
Abstract
Introduction
In Pakistan, chronic respiratory conditions contribute a large burden of morbidity and mortality. A major reason for this is the lack of availability of local evidence-based clinical practice guidelines (EBCPGs) in Pakistan, particularly at the primary care level. Thus, we developed EBCPGs and created clinical diagnosis and referral pathways for the primary care management of chronic respiratory conditions in Pakistan.
Methods
The source guidelines were selected by two local expert pulmonologists after a thorough literature review on PubMed and Google Scholar from 2010 to December 2021. The source guidelines covered idiopathic pulmonary fibrosis, asthma, chronic obstructive pulmonary disorders, and bronchiectasis. The GRADE-ADOLOPMENT process consists of three key elements: adoption (using recommendations as is or with minor changes), adaptation (effective context-specific changes to recommendations) or additions (including new recommendations to fill a gap in the EBCPG). We employed the GRADE-ADOLOPMENT process to adopt, adapt, adopt with minor changes, or exclude recommendations from a source guideline. Additional recommendations were added to the clinical pathways based on a best-evidence review process.
Results
46 recommendations were excluded mainly due to the unavailability of recommended management in Pakistan and scope beyond the practice of general physicians. Clinical diagnosis and referral pathways were designed for the four chronic respiratory conditions, explicitly delineating the role of primary care practitioners in the diagnosis, basic management, and timely referral of patients. Across the four conditions, 18 recommendations were added (seven for IPF, three for bronchiectasis, four for COPD, and four for asthma).
Conclusion
The widespread use of the newly created EBCPGs and clinical pathways in the primary healthcare system of Pakistan can help alleviate the morbidity and mortality related to chronic respiratory conditions disease in the country.
Similar content being viewed by others


Introduction
Chronic respiratory diseases are a leading cause of morbidity, mortality, and disability worldwide [1]. Chronic obstructive pulmonary disease (COPD) is the 3rd leading cause of mortality worldwide [2]. In the United States (US), the estimated prevalence of asthma and COPD in adults is 9.2% and 6.5%, respectively [3]. In Pakistan, a South Asian lower-middle-income country (LMIC), the prevalence of asthma in adults may be as high as 11.3% [4] and COPD as high as 13.8% [5]. Notable risk factors for chronic respiratory illnesses in Pakistan include exposure to environmental pollution, carbon emissions, excessive indoor air conditioner use, mosquito coil use, and high rates of smoking [6].
Evidence-based clinical practice guidelines (EBCPGs) assist the diagnosis and management of chronic respiratory conditions. Currently, most EBCPGs followed globally, such as the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines [7] and the Global Initiative for Asthma (GINA) guidelines [8], are created by institutions in high-income countries in the West. LMICs, like Pakistan, usually lack the research infrastructure and financial resources to independently created EBCPGs de novo for their own healthcare context [9], and instead adapt those already developed by Western countries. However, the application of such EBCPGs in Pakistan presents a problem, as the landscape of respiratory conditions differs in many aspects. These include but are not limited to epidemiology [4], genetic variability [10], healthcare financing and access [11], triggers and risk factors [12], socio-cultural influences [13], disease related awareness [14]. In addition, there is a lack of specialist pulmonologists in Pakistan, particularly in rural areas. Thus, the role of the general practitioner (GP) in the diagnosis and management of chronic respiratory diseases [15] is especially important in Pakistan.
The GRADE-ADOLOPMENT process [9], developed by GRADE (Grading of Recommendations Assessment, Development, and Evaluation), is a globally accepted and implemented process of EBCPG “adolopment”. “Adolopment” describes a combination of adoption (verbatim use), adaptation (contextual modifications), and de novo development/addition, thus leveraging the benefits of pre-existing high-quality EBCPGs while ensuring local appropriateness. GRADE provides a systematic process to assess the certainty of evidence and to make recommendations based on two standardized tables. The Summary of Findings (SoF) table, which presents a summary of findings and certainty of evidence rating for each included outcome, feeds into the evidence-to-decision (EtD) table. The EtD table serves as a template to summarize the quality of available evidence, the judgements that influence the quality rating, and the effects of different management action plans on the outcomes of choice. This helps guide panelists to make decisions regarding the need for contextual modifications of individual recommendations within an EBCPG [16]. GRADE-ADOLOPMENT has been used in countries and regions across the world, including Saudi Arabia [9], Australia [17], Tunisia [18], the Eastern Mediterranean region [19], the Asia-Pacific region [20], Mexico [21], Pakistan [22], and the United Kingdom [23].
