
Abstract
Background
Several cases of Burkholderia pseudomallei infection in CF have been previously reported. We aimed to identify all cases globally, risk factors for acquisition, clinical consequences, and optimal treatment strategies.
Methods
We performed a literature search to identify all published cases of B. pseudomallei infection in CF. In addition we hand-searched respiratory journals, and contacted experts in infectious diseases and CF around the world. Supervising clinicians for identified cases were contacted and contemporaneous clinical data was requested.
Results
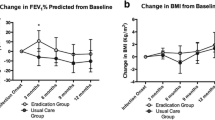
25 culture-confirmed cases were identified. The median age at acquisition was 21 years, mean FEV1 % predicted was 60 %, and mean BMI was 19.5 kg/m2. The location of acquisition was northern Australia or south-east Asia for most. 19 patients (76 %) developed chronic infection, which was usually associated with clinical decline. Successful eradication strategies included a minimum of two weeks of intravenous ceftazidime, followed by a consolidation phase with trimethoprim/sulfamethoxazole, and this resulted in a higher chance of success when instituted early. Three cases of lung transplantation have been recorded in the setting of chronic B. pseudomallei infection.
Conclusion
Chronic carriage of B. pseudomallei in patients with CF appears common after infection, in contrast to the non-CF population. This is often associated with an accelerated clinical decline. Lung transplantation has been performed in select cases of chronic B. pseudomallei infection.
Similar content being viewed by others


Background
Burkholderia pseudomallei is a gram-negative environmental bacterium found in soil and surface water that causes melioidosis, which most commonly occurs in south-east Asia and northern Australia [1]. Melioidosis has been increasingly recognised to occur in diverse tropical locations globally, including the Americas and Africa [2]. B. pseudomallei is now classified by the US CDC as a tier-1 select agent because of its aerosolized biothreat potential (http://www.selectagents.gov/). Infection can occur through inhalation, aspiration and ingestion, although transmission most commonly occurs via percutaneous inoculation [3]. Pneumonia is the most common clinical manifestation (presumably via haematogenous spread to the lungs), with a spectrum including mild self-limiting infection, subacute pulmonary disease mimicking tuberculosis, rapidly progressive multifocal pneumonia and systemic sepsis which confers a high mortality of over 50 % [4]. Melioidosis is often reported in people returning to their home country after travelling to an endemic region. At-risk tourists include those with diabetes and cystic fibrosis (CF) exposed to soil and surface water or monsoonal storms where aerosolization of B. pseudomallei may occur [1, 2].
Generally patients who survive infection clear the organism and rarely relapse following an adequate duration of therapy [5]. In the 25-year Darwin Prospective Melioidosis Study [6], only one of over 750 consecutive melioidosis patients had evidence of long-term persisting infection with B. pseudomallei. This patient with non-CF bronchiectasis has continued to have positive sputum culture results for B. pseudomallei 14 years after diagnosis and treatment of melioidosis. Whole genome sequencing of isolates obtained from this patient over a 12-year period demonstrates loss of virulence and immunogenic factors, as well as deletion of pathways involved in environmental survival [7]. There have been a number of published case reports of patients with CF who have acquired B. pseudomallei infection and a number of these cases have demonstrated chronic carriage of B. pseudomallei in patients with CF [8–17].
In this study, we aimed to describe the international experience of infection with B. pseudomallei in patients with CF. We have examined potential risk factors for acquisition and persistence of infection, summarised global experience of effective antibiotic strategies, and assessed the long-term clinical sequelae of infection.
Methods
The study was conducted in accordance with the amended Declaration of Helsinki, and was approved by the local human research ethics committee. (Metro North Hospital and Health Service Human Research Ethics Committee, Queensland, HREC/13/QPCH/51). A literature search (utilising Medline, Embase, CINAHL, AustHealth and ScienceDirect databases and by Google Scholar) was performed to identify all published cases of B. pseudomallei infection in patients with CF in July 2013 and repeated in August 2014 (Additional file 1). Case reports were hand-searched and clinicians from European, North American, and Australasian CF centres that had either reported B. pseudomallei in CF patients, or were experts from CF microbiology laboratories, were contacted to locate additional cases not previously reported. Data entry sheets were provided to the clinicians that had supervised the care of the identified cases, and results including contemporaneous clinical metrics were compiled (Additional file 2). Where supervising clinicians could not be contacted, information was extracted from the published reports [8, 9, 11, 14]. Chronic infection was defined as persistent cultures of B. pseudomallei from sputa or endobronchial washings for 12 months or more.
