
Abstract
Background
Little is known about the differences in medium to long-term recovery on spirometry, 6-minute walking distance (6MWD) and health-related quality of life (HRQoL) between COVID-19 and SARS.
Methods
We performed a 12-month prospective study on COVID-19 survivors. The changes in dynamic lung volumes at spirometry (%predicted FEV1, %predicted FVC), 6MWD and HRQoL at 1–3, 6 to 12 months were compared against a historical cohort of SARS survivors using the same study protocol. The residual radiological changes in HRCT in COVID-19 survivors were correlated with their functional capacity.
Results
108 COVID-19 survivors of various disease severity (asymptomatic 2.9%, mild 33.3%, moderate 47.2%, severe 8.3%, critical 8.3%) were recruited. When compared with 97 SARS survivors, 108 COVID-19 survivors were older (48.1 ± 16.4 vs. 36.1 ± 9.5 years, p < 0.001) and required less additional support during hospitalization; with lower dynamic lung volumes, shorter 6MWD and better physical component score. Both groups of survivors had comparable changes in these parameters at subsequent follow-ups. Both COVID-19 and SARS survivors had similar mental component score (MCS) at 6 and 12 months. COVID-19 survivors initially experienced less (between-group difference, -3.1, 95% confidence interval [CI] -5.5 to -0.7, p = 0.012) and then more improvement (between-group difference 2.9, 95%, CI 0.8 to 5.1, p = 0.007) than SARS survivors in the MCS at 1–3 to 6 months and 6 to 12 months respectively. Forty (44.0%) out of 91 COVID-19 survivors had residual abnormalities on HRCT at 12 months, with a negative correlation between the severity scores of parenchymal changes and 6MWD (r=-0.239, p < 0.05).
Conclusions
COVID-19 survivors demonstrated a similar recovery speed in dynamic lung volumes and exercise capacity, but different paces of psychological recovery as SARS survivors in the convalescent phase. The severity of parenchymal changes in HRCT is negatively correlated with the 6MWD of COVID-19 survivors.
Trial registration
This prospective study was registered at ClinicalTrials.gov on 2 November 2020 (Identifier: NCT04611243).
Similar content being viewed by others


Introduction
The outbreak of coronavirus disease 2019 (COVID-19) emerged since the end of 2019 has resulted in over 769 million confirmed cases and 6.9 million deaths globally [1]. In Hong Kong (HK), there were 2,876,106 confirmed COVID-19 cases and 13,333 related deaths as of 12 April 2023 [2]. Although the extent of impairment, in terms of lung function, exercise tolerance, health-related quality of life (HRQoL) and radiological findings after recovery has been reported, the results were variable owing to differences in the admission criteria, treatment options and background demographics [3,4,5,6,7,8,9,10,11]. In HK, all patients diagnosed with COVID-19 before February 2022 were hospitalized for isolation purposes, irrespective of disease severity. This provided an opportunity for prospective longitudinal assessments of a full spectrum of asymptomatic to critical COVID-19 subjects.
In contrast, severe acute respiratory syndrome (SARS), caused by SARS-CoV-1, from late 2002 to mid-2003, resulted in 8,098 patients infected worldwide and 774 deaths [12]. Significant impairment in lung function, exercise capacity and health status among SARS survivors one year after illness were remarkably lower than in a normal population [13]. Although the case-fatality rate of COVID-19 was lower than that of SARS (0.4% vs. 9.6%), [14] no study compared the long-term recovery between COVID-19 and SARS survivors. A comparative study would characterize and inform long-term management strategies for emerging coronavirus infection. We hypothesize that the recovery trajectory of COVID-19 survivors followed a better trend than SARS survivors, taking into consideration varying disease severity and level of care at the baseline. Our study aimed to evaluate the differences in the medium to long-term longitudinal changes in dynamic lung volumes, exercise tolerance and HRQoL between COVID-19 and SARS survivors.
Study design and methods
Subjects
This is an ongoing longitudinal, follow-up study of patients with COVID-19 discharged after surviving the major outbreak in HK from 5 to 2020 to 17 September 2020 from three tertiary care hospitals. Consecutive patients, irrespective of their disease severity, consenting to this study were recruited. All recruited patients had laboratory confirmation of SARS-CoV-2 by reverse transcription-polymerase chain reaction of the respiratory specimens and were hospitalized for isolation purposes. Patients who refused to join the study or cognitively impaired were excluded. A historical cohort containing 97 consecutive SARS patients after surviving the major outbreak in 2003, who were discharged between 28 and 2003 and 26 Jul 2003, was included for comparison [13]. The sample size of COVID-19 survivors was not predefined, as there was no prior data comparing SARS and COVID-19 survivors available. Therefore, we prospectively recruited patients who were admitted during the first three waves of COVID-19 community spread in Hong Kong (between February and August 2020). The recruitment was stopped due to a low level of community spread between the third and fourth waves. A matching criteria between the two groups of survivors were not applied as the disease behaviour of COVID-19 was not completely revealed during the recruitment period.
