
Abstract
Background
The main aim of this systematic review was to determine the effectiveness of postoperative rehabilitation interventions that include breathing exercises as a component to prevent atelectasis in lung cancer resection patients.
Methods
In this review, we systematically and comprehensively searched the Cochrane Library, PubMed, EMBASE, and Web of Science in English and CNKI and Wanfang in Chinese from 2012 to 2022. The review included any randomized controlled trials focusing on the effectiveness of postoperative rehabilitation interventions that include breathing exercises to prevent pulmonary atelectasis in lung cancer patients. Participants who underwent anatomic pulmonary resection and received postoperative rehabilitation interventions that included breathing exercises as a component were included in this review. The study quality and risks of bias were measured with the GRADE and Cochrane Collaboration tools, and statistical analysis was performed utilizing RevMan 5.3 software.
Results
The incidence of atelectasis was significantly lower in the postoperative rehabilitation intervention group (OR = 0.35; 95% CI, 0.18 to 0.67; I2 = 0%; P = 0.67) than in the control group. The patients who underwent the postoperative rehabilitation program that included breathing exercises (intervention group) had higher forced vital capacity (FVC) scores (MD = 0.24; 95% CI, 0.07 to 0.41; I2 = 73%; P = 0.02), forced expiratory volume in one second (FEV1) scores (MD = 0.31; 95% CI, 0.03 to 0.60; I2 = 98%; P < 0.01) and FEV1/FVC ratios (MD = 9.09; 95% CI, 1.50 to 16.67; I2 = 94%; P < 0.01).
Conclusion
Postoperative rehabilitation interventions that included breathing exercises decreased the incidence rate of atelectasis and improved lung function by increasing the FVC, FEV1, and FEV1/FVC ratio.
Similar content being viewed by others


Introduction
According to the World Health Organization, cancer is a leading cause of death worldwide, claiming nearly 10 million lives in 2020 [1]. In both sexes, the most common cancer was lung cancer, accounting for 11.6% of total cancer cases, and it was fatal with a mortality rate of 18.4% of total cancer deaths in 2018 [2]. Surgery is an important treatment option in which doctors excise the cancer tissue from patients [3]. However, postoperative pulmonary complications (PPCs) remain difficult clinical issues hindering recovery. The incidence of PPCs is approximately 32–39% depending on individual biases, such as in health conditions and surgical methods [4, 5]. Pneumonia and atelectasis are the most common PPCs after lung resection surgery [6]. Even mild PPCs can lead to serious clinical problems including increased early postoperative mortality and a prolonged length of stay in the intensive care unit or hospital [7]. Therefore, it is of great clinical value to determine specific rehabilitation interventions to decrease the incidence of PPCs and improve lung function in lung cancer patients after anatomic pulmonary resection.
Some preoperative pulmonary rehabilitation programs have been proven to play an important role in functional recovery. For example, exercise-based programs that included breathing exercises could improve exercise tolerance, and muscle strength, and enhance postoperative recovery [8]. Other postoperative training such as inspiratory muscle training and exercise training was associated with less sedentary activity and prevented a decline in physical activity [9]. Breathing exercises were also demonstrated to improve lung function and quality of life [10]. However, the evidence was controversial in some finer details. Although clinicians used breathing exercises as part of the treatment regimen for lung cancer patients after surgery, some studies found that preoperative interventions could not reduce the incidence of PPCs, such as pneumonia and atelectasis [11, 12].
Previous meta-analyses have quantified and drawn conclusions about the effects of preoperative breathing exercises on PPCs [13,14,15,16], while others were focused on perioperative pulmonary rehabilitation interventions [11, 12, 17, 18]. However, there has been no meta-analysis specifically focusing on postoperative interventions in addition to a regular rehabilitation program in reducing the incidence of atelectasis in lung cancer resection patients. Therefore, the purpose of this systematic review was to analyze the postoperative rehabilitation programs that include breathing exercises and determine whether they were effective in reducing the incidence of atelectasis and improving lung function.
