
Abstract
Background
This study aimed to establish normative spirometric equations in a healthy population of Iranian children and adults, and compare these equations with those developed by the Caucasian Global Lung Initiative (GLI) for the first time.
Methods
Spirometric data from healthy Iranian aged 4–82 years sampled in 2019 were used to derive reference equations using the generalized additive model for location (mu), shape (lambda), and scale (sigma).
Results
A total of 418 females and 204 males were included in the study. Applying the GLI standards for the Iranian population resulted from the Z scores of FEV1, FVC, FEV1/FVC, and FEF25−75% was not different from zero. Based on the newly calculated LLN, eleven individuals showed significant values below the LLN for FEV1/FVC. In all age groups, this frequency was less than 5%, except for men over 70 years of age, which was 12.5%. There are significant differences between new data and GLI for Caucasian data.
Conclusion
It is recommended that the values and equations generated from this study should be used by physicians and technicians in their routine practice for the diagnosis and assessment of pulmonary disorders.
Similar content being viewed by others


Introduction
Experimental diagnosis of respiratory diseases, their intensity, and prognosis are principally dependent on spirometric results [1]. Accurate interpretation of spirometry requires standardized reference values that are predicted from its population race, as well as, age, and height [2,3,4,5].
In 2012, the Global Lung Function Initiative (GLI-2012) reported normative reference values, derived from over 160,000 data points in combined datasets from 33 countries. The GLI-2012 equations provided sex, age, height, and ethnic-specific reference equations as well as the lower limit of normal (LLN) values for spirometry [5]. Although this approach included data from various countries, it did not include many populations.
Appropriateness of the GLI-2012 equations should be confirmed prior to their use for regions that are not currently covered by the reference equations [6]. In some studies has been confirmed suitability of GLI-2012 norms for their population, for example in the Australasian [7], Norwegian [8], German [9] and French [10] populations. But, the GLI-2012 norms seem inappropriate for use in the Swedish [11], Finnish [12], and Chinese [13] populations.
Our previous study found that Caucasian GLI equations were not suitable for the Iranian population, especially children under 10 years old [14]. The lack of predictive values specific to the Iranian population may lead to the misclassification of disease. Therefore, standardization of spirometry reference values is very necessary.
Respiratory scales dedicated by spirometry to each person, do not follow a linear model, and the lung volume changes according to height and age with a skewed distribution. A practical approach that has been applied for spirometric data is Generalized Additive Models for Location, Scale, and Shape (GAMLSS). GAMLSS model is a non-parametric regression equation that best fits pulmonary and spirometric measures distribution. This model is the best existing one for the prediction of pulmonary values and the prediction equations offered by GLI-2012 have been confirmed and endorsed by many international respiratory societies. [15, 16].
Simulations show that when the confounders have a non-linear association with the outcome, compared to a parametric representation, GAMLSS modelling reduce the mean squared error for the adjusted exposure effect and avoid inflation of the type I error for testing the exposure effect [17].
This, was the first study in the Iranian population that aimed to predict the standard values of spirometry for Iranian reference population.
Methods
Design
This cross-sectional study was performed in Iran (Tehran) in 2019. This study was approved by the National Institute for Medical Research Development (NIMAD) (code: 978,931, 2019/05/28) and the Ethics Committee (code: IR.NIMAD.REC.1398.257). Conscious and written consent was obtained from all participants.
The study population was gathered from Tehran, and those who referred to local health centers- associated with Tehran Municipality- were included in the study. Overall 44 local health centers were selected by the randomized clustering method. The age range for inclusion in the study was 3–95 years. Informed consent was obtained from all participants / their legal guardians.
Healthy non-smokers between 3 and 95 years old, without a history of current airway or lung disease were included in the study. Exclusion criteria were as follows: not eligible for spirometry test and occurrence of respiratory disorders such as sputum cough, and rhinorrhea in the last 7 days.
Demographical and anthropometric variables such as sex, age, height, and weight were documented. Spirometric indices included FEV1, FVC, FEV1/FVC, and FEF25–75% (Forced expiratory flow averaged over the middle portion of FVC) were measured.
The validity, repeatability, and quality control were done according to the American Thoracic Society/European Respiratory Society (ATS/ERS) recommendations [18, 19], and described in more detail in an earlier paper (first phase of this study) [14].
In this study, 418 females and 204 males in different age groups (4–82 years old) were eligible to enter the study.
