
Abstract
Background
High serum bilirubin levels have been shown to be associated with an improved pulmonary function test results. Their potential ability to similarly benefit pulmonary function in an environment of polluted air has not been tested. We retrospectively analyzed data of 15,605 apparently healthy individuals in order to evaluate the effect of serum bilirubin levels on forced expiratory volume in 1 s (FEV1).
Methods
Individuals attended the Tel-Aviv Medical Center Inflammatory Survey for a routine annual health check between February, 2002 and June, 2009 and were divided into low, medium and high serum bilirubin levels. Their FEV1 results were compared under various levels of air pollution. Air pollution and weather data were obtained from air pollution monitoring stations of the Israeli Ministry of Environmental Protection.
Results
The elevated serum bilirubin concentrations on FEV1 were evaluated under moderate and high pollution levels FEV1 and were significantly higher in participants with high blood bilirubin levels compared to medium or low levels (p < 0.001 and p = 0.018, respectively). Participants with high levels of bilirubin had preserved FEV1 under exposure to high and medium pollution levels of both Nitrogen Oxide (NOx) and Carbon Monoxide (CO) pollutants (p = 0.003 and p = 0.022, respectively). The multivariate regression analysis revealed that the influence of bilirubin under conditions of air pollution remained significant even after adjustment for FEV1 confounders, but the interaction was not significant.
Conclusions
Elevated serum bilirubin concentrations are associated with preserved lung function in healthy individuals in Israel exposed to high levels of air pollution.
Similar content being viewed by others


Background
Chronic respiratory diseases are among the leading causes of morbidity and mortality worldwide [1]. Short- and long-term exposures to elevated air pollution levels lead to deterioration of lung function in individuals of all ages [2,3,4]. In adults it has been shown that exposure to air pollution cause a decline in pulmonary function by generating oxidative stress in the lung tissue [5, 6]. Bilirubin is the end product of heme breakdown. The majority of bilirubin originates from degradation of erythrocyte hemoglobin in the reticuloendothelial system, while the remaining ~ 20% comes from inefficient erythropoiesis in bone marrow and other heme proteins degradation [7, 8]. Bilirubin was shown to exhibit anti-oxidative and anti-inflammatory properties in vitro and in vivo [9]. In a Swiss study on Air Pollution and Lung Disease in adults (SAPALDIA), increased concentrations of serum bilirubin were associated with improved parameters of forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) ratio (FEV1/FVC) and forced expiratory flow at 25–75% of FVC (FEF25–75%), after adjusting for the effects of sex, age, education, height, and weight and tobacco smoke exposure [10]. One longitudinal study demonstrated a significant negative relationship between baseline bilirubin levels, incidence of coronary heart disease (CHD), and mortality from cardiovascular disease (CVD) [11]. Another study showed inverse association between total bilirubin level and CVD risk, independent of other risk factors [12]. The inclusion of total bilirubin in the standard established risk factors panel, however, provided no significant improvement in CVD risk prediction. A large prospective Korean study revealed that a higher basal bilirubin level within the normal range was associated with a low risk of lung cancer. Smoking and low bilirubin levels have been cumulatively associated with a higher risk of lung cancer [13]. Moreover, bilirubin concentrations were negatively associated with the history, duration, and intensity of smoking, suggesting a possible role of inhaled tobacco in the pathogenesis of lung function deterioration related to oxidative stress [14].
To the best of our knowledge, there are no published data on any correlations between bilirubin levels and pulmonary function test results under conditions of air pollution. In the present study, we assessed this correlation and the interaction between functional parameters, levels of bilirubin and air pollution in a large cohort of apparently healthy Israeli individuals who participated in an annual health survey.
