
Abstract
Background
Tuberculous meningitis (TBM) emerges as a grave complication of tuberculosis in people living with HIV (PLWH). The diagnosis and treatment of TBM pose significant challenges, leading to elevated mortality rates. To comprehensively grasp the epidemiological landscape of TBM in PLWH, a systematic review and meta-analysis were meticulously undertaken.
Methods
We performed a comprehensive search in PubMed, Embase, and Web of Science from database inception to September 19th, 2023, with no limitations on the publication type. The search terms were HIV/AIDS terms (AIDS OR HIV OR PLWH) and TBM-related terms (tuberculous meningitis OR TBM). Studies included in this meta-analysis evaluated the incidence of TBM among PLWH, or we were able to calculate the incidence of TBM among PLWH from the research.
Results
The analysis revealed that the prevalence of TBM among PLWH was 13.6% (95% CI: 6.6–25.9%), with an incidence rate of 1.5 cases per 1000 persons per year. The case fatality rate was found to be 38.1% (95% CI: 24.3–54.1%). No significant publication bias was observed. Meta-regression analysis identified the proportion of females and finance situation as factors influencing the outcomes.
Conclusions
Our study highlights TBM as a prevalent opportunistic infection that targets the central nervous system in PLWH. The elevated case fatality rate is especially prominent among PLWH in impoverished regions, underscores the pressing necessity for enhanced management strategies for PLWH suffering from TBM.
Trial registration
PROSPERO; No: CRD42022338586.
Similar content being viewed by others


Background
Tuberculous meningitis (TBM) is a common neurological disorder in young children and people living with HIV (PLWH), and it accounts for approximately 1% of all cases of tuberculous (TB) [1, 2]. Moreover, TBM is a fatal form of TB that kills or severely disables up to 50% of infected individuals [3,4,5]. In many regions around the world, especially in countries with TB epidemics, TB is the predominant cause of bacterial meningitis due to the protective effects of vaccination against other forms of meningitis. Moreover, the challenge of diagnosis and treatment delay is compounded by the lack of specific clinical features and the insensitivity of laboratory tests, ultimately contributing to its elevated mortality rate [6]. Critical risk factors for TBM, including age, anti-TB regimens, disease duration, and HIV infection, may contribute to the incidence and outcomes of TBM [7, 8].
PLWHs have an increased risk of developing all forms of TB [9], coinfection with TB influences the pathogenesis of HIV and increases HIV‑1 replication in PLWH [10]. In adults, HIV-1 coinfection is the most significant risk factor for TBM. Additionally, TBM has become a severe HIV-associated CNS opportunistic infection and has increased the relative risk of death from two- to three-fold in PLWH, even with the introduction of antiretroviral therapy (ART) [11]. In the context of HIV infection, the pathological, clinical, and laboratory findings in patients with TBM are influenced in various ways, and the outcomes of TBM may be poor [12]. Although previous studies have shown that TBM is linked to a significant risk of neurological complications and death [13,14,15], and Purmohamad et al. found a high incidence of TBM-HIV coinfection [16], there is currently a lack of systematic analysis of the incidence, prevalence, and mortality rates of TBM infection in adult PLWH.
In this study, we performed a systematic review and meta-analysis to understand the global prevalence, incidence and case fatality of PLWH with TBM. Additionally, we aimed to analyse the potential risks of death associated with TBM in PLWH, providing new insights into strategies for diagnosing and treating the disease.
Methods
This study is registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration No: CRD42022338586). Furthermore, this study was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [17]. The PRISMA checklist is provided in Supplement Table 1.
Search strategy
We performed a comprehensive search in PubMed, Embase, and Web of Science from database inception to September 19th, 2023, with no limitations on the publication type. To avoid bias due to language barriers, we only searched the articles written in English. The search terms were HIV/AIDS terms (AIDS OR HIV OR PLWH) and TBM-related terms (tuberculous meningitis OR TBM). We further screened the reference lists of the selected articles to identify missing studies. A detailed description of the search strategies is provided in Supplement Table 2.