Analysis
In the earlier study [14] we measured the lower limits of normal (LLN), Z-scores and percentiles for FEV1, FVC, FEV1/FVC, and FEF25–75% for each person. We determined agreement between the observed values in our population and the GLI reference values. According to the agreement by the GLI team, a mean Z-score outside the range of ± 0.5 was considered clinically significant [5, 11, 20, 21, 22]. The relationship between Z-scores and age, height, weight, and sex was examined using multiple linear regression models in the previous article [14].
In this study, GLI-2012 equations were implemented using the Generalized Additive Models for Location, Scale, and Shape (GAMLSS4.3-1) in software R (version 3.1.2; http://www.r-project.org), this method permitted the fitness of mean (M), coefficient of variance (S), and skewness (L) (Lambda–Mu–Sigma (LMS) of spirometry indices [5, 23].
The spirometry indices were modeled in males and females by age and height as explanatory variables using the Box-Cox-Cole–Green (BCG) distribution. The fittest regression models were chosen by using Schwarz Bayesian Criterion (SBC), Akaike’s Information Criterion (AIC) and assessing optimal degrees of freedom (df) for the cubic spline curve. The goodness of fit was also checked by normal Q–Q plots. Mean (M) indicates the predicted value as follows: M = exp [a + b × ln (heightcm) + c × ln (ageyear) + M-spline] (a, b, and c are coefficients, and M-spline is an age-specific contribution from the spline function. Values of L and S were also calculated based on regression output values of Sspline and Lspline. Finally we calculated LLN as follows: LLN (5th percentage) = exp [ln (M) + ln (1 − 1.645 × L × S)/L]. Z-scores were calculated as (observed-predicted)/SD, where SD was calculated as (predicted-LLN)/1.645 [1, 23].
Agreement between Caucasian values and GLI-2012 Iranian prediction analyzed by Bland–Altman plots.
Result
Six hundred and twenty-two Iranian participants (418 females and 204 males) aged 4–82 years were finally included in this study. The mean (range) age was 38.34 (4–82) years for men and 44.55 (4–80) years for women. The mean (SD) height for men and women were 1.72 (0.08) m and 1.58 (0.08) m over 21 years, respectively. Thirty-nine (19.2%) men and 131 (31.4%) women had a BMI ≥ 30 kg/m2 (Table 1). Demographical and spirometry measurements of the reference population by gender are shown in Table 1 (Table 1).
The Caucasian GLI-2012 was applied to this sample in earlier study [14]. The mean Z-scores of FEV1, FVC and the FEV1/FVC for males and females in different age groups were higher than the Caucasian predicted values (range: 0.01 to 1.05) except for the FEV1/FVC in the age group under 21 years (range: −1.11 to − 0.09).
The Z-scores of FEV1, FVC, FEV1 /FVC, and FEF25–75% distribution based on Caucasian equation by sex and age in the Iranian healthy people is accessible in Table 2.
Iranian version of reference equations for spirometric values
We modeled GAMLSS regression equations for each spirometric parameter (FEV1, FVC, FEV1/FVC, and FEF25−75% obtained from the study population (Look up Tables and equations are available in the supplementary material). For new (Iranian) equations, none of the Z scores (FEV1, FVC, FEV1/FVC and FEF25−75%), are different from zero (by one-sample t-test analysis) in all age groups (P > 0.05). Distributions of Z-Scores based on Iranian (new) and Caucasian (GLI-2012 equations were shown in Table 2.
The obtained reference equations are used to estimate the Lower limit normal (LLN) of the spirometric parameters of FEV1, FVC, FEV1/FVC, and FEF25−75%, for the Iranian population (Look up Tables are available in the supplementary material). Based on the newly calculated LLN, only five individuals showed significant values below the LLN for FEV1, FVC and eleven individuals for FEV1/FVC. This value was calculated in the Caucasian equation of 29 cases [14]. In all age groups, the frequency of Z-score for FEV1/FVC below the LLN was less than 5% except in men aged 70–84 years (12.5%) (Table 3). In the Caucasian equations, the Z-score of FEV1/FVC was significantly higher among < 21 years old (46.2% and 40.0% in males and females respectively). Frequency of FEV1/FVC < LLN by age and sex in Caucasian and Iranian equation is shown in Table 3.