Methods
This systematic review was reported based on guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocol Statement (PRISMAP) [19] and the procedures used in this systematic review were based on the Cochrane Handbook for Systematic Reviews of Interventions [20]. The scope of the systematic review was specified using the PICOS (participants, interventions, comparisons, outcomes, study type) framework. The PICOS question was: in patients with pulmonary cancer who underwent surgical resection, do postoperative rehabilitation programs that include breathing exercises decrease the incidence rate of pulmonary atelectasis, compared to the regular rehabilitation program?
In this review, we defined the control group as patients who underwent regular rehabilitation programs, including medication management, physiotherapy, and health education. The intervention group was defined as patients who underwent postoperative rehabilitation programs that included any breathing exercises as a component, such as inspiratory muscle training, abdominal breathing training, and the utility of assistive training devices related to breathing.
All included studies were randomized controlled trials. We developed a review protocol using the planned analysis approach. This systematic review was registered in PROSPERO, and the registration number was CRD42022343946.
Inclusion criteria
Studies were eligible if participants with lung cancer underwent any type of surgical resection (all types of surgery were included); a comparison between postoperative rehabilitation programs including breathing exercises at any intensity and regular rehabilitation program was conducted; the incidence of pulmonary atelectasis as outcome measurement was provided; and the methods study type was a randomized controlled trial. Additionally, the included studies must have been published in peer-reviewed journals with full texts available either in English or Chinese.
Exclusion criteria
Studies were excluded if they were case reports, case series, or observational studies; if the reason for surgery was not lung cancer; if the participants from the intervention group did not receive any postoperative breathing training; if the language of the studies was neither English nor Chinese; or if they did not include the primary outcomes set by the protocol.
Outcomes
The primary outcome was the incidence rate of atelectasis after surgery. The secondary outcomes were FEV1, FVC, and the FEV1/FVC ratio, which are important indicators for factors to the prognosis of atrophic pulmonary resection [5, 21, 22].
Search strategy
One of the authors (JW) systematically and comprehensively searched the Cochrane Library, PubMed, EMBASE, and Web of Science in English, and CNKI and Wanfang in Chinese for studies published during the last decade (from 2012 to 2022) using medical and random terms. The authors also searched ClinicalTrials.gov and the World Health Organization International Clinical Trials Registry Platform to identify ongoing or unpublished eligible trials.
Study selection
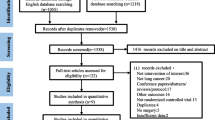
The search for articles was performed separately by two authors (JW, ND), and the results were imported into EndNote. After the removal of duplicates among the retrieved articles, the title and abstract of the articles were independently reviewed by two authors (JW, HH) to complete the rough screening process. If the results were inconsistent, the third author (FQ) resolved the issue through consensus. Finally, after reading the full text of the retrieved RCT articles, another researcher was consulted to make inclusion decisions if needed. All the processes are shown in a flow chart (Fig. 1).

Flow of the search strategy
Data collection process
All the data extraction processes were performed by two authors separately (JW, ND); the third researcher (FQ) was consulted if there were disagreements. If a study mentioned an outcome of interest without providing details, we contacted the author for the data. Disagreements were resolved by consensus.
Risk of bias assessment in individual studies
The quality of individual studies was assessed by two authors separately (ND, QL), using the Cochrane Collaboration risk of bias tool, and the quality of evidence for outcomes was examined using the Grading of Recommendations Assessment, Development, And Evaluation (GRADE) approach [23].
Data synthesis
Statistical analysis was performed by utilizing RevMan 5.3.3 software. This systematic review used odds ratios and their associated 95% confidence intervals to assess the primary outcome of, postoperative complications. The mean difference value was used to assess the secondary outcomes. If I2 > 50 and the p-value was less than 0.05, we considered the result to be heterogeneous and applied a random-effects model [24]. Accordingly, a subgroup was applied to analyze the heterogeneity. If I2 < 50 and the p-value was greater than 0.05, no significant heterogeneity was detected, and we applied a fixed-effects model.
Subgroup analysis
To determine intervention effects for different types of atelectasis, we intended to perform a subgroup analysis. However, the retrieved studies did not provide us with enough information about the types of atelectasis observed. Thus, the subgroup analysis was discontinued.