Methods
Description of study population
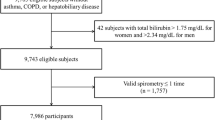
The study population included 15,605 individuals who attended the Tel-Aviv Medical Center Inflammatory Survey (TAMCIS) for a routine annual health check between February, 2002 and June, 2009 as previously described [5]. We excluded subjects for whom there were no bilirubin measurements (n = 1510), or no complete PFT results (n = 471), and those who lived within a radius > 11 km from an air pollution monitoring station (n = 4848). We also excluded 162 participants due to a malignancy history, immunosuppressive therapy, chronic lung disease, pregnancy, systemic steroidal or nonsteroidal treatment (except for aspirin at a dose of 325 mg/day), and serum bilirubin concentrations > 2 standard deviations (± 1.48 mg/dL). The final study cohort was comprised of 8614 individuals (Fig. 1).

Study population flow chart
Spirometry measurements
The PFT consisted of spirometry with a KoKo spirometer (Ferraris Respiratory, Louisville, Colorado, USA), according to the American Thoracic Society quality criteria [15]. The results are expressed as percentage of predictive values (age, height, and sex), and all tests were performed during the early hours of the day. Three to six trials were performed for each subject. All error-free trials were recorded only after there had been two consecutive reproducible trials. System calibrations were carried out daily. All PFTs were performed by a single highly trained technician.
Air pollution and weather data
Air pollution and weather data were obtained from air pollution monitoring stations of the Israeli Ministry of Environmental Protection. These stations are located at roof height in representative areas, which are not located inside neighborhoods with excessive sources of toxic emission, such as industrial plants or heavy traffic. All distances of these stations from the subject’s residence were supplied by the Survey of Israel. Temperature and relative humidity were measured every 30 min by the same air pollution monitoring station. The air monitoring stations continuously measure several major pollutants, specifically, carbon monoxide (CO), nitrogen oxide (NOx, generic nitric oxide), and nitrogen dioxide (NO2). The monitoring process is fully automated and approved by the U.S. Environmental Protection Agency. Stations undergo daily automated calibration and produce annual quality control and assurance test results. In addition, nitrogen dioxide is measured by a chemiluminescence analyzer (Model 42C, Thermo Environmental Instruments), ozone by a UV photometric O3 analyzer (Model 49C, Thermo Environmental Instruments), and carbon monoxide by a gas filter correlation CO analyzer (Model 48C, Thermo Environmental Instruments).
The exclusion of subjects living outside an 11-km radius from an air pollution monitoring station was based on earlier studies on the effect of environmental air pollution on PFT parameters [5, 16]. The levels of selected major pollutants were averaged over the 7 days prior to the participant’s visit to our medical center.
Statistical analysis
All continuous variables are displayed as means (standard deviation, SD) for normally distributed variables, or median (interquartile range, IQR) for variables with abnormal distribution, and were compared by a Student’s t-test and by Mann–Whitney U-test, respectively. Categorical variables are displayed as numbers (%) of patients within each group, and they were compared by a chi-squared test. The cohort was divided into three groups according to low, moderate, and high bilirubin and pollutants levels. We used one-way ANOVA and the Tukey post-hoc analysis to evaluate the differences within these groups. The contribution of bilirubin levels to changes in FEV1 values under different levels of NOx and CO was evaluated using a logistic regression model. FEV1 was defined as the dependent variable, and the model was adjusted for bilirubin levels, age, body mass index (BMI), sex, smoking status (current/past/never), and diabetes diagnosis (yes/no). All analyses were conducted using the SPSS Statistics 22.0 statistical package (IBM Corporation, Armonk, NY, USA).
Results
The study population consisted of 4646 (61.2%) men and 2641 (38.8%) women, with a mean age of 44.84 (± 11.27) years. Among them were 1338 (17.8%) current smokers. Individuals with lower FEV1 values (< 80% of predictive values) were more likely to be men, older, and have a higher BMI. The study population’s characteristics are presented in Table 1.
As expected, current smokers had lower FEV1 and FEV1/FVC values compared to past smokers and participants who never smoked. Additionally, women demonstrated higher FEV1, FVC, and FEV1/FVC values compared to men (Table 2).