Selection criteria
Studies included in this meta-analysis evaluated the incidence of TBM among PLWH, or provided data that allow for the calculation of the incidence of TBM among PLWH from the presented research. We excluded the following types of studies: (1) not related to HIV/AIDS; (2) research protocols or feedback reports; (3) case reports; (4) review articles; (5) children-oriented; (6) comparative study; (7) the prevalence or the incidence of TBM among PLWH could not be extracted; (8) participants less than 20. Researchers (XC and JW) removed duplicate studies using EndNote X9 software, selected preliminary search results through title and abstract, and then further determined the remaining articles by assessing full-text. Disagreements between reviewers about eligibility were resolved by discussion with TZ and YZ.
Data extraction
Two researchers (XC and JW) independently extracted and cross-checked relevant data using an Excel spreadsheet. The main information was the prevalence, incidence, and case fatality of TBM among PLWH. Additionally, we extracted other information from these articles, including authorship, year of publication, type of study, study location, sample size, mean age of participants, sex distribution, and current CD4+ T cell count from the total PLWH population and the TBM population.
Statistical analysis
Comprehensive Meta-Analysis (CMA) Version 3.0 (Biostat, Englewood, New Jersey) was adopted for quantitative analysis. Firstly, we calculated the combined event rate (ER) using the prevalence and death of TBM, and the total number of samples included. Next, the number of cases in the cohort articles was divided by the number of months of surveillance and then multiplied by 12 to calculate the number of cases per year [18]. Person-years were represented by the total number of HIV cases in each country during the study year, obtained from the UNAIDS website (https://www.unaids.org/en/regionscountries/countries). The rate was the number of cases per year multiplied by person per year. In addition, we conducted a random effects meta-analysis using the ER to estimate the prevalence and the case fatality of TBM among PLWH and used the rate to estimate the incidence of TBM among PLWH. Additionally, the Egger ranks correlation test was adopted to assess publication bias across studies. The I2 and Q-tests were used to evaluate the proportion and statistical significance of heterogeneity. The threshold for statistical significance was 2-tailed p < 0.05.
Quality assessment
Two researchers (XC and JW) used the Agency of Healthcare Research and Quality (AHRQ) methodology checklist (http://www.ncbi.nlm.nih.Gov/books/NBK35156/) for cross-sectional studies and independently assessed the individual studies. The checklist contained 11 items: (1) information source, (2) study criteria, (3) study period, (4) sampling, (5) interview method, (6) instrument validation, (7) exclusion criteria, (8) the measurement of confounding effects, (9) the process of dealing with missing values, (10) response rate, and (11) the use of follow-up assessment. According to this standard, studies were divided into three levels: high-quality (over 8 points), moderate-quality (4–7 points), and low-quality (0–3 points).
Meta regression
The primary outcome of our study was the prevalence and incidence of TBM among PLWH, and the secondary outcome was the case fatality of TBM among PLWH. The predefined continuous moderators were age, gender (the proportion of women), the current median/mean CD4+ T cell counts among PLWH and TBM, finance situation (Per capita gross domestic product (GDP) was obtained from the world bank website: https://data.worldbank.org.cn), and study quality. The categorical moderators were the study period, and the study design. Restricted ML meta-regression was used to evaluate associations. The results with p < 0.05 were considered as significance-level factors.
Results
Search results
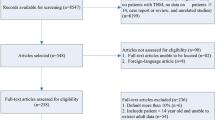
After removing all duplicates from the 1824 records, 1821 studies were screened. Of these, 1779 records were excluded based on the title and abstract, and 42 full-text articles were assessed for eligibility. Overall, 17 eligible studies were included in the meta-analysis. A flowchart of the study selection is shown in Fig. 1, and the details of the excluded articles are shown in Supplementary Table 3.

The flowchart of study selection
Study characteristics
Among the 17 studies included, 9 were retrospective, and 7 were prospective. The remaining studies were a combination of retrospective and prospective designs. In addition, 12 were cross-sectional studies, and five were cohort studies. Studies included data from Africa, Europe, Asia, and South America, comprising 6561 participants. Thirteen studies reported a mean age of 35 (range, 28–39) years; the mean female proportion was 36% (range, 14–68%). The current CD4+ T cell counts was 13–158 cells/µl in PLWH and 14–142 cells/µl in TBM. Six studies were considered moderate-quality studies, whereas the remaining were high-quality (Supplementary Table 4). Additional characteristics of the included studies and their corresponding participants are presented in Table 1.