Overall, residual Z-score for regression models was not beyond ± 3 for our model (the standard range for residual is ± 5). (Normal Q–Q plots (Additional file 1: Fig. S1a–h).

Nonlinear correlation analysis between FEV1, FVC and FEV1/FVC, and anthropometric parameters
We found that age and height were the main predictors of the FEV1 (males), FVC (males and females), and age for FEV1/FVC (not height) in both sex for final prediction models by nonlinear correlation analysis. The association between spirometric indices and anthropometric parameters is shown in Fig. 1a–l and Additional file 2: Table S1.
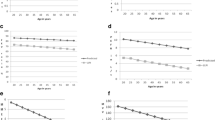
Agreement between Caucasian values and GLI-2012 Iranian prediction
The average differences (SDs) in FEV1 (L), FVC and FEV1/FVC (%) predictions were − 3.66(0.918), − 3.7 (1.087), and – 0.824 (0.034) for men, and − 2.63 (0.49), − 3.2(0.57), and − 0.821 (0.003) for women, respectively. The Bland-Altman plots of FEV1 (L), FVC and FEV1/FVC (%) are shown in Fig. 2a–f.

The Bland-Altman plots of FEV1, FVC and FEV1/FVC by gender
Discussion
This is the first study for the Iranian population that derived predictive equations and values using Lambda–Mu–Sigma (LMS) [18] by GAMLSS models. This model is preferable to the conventional multiple regression analysis which limits the model to several assumptions including normality of the residuals and constant variance [24]. On the other hand, LMS provides a variation in computing LLN through anthropometric data and prevents under-diagnosis of abnormalities in younger and taller individuals, and over-diagnosis of lung disorders in older and shorter people [25].
In this study, we have generated prediction equations for FEV1, FVC, FEV1/FVC, and FEF25−75% based on lung function data from 622 healthy Iranian populations. Genetic and environmental variables play a substantial role in the variability of lung function, so it is important to establish reference values appropriate to the ethnic and ecological characteristics of the local population [26, 27].
Our findings showed that GLI-2012 new equations adequately fitted FEV1, FVC, FEV1/FVC, and FEF25−75% data on the Iranian population for both genders.
In this population study of lung function, we assessed the agreement of lung function predictions between the GLI-2012 Caucasian values and GLI-2012 Iranian measures. The largest average difference was observed in FVC among men and the lowest difference was related to FEV1/FVC index in men and women.
In a study conducted on Jordanian people over 18 years old, based on Bland and Altman results, there were significant differences between the new equation and GLI for Caucasians equations too [24, 28].
In our study, age and height was the main predictors of the FEV1 (males), FVC (males and females), and age for FEV1/FVC (not height) for both sexes.
In different similar studies on various ethnicities, anthropometric predictors have been measured on spirometric indices in both sexes. In a study conducted in India, it was found that age and height were the main predictors of the FEV1 and FVC spirometry parameters in both sexes, for FEV1/FVC, only age was a significant predictor of outcome [29] but not height. This result was consistent with the findings of our study. Chang’s and colleagues reported, the height and weight, but not age, were important predictors in the final prediction models for FVC and FEV1 in Taiwanese children [30].
In our study, the frequency Z-score of FEV1/FVC below LLN was less than 5% in all age groups, except for the group of men over 70 years old (12.5%). This finding was consistent with the results of a study conducted in India 29. But this amount was estimated at 10% in Mozambique’s reference population (Southeast Africa) [31], also the LLNs of FEV1/FVC were less than 0.70 in men above 56 years of age and women above 60 years of age in Chinese aged 4–80 years [1]. Concerning the high prevalence in men over 70 years of age, this may be due to the low sample size in this age group (16 people). However, the initial interview to enter the study was accompanied strictly, but the possibility of bias could not be prevented absolutely. For example, some elderly men may have had the experience of smoking in the past but have forgotten or for some reason declare that they have not had this experience.
This study has several limitations. First, the sample size of this study is not very large. However, we would claim that the sample size of men and women is large enough to have enough power for validating spirometry reference values (at least 150 subjects for each gender) [32].
Conclusion
GLI-2012 Iranian equations fitted FEV1, FVC, FEV1/FVC, and FEF25−75% data of Iranian population for both gender. There were significant differences between measures by GLI for Caucasians and Iranian (new) equations. It is recommended that the values and equations generated from this study should be used by physicians and experts in practice for detecting the disease condition and its severity in Iranian populations.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from Dr. Leyla Sahebi (first author) on reasonable request.
