
Abstract
Background
The differential diagnosis of a mediastinal mass is a common challenge in clinical practice, with a wide range of differential diagnosis to be considered. One of the rarer causes is tuberculosis. Atypical presentations of tuberculosis are well documented in immunocompromised patients, but should also be considered in the immunocompetent.
Case presentation
This case outlines a previously healthy 22 year-old immunocompetent male presenting with worsening chest pain, positional dyspnea, dry cough and dysphagia. Chest x-ray showed evidence of an isolated anterior mediastinal mass, which was confirmed on computed tomography. A mediastinoscopy was diagnostic as histology revealed necrotizing granulomatous inflammation and the presence of acid-fast bacilli, indicating mediastinal tuberculosis.
Conclusion
Typically the underlying presentation of mediastinal tuberculosis is mediastinal lymphadenitis. This case was unusual in that we detected an isolated large anterior mediastinal mass accompanied by a relatively small burden of mediastinal lymphadenitis. Cases similar to this have been documented in immunosuppressed patients however in our case no evidence of immunosuppression was found. This case report emphasizes the importance that a detailed and logical pathway of investigation is pursued when encountering a mediastinal mass.
Similar content being viewed by others


Background
Mediastinal masses are routinely encountered in clinical practice and a wide range of differential diagnoses must be considered. A less common cause is tuberculosis, a disease recognized for its atypical presentations attributed to its ability to affect almost any organ system. Tuberculosis has an incidence of 126 per 100,000 according to the latest report from the World Health Organization (WHO) [1]. Mycobacterium tuberculosis undergoes lympho-heamatogenous dissemination after entering the respiratory tract. Typically the mediastinal and hilar lymph nodes are the first lymphatic tissues M. tuberculosis will encounter [2] and it may then spread to other organ systems. Thirty percent of patients present with extra-pulmonary tuberculosis, an example of which is illustrated by this case [3].
Case presentation
A 22-year-old Nigerian male presented to the accident and emergency department with a 2-week history of worsening chest pain associated with positional dyspnea, dry cough and dysphagia. He had no significant past history, was on no medication and denied any significant family history. The patient was resident in the Republic of Ireland since early childhood and had no recent travel abroad.
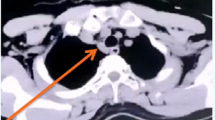
Chest radiography illustrated soft tissue enlargement within the right paratracheal stripe (Fig. 1a). Subsequent computed tomography of the thorax with contrast, revealed a large right-sided mediastinal mass with accompanying lymphadenopathy that encompassed the pre-tracheal, para-tracheal, tracheobronchial, hilar and subcarinal regions superior to the right brachiocephalic vein, superior vena cava right pulmonary artery and superior right pulmonary vein (Fig. 1b).

a Initial chest x-ray demonstrates soft tissue enlargement within the right paratracheal stripe; b Contrast computed tomography of the thorax shows a large right-sided mediastinal mass with accompanying lymphadenopathy encompassing the pre-tracheal, para-tracheal, tracheobronchial, hilar and subcarinal regions. (The images have been placed in reverse order and so the caption does not match the image. The CXR should be Figure 1a and the CT image should be Figure 1b)
Initial haematological testing revealed the following: C-reactive protein 62 (<5), ESR 102 (<20) and LDH 819 (208–378). Coagulation studies were also abnormal with a PT of 16.3 (11–13.5) and an INR of 1.4. Other laboratory tests including full blood count, liver function test, troponin, electrolytes and glucose were normal as were the tumor markers beta human chorionic gonadotrophin (hCG) and alpha-fetoprotein. Computed tomography of the abdomen and pelvis was also concurrently done and found to be normal, with no evidence of other lymphadenopathy or masses.
Bronchoscopic evaluation illustrated 50 % external compression of the distal trachea with normal distal airways and no endobronchial mass visualized. Trans-bronchial biopsies showed no abnormality and bronchoalveolar lavage (BAL) showed pus cells but no organisms and tested negative for acid-fast bacilli. A full virology screen including HIV, hepatitis B and C were also negative. Whilst lymphoma was our primary working diagnosis due to the patient’s age, mildly elevated LDH and the presence of a mass, tissue confirmation was pursued as initial bronchoscopic biopsies were not confirmatory.
A mediastinoscopy was subsequently performed and histology confirmed necrotizing granulomatous inflammation with the presence of acid fast bacilli (AFB) diagnostic of mediastinal tuberculosis (Fig. 2). The patient was commenced on a standard anti-tuberculosis regime for a total of 6 months and has since completed his course of treatment. His most recent chest x-ray (CXR) shows interval improvement (Fig. 3) and he has now been discharged from the respiratory service.