Sensitivity analysis
In this systematic review, we intended to conduct sensitivity analyses by excluding articles with a high risk of bias, which often has some different characteristics. In this way, we could use the random-effects model rather than the fixed-effects model. Alternatively, each study was excluded one by one, and the remaining studies were pooled to determine whether the results varied significantly.
Results
Flow of trials through the review process
The search strategy identified 1,830 records, of which 516 were found to be duplicates. After screening titles, abstracts, and reference lists, 33 potentially relevant full articles were screened. After evaluating full-text articles, 26 studies failing to meet the inclusion criteria were excluded, and 7 studies were included in this systematic review. Figure 1 outlines the flow of studies through the review process.
Characteristics of the included trials
The 7 included trials involved 569 participants and investigated the effect of postoperative rehabilitation programs on the incidence of atelectasis after lung resection. FEV1 was included in 5 studies [25,26,27,28,29], FVC in 3 studies [26, 27, 29] and FEV1/FVC in 2 studies [28, 29]. Six studies [25,26,27, 29,30,31] performed postoperative rehabilitation programs with at least one breathing exercise device. Two studies performed inspiratory muscle training [25, 30]. The initial resistance load was set at 30% and the load was gradually increased until the patient was discharged. The load of the training method was adjusted according to the patient’s tolerance. Additional relevant characteristics of the included studies are shown in Table 1. GRADE evidence quality ratings are shown in Table 2.
Risk of bias assessment
The outcomes of the quality assessment of the studies were conducted in Review Manager 5.3 software according to the quality assessment judgment criteria. The risk of bias was assessed as low, high, or unclear risk. None of the studies described detailed information about blinding participants; all the articles were single-center studies, and it was hard to blind the participants, so all studies had a high risk of performance bias. Six trials [25,26,27,28, 30, 31] had complete outcomes data, except for Zou et al.’s study [29]. Six trials [25, 27,28,29,30,31] were RCTs with a clear method of randomization, except Shen et al.’s study [26]. Brocki et al.’s study [30] was the only study that clearly explained assessors blinding, thus we only considered it as low risk of detection bias. Additional detailed information about the risk of bias assessments is shown in Figs. 2, 3.

Risk of bias summary respectively

Risk of bias summary generally
Primary outcome
Incidence of atelectasis
The effect of postoperative rehabilitation programs on atelectasis was examined by pooling the data from all 7 trials [25,26,27,28,29,30,31]. The result shows that there is no heterogeneity, so a fixed-effects model was applied. The incidence of atelectasis was significantly lower after postoperative rehabilitation programs (OR = 0.35; 95% CI, 0.18 to 0.67; I2 = 0%; P = 0.67) compared with the control group (Fig. 4).

The forest plot showing OR (95% CI) of atelectasis incidence after implementation of postoperative rehabilitation interventions that include breathing exercise
Secondary outcomes
FVC
The effect of breathing exercises on FVC was examined by pooling data from 5 trials [26,27,28,29,30]. However, complete data extraction failed in the studies of Zou et al. [29] and Brocki et al [30]. Therefore, a total of 3 trials [26,27,28] were included in the meta-analysis. When a random-effects model was applied, postoperative rehabilitation programs can improve the score of FVC (MD = 0.24; 95% CI, 0.07 to 0.41; I2 = 73%; P = 0.02) (Fig. 5).

FVC forest plot showing the mean difference (95% CI) of the effect of postoperative rehabilitation interventions that include breathing exercise on FVC
FEV1
6 trials collected the data on FEV1, but we failed to extract the data on FEV1 from Brocki et al. [30] and pooled the data from the other 5 trials [26,27,28,29, 31]. There was a difference between the experimental group and intervention group (MD = 0.31; 95% CI, 0.03 to 0.60; I2 = 98%; P < 0.01) (Fig. 6).

FEV1 forest plot showing the mean difference (95% CI) of the effect of postoperative rehabilitation interventions that include breathing exercise on FEV1
FEV1/FVC ratio
Four articles [27,28,29,30] reported the value of the FEV1/FVC ratio. We excluded two articles from Brocki et al. [30] and Yang et al., [27] because of a lack of original data. Thus, the effect of postoperative rehabilitation programs on the FEV1/FVC ratio was examined by pooling data from 2 trials [28, 29]. The result shows that postoperative rehabilitation programs can increase the grade of FEV1/FVC Ratio (MD = 9.09; 95% CI, 1.50 to 16.67; I2 = 94%; P < 0.01) (Fig. 7).