References
Jian W, Gao Y, Hao C, et al. Reference values for spirometry in chinese aged 4–80 years. J Thorac Dis. 2017;9(11):4538–49. https://doi.org/10.21037/jtd.2017.10.110.
Braun L, Wolfgang M, Dickersin K. Defining race/ethnicity and explaining difference in research studies on lung function. Eur Respir J. 2013;41(6):1362–70. https://doi.org/10.1183/09031936.00091612.
Strippoli MP, Kuehni CE, Dogaru CM, et al. Etiology of ethnic differences in childhood spirometry. Pediatrics. 2013;131(6):e1842-9. https://doi.org/10.1542/peds.2012-3003.
Yang TS, Peat J, Keena V, Donnelly P, Unger W, Woolcock A. A review of the racial differences in the lung function of normal Caucasian, Chinese and Indian subjects. Eur Respir J. 1991;4(7):872–80.
Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–43. https://doi.org/10.1183/09031936.00080312.
Blake TL, Chang AB, Chatfield MD, Marchant JM, McElrea MS. Global lung function Initiative-2012 ‘other/mixed’ spirometry reference equation provides the best overall fit for Australian Aboriginal and/or Torres Strait Islander children and young adults. Respirology (Carlton Vic). 2020;25(3):281–8. https://doi.org/10.1111/resp.13649.
HALL GL, THOMPSON BR, et al. The global lung Initiative 2012 reference values reflect contemporary Australasian spirometry. Respirology (Carlton Vic). 2012;17(7):1150–1. https://doi.org/10.1111/j.1440-1843.2012.02232.x.
Langhammer A, Johannessen A, Holmen TL, et al. Global lung function Initiative 2012 reference equations for spirometry in the norwegian population. Eur Respir J. 2016;48(6):1602–11. https://doi.org/10.1183/13993003.00443-2016.
Hüls A, Krämer U, Stolz S, et al. Applicability of the global lung Initiative 2012 reference values for spirometry for longitudinal data of elderly women. PLoS One. 2016;11(6):e0157569. https://doi.org/10.1371/journal.pone.0157569.
Hulo S, de Broucker V, Giovannelli J, et al. Global lung function Initiative reference equations better describe a middle-aged, healthy french population than the European community for steel and coal values. Eur Respir J. 2016;48(6):1779–81. https://doi.org/10.1183/13993003.00606-2016.
Backman H, Lindberg A, Sovijärvi A, Larsson K, Lundbäck B, Rönmark E. Evaluation of the global lung function initiative 2012 reference values for spirometry in a swedish population sample. BMC Pulm Med. 2015;25:26. https://doi.org/10.1186/s12890-015-0022-2.
Kainu A, Timonen KL, Toikka J, et al. Reference values of spirometry for finnish adults. Clin Physiol Funct Imaging. 2016;36(5):346–58. https://doi.org/10.1111/cpf.12237.
Zhang J, Hu X, Shan G. Spirometry reference values for population aged 7–80 years in China. Respirology (Carlton Vic). 2017;22(8):1630–6. https://doi.org/10.1111/resp.13118.
Sahebi L, Rahimi B, Shariat M, Mousavy SH. Evaluation of the Global Lung Function Initiative 2012 reference values for spirometry in an Iranian population. Sci Rep. 2022;12(1):12784. https://doi.org/10.1038/s41598-022-17306-9.
Cole TJ, Stanojevic S, Stocks J, Coates AL, Hankinson JL, Wade AM. Age- and size-related reference ranges: a case study of spirometry through childhood and adulthood. Stat Med. 2009;28(5):880–98. https://doi.org/10.1002/sim.3504.
Rigby RA, Stasinopoulos DM. Smooth centile curves for skew and kurtotic data modelled using the Box-Cox power exponential distribution. Stat Med. 2004;15(19):3053–76. https://doi.org/10.1002/sim.1861.
Benedetti A, Abrahamowicz M. Using generalized additive models to reduce residual confounding. Stat Med. 2004;30(24):3781–801. https://doi.org/10.1002/sim.2073.
Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948–68. https://doi.org/10.1183/09031936.05.00035205.
Hankinson JL, Eschenbacher B, Townsend M, Stocks J, Quanjer PH. Use of forced vital capacity and forced expiratory volume in 1 second quality criteria for determining a valid test. Eur Respir J. 2015;45(5):1283–92. https://doi.org/10.1183/09031936.00116814.