Histology slide of a tissue specimen obtained via mediastinoscopy with Ziehl Neelsen staining shows a single acid-fast bacilli in center of necrosis

Follow up chest x-ray shows considerable reduction in the soft tissue previously noted in relation to the right paratracheal stripe
Conclusions
The differential diagnosis of a mediastinal mass is a common challenge in clinical practice (Table 1)[4]. Patients with these lesions are typically asymptomatic until they develop mass effects, such as chest pain, dyspnea or cough due to compression of local structures. Such symptoms prompted this patient’s presentation. Investigation of such lesions must consider the wide range of differentials. As part of the initial evaluation, a detailed history and physical examination should be performed, looking specifically for lymphadenopathy, thyroid enlargement, testicular masses or evidence of immunosuppression. None of these features were present in this patient. A full haematological screen should be performed including relevant tumor markers including beta hCG and alpha-fetoprotein. Gene Xpert analysis is another well-recognized modality in rapid diagnosis of tuberculosis and should be considered in the work up of a mediastinal mass. Contrast computed tomography (CT) of the thorax is useful to further characterize a mediastinal mass. Radiographic findings suggestive of tuberculosis are a ghost like ring enhancement within a matted mass of nodes [5]. Importantly, tuberculosis has been shown to mimic malignancy both radiologically and clinically [6] hence diagnostic confirmation by histology is imperative prior to therapeutic intervention. This can be obtained by bronchoscopy or endoscopic bronchial ultrasound allowing for fine needle aspirate cytology or transbronchial needle aspirate to obtain a diagnostic pathological specimen.
There are several and varied presentations of mediastinal tuberculosis including lymph node calcification, oesophagomediastinal fistula, pericardial TB and fibrosing mediastinitis. The underlying cause of these lesions is mediastinal lymphadenitis, which extends to involve surrounding structures creating strictures and fistulation [7]. This case was unusual in that we detected an isolated large anterior mediastinal mass accompanied by a relatively small burden of mediastinal lymphadenitis. Prior cases similar to this have been noted to occur in immunosuppressed individuals such as those with seropositive HIV with a CD4 T lymphocyte count <200/mm^3 but are even more rarely found in HIV positive patients with a CD4 T lymphocyte count >200/mm^3 [8, 9]. Such a presentation is unusual in immunocompetent patients, although has been shown to occur more frequently in patients from countries where TB is endemic [10].
There are few documented cases of tuberculosis presenting as an isolated anterior mediastinal mass in an immunocompetent patient. Comprehensive review of the literature reveals ten similarly described cases with the majority occurring in the pediatric population aged 2 years or younger. Of the published cases on adults all three patients were male with age ranging from 32 to 76 years [11–14]. The masses varied in composition and behavior, with one case describing a cystic mass and another a mass infiltrating the right atrium. Similar to this case all three patients were treated with medical therapy. The limited published data on adult presentations of mediastinal tuberculosis in immunocompetent patients does reveal that presentation is usually associated with mass effect symptoms and that a diagnosis was only revealed following histological confirmation, both features observed in this case [15–20].
In summary, while the aetiology of a mediastinal mass can be difficult to establish because of the wide differential, it is imperative that a through and logical scheme of investigation including tissue diagnosis is pursued. This case aims to highlight the importance of considering tuberculosis in the differential even in immunocompetent patients presenting with an isolated mediastinal mass that cannot otherwise be explained.
Ethics, consent & permissions
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor of this journal. This project was carried out within an appropriate ethical framework. This manuscript conforms with the CARE guidelines published in 2013 (see Additional file 1).
Consent to publish
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Availability of data
N/A.
Abbreviations
- HIV:
-
Human innunodeficiency virus
- ESR:
-
Erythrocyte sedimentation rate
- LDH:
-
Lactate dehydrogenase
- INR:
-
International normalized ratio
- PT:
-
Prothrombin time
- Beta hCG:
-
Human chorionic gonadotrophin
- CXR:
-
Chest x-ray
- ZN:
-
Ziehl Neelsen
- AFB:
-
Acid fast bacilli
- CT:
-
Computed tomography
References
World Health Organization. Global tuberculosis report 2014. Geneva: World Health Organization; 2014.
Rom WN, Garay SM. Tuberculosis. 2nd ed. New York: Little Brown and Company; 2000. p. 577.
CDC. Reported Tuberculosis in the United States, 2013. Atlanta: U.S. Department of Health and Human Services, CDC; 2014.