While the Pakistan Chest Society (PCS), established 1983, is involved in the creation of local EBCPGs for management of common respiratory diseases [24], the processes involved in the development of these EBCGPs are not explicitly delineated. Consequently, there is immense need for local respiratory EBCPGs to be developed following a transparent, standardized process that makes use of existing available EBCPGs with appropriate context-specific modifications. Such EBCPGs would bring the healthcare system of Pakistan a step closer to achieving optimal health outcomes in respiratory diseases and would have high credibility, by virtue of their transparent development processes. Thus, we aimed to employ the GRADE-ADOLOPMENT process to develop local EBCPGs and create clinical diagnosis and referral pathways for the primary care management of chronic respiratory conditions in adults by GPs in Pakistan.
Methodology
Setting
This process was conducted at the CITRIC (Clinical and Translational Research Incubator) Center for Clinical Best Practices (CCBP) at the Aga Khan University (AKU), Pakistan. The AKU is a private sector, not-for‐profit hospital in Pakistan, and is also the country’s leading healthcare and biomedical research facility [25].
The CITRIC CCBP at AKU is tasked with the adaptation and development of EBCPG and care pathways to standardize and improve healthcare in Pakistan for the adult population. The GRADE-ADOLOPMENT processes described in this study have been implemented by the CCBP, in collaboration with the expertise of the Section of Pulmonology (within the Department of Medicine) at AKU and the GRADE-USA working group, in the development of EBCPGs for the management of chronic respiratory conditions by GPs in Pakistan. The decision to create EBCPGs for GPs rather than specialist pulmonologists is due to the lack of specialists in Pakistan [26].
Study team
The study team is comprised of the CCBP research staff (who are proficient in GRADE methodology and in the development of EBCPGs) as well as pulmonology faculty led by Section Head of Pulmonology at AKU.
Source guideline selection
The CCBP team first requested the Section of Pulmonology to identify the most common and most impactful respiratory conditions based on their clinical expertise and experience. After finalizing these conditions, the selection process for appropriate and suitable source guidelines was initiated. The source guideline is the single, original, “parent” EBCPG that undergoes the GRADE-ADOLOPMENT process in the development of a local EBCPG. Two local expert pulmonologists appraised various guidelines after an extensive literature review on PUBMED and Google Scholar from 2010 to December 2021, considering criteria such as scope, local familiarity and applicability, rigor, and credibility of creating bodies for each EBCPG. The following were selected as source EBCPGs:
-
1.
British Thoracic Society Guideline for Bronchiectasis in Adults [27].
-
2.
An Official American Thoracic Society/European Respiratory Society/Japanese Respiratory Society/Latin American Thoracic Association Clinical Practice Guideline: Treatment of Idiopathic Pulmonary Fibrosis. An Update of the 2011 Clinical Practice Guideline [28].
-
3.
Global Initiative for Asthma Strategy 2022: Executive Summary and Rationale for Key Changes [29].
-
4.
Global Initiative for Chronic Obstructive Lung Disease (2022 Edition) [30].