This prospective study was approved by the Clinical Research Ethics Committees of the Chinese University of Hong Kong (CREC-2020.229) and registered at ClinicalTrials.gov (Identifier: NCT04611243). The study was performed in accordance with Declaration of Helsinki.
Assessment
Following hospital discharge, COVID-19 survivors were evaluated at 1 to 3 months (a wide range of timings was allowed depending on the patient’s recovery and policy of social restriction), 6 and 12 months after discharge. During the visit, subjects were evaluated for baseline demographics, premorbid conditions, pulmonary function tests (measuring static and dynamic lung volumes, and diffusion capacity for carbon monoxide [DLCO]), 6-minute walk test (6MWT), and Medical Outcomes Study 36-Item Short-Form General Health Survey (SF-36) questionnaire. Respiratory comorbidities included underlying chronic airway or structural parenchymal diseases, including chronic obstructive pulmonary disease (COPD) and asthma (as defined by Global Initiative for Chronic Obstructive Lung Disease and Global Initiative for Asthma). This assessment package was performed according to international standards and used for assessing SARS survivors in 2003, [13, 15,16,17,18,19,20]with details explained in Appendix S1. The physiological and functional parameters assessed were compared to the normative data of HK [21,22,23,24]. Only patients who had completed both 6 and 12-month clinical follow-ups were included for statistical analysis.
High-resolution computed tomography (HRCT)
All COVID-19 survivors underwent a thin-section HRCT from the lung apices to the diaphragm at 12 months. The involvement of parenchymal changes was defined by a combination of consolidation, ground-glass opacity (GGO) and fibrosis, with the extent of involvement in each lobe graded, similar to previously described studies for SARS [25, 26]and COVID-19 [27, 28]. The radiological descriptive terms were based on the glossary defined by the Fleischner Society [29]. The details of the scanning protocol are explained in Appendix S2.
Study outcomes
The primary outcomes were the between-group differences in the longitudinal changes of dynamic lung volumes, 6-minute walking distance (6MWD) and SF-36 scores from 6 to 12 months between COVID-19 and SARS survivors. The secondary outcomes included the within-group and between-group comparison of these parameters between COVID-19 survivors, SARS survivors and HK normative data at different time points, identification of factors determining the longitudinal changes, and the presence of residual radiological abnormalities on HRCT at 12 months and its correlation with baseline characteristics and various functional parameters.
Statistical analysis
STROBE guideline was applied. Data were presented as n (%) or mean with standard deviation (SD), as appropriate. Independent t-tests and paired t-tests were used to compare the between-group and within-group differences in the changes in dynamic lung volumes, 6MWD and HRQoL over different time points respectively. Multivariate analysis (analysis of variance with repeated measures) incorporating the need for oxygen and corticosteroids during hospitalization, age and sex [17, 24] was performed to evaluate the potential determinants of these longitudinal changes. The need for additional support during hospitalization was included as the independent variable in the analysis as there was no shared severity score for both diseases. Spearman correlations were used to analyze associations among radiological changes, lung function tests and 6MWD at 12 months. Data were analyzed using SPSS version 26.0 (IBM Corp., USA). All statistical tests were two-tailed. Statistical significance was taken as p < 0.05. The details of the statistical analysis are explained in Appendix S3.
Results
Baseline characteristics of COVID-19 survivors
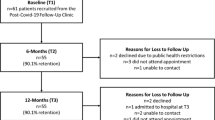
Five hundred and ninety COVID-19 patients were screened and 268 patients refused to join the study. Two hundred and fourteen COVID-19 survivors dropped out from subsequent follow-ups for various reasons, and only 108 of them completed both 6 and 12-month follow-ups. The number of COVID-19 and SARS survivors who underwent various clinical assessments throughout the study is shown in Fig. 1. During the COVID-19 outbreak, especially during the 1-to-3-month follow-up, clinical assessment including full lung function test (lung volumes and DLCO) and 6MWT was heavily compromised due to infection control concerns among the nursing staff. However, the demographics and outcomes of those who had performed spirometry, 6MWT during the 1-to-3-month follow-up, full lung function tests at 6 and 12 months, and those who did not were largely comparable (Tables S1-S2).