Results
Case identification
Twenty-five culture-proven cases between 1987 and 2015 were identified (Table 1). 16 cases were identified by literature search. A further nine cases were identified through international consultation with experts of CF and infectious disease that had experience in the diagnosis and management of B. pseudomallei infection. Of the 25 cases, detailed clinical data were made available by the treating clinicians for 21 cases, and in the remaining four cases details were extracted from published reports. An additional two cases were identified where melioidosis was suspected based on positive B. pseudomallei serology, although culture confirmation was elusive. Both cases died from progressive refractory respiratory infection after being presumptively infected while travelling overseas; these cases were not included further in this analysis. Three additional possible cases from Mexico were identified through hand-searching references of published articles [18]. There were insufficient data available and the accuracy of bacterial identification was uncertain, therefore these cases were also excluded.
Epidemiology and risk factors for B. Pseudomallei acquisition
Of the 25 cases, 15 (62.5 %) were males, and ten females. The median age at acquisition was 21 years (range 7–38 years). The presumptive location of acquisition for the majority was either northern Australia or South-east Asia. There was one case each of presumed acquisition in Brazil, Aruba and the British Virgin Islands, respectively. The mean forced expiratory volume in 1 s (FEV1) was 60 % predicted (range 38-107 %) and mean body mass index (BMI) was 19.5 kg/m2 (range 13–24). Two cases were siblings. Specific Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) mutations were documented in 17 of the 25 patients. Of these, 47 % (8) were F508del homozygotes and 35 % (6) were F508del heterozygotes. Having CF (pulmonary disease) was the apparent major risk factor in all patients. Of the 19 patients where data were available, CF-related diabetes was present in three (16 %) and there was impaired glucose tolerance in one. Other common risk factors for infection with B. pseudomallei such as hazardous alcohol use, chronic renal disease, congestive cardiac failure, rheumatic heart disease and immunosuppressive therapy were not reported in any of the cases.
Clinical and radiological manifestations of infection with B. Pseudomallei
Of the 25 patients, clinical manifestations at the presumed time of acquisition were available in 24. In ten (42 %), isolation of B. pseudomallei was an incidental finding on routine sputum surveillance and in the remaining 14 patients (61 %), isolation of B. pseudomallei was associated with symptoms of increased cough and sputum. Systemic features (either one or a combination of the following: fever, weight loss or deteriorating glycemic control) were reported in 10 patients. New radiological changes were documented in eight patients, with patchy areas of consolidation being the most common abnormality reported. Lobar consolidation, progressive lobar destruction, increased bronchiolectasis with “tree-in-bud” opacities and progressive bronchiectasis were also reported.
Long-term outcomes following infection with B. Pseudomallei
In five patients, acquisition of B. pseudomallei did not result in chronic infection (≥12 months). In one of these patients (patient 9), there were three different B. pseudomallei infections over an eight-year period, each with distinct organisms as confirmed by multilocus sequence typing, [6] and each episode was successfully cleared with 2 to 3 week courses of intravenous ceftazidime and oral trimethoprim/sulfamethoxazole (TMP/SMX) followed by consolidation with three months of oral TMP/SMX. This case was considered to have been infected with distinct B. pseudomallei strains on three occasions [6]. Two patients presented with acute pneumonia and the organism was eradicated after a combination of intravenous followed by consolidation nebulized and oral antibiotics (patient 16 and 20). One further patient who was not unwell at the time of isolation of the organism spontaneously cleared the infection without specific antibiotics directed at B. pseudomallei (patient 19).