Strollo DC, Rosado de Christenson ML, Jett JR. Primary mediastinal tumors. Part 1: tumors of the anterior mediastinum. Chest. 1997;112(2):511–22.
Andronikou S, Joseph E, Lucas S, Brachmeyer S, Du Toit G, Zar H, et al. CT scanning for the detection of tuberculous mediastinal and hilar lymphadenopathy in children. Pediatr Radiol. 2004;34(3):232–6.
Tan CH, Kontoyiannis DP, Viswanathan C, Iyer RB. Tuberculosis: A benign imposter. AJR Am J Roentgenol. 2010;194(3):555–61.
Jeong YJ, Lee KS. Pulmonary Tuberculosis: Up-to-date imaging and management. AJR Am J Roentgenol. 2008;191(3):834–44.
Kim HY, Song KS, Goo JM, Lee JS, Lee KS, Lim TH. Thoracic sequelae and complications of tuberculosis. Radiographics. 2001;21(4):839–60.
Leung AN, Brauner MW, Gamsu G, Mlika-Cabanne N, Ben Romdhane H, Carrette MF, et al. Pulmonary tuberculosis: comparison of CT findings in HIV-seropositive and HIV-seronegative patients. Radiology. 1996;198(3):687–91.
Codecasa LR, Besozzi G, De Cristofaro L, Miradoli A, Sabolla L, Tagliaferri B. Epidemiological and clinical patterns of intrathoracic lymph node tuberculosis in 60 human immunodeficiency virus-negative adult patients. Monaldi Arch Chest Dis. 1998;53:277–80.
Vincken W, Vandenbrande P, Roels P, Pirngadi J, Welch W. Isolated paratracheal mass of tuberculosis origin in an adult patient. Eur J Respir Dis. 1983;64(8):630–5.
Jain N, Khilnani G, Hadda V, Iver V. Cystic mediastinal mass: A rare presentation of tuberculosis; Chest. 2013 Oct; 144:4 Meeting Abstract
Kumar N, Gera C, Philip N. Isolated mediastinal tuberculosis: a rare entity. J Assoc Physicians India. 2013;61(3):202–3.
Maeder M, Ammann P, Rickli H, Schoch OD. Fever and night sweats in a 22-year-old man with a mediastinal mass involving the heart. Chest. 2003;124(5):2006–9.
Gillies MJ, Farrugia MK, Lakhoo K. An unusual cause of a superior mediastinal mass in an infant. Pediatr Surg Int. 2008;24(4):485–6.
Ahmed A, Mirza S, Rothera MP. Mediastinal tuberculosis in a 10- month-old child. J Laryngol Otol. 2001;115(2):161–3.
Khilnani GC, Jain N, Hadda V, Arava SK. Anterior mediastinal mass: a rare presentation of tuberculosis. J Trop Med. 2011;2011:635385.
De Ugarte DA, Shapiro NL, Williams HL. Tuberculous mediastinal mass presenting with stridor in a 3-month-old child. J Pediatr Surg. 2003;38(4):624–5.
Thirithuvathas AJ, Ravikumar S, Gnanaseelan T. Huge prepericardial tuberculosis abscess in a 2-year-old child. J Pediatr Surg. 1989;24(11):1124.
Boussetta K, Tinsa F, Ghaffari H, Brini I, Aloui N, Jaubert F, et al. Mediastina Tuberculosis mass in a three-month-old boy. Tunis Med. 2010;88(8):602–4.
Acknowledgements
N/A.
Funding
No funding was required for this case report or the research involved.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None of the authors involved in this case report have any competing interest in accordance with BioMed Central’s guidelines.
Authors’ contributions
SM was the primary author and was responsible for gathering all relevant patient data, conducting a literature review and drafting the case report. SC was responsible for editing and formatting of the case report. VP also assisted with critical editing. LC provided advice on discussion points in the conclusion. CR and CO provided diagnostic evaluation of the tissue samples and supplied the histopathology images in this report. KR assisted in diagnostic investigations resulting in the diagnosis. CS was the primary consultant for this patient and also provided critical review of the case report. All authors read and approved the final manuscript.
Additional file
Additional file 1:
CARE Checklist (2013) of information to include when writing a case report. (DOCX 1644 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Maguire, S., Chotirmall, S.H., Parihar, V. et al. Isolated anterior mediastinal tuberculosis in an immunocompetent patient. BMC Pulm Med 16, 24 (2016). https://doi.org/10.1186/s12890-016-0175-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-016-0175-7