Number of COVID-19 and SARS survivors who had completed the clinical assessments at different time points. a 41 COVID-19 survivors who performed spirometry both at months 1 to 3 and 6. b 53 COVID-19 survivors who performed 6-minute walking tests at months 1 to 3 and 6. c 89 COVID-19 survivors who performed spirometry both at months 6 and 12. d 104 COVID-19 survivors who performed 6-minute walking tests both at months 6 and 12. 6MWT: 6-minute walking test; COVID-19: coronavirus disease 2019; CXR: chest X-ray; DLCO: diffusion capacity of carbon monoxide; HRCT: high-resolution computed tomography; SARS: severe acute respiratory syndrome; SF-36: Medical Outcomes Study 36-Item Short-Form General Health Survey
Among the 108 COVID-19 survivors, nearly half (52, 48.1%) were men with a mean age of 48.1 ± 16.4 years. None of them had COVID-19 reinfection, and all were unvaccinated with any COVID-19 vaccines before the completion of the study. The circulating strains of SARS-CoV-2 viruses involved in HK were the Wuhan wild type and D614G variant from May to October 2020. However, information on the specific variant was unavailable for individual COVID-19 survivors. The treatment used for COVID-19 during hospitalization is listed in Table S3. Only 2 (1.9%) COVID-19 survivors, but none of the SARS survivors had received lung function tests before the acute infection.
According to the World Health Organization (WHO) classifications of COVID-19 severity, [30] 3 (2.9%), 36 (33.3%), 51 (47.2%), 9 (8.3%) and 9 (8.3%) had asymptomatic, mild, moderate, severe and critical diseases respectively. The diagnosis of pneumonia was defined by clinical signs, symptoms (fever, cough, dyspnoea, tachypnoea) and chest imaging, with its severity based on the occurrence of haemodynamic and respiratory compromise. The disease severity of COVID-19 subjects who were either excluded from screening or subsequent follow-ups was listed in Table S4. Patients who had required intensive care unit (ICU) admission, oxygen, mechanical ventilation (MV) and received corticosteroids were older than those who did not require these treatment modalities. COVID-19 survivors who had required ICU admission or MV had higher %predicted dynamic lung volumes at 6 and 12 months than their counterparts (Tables S5-S6).
Comparison of COVID-19 survivors, SARS survivors and HK normative data
Compared with the historical cohort of 97 SARS survivors, COVID-19 survivors were older with more comorbidities, similar MV usage but required fewer ICU admissions and oxygen during hospitalization. Sixty-nine (63.9%) and 90 (92.8%) of COVID-19 and SARS survivors had pneumonia respectively. Significantly more SARS survivors underwent pulmonary rehabilitation than COVID-19 survivors. None of the survivors in both groups required long-term oxygen therapy after the index infections (Table 1). Further subgroup analyses based on the level of care are shown in Tables S7-S8.
Both COVID-19 and SARS survivors had %predicted forced expiratory volume in 1 s (FEV1), %predicted forced vital capacity (FVC) and static lung volumes within or above the normal range at 6 and 12 months. The %predicted FEV1 and %predicted FVC at all 3 visits, and %predicted DLCO at 12 months were lower among COVID-19 survivors (Table 2; Fig. 2A and B). At all 3 visits, the PCS and MCS of both COVID-19 and SARS survivors were generally lower than normal. COVID-19 survivors experienced shorter 6MWD (especially in the younger age groups), but better PCS, MCS (at 1–3 months) and individual SF-36 domains than SARS survivors (Table 3, S9-S12, Fig. 2 C to 2G).

Within-group and between-group differences in serial changes of various physiological parameters and health-related quality of life between COVID-19 and SARS survivors at different time points. Differences are shown in mean ± standard deviation (95% confidence interval) followed by p-value. A: FEV1, B: FVC; C: 6-minute walking distance of the whole cohort; D: 6-minute walking distance of male survivors; E: 6-minute walking distance of female survivors; F: physical component score; G: mental component score. CI: confidence interval; COVID-19: coronavirus disease 2019; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; SARS: severe acute respiratory syndrome
Residual radiological abnormalities on HRCT
Ninety-one COVID-19 survivors underwent HRCT at 12 months, and 40 (44.0%) had radiological abnormalities. Twenty-three (25.3%) patients had parenchymal bands, 13 (14.3%) had pleural thickening, 12 (13.2%) had interlobular lines, 12 (13.2%) had GGO, 7 (7.7%) had bronchiectasis, 4 (4.4%) had mosaic attenuation and 2 (2.2%) had emphysema. None had consolidation, honeycombing, pleural effusion or thoracic lymphadenopathy on the HRCT. The distribution and involvement of GGO, fibrosis and parenchymal changes in each lobe are shown in Figure S1. These radiological abnormalities and their severities were closely related to the need for ICU admission, oxygen, MV and corticosteroids use during hospitalization. The severity scores of involvement by fibrosis and parenchymal changes correlated negatively with 6MWD, but not other lung function parameters at 12 months, while the involvement by GGO was independent of the 6MWD and lung function parameters (Tables S13-S14).