To evaluate the effect of total serum bilirubin levels on FEV1, we divided the cohort into low, medium, and high serum bilirubin levels. The results showed that FEV1, but not FVC or FEV1/FVC, was significantly higher in participants with high blood bilirubin compared to low or medium levels (p < 0.001 and p = 0.018, respectively) (Fig. 2).

Assessment of FEV1 according to different levels of serum bilirubin. FEV1 forced expiratory volume in 1 s. Y axis—mean level of FEV1 percent of predictive values. X axis—bilirubin level (mg/dL) divided according to low, moderate, and high serum bilirubin; 0.1–0.59 mg/dL, 0.6–0.8 mg/dL and 0.81–1.47 mg/dL, respectively
Next, we explored the possible effect of bilirubin on FEV1 under conditions of exposure to major air pollutants. Importantly, participants with high levels of bilirubin presented with preserved lung function (FEV1 values) under conditions of exposure to high and medium pollution levels of both NOx and CO pollutants (p = 0.003 and p = 0.022, respectively, Fig. 3a, b). FEV1, under moderate and high level of NOx with high bilirubin, compared to low bilirubin level and moderate bilirubin level is significantly high, p = 0.014, and p < 0.001 respectively (Fig. 3a). Under moderate and high level of CO with high bilirubin, compared to low bilirubin level and moderate bilirubin level, FEV1 is also significantly high, p = 0.027 and p = (Fig. 3b). The apparently protective effect of elevated serum bilirubin concentrations on FEV1 under conditions of moderate and high NOx and CO pollution levels also remained significant after adjusting for age, BMI, sex, smoking status, and diabetes diagnosis (Fig. 4a, b). The interactions between air pollutants (NOx or CO) with bilirubin on PFT results were not significant.

a Assessment of FEV1 according to different levels of serum bilirubin under different NOx levels. FEV1 forced expiratory volume in 1 s, Nox nitrogen oxide. Y axis—mean level of FEV1 percent of predictive values. X axis—NOx level (low, medium and high; 0.4–14.0 ppm; 14.1–22.1 ppm and 22.2–33.5 ppm, respectively). Bilirubin level (mg/dL) divided according to low, moderate, and high serum bilirubin; 0.1–0.59 mg/dL, 0.6–0.8 mg/dL and 0.81–1.47 mg/dL, respectively. b Assessment of FEV1 according to different levels of serum bilirubin under different CO levels. FEV1 forced expiratory volume in 1 s, CO carbon monoxide. Y axis—mean level of FEV1 percent of predictive values. X axis—CO level (low 0.1–0.7 ppm; medium and high 8–0.9 ppm and 1–1.2 ppm). Bilirubin level (mg/dL) divided according to low, moderate, and high serum bilirubin; 0.1–0.59 mg/dL, 0.6–0.8 mg/dL and 0.81–1.47 mg/dL, respectively

a Estimated mean levels of FEV1 in low versus moderate and high levels of bilirubin to NOx adjusted for age, sex, BMI, diabetes, and smoking. FEV1 forced expiratory volume in 1 s, Nox nitrogen oxide, BMI body mass index. Y axis—mean level of FEV1 percent of predictive values. X axis—bilirubin level (mg/dL) divided according to low, moderate, and high serum bilirubin; 0.1–0.59 mg/dL, 0.6–0.8 mg/dL and 0.81–1.47 mg/dL, respectively. Gray line: low NOx level 0.4–14.0 ppm; Black line: 14.1–22.1 ppm and 22.2–33.5 ppm. b Estimated mean levels of FEV1 in low versus moderate and high levels of exposure to CO adjusted for age, sex, BMI, diabetes, and smoking. FEV1 forced expiratory volume in 1 s, CO carbon monoxide, BMI body mass index. Y axis—mean level of FEV1 percent of predictive values. X axis—bilirubin level (mg/dL) divided according to low, moderate, and high serum bilirubin; 0.1–0.59 mg/dL, 0.6–0.8 mg/dL and 0.81–1.47 mg/dL, respectively. Gray line: low CO level 0.1–0.7 ppm; Black line: 0.8–0.9 ppm and 1–1.2 ppm
Discussion
The main finding of this study is the positive association between total serum bilirubin concentrations and lung function in subjects exposed to elevated levels of air pollution. Our relatively large study sample (n = 15,605) was comprised of apparently healthy individuals residing in a major metropolitan area, supporting the likelihood that our findings are applicable to other large urban areas worldwide.