Guideline review
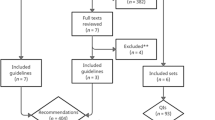
Figure 1 delineates the “adolopment” process used in our study. First, a Table of Recommendations (ToR) was created by extracting and compiling all recommendations mentioned in the source EBCPG. Two senior attending pulmonologists reviewed the ToR independently and marked each recommendation as either “Adopt,” “Adapt” or “Exclude.” Discrepancies were settled in consensus with the Section Head of Pulmonology. Recommendations marked “Adopt” were incorporated as is or with minor changes into the recommendations of our local EBCPG, while recommendations marked “Exclude” were omitted from the final local EBCPG. Exclusion was based on the recommendation pertaining to pediatric or inpatient management, or if the recommendation was deemed irrelevant to the local Pakistani context. Other reasons for exclusion were required to be explained by the reviewers. Recommendations marked “Adapt” were deemed to warrant additional review and revision via the GRADE-ADOLOPMENT process (detailed in the Supplement) before incorporation into the local EBCPGs.
Our “adolopment” process (Fig. 1) had an important difference from the one described originally [31]: recommendations that were deemed to require only minor and straightforward changes prior to adoption and which did not alter the meaning of recommendation but only provided supporting information/clarification, were not subjected to the complete adaptation process consisting of EtD tables and expert panel review. In the original GRADE-ADOLOPMENT process, adaptation is performed if content changes are deemed potentially necessary for a specific recommendation. This is conducted via the creation of an EtD table and subsequent panel review. In our study however, after a thorough review of the recommendations, it was deemed by the experts that no recommendation needed adaptation. Lastly, if any gaps were found during the formation of the clinical diagnosis and referral pathways, additional recommendations were sought through the best-evidence systematic review process. This ideally included use of recommendations from pre-existing EBCPGs other than the source EBCPG. The evidence used to develop this specific recommendation was reviewed by the experts. If no pre-existing suitable pre-existing EBCPGs were found, recommendations were created and added to the clinical diagnosis and referral pathway using peer-reviewed evidence from reputable information sources, such as Medscape. If the best-evidence systematic review process yielded absolutely no citable evidence, additions were made based on expert consensus.

Process of GRADE-ADOLOPMENT and Primary Care Clinical Pathway Creation
Two focus group discussions (FGDs) were conducted to identify challenges faced throughout the entire GRADE-ADOLOPMENT process and to explore corresponding solutions. These FGDs were moderated by one of the authors who was selected due to their holistic experience and qualifications. These qualifications included a medical degree (Bachelor of Medicine, Bachelor of Surgery), a postgraduate public health degree (Master’s in Public Health), and certified training in GRADE methodology. In addition, the moderator also had extensive prior experience and training in conducting FGDs during their postgraduate degree. The FGDs were conducted in English, as all participants possessed complete professional competency in the English language. None of the participants disclosed any conflicts of interest with regards to participating in the FGDs.
The two FGDs each included six participants, including the CCBP staff and the Section Head of Pulmonology, a moderator, and a scribe. The scribe did not participate in the discussion but took notes and recorded the audio of the discourse. Each FGD was one hour-long FGDs. Experts were given the opportunity to first brainstorm challenges and solutions independently based on the challenges faced during the GRADE-ADOLOPMENT process for local EBCPG creation. These challenges and solutions were then discussed within the FGD. At the end of each session, a feedback form was given to elicit additional anonymous feedback. After both FGDs were concluded, the audio recordings were transcribed and annotated with the scribes’ notes. Two members of the research team went through the transcriptions and identified challenges and solutions. Each challenge was decided as per consensus opinion to be either a major or minor challenge. The CCBP team then categorized the final list of specific challenges within broad themes, and their corresponding solutions were presented alongside them.
Timeline of creation of chronic pulmonary disease EBCPGs for Pakistan
The methodology described in this study was carried out according to the following timeline, spanning October 2021-October 2022:
-
Source Guideline Selection: October 2021-March 2022 (about 3 weeks for each of the four guidelines).
-
Creation of Table of Recommendations: March 2022 (3 weeks for all four guidelines).
-
Review of Table of Recommendations: April - May 2022 (for all four guidelines).
-
Creation of final Pakistani Chronic Pulmonary Disease EBCPG: June-July 2022 (all four guidelines).