Within-group differences over 12 months
Both COVID-19 and SARS survivors did not experience significant changes in dynamic lung volumes and PCS between follow-ups. The mean 6MWD of COVID-19 survivors (whole cohort: 3.5 to 32.1 m from 1–3 to 6 month, p = 0.015; 7.5 to 28.1 m, p = 0.001), especially among females (1.8 to 38.6 m from 1–3 to 6 month, p = 0.033; 7.6 to 38.0 m from 6 to 12 month, p = 0.004), increased between the three follow-ups. The MCS of COVID-19 survivors also improved from 6 to 12 months. SARS survivors only had improvement in 6MWD, especially among males, and MCS from 1–3 to 6 months (Tables S15-S17, Fig. 2A and G).
Between-group differences over 12 months
There was no significant difference in changes in %predicted FEV1, %predicted FVC, 6MWD and PCS throughout 12 months between COVID-19 and SARS survivors. Although SARS survivors experienced greater improvement in MCS and some SF-36 domains from 1–3 to 6 months than the COVID-19 survivors, they had a decline in MCS and several other SF-36 domains from 6 to 12 months (Table 4; Fig. 2A and G).
Regression analysis retained the presence of respiratory comorbidities as being independently associated with the improvement of %predicted FEV1, %predicted FVC and 6MWD, while age ≥ 40 years old was associated with the improvement of MCS in the pooled cohort of COVID-19 and SARS survivors from 6 to 12 months (Table S18).
Multivariate analysis retained the presence of respiratory comorbidities as being independently associated with the improvement of %predicted FEV1, %predicted FVC and MCS, whereas the use of oxygen and the presence of parenchymal changes on HRCT at 12 months were associated with the change in 6MWD in COVID-19 survivors from 6 to 12 months (Table S19).
Discussion
To the best of our knowledge, this is the first study directly comparing various physiological and functional domains between COVID-19 and SARS survivors from a longitudinal perspective. The current cohort included a full spectrum of COVID-19 survivors, ranging from asymptomatic to critical diseases, who were compared with SARS survivors. COVID-19 and SARS survivors reached a similar score on the MCS, but had different paces in the recovery of MCS, with more improvement from 6 to 12 months in the COVID-19 survivors. Despite a difference in the age, baseline comorbid status and disease severity, there was no difference in the change of dynamic lung volumes, 6MWD and PCS between the two groups between 1–3 and 6 months and from 6 to 12 months. When focusing on the changes from 6 to 12 months, the presence of respiratory comorbidities was an essential factor associated with the improvement of various physiological parameters in the pooled cohort of COVID-19 survivors alone. Residual radiological changes were common among COVID-19 survivors, and specific patterns were associated with shorter 6MWD and additional support during hospitalization.
The observations in the study support a similar medium to long-term physiological recovery trajectory after COVID-19 and SARS. The findings of relatively normal dynamic lung volumes with low DLCO [7, 8, 31] and reduced 6MWD [3, 32] were also reported by other prospective cohorts. COVID-19 survivors, who had a less eventful course of disease and comparable baseline smoking status, in general, had consistently inferior age-adjusted dynamic lung volumes than SARS survivors. The commonly found residual radiological changes among SARS [13] and COVID-19 survivors [7, 31,32,33,34,35] may contribute to the persistently lower physiological capacity, especially spirometry performance, [5, 32] gas exchange [7, 13, 32] and 6MWD [7, 32]than normal population. Although the radiological changes are common in our cohort, and were associated with a shorter and slower recovery of 6MWD, we could not confirm its association with dynamic lung volumes (similar to SARS survivors) [13]and DLCO (due to limited data available) [36]. All these suggest the detrimental role of parenchymal involvement as a major determinant of long-term physiological recovery in COVID-19 and SARS survivors [13]. Recent data suggested COVID-19 survivors may have persistent and non-progressive fibrotic changes on CT thorax at a rate of 10–24%, which is comparable to our cohort [5, 37]. It should be realized that factors determining the exercise capacity in COVID-19 survivors could be more complicated and multifactorial. Emerging data suggested that these survivors may have physical deconditioning, as reflected by cardiopulmonary exercise test performance, which is independent of residual radiological and lung function abnormalities, and leading to a reduction in physical capacity [38, 39]. Similar results had been reported for SARS survivors [40].
