5):340–6.
Niu Y, Bai Y, Xu S, et al. Treatment of lower extremity long bone nonunion with expandable intramedullary nailing and autologous bone grafting. Arch Orthop Trauma Surg. 2011;131(7):885–91.
Liang K, Cen S, Xiang Z, et al. Massive juxta-articular defects of the distal femur reconstructed by series connected double-strut free-vascularized fibular grafts. J Trauma Acute Care Surg. 2012;72(2):E71–6.
Gulan G, Jotanović Z, Jurdana H, et al. Treatment of infected tibial nonunion with bone defect using central bone grafting technique. Coll Antropol. 2012;36(2):617–21.
Liang K, Xiang Z, Chen S, et al. Folded free vascularized fibular grafts for the treatment of subtrochanteric fractures complicated with segmental bone defects. J Trauma Acute Care Surg. 2012;72(5):1404–10.
Gao YS, Ai ZS, Yu XW, et al. Free vascularised fibular grafting combined with a locking plate for massive bone defects in the lower limbs: a retrospective analysis of fibular hypertrophy in 18 cases. Injury. 2012;43(7):1090–5.
Niu Y, Bai Y, Xu S, et al. Treatment of bone nonunion and bone defects associated with unsuccessful humeral condylar fracture repair with autogenous iliac bone reconstruction. J Shoulder Elbow Surg. 2012;21(8):985–91.
Özaksar K, Sügün TS, Toros T, et al. Free vascularized fibular grafts in Type 3 open tibia fractures. Acta Orthop Traumatol Turc. 2012;46(6):430–7.
El-Gammal TA, Shiha AE, El-Deen MA, et al. Management of traumatic tibial defects using free vascularized fibula or Ilizarov bone transport: a comparative study. Microsurgery. 2008;28(5):339–46.
Acknowledgements
The authors would like to thank the whole AOCID (AO Clinical Investigation and Documentation) team for the support developing the manuscript.
Funding
No funding was obtained for this study.
Availability of data and materials
Data was presented in the main text and in the additional files. It is also available from published papers as per references.
Authors’ contributions
MA and AA made substantial contributions to: conception and design, acquisition of data, analysis and interpretation of data, drafting of manuscript and its critical revision. IS made substantial contributions to: analysis and interpretation of data, drafting of manuscript and its critical revision. MK and AM made substantial contributions to: drafting of manuscript and its critical revision. AJ made substantial contributions to: conception and design, interpretation of data, drafting of manuscript and its critical revision. All of the authors reviewed and approved the final version.
Competing interests
MA and AA were supported by the AO foundation via an AO Trauma fellowship at AOCID. None of the authors has received any financial support from any commercial company or institution directly or indirectly related to the subject of this article.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Additional files
Additional file 1:
Table modified Coleman methodology score for bone defect. (DOCX 74 kb)
Additional file 2:
Table studies excluded after full text review. (DOCX 99 kb)
Additional file 3:
Table removed cases from included studies and technical notes. Technical notes represent values related to the entire sample of the studies where it was not possible to individualize data of the included cases. (DOCX 52 kb)
Additional file 4:
Table additional procedures to achieve healing. (DOCX 60 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Azi, M.L., Aprato, A., Santi, I. et al. Autologous bone graft in the treatment of post-traumatic bone defects: a systematic review and meta-analysis. BMC Musculoskelet Disord 17, 465 (2016). https://doi.org/10.1186/s12891-016-1312-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-016-1312-4