-
Focal group discussion: July 2022 (2 weeks to determine the challenges and solution).
-
Primary care clinical diagnosis and referral pathways draft creation: August 2022 (2 weeks for all four guidelines).
-
Additional recommendations based on best evidence review: September 2022 (2 weeks for all additional recommendations).
-
Primary care clinical diagnosis and referral pathways finalized: October 2022 (2 weeks for all four pathways).
Results
The total number of recommendations within the source EBCPGs were 24 for idiopathic pulmonary fibrosis (IPF), 59 for bronchiectasis, 93 for COPD and 102 for asthma. Minor changes to recommendations were made for the IPF and bronchiectasis EBCPGs (Tables 1 and 2). Across the four conditions, a total of 46/278 (IPF: 2/24; bronchiectasis: 1/59; COPD: 12/93; and asthma: 31/102) recommendations were excluded, and the recommendations with the reason for exclusion can be found in Supplement Sects. 3–6. The complete EBCPG can be found in the Supplementary Materials.
Primary care clinical diagnosis and referral pathways for the four chronic respiratory conditions are depicted in Supplementary Figs. 1–4. The flowcharts focused on appropriate assessment, counseling, preliminary management, and timely referral. Additional recommendations were included for the IPF (Table 1), bronchiectasis (Table 2), COPD (Table 3), and asthma (Table 4) clinical pathways to cover any clinical gap found.
Challenges and solutions
The challenges faced were broadly categorized into four main themes: resources, stakeholder support and involvement, resistance to change, and methodological limitations (Table 5).
Discussion
We aimed to apply the GRADE-ADOLOPMENT process for EBCPGs creation for the primary care management of four chronic respiratory diseases, and create clinical pathways guiding diagnosis and referral, for general practitioners (GPs) in Pakistan. The primary care pathways derived from the created EBCPGs outlined steps for initial diagnosis by GPs and indications for specialist referral. The best-evidence review process resulted in the addition of seven recommendations for IPF, three recommendations for bronchiectasis, four recommendations for COPD, and four recommendations for asthma to cover gaps in practice.
In Pakistan, currently, there are no frameworks that guide GPs to manage patients with chronic respiratory conditions at the primary care level before referring them to a specialist. This results in patients either being referred without appropriate baseline investigations or not being diagnosed and referred at all, with the existing set-up is inefficient in its utilization of scare resources, time, funds, and limited specialist availability. The delays in specialist pulmonology care also stem from a low index of suspicion exercised by GPs and unsurety of how to proceed with diagnosis and referral [55]. Thus, the implementation of a standardized primary care triage framework may support the identification, appropriate work-up, and timely referral of patients suffering from potentially debilitating chronic lung diseases. The benefits of such systems are well-supported by experiences in other settings across the globe. In the United Kingdom, the implementation of dedicated proformas and care pathways at the primary care level results in considerable savings in healthcare costs due to reduced unwarranted specialist referrals [2]. Moreover, approximately 18 days are saved if GPs themselves refer patients for appropriate work-up, before specialist referral, as opposed to directly to a specialist without work-up [56]. In the Netherlands, the implementation of an asthma care pathway considerably improved GPs awareness regarding asthma care and improved their diagnostic and therapeutic approaches [57].
Amongst the most notable additions made were those pertaining to the management of IPF. This included a recommendation for home oxygen therapy for hypoxemic patients to maintain their SpO2 levels above 90% throughout the day, and the appropriate management of comorbid gastroesophageal reflux disease (GERD) in patients with IPF. The benefits of home oxygen therapy may range from improved exercise tolerance [58] and lesser dyspnea [58] to the attenuation of cardiac dysfunction [59]. Symptoms of GERD are present in more 33% of patients with IPF [38]. The relationship between GERD and IPF is reciprocal, with chronic reflux and micro aspiration causing alveolar injury and remodeling, and the increased negative intrathoracic pressure seen in IPF causing esophageal sphincter dysfunction [60]. Appropriate management of comorbid GERD can thus improve the prognosis of patients with IPF.