The positive and independent association of baseline respiratory comorbidities (mainly COPD and asthma in COVID-19 and SARS survivors respectively) and medium to long-term recovery of physiological parameters is a novel finding. This may reflect a slow but progressive recovery of airway status after the initial insult in susceptible patients, which was also observed in patients with COPD after exacerbations in medium-term prospective studies [41]. However, the relatively small number, paucity of baseline lung function test before the index infection and lack of other types of respiratory diseases may preclude the generalization of this result. Although various studies have examined the long-term physiological effects and exercise capacity of COVID-19 survivors, limited data has addressed the physiological recovery trajectory in those with pre-existing chronic airway diseases. A nationwide survey in the United Kingdom found that patients with asthma had increased inhaler use and worse asthma management after COVID-19 infection, but this was not accompanied with any physiological measurements [42].
Despite the older age and inferior physiological capacity, COVID-19 survivors outperformed SARS survivors in most SF-36 domains at different time points and they demonstrated differential paces of recovery. This could be due to a less severe disease course during hospitalization and implied that the HRQoL status cannot be fully translated by the inferior physical status (dynamic lung volumes and 6MWD). The initial slower improvement and later overtaking of MCS in COVID-19 survivors, in comparison with SARS survivors, merits attention. Non-measurable factors, in addition to physiological impairment imposed on individuals, should be considered in the COVID-19 pandemic, as the prolonged period of stringent social distancing measures and city lockdown, might cause a significant psychological and social impact on both normal population and COVID-19 survivors, [43, 44]while all these measures were not implemented for a prolonged period in the SARS era. With time, COVID-19 survivors are expected to recover slowly and adapt to the new social norm, as reflected by the HRQoL recovery trajectory [7].
Our findings have several clinical implications. A structured physiological and psychological rehabilitation should be set up for COVID-19 survivors, especially those with underlying respiratory comorbidities. As 6MWD is closely correlated with residual radiological changes on HRCT, serial 6MWD measurements is a useful surrogate to gauge functional recovery and supplement the radiological changes when HRCT is not readily available. A recent study evaluated 21 participants with long COVID-19 at 7 ± 4 months (baseline) and 14 ± 4 months (follow-up) post-infection and found improvement of DLCO and St George’s Respiratory Questionnaire but these values did not normalize 14 months post-infection [45]. Recent data suggested SARS could lead to permanent lung damage 15 years after the infection, [46] whether there is a similar effect on COVID-19 survivors deserves further exploration.
Several limitations of the study exist. First, the number of full lung function tests and other assessments of COVID-19 survivors in early study period was limited due to tight resources and concern with infection control [31]. However, the comparable baseline characteristics between attendants and non-attendants allows us to generalize the available results and compare them with those of SARS survivors. Similarly, HRCT was not incorporated into the acute care and interim follow-up of COVID-19 survivors, thus lacking important serial radiological abnormalities to correlate the changes of various physiological parameters. Han et al. have shown that fibrotic changes shown in the CT thorax at 6-month follow-up were associated with a higher initial CT score in COVID-19 survivors, baseline disease severity and age [47]. Second, the radiological findings between the two cohorts could not be compared directly, as HRCT was not routinely performed during the follow-up of SARS survivors. However, we believe that HRCT is a better investigation tool in assessing the location and extent of the parenchymal involvement, and a negative correlation between overall reticulation and total parenchymal involvement with DLCO has been demonstrated in SARS survivors [48]. Third, a significant number of COVID survivors defaulted or refused follow-up, and among these, 55.3% of them had pneumonia. This may introduce selection bias in the statistical analysis. Nevertheless, those 108 patients who remained in the study, albeit modest in the sample size, were recruited from 3 different hospitals with a common treatment protocol provided by the HK Hospital Authority. The prospective nature and detailed characterization allowed us to generalize the results in the appropriate clinical context. Fourth, the missing information on specific SARS-CoV-2 variants and the lack of matching disease severity between two groups of survivors may limit the data interpretation.