Our results of elevated serum bilirubin levels being associated with improved lung function are compatible with the findings in Swiss [10] and South Korean [14] populations that also described positive associations between serum bilirubin levels and lung function in healthy populations. Moreover, there was an association between a lower risk of respiratory disease and all-cause mortality in patients with normal-range bilirubin levels, while relatively higher levels of bilirubin were associated with a lower risk of respiratory diseases [17]. In another study, bilirubin levels were associated with a longer 6-min walk distance and a better quality of life [18].
Bilirubin is known as a potential antioxidant with anti-inflammatory properties. Elevated bilirubin levels have cytoprotective properties, including antioxidant, anti-inflammatory, and antiproliferative effects [19]. These effects seem to be mediated by an elevated heme oxygenase 1 (HO-1) activity which may be moderated by genetic variations or environmental factors. The role of HO-1 in correlation with the environment was shown in some other studies as well. Moreover, environmental cadmium moderates diabetes type 2 through HO-1 activity [20] and the effect of environmental toxins, such as cigarette smoke, silica, and asbestos on different lung diseases seem to be mediated by bilirubin derivate HO-1 [21]. In contrast to all of these studies that correlated bilirubin with the environment or the effect of bilirubin on functional parameters of respiration, we extended these investigations and looked at how bilirubin levels and pulmonary function test findings were correlated to environmental pollutants.
Our novel finding is that the positive association between pulmonary function tests and bilirubin was significantly stronger among participants exposed to elevated levels of major air pollutants, such as CO and NOx, suggesting that high levels of circulating bilirubin may have a protective effect against lung impairment under conditions of exposure to ordinary urban air pollution. This led us to focus our attention upon a possible mechanism of this protection looking at the metabolism of HO-1 and its therapeutic effects. The use of pharmacological agents that augment expression of HO-1 has been recently investigated, and the results showed protection against a variety of oxidative stress and inflammatory conditions [22]. Induction of HO-1 by a triterpenoid protected neurons against ischemic injury [23], and HO-1 was expressed more abundantly in the lesions of synovial tissue from rheumatoid arthritis patients than in those from the other patient groups. Hemin, auranofin, and HO-1-expression vector induced HO-1, and reduced expression of Tumor Necrosis Factor may mediate less inflammation in those patients [23]. Consequently, its metabolites, such CO, biliverdin and bilirubin, could become parts of a therapeutic strategy for the treatment of various inflammatory illnesses [24, 25].
We are aware that this study has several limitations that bear mention, one of which is its retrospective design. We do not have follow-up data on major respiratory or cardiovascular events, thus precluding any prognostic application of our findings. In addition, measurements of air pollution levels were made according to the subjects’ residential areas and did not take into account their places of work. Finally, we did not perform any mechanistic-oriented studies.
Conclusions
The key finding of this study was that elevated serum bilirubin concentrations are associated with preserved lung function in healthy individuals exposed to elevated levels of air pollution. Bilirubin should be further studied as a surrogate marker for lung function in respiratory diseases in which there are elevated levels of oxidative stress.
Availability of data and materials
The data that support the findings of this study are available from Prof. Shlomo Berliner but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Prof. Shlomo Berliner (Principle investigator).