We faced several challenges in the creation of primary care pathways. Firstly, we were unable to find pre-existing EBCPGs that holistically covered all aspects of primary care management for the selected chronic respiratory conditions (diagnosis, basic management, and referral). Finer details, such as the signs and symptoms, and risk factors, for each disease were routinely missed. Thus, information had to be compiled from a variety of sources to develop a coherent and complete care pathway. Secondly, the recommendations within the selected source EBCPGs were not structured in a stepwise manner conducive to adaptation into a care pathway. In addition, it was difficult to establish what level of care could be expected from GPs at the primary care level, in terms of basic and sophisticated diagnostic modalities, and disease treatment. It was also important to remain cognizant of the considerable variability in available resources across primary care set-ups in different regions in Pakistan. The focus was thus majorly maintained on a focused history and examination, followed by basic diagnostic investigations, and prompt referral.
Our study has a few limitations. We did not include additional significant stakeholders, such as primary care physicians, nurses, patients, allied health professionals, experts outside of AKU, external organizations concerned with ENT, provincial or federal authorities. This decision was taken in order to minimize undue delays stemming from factors including logistical challenges, a lack of mutual availability, political pressures, conflict of interest, and a lack of incentives. These issues reflect hurdles to the application of the ideal GRADE-ADOLOPMENT process, particularly in LMICs like Pakistan, and exacerbate the processes’ intrinsic partiality. Moreover, while the benefits of primary care triage for chronic respiratory diseases in Pakistan are significant, the feasibility of such practice remains to be seen with particular concern for rural implementation. Rural locations in Pakistan often lack the infrastructure and healthcare facilities needed to provide specialist services, should patients require it. Geographical and financial barriers remain significant challenges to the implementation of the clinical diagnosis and referral pathways. Lastly, there is subjectivity in the TOR review process, as this is done by the individual experts, thus introducing possible bias in the decision to adopt, adapt, or create recommendations.
Conclusion
Our study employed the GRADE-ADOLOPMENT process to create EPCPGs for four chronic respiratory conditions, namely IPF, bronchiectasis, asthma, and COPD. Furthermore, we also created clinical diagnosis and referral pathways for the primary care management of the aforementioned chronic respiratory conditions, clearly delineating a GPs role in diagnosis and timely referral. The widespread adoption of these EPCPGs and clinical pathways in the healthcare system of Pakistan can help alleviate the considerable burden of chronic respiratory illnesses in the country.
Data Availability
All data generated or analyzed during this study are included in this published article and its supplementary information files.
References
Wisnivesky J, De-Torres JPJAogh. The global burden of pulmonary diseases: most prevalent problems and opportunities for improvement. 2019;85(1).
WHO. Global Health Estimates. 2019.
April ALAJA. Methodology: estimated prevalence and incidence of lung disease Available at: https://www.lung.org/research/trends-in-lung-disease/prevalence-incidence-lung-disease/methodology. 2020;30.
Razzaq S, Nafees AA, Rabbani U, Irfan M, Naeem S, Khan MA, et al. Epidemiology of asthma and associated factors in an urban pakistani population: adult asthma study-Karachi. BMC Pulm Med. 2018;18(1):184.
Society PC. Guidelines for the Management of COPD. 2020.
Akhter Z, Nafees AA, Rabbani U, Razzaq S, Irfan M. Risk factors of respiratory symptoms in urban Pakistani population. 2018;52(suppl 62):PA4530.
Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD Exec summary. 2017;195(5):557–82.
Boulet L-P, Reddel HK, Bateman E, Pedersen S, FitzGerald JM, O’Byrne PMJERJ. The global initiative for asthma (GINA): 25 years later. 2019;54(2).
Schünemann HJ, Wiercioch W, Brozek J, Etxeandia-Ikobaltzeta I, Mustafa RA, Manja V, et al. GRADE evidence to decision (EtD) frameworks for adoption, adaptation, and de novo development of trustworthy recommendations: GRADE-ADOLOPMENT. J Clin Epidemiol. 2017;81:101–10.