To conclude, although COVID-19 survivors required less respiratory support during hospitalization with lower dynamic lung volumes (%predicted FEV1, %predicted FVC), lower %predicted DLCO and exercise capacity (6MWD) during the recovery phase, they had different recovery trajectories in the mental status but a similar speed of recovery in dynamic lung volumes and exercise capacity when compared with SARS survivors. A significant proportion of COVID-19 survivors had residual radiological changes that were associated with additional support during hospitalization and shorter 6MWD. Long-term and multidimensional monitoring during recovery is advised for COVID-19 survivors.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- 6MWD:
-
6-minute walking distance
- 6MWT:
-
6-minute walking test
- BMI:
-
Body mass index
- BP:
-
Bodily pain
- COPD:
-
Chronic obstructive pulmonary disease
- COVID-19:
-
Coronavirus disease 2019
- DLCO:
-
Diffusion capacity for carbon monoxide
- FEV1 :
-
Forced expiratory volume in one second
- FVC:
-
Forced vital capacity
- GGO:
-
Ground-glass opacity
- GH:
-
General health
- HK:
-
Hong Kong
- HRCT:
-
High-resolution computed tomography
- HRQoL:
-
Health-related quality of life
- ICU:
-
Intensive care unit
- MCS:
-
Mental component score
- MH:
-
Mental health
- MV:
-
Mechanical ventilation
- PCS:
-
Physical component score
- PF:
-
Physical functioning
- RE:
-
Role limitation due to emotional problem
- RP:
-
Role limitation due to physical problems
- RV:
-
Residual volume
- SARS:
-
Severe acute respiratory syndrome
- SARS-CoV-1:
-
Severe acute respiratory syndrome coronavirus-1
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus-2
- SD:
-
Standard deviation
- SF:
-
Social functioning
- SF-36:
-
Medical Outcomes Study 36-Item Short-Form General Health Survey
- TLC:
-
Total lung capacity
- VA :
-
Alveolar volume
- VC:
-
Vital capacity
- VT:
-
Vitality
- WHO:
-
World Health Organization
References
WHO Coronavirus (COVID-19) Dashboard. World Health Organization. https://covid19.who.int/?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQjwr4eYBhDrARIsANPywCjfekv7dkHdZ6IwpwelpVAOyNT9n8cjPLGW47OL_PqcoHWcW2je4IsaAv6dEALw_wcB. Date accessed: 25 August 2023.
Centre for Health Protection, Department of Health, The Government of the Hong Kong Special Administrative Region. Latest situation of cases of COVID-19. https://chp-dashboard.geodata.gov.hk/covid-19/en.html. Date accessed: 12 April 2023.
Huang L, Yao Q, Gu X, Wang Q, Ren L, Wang Y, et al. 1-year outcomes in hospital survivors with COVID-19: a longitudinal cohort study. Lancet. 2021;398(10302):747–58.
Trinkmann F, Müller M, Reif A, Kahn N, Kreuter M, Trudzinski F, et al. Residual symptoms and lower lung function in patients recovering from SARS-CoV-2 Infection. Eur Respir J. 2021;57(2):2003002.
Wu X, Liu X, Zhou Y, Yu H, Li R, Zhan Q, et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: a prospective study. Lancet Respir Med. 2021;9(7):747–54.
Huang L, Li X, Gu X, Zhang H, Ren L, Guo L et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: a longitudinal cohort study. Lancet Respir Med. 2022:S2213-2600(22)00126-6.
Lorent N, Vande Weygaerde Y, Claeys E, Guler Caamano Fajardo I, De Vos N, De Wever W, et al. Prospective longitudinal evaluation of hospitalised COVID-19 survivors 3 and 12 months after discharge. ERJ Open Res. 2022;8(2):00004–2022.
Faverio P, Luppi F, Rebora P, D’Andrea G, Stainer A, Busnelli S, et al. One-year pulmonary impairment after severe COVID-19: a prospective, multicenter follow-up study. Respir Res. 2022;23(1):65.
Marando M, Fusi-Schmidhauser T, Tamburello A, Grazioli Gauthier L, Rigamonti E, Argentieri G, et al. 1-year radiological, functional and quality-of-life outcomes in patients with SARS-CoV-2 Pneumonia – A prospective observational study. NPJ Prim Care Respir Med. 2022;32(1):8.
Steinbeis F, Thibeault C, Doellinger F, Ring RM, Mittermaier M, Ruwwe-Glösenkamp C, et al. Severity of Respiratory Failure and computed chest tomography in acute COVID-19 correlates with pulmonary function and respiratory symptoms after Infection with SARS-CoV-2: an observational longitudinal study over 12 months. Respir Med. 2022;191:106709.
Shah AS, Ryu MH, Hague CJ, Murphy DT, Johnston JC, Ryerson CJ, et al. Changes in pulmonary function and patient-reported outcomes during COVID-19 recovery: a longitudinal, prospective cohort study. ERJ Open Res. 2021;7(3):00243–2021.
Hui DSC, Zumla A. Severe Acute Respiratory Syndrome: historical, epidemiologic, and clinical features. Infect Dis Clin North Am. 2019;33(4):869–89.
Hui DS, Wong KT, Ko FW, Tam LS, Chan DP, Woo J, et al. The 1-year impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and quality of life in a cohort of survivors. Chest. 2005;128(4):2247–61.