In 19 patients (79 %), initial infection was followed by evidence of chronic infection (range 1 – 11 years) (Table 2). Of these patients, 14 were thought to have had an accelerated decline in pulmonary status by their physician, although in one case the reported decline occurred after a four-year period of clinical stability despite evidence of persistent infection. Markers of clinical deterioration that were reported included increased exacerbation frequency, reduced response to intravenous antibiotics and an accelerated decline in lung function. Six patients had died by August 2014, between two and six years after the first isolation of B. pseudomallei (patients 6, 7, 8, 11, 15 and 18). In two, septicemia was documented and complicated by respiratory failure and death (patients 7 and 15). In one recurrent bacteraemia occurred and oral corticosteroids appeared to precipitate an episode (patient 15). Tigecycline controlled bacteremia despite progressive resistance to TMP/SMX and ceftazidime.
In five patients, evidence of chronic infection (duration 5–17 years) was not associated with clinical deterioration (patients 1, 2, 10, 17 and 22).
In one patient duration of infection and outcome was unknown (patient 5), and another one patient was identified shortly prior to publication (patient 25). Initial sputa have been clear after three weeks of intravenous antibiotics. The patient continues on suppressive oral antibiotics, and long term outcomes are awaited.
Eradication strategies
Specific eradication strategies were documented in 19 of the 25 patients. Six patients (including patient 9 - multiple episodes of infection) achieved clearance of B. pseudomallei. Eradication attempts were unsuccessful in 11 patients and there was an unknown outcome in two patients (patient 24, patient 25, Table 3). For cases of successful eradication, the period of known infection was usually less than 12 months, whereas failed eradication usually occurred where long-term infection was evident. Ceftazidime was a key component of induction therapy in all but one of the patients with successful eradication, and all had consolidation therapy from one to four months after completion of intravenous antibiotics and in most cases, oral TMP/SMX was used. In select cases, antibiotic regimens also included combinations of oral amoxicillin/clavulanic acid, doxycycline and chloramphenicol, and nebulized meropenem (250–500 mg twice daily in 4 ml of sterile water).
Two patients spontaneously cleared infection without specific eradication strategies (patients 2 and 19) (Table 2). Whilst not a formal approach at eradication of B. pseudomallei, patient 12 was treated with 3-week courses of ceftazidime, meropenem and tobramycin over a 15-month period for repeated episodes of pneumonia, after which time B. pseudomallei was no longer cultured from sputum.
Transplantation with B. pseudomallei
Transplantation was considered for six patients but two patients were not listed due to concerns about the potential risk of B. pseudomallei graft infection after transplantation (patient 15, patient 18). One patient was listed for transplant but deteriorated very rapidly and died several months later without transplant (patient 8). Three patients have undergone lung transplants (patients 1, 11 and 21) and immediate post-transplant results have been satisfactory. One patient (patient 1) remains well 10 years post-transplant with normal lung function despite endobronchial washings remaining positive for B. pseudomallei; another patient (patient 12) died five years after transplantation, and post-transplant endobronchial washings were positive; and the third patient (patient 21) is alive two years after transplantation also with B. pseudomallei recurrently isolated from post-transplant respiratory samples. Chronic B. pseudomallei suppression has been used in all cases (either TMP/SMX or doxycycline).
Discussion
CF is a disease that predominates in people of Caucasian descent and most patients do not live in tropical or sub-tropical regions where B. pseudomallei is endemic. As survival has increased, CF patients have increasingly had the opportunity to travel, and as a consequence over the past two decades there have been a number of reports of infection with B. pseudomallei in CF patients [8–17].
We have identified 25 cases of B. pseudomallei in CF patients and the vast majority of CF patients who have become infected with B. pseudomallei have acquired the organism through travel to endemic areas such as Southeast Asia and northern Australia. Most patients already had significant structural lung disease and low BMI, which suggests these factors are likely to be important risk factors for acquisition of the organism in CF. However severe CF disease per se was not an obvious prerequisite for acquisition. Some patients were also diabetic but other risk factors for melioidosis such as hazardous alcohol use, chronic renal disease, heart disease and immunosuppressive therapy were not present in this cohort.