Sabar MF, Ghani MU, Shahid M, Sumrin A, Ali A, Akram M, et al. Genetic variants of ADAM33 are associated with asthma susceptibility in the Punjabi population of Pakistan. J asthma: official J Association Care Asthma. 2016;53(4):341–8.
Agarwal D, Hanafi NS, Chippagiri S, Brakema EA, Pinnock H, Khoo EM, et al. Systematic scoping review protocol of methodologies of chronic respiratory disease surveys in low/middle-income countries. NPJ Prim care respiratory Med. 2019;29(1):17.
Burney P, Patel J, Minelli C, Gnatiuc L, Amaral AFS, Kocabaş A, et al. Prevalence and Population-Attributable risk for chronic airflow obstruction in a large multinational study. Am J Respir Crit Care Med. 2021;203(11):1353–65.
Rehman A, Amin F, Sadeeqa S. Prevalence of asthma and its management: a review. JPMA The Journal of the Pakistan Medical Association. 2018;68(12):1823–7.
Amir Khan M, Ahmar Khan M, Walley JD, Khan N, Imtiaz Sheikh F, Ali S, et al. Feasibility of delivering integrated COPD-asthma care at primary and secondary level public healthcare facilities in Pakistan: a process evaluation. BJGP Open. 2019;3(1):bjgpopen18X101632.
Santus P, Picciolo S, Proietto A, Falcone F, Mangiacavallo A, Marrocco W, et al. General practitioners and management of patients with respiratory diseases in a real life survey. Panminerva Med. 2012;54(4):293–8.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, et al. GRADE evidence to decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: clinical practice guidelines. BMJ. 2016;353:i2089.
Okely AD, Ghersi D, Loughran SP, Cliff DP, Shilton T, Jones RA, et al. A collaborative approach to adopting/adapting guidelines. The australian 24-hour movement guidelines for children (5–12 years) and young people (13–17 years): an integration of physical activity, sedentary behaviour, and sleep. Int J Behav Nutr Phys Activity. 2022;19(1):2.
Kahale LA, Ouertatani H, Brahem AB, Grati H, Hamouda MB, Saz-Parkinson Z, et al. Contextual differences considered in the tunisian ADOLOPMENT of the european guidelines on breast cancer screening. Health Res policy Syst. 2021;19(1):80.
Darzi A, Harfouche M, Arayssi T, Alemadi S, Alnaqbi KA, Badsha H, et al. Adaptation of the 2015 American College of Rheumatology treatment guideline for rheumatoid arthritis for the Eastern Mediterranean Region: an exemplar of the GRADE Adolopment. Health Qual Life Outcomes. 2017;15(1):183.
Loo BKG, Okely AD, Pulungan A, Jalaludin MY. Asia-Pacific Consensus Statement on integrated 24-hour activity guidelines for children and adolescents. Br J Sports Med. 2022;56(10):539–45.
Coronado-Zarco R, de Olascoaga-Gómez A, Faba-Beaumont MG. Adaptation of clinical practice guidelines for osteoporosis in a mexican context. Experience using methodologies ADAPTE, GRADE-ADOLOPMENT, and RAND/UCLA. J Clin Epidemiol. 2021;131:30–42.
Martins RS, Masood MQ, Mahmud O, Rizvi NA, Sheikh A, Islam N, et al. Adolopment of adult diabetes mellitus management guidelines for a pakistani context: methodology and challenges. Front Endocrinol (Lausanne). 2022;13:1081361.
Reilly JJ, Hughes AR, Janssen X, Hesketh KR, Livingstone S, Hill C, et al. GRADE-ADOLOPMENT process to develop 24-Hour Movement Behavior Recommendations and Physical Activity Guidelines for the Under 5s in the United Kingdom, 2019. J Phys Act Health. 2020;17(1):101–8.