FEV1/FVC forest plot showing the mean difference (95%) of the effect of postoperative rehabilitation interventions that include breathing exercise on the FEV1/FVC ratio
Discussion
This systematic review included 7 studies in total that reported the incidence of atelectasis after postoperative intervention as one of the outcome measurements. By analyzing these RCT articles, we found that lung cancer patients undergoing surgical resection would benefit from postoperative rehabilitation programs that include breathing exercises to decrease their incidence of atelectasis, a common PPC. In addition, the heterogeneity was negligible for this indicator. We also performed a sensitivity analysis using the leave-one-out method and excluding one study at a time to change the fixed model to a random-effects model. The results remained robust (Sup. 1).
A previous meta-analysis also assessed the effects of breathing exercises on PPCs in lung cancer patients. Wang et al. collected data through 20 December 2017 and grouped the breathing exercises based on different stages including preoperative, postoperative, and perioperative in their retrieved studies. [12] However, their data analysis was debatable, with a view to the inclusion criteria of postoperative rehabilitation interventions and the computation methods of incidence of atelectasis. In our meta-analysis, we reviewed the research during the last decade through 2022 and focused on postoperative rehabilitation interventions that included breathing exercises as a component. Additionally, we used the incidence of atelectasis as the primary outcome. Therefore, our review was more focused on postoperative interventions and their preventive effects on atelectasis. Another reason for selecting postoperative rehabilitation was the unique medical-social phenomenon in China. In Lai et al.’s study, 22 eligible patients refused to participate in preoperative rehabilitation treatment. [32] The primary causes for lung patients’ reluctance were the lack of public health consciousness and financial problems caused by a prolonged length of stay in the hospital, which is a common social issue in China and other developing countries [33]. Lung cancer patients hope to undergo the operation as soon as possible when they are admitted to the hospital rather than receive preoperative rehabilitation. Therefore, we considered it more practical to study postoperative rehabilitation in developing countries. In the future, as health care and awareness improve, our research will focus more on not only postoperative but also perioperative breathing exercises, which are also of great clinical significance [8, 31].
According to our results, we had positive findings for FEV1, the FEV1/FVC ratio, and FVC, which indicated that a postoperative rehabilitation program including breathing exercises would help lung cancer patients improve their lung function. However, the heterogeneity among those values was significant. To analyze the heterogeneity source of FEV1, we conducted a subgroup analysis for possible influencing factors, including intervention types, intervention timing, and others. We found that the use of Acapella could be an influencing factor (Sup. 2). The intervention group participants in the studies of Li et al. and Zhou et al. were provided with Acapella, a widely used breathing training device in pulmonary rehabilitation. [28, 31] Only two from Zhou et al. and Zou et al. included reported the FEV1/FVC ratio. [28, 29] Thus, we were unable to conduct a subgroup analysis. We reviewed the details of the articles and discovered that the risk of bias could be the primary cause of the heterogeneity. We evaluated the risks of attribution bias and reporting bias in the study by Zou et al., which were both high. [29] This study mentioned FVC in the abstract as an outcome measure, but no data were found in the results section, which was considered incomplete outcome data. On the other hand, the risks of bias in the above two aspects in the study by Zhou et al. [28] were low. The substantial difference in the risks of bias could also be the reason why Zou et al. [29] found much greater positive effects between the study groups than the study by Zhou et al. [28] In terms of FVC, the heterogeneity could derive from the interventions provided to the control group. The control group participants in the study by Yang et al. [27] did not receive any physiotherapy, while the studies by Shen et al. [26] and Zhou et al. [28] provided a common physiotherapy intervention to the participants in the control group.