Meta-analysis of prevalence, incidence and case fatality of TBM
Prevalence
Twelve studies reported the prevalence of TBM among PLWH. The combined ER of TBM was 13.6% (95% confidence interval [CI]: 6.6–25.9%). Significant heterogeneity was detected (Q: 520.4; I2: 97.9%; p < 0.001). Publication bias of the included studies had no statistical significance (intercept: -0.1, 95% CI: -114.4 to 14.3; p = 0.9) (Fig. 2).
Incidence
Five studies reported the incidence of TBM among PLWH. The combined rate of TBM was 1.5 per 1000 per year (95% CI: 0.6–2.5 per 1000 per year). Significant heterogeneity was detected (Q: 43.9; I2: 90.9%; p < 0.001). Publication bias of the included studies had no statistical significance (intercept: 5.6, 95% CI: -2.5 to 13.7; p = 0.1) (Fig. 3).
Case fatality
Twelve studies reported on the case fatality of patients with TBM. The combined ER was 38.1% (95% CI: 24.3–54.1%), and a significant heterogeneity was detected (Q: 69.1; I2: 84.1%; p < 0.001). No significant publication bias was found (intercept: -1.5, 95% CI: -5.8 to 2.8; p = 0.4). The detailed results of the meta-analysis are presented in Fig. 4.
Meta-regression
We conducted meta-regressions on all factors extracted from the studies to analyse the prevalence and case fatality among patients with TBM. While no significant results were found for prevalence, two factors produced substantial changes in outcomes: female proportion (coefficient: 0.05; p < 0.01) and finance situation (coefficient: -1.16; p = 0.02). The detailed results for the meta-regression are available in Supplementary Table 5.
Discussion
This comprehensive systematic review and meta-analysis was conducted to elucidate the prevalence incidence of TBM in PLWH and the corresponding case fatality in this population. We found that the prevalence, incidence and case fatality were approximately 13.6%, 1.5 per 1000 per year, and 38.1%, respectively, indicating that the prevalence and incidence of TBM were relatively low, while TBM-associated case fatality was high in PLWH. Moreover, the results of the meta-regression analysis suggested that the proportion of females and the finance situation may have substantial impacts on the outcomes.
PLWH are approximately 14 times more likely to develop TB, and face more than double the mortality rate during TB treatment compared to the general population [19]. PLWH are at heightened risk for TBM, particularly at more advanced stages of immunosuppression [20]. Moreover, TBM in PLWH has a poor prognosis, with no appreciable difference in survival probability based on ART timing [21]. Navarro-Flores et al. found that the prevalence of HIV was positively associated with the prevalence of TBM, identifying HIV infection as a moderator in the prevalence of TBM among hospitalized patients [13]. Moreover, a meta-analysis conducted by Stadelman et al. also suggested that the mortality of adult TBM was high and is influenced by HIV status [22]. Our study demonstrated that TMB-associated case fatality is high in PLWH, consistent with previous research on patients with TB [4].
Several risk factors influence the outcomes of CNS OIs in PLWH, including region distribution, age, sex, prophylactic history, and CD4+ T cell counts [23]. Our study analysed the related risk factors, including age, sex (the proportion of women), the current median/mean CD4+ T cell counts, and financial situation among PLWH and TBM. However, we did not find significant results for prevalence.
In addition, we found a marginal correlation effect (coefficient: -1.16; p = 0.02) between case fatality and socioeconomic status, indirectly indicating the region’s impact on case fatality. The changes in outcomes influenced by regional distribution are consistent with previous studies on TB/HIV coinfection, which showed that high morbidity and mortality rates were observed among PLWH and TB in resource-limited countries such as those in sub-Saharan Africa [24].
In our study, another factor influencing case fatality was the proportion of females, which suggests that as the proportion of females increases, so does the case fatality rate. The worldwide incidence of TB has consistently been higher in men compared with women, although the male-to-female ratio varies per region [25]. However, HIV infection significantly contributed to the epidemic rates of TB in women, leading to a 5.3-fold increase, which was notably higher compared to men. Since there are only a few studies on sex in patients with TBM, we speculate that our findings could be attributed to the increased rates of TBM in women with the onset of HIV and more susceptibility to HIV.