Stellman SD. Book Review: Epidemiology, L. Gordis, 2009, Saunders. 2010.
Haq IU, Rehman ZU. Medical Research in Pakistan; A Bibliometric Evaluation from 2001 to 2020. Library Philosophy and Practice. 2021:1–13.
Bhatti MW. ‘Country facing shortage of internal medicine specialists owing to non-practising female doctors’. The News. 2022.
Hill T, L Sullivan A A, Chalmers D, De Soyza J, Stuart Elborn A, Andres Floto J. R et al British Thoracic Society Guideline for bronchiectasis in adults. 2019;74(Suppl 1):1–69.
Raghu G, Rochwerg B, Zhang Y, Garcia CA, Azuma A, Behr J, et al. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline: treatment of idiopathic pulmonary fibrosis. An update of the 2011 clinical practice Guideline. Am J Respir Crit Care Med. 2015;192(2):e3–19.
GINA. 2022 GINA Report, Global Strategy for Asthma Management and Prevention. 2022.
Disease GIfCOL. Pocket Guide to COPD Diagnosis, Management, and Prevention. 2022.
Schünemann HJ, Wiercioch W, Brozek J, Etxeandia-Ikobaltzeta I, Mustafa RA, Manja V, et al. GRADE evidence to decision (EtD) frameworks for adoption, adaptation, and de novo development of trustworthy recommendations: GRADE-ADOLOPMENT. J Clin Epidemiol. 2017;81:101–10.
Alaa Abu Sayf DRO. Idiopathic Pulmonary Fibrosis (IPF) Clinical Presentation 2021 [Available from: https://emedicine.medscape.com/article/301226
Munchel JK, Shea BS. Diagnosis and Management of Idiopathic Pulmonary Fibrosis. R I, Med J. (2013). 2021;104(7):26 – 9.
Verma S, Slutsky AS. Idiopathic pulmonary fibrosis–new insights. N Engl J Med. 2007;356(13):1370–2.
Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788–824.
Fischer A, Antoniou KM, Brown KK, Cadranel J, Corte TJ, du Bois RM, et al. An official european respiratory Society/American thoracic society research statement: interstitial pneumonia with autoimmune features. Eur Respir J. 2015;46(4):976–87.
American Academy of Family Physicians. Idiopathic Pulmonary Fibrosis [Available from: https://www.aafp.org/family-physician/patient-care/care-resources/respiratory-health/idiopathic-pulmonary-fibrosis.html
Lee JS, Ryu JH, Elicker BM, Lydell CP, Jones KD, Wolters PJ, et al. Gastroesophageal reflux therapy is associated with longer survival in patients with idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;184(12):1390–4.
Ethan E, Emmons. Bronchiectasis 2020 [Available from: https://emedicine.medscape.com/article/296961-overview
Rosen MJ. Chronic cough due to bronchiectasis: ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1 Suppl):122s–31s.
NIH National Heart L, and Blood Institute. Bronchiectasis:Causes and Risk Factors. 2022.
Chang CC, Singleton RJ, Morris PS, Chang AB. Pneumococcal vaccines for children and adults with bronchiectasis. Cochrane Database Syst Rev. 2009;2009(2):Cd006316.
Zab Mosenifar AH, Nidhi S, Nikhanj, Nader Kamangar. Chronic Obstructive Pulmonary Disease (COPD) 2022 [Available from: https://emedicine.medscape.com/article/297664-overview
Qaseem A, Wilt TJ, Weinberger SE, Hanania NA, Criner G, van der Molen T, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of chest Physicians, american thoracic society, and european respiratory society. Ann Intern Med. 2011;155(3):179–91.
Nagelmann A, Tonnov Ä, Laks T, Sepper R, Prikk K. Lung dysfunction of chronic smokers with no signs of COPD. Copd. 2011;8(3):189–95.
Andersen ZJ, Hvidberg M, Jensen SS, Ketzel M, Loft S, Sørensen M, et al. Chronic obstructive pulmonary disease and long-term exposure to traffic-related air pollution: a cohort study. Am J Respir Crit Care Med. 2011;183(4):455–61.