In contrast with the general population, acquisition of B. pseudomallei in CF appeared to be more likely to result in chronic infection, which is problematic given how difficult it can be to eradicate this pathogen even with targeted antimicrobial therapy. Whilst the clinical manifestations of infection were varied in the CF patients, and a chronic quiescent disease state can obviously occur, the establishment of chronic infection in most patients usually heralded further clinical deterioration, with progressively refractory bronchopulmonary sepsis being a common feature. Delayed diagnosis may contribute to chronic infection and early attempts to eradicate are recommended. This requires expeditious recognition of the infection in travellers returning from endemic areas. The identification of B. pseudomallei can be challenging, and it is possible that isolates may be confused with other more common CF pathogens including other Burkholderia species, particularly if laboratories are not familiar with in vitro characteristics of B. pseudomallei [8, 14, 15]. Furthermore, infection with B. pseudomallei does not always result in immediate onset of symptoms as it often would in patients without CF, and symptoms may masquerade as those typical of pulmonary exacerbation. It is therefore important that CF clinicians have a high index of suspicion for patients returning from endemic areas.
Whilst not universally successful, approaches that utilise a 2–3 week course of parenteral ceftazidime, followed by a 3-month consolidation course of oral.
TMP/SMX, appear to be the most effective. This approach is similar to that recommended for melioidosis therapy [1, 2, 19]. If initial response does not successfully result in persistently negative sputum cultures for B. pseudomallei, then a longer course of parenteral ceftazidime or meropenem (≥4 weeks) should be considered [2]. If patients are allergic to or intolerant of TMP/SMX, consolidation with several months of doxycycline or amoxycillin/clavulanic acid have also been successfully used. When eradication is not possible, and a progressive decline in health ensues, lung transplantation may be considered. To date, early post-transplant outcomes have been acceptable despite persistence of B. pseudomallei.
This case series has several limitations. Firstly, it is likely other cases have not been identified, either because they have not been reported, or the infection was not recognised. For example, we excluded three possible cases from Mexico because of insufficient details [18]. Secondly, outcomes were not available for some patients, we were unable to access data (patients 5, 13 and 14), or cases lost to follow-up (patients 16 and 23). Interestingly, two patients were reported by two CF centres, by two UK-based centres, and by centres in the UK and Canada, respectively (patients 15 and 16). After further investigation we noted they were the same persons, highlighting the mobility of CF patients.
Conclusion
The international experience with B. pseudomallei described here demonstrates that this organism has the potential to exhibit novel behaviours in the CF host, including the development of chronic infection. Further analysis of B. pseudomallei isolates from those CF patients with persisting infection may inform on the key mechanisms contributing to bacterial persistence [7]. As a result of this analysis suggest the following recommendations:
-
1.
Clinicians should have a high index of suspicion for B. pseudomallei infection for CF patients living in or returning from areas where it is endemic. Suspicion should be heightened when fever and or pneumonia occurs. Close liaison with the CF microbiology laboratory is important.
-
2.
Eradication of B. pseudomallei infection should be attempted for CF patients when this pathogen is first isolated.
-
3.
Initial intravenous therapy should include a minimum of two weeks intravenous ceftazidime (and or meropenem if severe sepsis). Consideration should be given to extending the duration of intravenous in those CF patients who are persistently culture-positive on therapy. We also recommend addition of oral/intravenous TMP/SMX from the onset of therapy and this should continue where possible for three months, with regular clinical monitoring for potential adverse effects including renal and hepatic dysfuntion, bone marrow toxicity and potentially life-threatening skin reactions including DRESS syndrome (drug reaction with eosinophilia and systemic symptoms).
-
4.
Travel should be avoided to northern Australia or south-east Asia during the monsoonal season, with particular care to minimise exposure to wet season soils and rain in resident patients [20].
-
5.
Person-to-person transmission of B. pseudomallei is generally thought not to occur. However one case of siblings who developed infection with identical strains raises the possibility of cross-infection in CF and should carefully consider the risks and benefits of segregation of patients who have isolated this organism.
Abbreviations
- BMI:
-
Body mass index
- B. pseudomallei :
-
Burkholderia pseudomallei
- CF:
-
Cystic fibrosis
- CFTR:
-
Cystic Fibrosis Transmembrane Conductance Regulator
- FEV1:
-
Forced expiratory volume in 1 second
- TMP/SMX:
-
Trimethoprim/sulfamethoxazole
References
Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med. 2012;367(11):1035–44. doi:10.1056/NEJMra1204699.
Currie BJ. Melioidosis: evolving concepts in epidemiology, pathogenesis and treatment. Semin Respir Crit Care Med. 2015;36:111–25.