In certain cohorts, the mortality rate among HIV patients coinfected with TBM exceeds 50% [26]. Important contributing factors include the level of immunosuppression due to HIV and immune reconstitution inflammatory syndrome (IRIS) resulting from ART [27, 28]. In our study, we used CD4+ T cell counts to measure the degree of immunosuppression in PLWH and found that the current CD4+ T cell counts ranged from 13 to 96 cells/µl among PLWH and 12–142 cells/µl among PLWH with TBM, suggesting that these populations are severely immunocompromised. The CD4+ T cell counts may be associated with the case fatality of PLWH and TBM in our study. However, our study did not mention other potential risk factors among PLWH and TBM, such as drug-resistant TB, specific anti-TB regimens, disease duration, and the presence of accompanying pulmonary TB or other systemic TB, which could also be critical in determining the case fatality rate.
This study had several limitations. First, the number of included studies was limited, which restricted the generalizability of the results. Second, PLWH with TBM typically experience severe immunosuppression, characterized by significantly low CD4+ T cell counts. Therefore, it may affect the generalization of our findings to all PLWH. Third, the incomplete and discrepant data in the original articles, coupled with a dearth of detailed information from individual studies, resulted in inadequate subgroup analyses. For example, age and CD4+ T cell counts showed no remarkable difference in the prevalence and case fatality. This lack of significance could be attributed to several factors: (1) in all studies, the mean age was approximately 30 years, which is consistent with the peak age at onset of TB; and (2) since the population in our study was PLWH and TBM, the CD4+ T cell counts in each study were relatively low, with the highest not exceeding 150 cells/µl, leading to low statistical power in this subgroup analysis. In addition, the regional distribution is limited owing to few relevant studies. Thus, our findings of regional differences do not reflect the global distribution and lack validity and generalizability. For example, the outcomes of the regional distribution in the population suggested that Europe has the most significant number of studies, the prevalence of TBM in PLWH is generally high (up to 13%), and the prevalence in Africa and South America is nearly 10%. In contrast, the prevalence in Asia is as high as 55.3% (Supplement Fig. 1); the case fatality in Africa was the highest (up to 60%); this disparity may be linked to limited access to treatment, poverty, gender inequality, and societal stigma towards HIV in Africa [29, 30]. When compared to other regions, this situation is more widespread in Africa [31, 32] (Supplement Fig. 2). Fourth, the heterogeneity in this meta-analysis was high (Q: 72.081; I²: 81.97%; p < 0.001), likely due to significant differences in study design, including variations in sample sizes, methodologies, and population characteristics. This heterogeneity may contribute to limited generalizability and potential biases in our study.

Meta-analysis of prevalence of TBM among PLWH

Meta-analysis of incidence of TBM among PLWH

Meta-analysis of case fatality of TBM among PLWH
Conclusions
In conclusion, this systematic review and meta-analysis provided a comprehensive epidemiological landscape of TBM in PLWH exhibiting low prevalence and incidence rates alongside high case fatality rates, particularly those from economically disadvantaged areas. Additionally, meta-regressions were performed to investigate the pertinent risk factors influencing TBM prevalence and case fatality rates among PLWH. Notably, the financial situation and the proportion of females were identified as significant factors influencing these outcomes. This study underscores the critical necessity for immediate public health interventions to enhance patient care for individuals affected by PLWH and TBM.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- TBM:
-
Tuberculous meningitis
- TB:
-
Tuberculous
- PLWH:
-
People living with HIV
- CNS:
-
Central nervous system
- OIs:
-
Opportunistic infections
- ART:
-
Antiretroviral therapy
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- CMA:
-
Comprehensive Meta-Analysis
- ER:
-
Event rate
- AHRQ:
-
Agency of Healthcare Research and Quality
- GDP:
-
Gross domestic product
- PML:
-
Progressive multifocal leukoencephalopathy
- IRIS:
-
Immune reconstitution inflammatory syndrome
References
Jain S, Tobin D, Tucker E, Venketaraman V, Ordonez A, Jayashankar L, Siddiqi O, Hammoud D, Prasadarao N, Sandor M, et al. Tuberculous meningitis: a roadmap for advancing basic and translational research. Nat Immunol. 2018;19(6):521–5.