Halpin DM, Criner GJ, Papi A, Singh D, Anzueto A, Martinez FJ, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36.
Morris MJ, Asthma DJP. 2022 [Available from: https://emedicine.medscape.com/article/296301-overview
Education NA, Program P. Expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma-summary report 2007. J Allergy Clin Immunol. 2007;120(5 Suppl):94–S138.
Camargo CA Jr, Weiss ST, Zhang S, Willett WC, Speizer FE. Prospective study of body mass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med. 1999;159(21):2582–8.
Tarlo SM, Balmes J, Balkissoon R, Beach J, Beckett W, Bernstein D, et al. Diagnosis and management of work-related asthma: american college of chest Physicians Consensus Statement. Chest. 2008;134(3 Suppl):1s–41s.
Harding SM. Gastroesophageal reflux, asthma, and mechanisms of interaction. Am J Med. 2001;111(Suppl 8):8s–12s.
Health NIf, Excellence C. Asthma: diagnosis, monitoring and chronic asthma management. National Institute for Health and Care Excellence (NICE); 2017.
Louis R, Satia I, Ojanguren I, Schleich F, Bonini M, Tonia T et al.European Respiratory Society guidelines for the diagnosis of asthma in adults. 2022.
Parente P, Chan BA, Hughes BGM, Jasas K, Joshi R, Kao S, et al. Patterns of care for stage III non-small cell lung cancer in Australia. Asia-Pac J Clin Oncol. 2019;15(3):93–100.
Orchard P, Arvind N, Wint A, Kynaston J, Lyons A, Loveday E, et al. Removing hospital-based triage from suspected colorectal cancer pathways: the impact and learning from a primary care-led electronic straight-to-test pathway. BMJ Qual Saf. 2021;30(6):467–74.
Meuwissen J, Heynens J, Dauven T, Crasborn L, Smeenk F, van der Weijden T, et al. Interprofessional pulmocheck care pathway: an innovative approach to managing pediatric asthma care in the Netherlands. J asthma: official J Association Care Asthma. 2018;55(7):779–84.
Abuserewa ST, Duff R, Becker G. Treatment of idiopathic pulmonary fibrosis. Cureus. 2021;13(5):e15360.
Poloński L, Kuśnierz B, Krzywiecki A, Polońska A, Tendera M, Oklek K, et al. [Effects of long term oxygen therapy in patients with idiopathic pulmonary fibrosis. II. Effect of oxygen therapy on function of heart ventricles]. Pol Arch Med Wewn. 1995;94(4):337–41.
Ghisa M, Marinelli C, Savarino V, Savarino E. Idiopathic pulmonary fibrosis and GERD: links and risks. Therapeutics and clinical risk management. 2019;15:1081–93.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
M.I., A.B.S.Z., A.S.A, S.S., R.K., N.A.R., B.A., S.S.A., M.A.M., A.A.R., S.N., and A.H.H. were all involved in the conceptualization of the guideline process and the creation of the guideline via the grade adolopment process. The initial draft of the manuscript was written by R.S.M., A.P., H.H. and M.C. The manuscript was critically reviewed and approved by all the authors.
Corresponding author
Ethics declarations
Ethics approval
Given the lack of involvement of patients or other human participants, a waiver of ethics approval and informed consent was obtained from the Ethics Review Committee of the Aga Khan University. All methods were conducted in accordance with the highest ethical standards outlined in the 1964 Declaration of Helsinki and its future amendments.
Consent to participate
Not applicable.
Consent to publish
Not applicable.
Conflict of Interest
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Martins, R.S., Hussain, H., Chaudry, M. et al. GRADE-ADOLOPMENT of clinical practice guidelines and creation of clinical pathways for the primary care management of chronic respiratory conditions in Pakistan. BMC Pulm Med 23, 123 (2023). https://doi.org/10.1186/s12890-023-02409-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-023-02409-4