Currie BJ, Fisher DA, Howard DM, Burrow JN, Selvanayagam S, Snelling PL, et al. The epidemiology of melioidosis in Australia and Papua New Guinea. Acta Trop. 2000;74(2–3):121–7.
Meumann EM, Cheng AC, Ward L, Currie BJ. Clinical features and epidemiology of melioidosis pneumonia: results from a 21-year study and review of the literature. Clin Infect Dis. 2012;54(3):362–9. doi:10.1093/cid/cir808.
Sarovich DS, Ward L, Price EP, Mayo M, Pitman MC, Baird RW, et al. Recurrent melioidosis in the Darwin prospective melioidosis study: improving therapies mean that relapse cases are now rare. J Clin Microbiol. 2014;52(2):650–3. doi:10.1128/JCM.02239-13.
Currie BJ, Ward L, Cheng AC. The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS Negl Trop Dis. 2010;4(11):e900. doi:10.1371/journal.pntd.0000900.
Price EP, Sarovich DS, Mayo M, Tuanyok A, Drees KP, Kaestli M et al. Within-host evolution of Burkholderia pseudomallei over a twelve-year chronic carriage infection. MBio. 2013;4(4). doi:10.1128/mBio.00388-13.
Asiah K, Hanifah YA, Norzila MZ, Hasniah L, Rusanida A. Unrecognised infection in a cystic fibrosis patient. J Paediatr Child Health. 2006;42(4):217–8.
Barth AL, de Abreu E, Silva FA, Hoffmann A, Vieira MI, Zavascki AP, et al. Cystic fibrosis patient with Burkholderia pseudomallei infection acquired in Brazil. J Clin Microbiol. 2007;45(12):4077–80.
Corral DM, Coates AL, Yau YCW, Tellier R, Glass M, Jones SM, et al. Burkholderia pseudomallei infection in a cystic fibrosis patient from the Caribbean: a case report. Can Respir J. 2008;15(5):237–9.
Dance DA, Smith MD, Aucken HM, Pitt TL. Imported melioidosis in England and Wales. Lancet. 1999;353(9148):208.
O’Carroll MR, Kidd TJ, Coulter C, Smith HV, Rose BR, Harbour C, et al. Burkholderia pseudomallei: another emerging pathogen in cystic fibrosis. Thorax. 2003;58(12):1087–91.
O’Sullivan BP, Torres B, Conidi G, Smole S, Gauthier C, Stauffer KE, et al. Burkholderia pseudomallei infection in a child with cystic fibrosis: acquisition in the Western Hemisphere. Chest. 2011;140(1):239–42. doi:10.1378/chest.10-3336.
Schülin T, Steinmetz I. Chronic melioidosis in a patient with cystic fibrosis. J Clin Microbiol. 2001;39(4):1676–7.
Visca P, Cazzola G, Petrucca A, Braggion C. Travel-associated Burkholderia pseudomallei infection (Melioidosis) in a patient with cystic fibrosis: a case report. Clin Infect Dis. 2001;32(1):E15–6.
Holland DJ, Wesley A, Drinkovic D, Currie BJ. Cystic fibrosis and Burkholderia pseudomallei infection: an emerging problem? Clin Infect Dis. 2002;35(12):e138–40.
Radhakrishna N, Morton J. Burkholderia pseudomallei in cystic fibrosis and treatment complications. Respirol Case Rep. 2014. doi:10.1002/rcr2.86.
Lezana JL, Novoa O, Lezana MA. Epidemiology of Pseudomonas in Mexican CF patients [abstract]. Pediatric Pulmonolgy. 1989;4(Supplement):138.
Lipsitz R, Garges S, Aurigemma R, Baccam P, Blaney DD, Cheng AC, et al. Workshop on treatment of and postexposure prophylaxis for Burkholderia pseudomallei and B. mallei Infection, 2010. Emerg Infect Dis. 2012;18(12):e2. doi:10.3201/eid1812.120638.
Melioidosis. Centre for Disease Control, Darwin. 2012. http://health.nt.gov.au/library/scripts/objectifyMedia.aspx?file=pdf/43/46.pdf&siteID=1&str_title=Melioidosis.pdf. Accessed December 2 2014 2104.