Marais S, Thwaites G, Schoeman J, Török M, Misra U, Prasad K, Donald P, Wilkinson R, Marais B. Tuberculous meningitis: a uniform case definition for use in clinical research. Lancet Infect Dis. 2010;10(11):803–12.
Wilkinson R, Rohlwink U, Misra U, van Crevel R, Mai N, Dooley K, Caws M, Figaji A, Savic R, Solomons R, et al. Tuberculous meningitis. Nat Reviews Neurol. 2017;13(10):581–98.
Graham S, Donald P. Death and disability: the outcomes of tuberculous meningitis. Lancet Infect Dis. 2014;14(10):902–4.
Dian S, Rahmadi R, van Laarhoven A, Ganiem A, van Crevel R. Predicting Mortality of Tuberculous Meningitis. Clin Infect Diseases: Official Publication Infect Dis Soc Am. 2018;67(12):1954–5.
Thwaites G, van Toorn R, Schoeman J. Tuberculous meningitis: more questions, still too few answers. Lancet Neurol. 2013;12(10):999–1010.
Huynh J, Donovan J, Phu N, Nghia H, Thuong N, Thwaites G. Tuberculous meningitis: progress and remaining questions. Lancet Neurol. 2022;21(5):450–64.
Tenforde M, Mokomane M, Leeme T, Tlhako N, Tsholo K, Chebani T, Stephenson A, Hutton J, Mitchell H, Patel R, et al. Mortality in adult patients with culture-positive and culture-negative meningitis in the Botswana national meningitis survey: a prevalent cohort study. Lancet Infect Dis. 2019;19(7):740–9.
Berenguer J, Moreno S, Laguna F, Vicente T, Adrados M, Ortega A, González-LaHoz J, Bouza E. Tuberculous meningitis in patients infected with the human immunodeficiency virus. N Engl J Med. 1992;326(10):668–72.
Bell L, Noursadeghi M. Pathogenesis of HIV-1 and Mycobacterium tuberculosis co-infection. Nat Rev Microbiol. 2018;16(2):80–90.
Heemskerk A, Bang N, Mai N, Chau T, Phu N, Loc P, Chau N, Hien T, Dung N, Lan N, et al. Intensified antituberculosis therapy in adults with tuberculous meningitis. N Engl J Med. 2016;374(2):124–34.
Garg R, Sinha M. Tuberculous meningitis in patients infected with human immunodeficiency virus. J Neurol. 2011;258(1):3–13.
Navarro-Flores A, Fernandez-Chinguel JE, Pacheco-Barrios N, Soriano-Moreno DR, Pacheco-Barrios K. Global morbidity and mortality of central nervous system tuberculosis: a systematic review and meta-analysis. J Neurol. 2022;269(7):3482–94.
Nataprawira HM, Gafar F, Risan NA, Wulandari DA, Sudarwati S, Marais BJ, Stevens J, Alffenaar J-WC, Ruslami R. Treatment outcomes of Childhood Tuberculous meningitis in a real-world retrospective cohort, Bandung, Indonesia. Emerg Infect Dis. 2022;28(3):660–71.
Merkler AE, Reynolds AS, Gialdini G, Morris NA, Murthy SB, Thakur K, Kamel H. Neurological complications after tuberculous meningitis in a multi-state cohort in the United States. J Neurol Sci. 2017;375:460–3.
Purmohamad A, Azimi T, Nasiri MJ, Goudarzi M, Zangiabadian M, Sedighian H, Fooladi AAI. HIV-Tuberculous meningitis Co-infection: a systematic review and Meta-analysis. Curr Pharm Biotechnol. 2021;22(7):960–8.
Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Shrestha DB, Budhathoki P, Gurung B, Subedi S, Aryal S, Basukala A, Aryal B, Adhikari A, Poudel A, Yadav GK et al. Epidemiology of dengue in SAARC territory: a systematic review and meta-analysis. Parasite Vector 2022, 15(1).
WHO. Global tuberculosis report 2023. 2023.
Vinnard C, Macgregor RR. Tuberculous meningitis in HIV-infected individuals. Curr HIV/AIDS Rep. 2009;6(3):139–45.