Lui GC, Yip TC, Wong VW, Chow VC, Ho TH, Li TC, et al. Significantly lower case-fatality ratio of Coronavirus Disease 2019 (COVID-19) than severe Acute Respiratory Syndrome (SARS) in Hong Kong-A territory-wide Cohort Study. Clin Infect Dis. 2021;72(10):e466–75.
Ngai JC, Ko FW, Ng SS, To KW, Tong M, Hui DS. The long-term impact of severe acute respiratory syndrome on pulmonary function, exercise capacity and health status. Respirology. 2010;15(3):543–50.
Li TS, Gomersall CD, Joynt GM, Chan DP, Leung P, Hui DS. Long-term outcome of acute respiratory distress syndrome caused by severe acute respiratory syndrome (SARS): an observational study. Crit Care Resusc. 2006;8(4):302–8.
Hui DS, Joynt GM, Wong KT, Gomersall CD, Li TS, Antonio G, et al. Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax. 2005;60(5):401–9.
American Thoracic Society. Standardization of spirometry, 1994 update. Am J Respir Crit Care Med. 1995;152(3):1107–36.
Lung function testing. Selection of reference values and interpretative strategies. American thoracic society. Am Rev Respir Dis. 1991;144(5):1202–18.
McHorney CA, Ware JE Jr, Lu JF, Sherbourne CD. The MOS 36-item short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care. 1994;32(1):40–66.
Ip MS, Ko FW, Lau AC, Yu WC, Tang KS, Choo K, et al. Hong Kong Thoracic Society and American College of Chest Physicians (Hong Kong and Macau chapter). Updated spirometric reference values for adult Chinese in Hong Kong and implications on clinical utilization. Chest. 2006;129(2):384–92.
Enright PL, Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1384–7.
Lam CL, Tse EY, Gandek B, Fong DY. The SF-36 summary scales were valid, reliable, and equivalent in a Chinese population. J Clin Epidemiol. 2005;58(8):815–22.
Wong CKH, Mulhern B, Cheng GHL, Lam CLK. Population based norming of the Chinese (HK) version of the SF 36 health survey. Hong Kong Practitioner. 1999;21:460–70.
Antonio GE, Wong KT, Hui DS, et al. Thin-section CT in patients with severe acute respiratory syndrome following hospital discharge: preliminary experience. Radiology. 2003;228(3):810–5.
Chang YC, Yu CJ, Chang SC, et al. Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: evaluation with thin-section CT. Radiology. 2005;236(3):1067–75.
Chung M, Bernheim A, Mei X, et al. CT imaging features of 2019 Novel Coronavirus (2019-nCoV). Radiology. 2020;295(1):202–7.
Pan F, Ye T, Sun P, et al. Time Course of Lung Changes at chest CT during recovery from Coronavirus Disease 2019 (COVID-19). Radiology. 202;295(3):715–21.
Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697–722.
World Health Organization. Clinical management of COVID-19 patients: living guidance 25 January 2021: v0.16. https://apps.who.int/iris/handle/10665/338882. Date accessed: 12 April 2023.
Guler SA, Ebner L, Aubry-Beigelman C, Bridevaux PO, Brutsche M, Clarenbach C, et al. Pulmonary function and radiological features 4 months after COVID-19: first results from the national prospective observational Swiss COVID-19 lung study. Eur Respir J. 2021;57(4):2003690.
González J, Benítez ID, Carmona P, Santisteve S, Monge A, Moncusí-Moix A, et al. CIBERESUCICOVID Project (COV20/00110, ISCIII). Pulmonary function and radiologic features in survivors of critical COVID-19: a 3-Month prospective cohort. Chest. 2021;160(1):187–98.
Xiong Y, Sun D, Liu Y, Fan Y, Zhao L, Li X, et al. Clinical and high-resolution CT features of the COVID-19 Infection: comparison of the initial and follow-up changes. Invest Radiol. 2020;55(6):332–9.
Han X, Cao Y, Jiang N, Chen Y, Alwalid O, Zhang X, et al. Novel coronavirus Disease 2019 (COVID-19) Pneumonia progression course in 17 discharged patients: comparison of clinical and thin-section computed Tomography features during recovery. Clin Infect Dis. 2020;71(15):723–31.
Luger AK, Sonnweber T, Gruber L, Schwabl C, Cima K, Tymoszuk P, et al. Chest CT of Lung Injury 1 year after COVID-19 Pneumonia: the CovILD Study. Radiology. 2022;304(2):462–70.
Orzes N, Pini L, Levi G, Uccelli S, Cettolo F, Tantucci C. A prospective evaluation of lung function at three and six months in patients with previous SARS-COV-2 Pneumonia. Respir Med. 2021;186:106541.