Acknowledgments
There was no external funding body involved in the design of the study, data collection and analysis, or manuscript preparation. JBG was an employee of Queensland Health, Australia. DWR is an employee of Queensland Health and the recipient of a research fellowship with the Queensland Institute of Medical Research, Australia. BJC is employed by the Northern Territory Department of Health and Families and the Menzies School of Health Research, Australia. SCB is an employee of Queensland Health and the recipient of a research fellowship with the Queensland Institute of Medical Research, Australia.
Collaborators
Writing Committee Members for the MelioidCF Group.
Rowland Bright-Thomas, Manchester Adult Cystic Fibrosis Centre
University Hospital South Manchester1, University of Manchester Institute of Inflammation and Repair 2.
Jane Dewar, Wolfson Adult Cystic Fibrosis Unit, Nottingham University Hospitals NHS Trust, Nottingham, United Kingdom.
Steve Holden, Department of Clinical Microbiology, Nottingham University Hospitals NHS Trust, Nottingham, United Kingdom.
Nicholas Simmonds Department of Cystic Fibrosis Royal Brompton Hospital/Imperial College London, UK, SW3 6NP.
Khin Gyi, Department of Cystic Fibrosis, Royal Brompton Hospital and Imperial College, London SW3 6NP, United Kingdom.
Dervla Kenna, Antimicrobial Resistance and Healthcare Associated Infections Reference Unit, Public Health, England, London, United Kingdom.
Valerie Waters, Division of Infectious Diseases, Department of Pediatrics, Hospital for Sick Children, University of Toronto, Toronto.
Mary Jackson, Adult CF Clinic St Mary's Hospital, Kitchener, Ontario Canada.
Brian O’Sullivan, Professor of Pediatrics, CF Center Director, Director, Bioethics Core, UMass Medical School, 55 Lake Ave Worcester, MA 01655.
Giovanni Taccetti, Cystic Fibrosis Centre, Department of Paediatric Medicine, Anna Meyer Children’s University Hospital, Florence, Italy.
John Kolbe, Respiratory Services, Auckland City Hospital, New Zealand1, School of Medicine, Auckland City Hospital, New Zealand2.
Mark O’Carroll, Respiratory Services, Auckland City Hospital.
Catherine Byrnes Starship Children’s Health, ADHB, Auckland, New Zealand.
Dee Campbell, Clinical Nurse Specialist, Waikato Hospital, Private Bag 3200, Hamilton, New Zealand.
Mirjana Jaksic, Starship Children’s Health, ADHB, Auckland, New Zealand1, School of Medicine and Health Science, University of Auckland, New Zealand.
Naghmeh Radhakrishna, Allergy, Immunology and Respiratory Medicine, The Alfred Hospital, Melbourne, 3004.
Timothy J. Kidd, Centre for Infection and Immunity, Queen’s University, Belfast, Belfast, Northern Ireland, United Kingdom.
William Flight, Oxford Centre for Respiratory Medicine, Churchill Hospital, Oxford, United Kingdom.
Summary At A Glance: We confirmed that Burkholderia pseudomallei commonly behaves in novel ways in the CF host, frequently establishing chronic infection, which often results in poor long-term outcomes. Eradication should be attempted early where possible, but if unsuccessful, transplantation can be carefully considered despite chronic infection.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
All authors declare they have no competing interests.
Authors’ contributions
JBG participated in design of the study, collated clinical data, and drafted the manuscript. DWR participated in the design of the study and edited the manuscript. BJC participated in design of the study, provided clinical data on study subjects, and edited the final manuscript. SCB conceived the study, participated in design of the study, and edited the final manuscript. The Melioid CF Group provided clinical data on study subjects and edited the final manuscript. All authors read and approved the final manuscript.
Authors' information
Not applicable
Availability of data and materials
Not applicable
Additional files
Additional file 1:
online search strategy. (DOC 23 kb)
Additional file 2:
clinical data entry sheet. (DOC 77 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Geake, J.B., Reid, D.W., Currie, B.J. et al. An international, multicentre evaluation and description of Burkholderia pseudomallei infection in cystic fibrosis. BMC Pulm Med 15, 116 (2015). https://doi.org/10.1186/s12890-015-0109-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12890-015-0109-9