Abdullah N, Borhanuddin B, Shah SA, Hassan T, Jamal R. Global Lung Initiative 2012 spirometry reference values in a large Asian cohort of Malay, Chinese and Indian ancestry. Respirology (Carlton, Vic). 2018;23(12):1173–9. https://doi.org/10.1111/resp.13330.
Ben Saad H, El Attar MN, Hadj Mabrouk K, et al. The recent multi-ethnic Global Lung Initiative 2012 (GLI2012) reference values don’t reflect contemporary adult’s north African spirometry. Respiratory Med. 2013;107(12):2000–8. https://doi.org/10.1016/j.rmed.2013.10.015.
Arigliani M, Canciani MC, Mottini G, et al. Evaluation of the Global Lung Initiative 2012 reference values for spirometry in African children. Am J Respir Crit care Med. 2017;15(2):229–36. https://doi.org/10.1164/rccm.201604-0693OC.
Quanjer PHSS, Stocks J, Cole TJ, Stocks J. GAMLSS in action, 2012.
Al-Qerem W, Hammad A, Gassar E, Al-Qirim R, Ling J. Spirometry reference equations for an adult Middle Eastern population. Expert Rev Respir Med. 2019. https://doi.org/10.1080/17476348.2019.1601560.
Culver BH. How should the lower limit of the normal range be defined? Respir Care. 2012;57(1):136–45. https://doi.org/10.4187/respcare.01427. discussion 143-5.
Schwartz J, Katz SA, Fegley RW, Tockman MS. Sex and race differences in the development of lung function. Am Rev Respir Dis. 1988;138(6):1415–21. https://doi.org/10.1164/ajrccm/138.6.1415.
Quanjer PH, Stanojevic S. Do the global lung function Initiative 2012 equations fit my population? Eur Respir J. 2016;48(6):1782–5. https://doi.org/10.1183/13993003.01757-2016.
Al-Qerem W, Alassi A, Jarab A, Ling J. The applicability of the Global Lung Initiative equations and other regional equations on a sample of healthy Middle Eastern adolescents. Clin Respir J. 2021. https://doi.org/10.1111/crj.13329.
Agarwal D, Parker RA, Pinnock H, et al. Normal spirometry predictive values for the western indian adult population. Eur Respir J. 2020. https://doi.org/10.1183/13993003.02129-2019.
Chang SM, Tsai HJ, Tzeng JY, et al. Reference equations for spirometry in healthy asian children aged 5 to 18 years in Taiwan. World Allergy Org J. 2019;12(11):100074. https://doi.org/10.1016/j.waojou.2019.100074.
Ivanova O, Khosa C, Bakuli A, et al. Lung function testing and prediction equations in adult population from Maputo, Mozambique. Int J Environ Res Public Health. 2020. https://doi.org/10.3390/ijerph17124535.
Quanjer PH, Stocks J, Cole TJ, Hall GL, Stanojevic S. Influence of secular trends and sample size on reference equations for lung function tests. Eur Respir J. 2011;37(3):658–64. https://doi.org/10.1183/09031936.00110010.
Acknowledgements
The authors wish to thank the staff of health houses affiliated with Tehran Municipality and all participants for their collaboration with the research team.
Funding
Noting.
Author information
Authors and Affiliations
Contributions
LS, BR: Writing proposal. BR, LS, SHM: data gathering. SHM: Administration Manager. BR: Clinical manager. LS and MH: Statistical analysis. LS, MSh: Writing draft. BR: Editing manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
This article was the result of a research project approved by the National Institute for Medical Research Development (NIMAD) (code: 978931, 2019/05/28) and the Ethics Committee (code: IR.NIMAD.REC.1398.257). All methods were carried out in accordance with relevant guidelines and regulations. Written and informed consent was obtained from all participants for pulmonary function test using spirometry.
Consent for publication
No personal information of the participants in the article was reported.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Fig. S1.
Normal Q–Q plots for FEV1, FVC, FEV1/FVCand FEF25–75% by gender.
Additional file 2: Table S1.
The association between spirometric indices and anthropometric parameters.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sahebi, L., Rahimi, B., Shariat, M. et al. Normal spirometry prediction equations for the Iranian population. BMC Pulm Med 22, 472 (2022). https://doi.org/10.1186/s12890-022-02273-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-022-02273-8