Finally, for this meta-analysis, explicit eligibility criteria were established, and a meticulous search of the different databases was performed. We assessed the risk of bias to determine the reliability of the evidence. Additionally, the included studies were limited to the highest standard of evidence, only RCTs. However, the secondary outcome findings should be generalized carefully due to the limited number of cases, the deficiency in the blinding of therapists and patients, and the diversity in the content of breathing exercise programs in the retrieved studies. To conclude, this meta-analysis revealed that postoperative rehabilitation interventions that include breathing exercises could decrease the incidence of atelectasis in patients with lung cancer after surgery. Additionally, it provided a clinical basis for future considerations on whether postoperative rehabilitation interventions that include breathing exercises should be implemented after surgery.
Study limitations
The main limitation of this review was the obvious heterogeneity in the secondary outcomes of FVC, FEV1 and the FVE1/FVC ratio. However, there were only a few studies that reported FVC and the FEV1/FVC ratio, and it was difficult to conduct subgroup analysis. Thus, we compared the detailed information, including research design, intervention methods, and data collection. Second, no studies performed well in preventing performance bias, and only the study by Brocki et al. performed well in blinding for outcome assessments. [30] This led to a low level of evidence. Third, the rehabilitation intervention in the study by Brocki et al. was started one day before surgery; however, since the majority part of the intervention was performed after the surgery, [30] we still considered it to be a postoperative intervention.
Additionally, it was difficult to determine the effect of breathing exercises alone without involving any other general rehabilitation interventions given the objective facts in the clinical settings and ethical considerations. We cannot deduce whether these breathing exercises will work independently from any other rehabilitation interventions.
Availability of data and materials
Detailed information on search strategies and other relevant material that support the findings of this systematic review is available from the corresponding author upon reasonable request.
Abbreviations
- CI:
-
Confidence interval
- RCTs:
-
Randomized controlled trials
- PPCs:
-
Postoperative pulmonary complications
- 6MWT:
-
The 6-min walk test
- FVC:
-
Forced vital capacity
- FEV1:
-
Forced expiratory volume in 1-s
References
“Cancer.” World Health Organization, World Health Organization, 3 Feb. 2022. (https://www.who.int/news-room/fact-sheets/detail/cancer).
Bray F, Jacques F, Isabelle S, Rebecca LS, Lindsey AT, Ahmedin J. Global Cancer Statistics 2018: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2018;68(6):394–424. https://doi.org/10.3322/caac.21492.
“How Is Lung Cancer Diagnosed and Treated?” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 25 Oct. 2022, https://www.cdc.gov/cancer/lung/basic_info/diagnosis_treatment.htm.
Bailey KL, Merchant N, Seo YJ, Elashoff D, Benharash P, Yanagawa J. Short-Term Readmissions After Open, Thoracoscopic, and Robotic Lobectomy for Lung Cancer Based on the Nationwide Readmissions Database. World J Surg. 2019;43(5):1377–84. https://doi.org/10.1007/s00268-018-04900-0.
Linden PA, Bueno R, Colson YL, Jaklitsch MT, Lukanich J, Mentzer S, Sugarbaker DJ. Lung resection in patients with preoperative FEV1 < 35% predicted. Chest. 2005;127(6):1984–90. https://doi.org/10.1378/chest.127.6.1984.
Lugg ST, Agostini PJ, Tikka T, Kerr A, Adams K, Bishay E, Kalkat MS, Steyn RS, Rajesh PB, Thickett DR, Naidu B. Long-term impact of developing a postoperative pulmonary complication after lung surgery. Thorax. 2016;71(2):171–6. https://doi.org/10.1136/thoraxjnl-2015-207697.
Fernandez-Bustamante A, Frendl G, Sprung J, Kor DJ, Subramaniam B, Martinez Ruiz R, Lee JW, Henderson WG, Moss A, Mehdiratta N, Colwell MM, Bartels K, Kolodzie K, Giquel J, Vidal Melo MF. Postoperative Pulmonary Complications, Early Mortality, and Hospital Stay Following Noncardiothoracic Surgery: A Multicenter Study by the Perioperative Research Network Investigators. JAMA Surg. 2017;152(2):157–66. https://doi.org/10.1001/jamasurg.2016.4065.
Sebio García R, Yáñez-Brage MI, Giménez Moolhuyzen E, Salorio Riobo M, Lista Paz A, Borro Mate JM. Preoperative exercise training prevents functional decline after lung resection surgery: a randomized, single-blind controlled trial. Clin Rehabil. 2017;31(8):1057–67. https://doi.org/10.1177/0269215516684179.