Abbreviations
- BMI:
-
Body mass index
- CHD:
-
Coronary heart disease
- CO:
-
Carbon monoxide
- CVD:
-
Cardiovascular disease
- FEF25–75%:
-
Forced expiratory flow at 25–75% of FVC
- FEV1:
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
- HO-1:
-
Heme oxygenase 1
- NO2 :
-
Nitrogen dioxide
- NOx:
-
Nitrogen oxide
- PFT:
-
Pulmonary function test
- TAMCIS:
-
Tel-Aviv Medical Center Inflammatory Survey
References
Birben E, Sahiner UM, Sackesen C, Erzurum S, Kalayci O. Oxidative stress and antioxidant defense. World Allergy Organ J. 2012;5(1):9. https://doi.org/10.1097/WOX.0b013e3182439613.
Chen PC, Lai YM, Chan CC, Hwang JS, Yang CY, Wang JD. Short-term effect of ozone on the pulmonary function of children in primary school. Environ Health Perspect. 1999;107:921–5 (PMID: 10544161).
Schindler C, Künzli N, Bongard JP, Leuenberger P, Karrer W, Rapp R, Monn C, Ackermann-Liebrich U. Short-term variation in air pollution and in average lung function among never-smokers. The Swiss study on air pollution and lung diseases in adults (SAPALDIA). Am J Respir Crit Care Med. 2001;163:356–61. https://doi.org/10.1164/ajrccm.163.2.9911116.
Downs SH, Schindler C, Liu L-JS, Keidel D, Bayer-Oglesby L, Brutsche MH, Gerbase MW, Keller R, Künzli N, SAPALDIA Team, et al. Reduced exposure to PM10 and attenuated age-related decline in lung function. N Engl J Med. 2007;357:2338–47. https://doi.org/10.1056/NEJMoa073625.
Steinvil A, Shmueli H, Ben-Assa E, Leshem-Rubinow E, Shapira I, Berliner S, Kordova-Biezuner L, Rogowski O. Environmental exposure to combustion-derived air pollution is associated with reduced functional capacity in apparently healthy individuals. Clin Res Cardiol. 2013;102:583–91. https://doi.org/10.1007/s00392-013-0569-y.
Devasagayam TPA, Tilak JC, Boloor KK, Sane KS, Ghaskadbi SS, Lele RD. Free radicals and antioxidants in human health: current status and future prospects. J Assoc Phys India. 2004;52:794–804.
Berk PD, Howe RB, Bloomer JR, Berlin NI. Studies of bilirubin kinetics in normal adults. J Clin Investig. 1969;48:2176–90.
Tenhunen R, Marver HS, Schmid R. The enzymatic conversion of heme to bilirubin by microsomal heme oxygenase. Proc Natl Acad Sci USA. 1968;61:748–55.
Yoshikawa, T. Free radicals in chemistry, biology, and medicine. OICA; 2019. International. http://epubs.aims.gov.au/handle/11068/296;jsessionid=2B2C01A7AC7927CD5F044D23E023F026.
Curjuric I, Imboden M, Adam M, Robert W, Margaret W, Gerbase M, et al. Serum bilirubin is associated with lung function in a Swiss general population sample. Eur Respir J. 2014;43:1278–88. https://doi.org/10.1183/09031936.00055813.
Sunghwan S, Young RC. Relationship between serum bilirubin levels and cardiovascular disease. PLoS ONE. 2018;13(2):e0193041.
Kunutsor SK, Bakker SJ, Gansevoort RT, Chowdhury R, Dullaart RP. Circulating total bilirubin and risk of incident cardiovascular disease in the general population. Arterioscler Thromb Vasc Biol. 2015;35(3):716–24.
Lim JE, Kimm H, Jee SH. Combined effects of smoking and bilirubin levels on the risk of lung cancer in Korea: the severance cohort study. PLoS ONE. 2014;9(8):e103972. https://doi.org/10.1371/journal.pone.0103972.