Lerum TV, Meltzer C, Rodriguez JR, Aaløkken TM, Brønstad E, Aarli BB et al. A prospective study of pulmonary outcomes and chest CT the first year after COVID-19. ERJ Open Res. 2022:00575–2022.
Rinaldo RF, Mondoni M, Parazzini EM, Pitari F, Brambilla E, Luraschi S, et al. Deconditioning as main mechanism of impaired exercise response in COVID-19 survivors. Eur Respir J. 2021;58(2):2100870.
Jahn K, Sava M, Sommer G, Schumann DM, Bassetti S, Siegemund M, et al. Exercise capacity impairment after COVID-19 Pneumonia is mainly caused by deconditioning. Eur Respir J. 2021;59(1):2101136.
Ong KC, Ng AW, Lee LS, Kaw G, Kwek SK, Leow MK. e tal. Pulmonary function and exercise capacity in survivors of severe acute respiratory syndrome. Eur Respir J. 2004;24(3):436 – 42.
Wageck B, Cox NS, Holland AE. Recovery following Acute exacerbations of Chronic Obstructive Pulmonary Disease - A Review. COPD. 2019;16(1):93–103.
Philip KEJ, Buttery S, Williams P, Vijayakumar B, Tonkin J, Cumella A, et al. Impact of COVID-19 on people with Asthma: a mixed methods analysis from a UK wide survey. BMJ Open Respir Res. 2022;9(1):e001056.
Chinna K, Sundarasen S, Khoshaim HB, Kamaludin K, Nurunnabi M, Baloch GM, et al. Psychological impact of COVID-19 and lock down measures: an online cross-sectional multicounty study on Asian university students. PLoS ONE. 2021;16(8):e0253059.
Dratva J, Zysset A, Schlatter N, von Wyl A, Huber M, Volken T. Swiss University Students’ risk perception and general anxiety during the COVID-19 pandemic. Int J Environ Res Public Health. 2020;17(20):7433.
Matheson AM, McIntosh MJ, Kooner HK, Abdelrazek M, Albert MS, Dhaliwal I, et al. Longitudinal follow-up of postacute COVID-19 syndrome: DLCO, quality-of-life and MRI pulmonary gas-exchange abnormalities. Thorax. 2023;78(4):418–21.
Li J, Zheng Y, Zhao L, Yue Z, Pan F, Chen Y, et al. Investigation of the impact of SARS-CoV Infection on the immunologic status and lung function after 15 years. BMC Infect Dis. 2021;21(1):1183.
Han X, Fan Y, Alwalid O, Li N, Jia X, Yuan M, et al. Six-month follow-up chest CT findings after severe COVID-19 Pneumonia. Radiology. 2021;299(1):E177–86.
Wong KT, Antonio GE, Hui DS, Ho C, Chan PN, Ng WH, et al. Severe acute respiratory syndrome: thin-section computed tomography features, temporal changes, and clinicoradiologic correlation during the convalescent period. J Comput Assist Tomogr. 2004;28(6):790–5.
Acknowledgements
We thank Ken KC Ling for the arrangement of lung function tests and for entering the data of the project.
Funding
This study is supported by the Health and Medical Research Fund Commissioned Research on the Novel Coronavirus Disease (COVID-19), Hong Kong SAR (COVID 1903003), RGC theme-based research schemes (T11-712/19-N and T11-705/21-N), RMG (8601330 and 8601372), Kai Chong Tong, and the SH Ho Foundation. The funding source had no role in the design of this study, execution, analyses, interpretation of the data, or decision to submit results.
Author information
Authors and Affiliations
Contributions
KKPC and SSSN had equal contributions to the manuscript. KKPC, SSSN, GCYL and DSCH contributed substantially to the conception, design of the study, and final approval of the version to be published. KTW, HSL and WCWC performed the radiological examination. TOC and KYSY acquired data and subsequent data analysis. EYKT, KWT, JCLN, TWHY, RLPL, JKCN and FWSK contributed to the study design and interpretation of data. KKPC and DSCH are the guarantors of the paper, taking responsibility for the integrity of the work as a whole, from inception to published article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by Clinical Research Ethics Committees of the Chinese University of Hong Kong (CREC-2020.229). Informed consent was obtained from all the participants. The study was performed in accordance with Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chan, K.K.P., Ng, S.S.S., Lui, G.C.Y. et al. Comparison of the 12-month impact of COVID-19 and SARS on physiological capacity and health-related quality of life. BMC Pulm Med 23, 441 (2023). https://doi.org/10.1186/s12890-023-02750-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-023-02750-8