Brocki BC, Andreasen JJ, Westerdahl E. Inspiratory Muscle Training in High-Risk Patients Following Lung Resection May Prevent a Postoperative Decline in Physical Activity Level. Integr Cancer Ther. 2018;17(4):1095–102. https://doi.org/10.1177/1534735418796286.
Liu W, Pan YL, Gao CX, Shang Z, Ning LJ, Liu X. Breathing exercises improve post-operative pulmonary function and quality of life in patients with lung cancer: A meta-analysis. Exp Ther Med. 2013;5(4):1194–200. https://doi.org/10.3892/etm.2013.926.
Crandall K, Maguire R, Campbell A, Kearney N. Exercise intervention for patients surgically treated for Non-Small Cell Lung Cancer (NSCLC): a systematic review. Surg Oncol. 2014;23(1):17–30. https://doi.org/10.1016/j.suronc.2014.01.001.
Wang YQ, Liu X, Jia Y, Xie J. Impact of breathing exercises in subjects with lung cancer undergoing surgical resection: A systematic review and meta-analysis. J Clin Nurs. 2019;28(5–6):717–32. https://doi.org/10.1111/jocn.14696.
Bibo L, Goldblatt J, Merry C. Does preoperative pulmonary rehabilitation/physiotherapy improve patient outcomes following lung resection? Interact Cardiovasc Thorac Surg. 2021;32(6):933–7. https://doi.org/10.1093/icvts/ivab011.
Pu CY, Batarseh H, Zafron ML, Mador MJ, Yendamuri S, Ray AD. Effects of Preoperative Breathing Exercise on Postoperative Outcomes for Patients With Lung Cancer Undergoing Curative Intent Lung Resection: A Meta-analysis. Arch Phys Med Rehabil. 2021;102(12):2416–2427.e4. https://doi.org/10.1016/j.apmr.2021.03.028.
de Oliveira VC, Martha BA, Macagnan FE. Effect of inspiratory muscle training associated or not to physical rehabilitation in preoperative anatomic pulmonary resection: a systematic review and meta-analysis. Support Care Cancer. 2022;30(2):1079–92. https://doi.org/10.1007/s00520-021-06467-4.
Rosero ID, Ramírez-Vélez R, Lucia A, Martínez-Velilla N, Santos-Lozano A, Valenzuela PL, Morilla I, Izquierdo M. Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer. Cancers (Basel). 2019;11(7):944. https://doi.org/10.3390/cancers11070944.
Mao X, Ni Y, Niu Y, Jiang L. The Clinical Value of Pulmonary Rehabilitation in Reducing Postoperative Complications and Mortality of Lung Cancer Resection: A Systematic Review and Meta-Analysis. Front Surg. 2021;8:685485. https://doi.org/10.3389/fsurg.2021.685485.
Deng J, Li R. The effect of rehabilitation training on postoperative lung cancer patients: A systematic review and meta-analysis. Asian J Surg. 2022;S1015–9584(22):00428–36. https://doi.org/10.1016/j.asjsur.2022.04.036.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647. https://doi.org/10.1136/bmj.g7647.
Higgins J, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 5.2 (updated June 2017). 2017. www.training.cochrane.org/handbook
Brunelli A, Charloux A, Bolliger CT, Rocco G, Sculier JP, Varela G, Licker M, Ferguson MK, Faivre-Finn C, Huber RM, Clini EM, Win T, De Ruysscher D, Goldman L. European Respiratory Society and European Society of Thoracic Surgeons joint task force on fitness for radical therapy. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J. 2009;34(1):17–41. https://doi.org/10.1183/09031936.00184308.
Wasswa-Kintu S, Gan WQ, Man SF, Pare PD, Sin DD. Relationship between reduced forced expiratory volume in one second and the risk of lung cancer: a systematic review and meta-analysis. Thorax. 2005;60(7):570–5. https://doi.org/10.1136/thx.2004.037135.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schünemann HJ, GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6. https://doi.org/10.1136/bmj.39489.470347.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58. https://doi.org/10.1002/sim.1186.