Kimm H, Yun JE, Lee KJ, Jee SH. Cigarette smoking and serum bilirubin subtypes in healthy Korean men: the Korea Medical Institute study. J Prev Med Public. 2012;45:105–12. https://doi.org/10.3961/jpmph.2012.45.2.105.
Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, Hallstrand TS, Kaminsky DA, McCarthy K, Meredith, C Standardization of Spirometry Update. An official American thoracic society and European respiratory society technical statement. Am J Resp Crit Care Med. 2019;200:e70–88.
Steinvil A, Fireman E, Kordova-Biezuner L, Cohen M, Shapira I, Berliner S, Rogowski O. Environmental air pollution has decremental effects on pulmonary function test parameters up to one week after exposure. Am J Med Sci. 2019;338(4):273–9. https://doi.org/10.1097/MAJ.0b013e3181adb3ed.
von Eckardstein A, Kronenberg F, Probst-Hensch NM, Horsfall JL, Rait G, Walters K, Swallow DM, Pereira SP, Nazareth I, Petersen I. Serum bilirubin and risk of respiratory disease and death. JAMA. 2011;305:691–7.
Leem A, Kim Y, Lee JH, Kim TH, Kim HY, et al. Serum bilirubin level is associated with exercise capacity and quality of life in chronic obstructive pulmonary disease. Respir Res. 2019;20:279.
Lin JP, Vitek L, Schwertner HA. Serum bilirubin and genes controlling bilirubin concentrations as biomarkers for cardiovascular disease. Clin Chem. 2010;56:1535–43.
Satarung S, Moore M. Emerging role of cadmium and Heme Oxygenase 1 on Type 2 diabetes and cancer susceptibility Tohoku. J Exp Med. 2012;228:267–88.
Wu ML, Layne MD, Yet SF. Heme oxygenase-1 in environmental toxin-induced lung disease. J Toxicol Mech Methods. 2012;22(5):323–9.
Motterlini R, Foresti R. Heme oxygenase-1 as a target for drug discovery. Antioxid Redox Signal. 2014;20–26:1810–6.
Feng Zhang F, Wang S, Zhang M, Weng Z, Li P, Gan Y, Zhang L, et al. Pharmacological induction of heme oxygenase-1 by a triterpenoid protects neurons against ischemic injury. Stroke. 2012;43:1390–7.
Kobayashi H, Takeno M, Saito T, Takeda Y, Kirino Y, Noyori K, et al. Regulatory role of heme oxygenase 1 in inflammation of rheumatoid arthritis. Arthritis Rheumatol. 2006;54:1132–42.
Ryter WS, Choi AMK. Targeting heme oxygenase-1/carbon monoxide for therapeutic modulation of inflammation. Transl Res. 2016;167:7–34.
Acknowledgements
Not applicable.
Funding
The authors received no financial support for the research.
Author information
Authors and Affiliations
Contributions
EF, US, DZ, IS, OR, SST and SB participated in study conception and design. RYB, OR, DZ, SB, and SST participated in patient recruitment as well as collection of clinical information. US, RYB, OR, SST, SB, IZ and EF participated in analysis and interpretation of the data. US, EF, SST drafted the manuscript and IS, DZ, SB, OR and RYB helped in critical review of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All investigations were conducted in accordance with the ethical standards of The Tel Aviv Sourasky Medical Center and the World Medical Association Declaration of Helsinki. The study was approved by the Institutional Review Board of The Tel Aviv Sourasky Medical Center with approval number 2002-049-TLV. Written informed consent was obtained from all individuals.
Consent for publication
All of the authors have read and approved the final manuscript for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shapira, U., Brezinski, R.Y., Rogowski, O. et al. Association between elevated serum bilirubin levels with preserved lung function under conditions of exposure to air pollution. BMC Pulm Med 21, 119 (2021). https://doi.org/10.1186/s12890-021-01488-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-021-01488-5