Liu J, Kuo N, Fang T, Chen J, Lu H, Lin H. A six-week inspiratory muscle training and aerobic exercise improves respiratory muscle strength and exercise capacity in lung cancer patients after video-assisted thoracoscopic surgery: A randomized controlled trial. Clin Rehabil. 2021;35(6):840–50. https://doi.org/10.1177/0269215520980138.
Shen L, Guo H, Ye M. Application of breathing exerciser after thoracoscopic radical resection of non-small cell lung cancer CHINA MODERN DOCTOR Vol. 59 No. 17 June 2021. https://www.cnki.com.cn/Article/CJFDTotal-ZDYS202117020.htm.
Yang J, Zhao Y, Wang D, Wang Ning. Effect of early respiratory function training on patients’ pulmonary function and quality of life after radical lung cancer surgery. Oncology Progress. Jul 2021 Vol. 19, No. 14 https://doi.org/10.11877/j.issn.1672-1535.2021.19.14.25. https://www.cnki.com.cn/Article/CJFDTotal-AZJZ202114025.htm
Zhou T, Sun C. Effect of physical manipulation pulmonary rehabilitation on lung cancer patients after thoracoscopic lobectomy. Thorac Cancer. 2022;13(3):308–15. https://doi.org/10.1111/1759-7714.14225.
Zou H, Qin Y, Gong F, Liu J, Zhang J, Zhang L. ABCDEF pulmonary rehabilitation program can improve the mid-term lung function of lung cancer patients after thoracoscopic surgery: A randomized controlled study. Geriatr Nurs. 2022;44:76–83. https://doi.org/10.1016/j.gerinurse.2021.12.021.
Brocki BC, Andreasen JJ, Langer D, Souza DS, Westerdahl E. Postoperative inspiratory muscle training in addition to breathing exercises and early mobilization improves oxygenation in high-risk patients after lung cancer surgery: a randomized controlled trial. Eur J Cardiothorac Surg. 2016;49(5):1483–91. https://doi.org/10.1093/ejcts/ezv359.
Li P, Lai Y, Zhou K, Su J, Che G. Can Perioperative Oscillating Positive Expiratory Pressure Practice Enhance Recovery in Lung Cancer Patients Undergoing Thorascopic Lobectomy? Zhongguo Fei Ai Za Zhi. 2018;21(12):890–5. https://doi.org/10.3779/j.issn.1009-3419.2018.12.06 (https://www.cnki.com.cn/Article/CJFDTOTAL-FAIZ201812003.htm).
Lai Y, Huang J, Yang M, Su J, Liu J, Che G. Seven-day intensive preoperative rehabilitation for elderly patients with lung cancer: a randomized controlled trial. J Surg Res. 2017;209:30–6. https://doi.org/10.1016/j.jss.2016.09.033.
Huang J, Lai Y, Zhou X, Li S, Su J, Yang M, Che G. Short-term high-intensity rehabilitation in radically treated luner: a three-armed randomized controlled trial. J Thorac Dis. 2017;9(7):1919–29. https://doi.org/10.21037/jtd.2017.06.15.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
JW helped in the Conceptualization and the Methodology. HH and FQ helped in the data curation. HH and FQ helped in the Formal analysis. ND and QL helped in the Investigation. ND helped in the Project administration. JW and DN helped with the Resources. JW and QL assisted in the operation of the Software. JW assisted in the supervision and validation. HH and XJ assisted in the visualization. JW and DN assisted in the Writing of the original draft. JW and HH assisted with the Writing of the review & editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No ethical approval was required.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Sup. 1. The forest plot showing OR (95% CI) of atelectasis incidence after implementation postoperative rehabilitation programs (random model).
Additional file 2:
Sup. 2. FEV1 forest plot showing the total mean difference (95% CI) of the effect of postoperative rehabilitation interventions that include breathing exercise on FEV1 subgroup score (subgroup: with or without the device of Acapella).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, J., Deng, N., Qi, F. et al. The effectiveness of postoperative rehabilitation interventions that include breathing exercises to prevent pulmonary atelectasis in lung cancer resection patients: a systematic review and meta-analysis. BMC Pulm Med 23, 276 (2023). https://doi.org/10.1186/s12890-023-02563-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-023-02563-9