Lawn S, Wood R. Poor prognosis of HIV-associated tuberculous meningitis regardless of the timing of antiretroviral therapy. Clin Infect Diseases: Official Publication Infect Dis Soc Am. 2011;52(11):1384–7.
Stadelman AM, Ellis J, Samuels THA, Mutengesa E, Dobbin J, Ssebambulidde K, Rutakingirwa MK, Tugume L, Boulware DR, Grint D, et al. Treatment outcomes in adult tuberculous meningitis: a systematic review and Meta-analysis. Open Forum Infect Dis. 2020;7(8):ofaa257.
Agnihotri S. Central Nervous System opportunistic infections. Semin Neurol. 2019;39(3):383–90.
Osman M, Welte A, Dunbar R, Brown R, Hoddinott G, Hesseling A, Marx F. Morbidity and mortality up to 5 years post tuberculosis treatment in South Africa: a pilot study. Int J Infect Diseases: IJID : Official Publication Int Soc Infect Dis. 2019;85:57–63.
WHO. Global tuberculosis report. 2021.
Thao LTP, Heemskerk AD, Geskus RB, Mai NTH, Ha DTM, Chau TTH, Phu NH, Chau NVV, Caws M, Lan NH, et al. Prognostic models for 9-Month Mortality in Tuberculous Meningitis. Clin Infect Diseases: Official Publication Infect Dis Soc Am. 2018;66(4):523–32.
Marais S, Lai RPJ, Wilkinson KA, Meintjes G, O’Garra A, Wilkinson RJ. Inflammasome Activation Underlying Central Nervous System Deterioration in HIV-Associated Tuberculosis. J Infect Dis. 2017;215(5):677–86.
Thwaites GE, N DB, N HD, H TQ, D TTO, N TCT, N QH, N TT, N NH, N TNL, et al. The influence of HIV infection on clinical presentation, response to treatment, and outcome in adults with tuberculous meningitis. J Infect Dis. 2005;192(12):2134–41.
Harrison A, Colvin CJ, Kuo C, Swartz A, Lurie M. Sustained high HIV incidence in Young Women in Southern Africa: social, behavioral, and structural factors and emerging intervention approaches. Curr HIV/AIDS Rep. 2015;12(2):207–15.
Delva W, Abdool Karim Q. The HIV epidemic in Southern Africa - is an AIDS-free generation possible? Curr HIV/AIDS Rep 2014, 11(2).
Shah G, Ewetola R, Etheredge G, Maluantesa L, Waterfield K, Engetele E, Kilundu A. Risk factors for TB/HIV coinfection and consequences for patient outcomes: evidence from 241 clinics in the Democratic Republic of Congo. Int J Environ Res Public Health 2021, 18(10).
Dong K, Thabethe Z, Hurtado R, Sibaya T, Dlwati H, Walker B, Wilson D. Challenges to the success of HIV and Tuberculosis care and treatment in the public health sector in South Africa. J Infect Dis 2007:S491–496.
Acknowledgements
Not applicable.
Funding
This research was funded by the Beijing Natural Science Foundation (Z220018, 7222095); the Capital’s Funds for Health Improvement and Research (2022-1-1151), the National Key R&D Program of China (2023YFE0116000, 2023YFC2308300), the National Natural Science Foundation of China (81571178, 81873761, 82072271); the Climbing the Peak (Deng feng) Talent Training Program of the Beijing Hospitals Authority (DFL20191701); the Beijing Health Technologies Promotion Program (BHTPP2020); and the Beijing Key Laboratory for HIV/AIDS Research (BZ0089); Beijing research center for respiratory infectious diseases project (BJRID2024-001).
Author information
Authors and Affiliations
Contributions
Conceptualization: XC, JW; methodology and software; analysis: JW and MZ; writing—original draft preparation: XC, JW; writing—review and editing: XC, MR, BS and MC; supervision and funding acquisition: YZ, TZ. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chen, X., Wei, J., Zhang, M. et al. Prevalence, incidence, and case fatality of tuberculous meningitis in adults living with HIV: a systematic review and meta-analysis. BMC Public Health 24, 2145 (2024). https://doi.org/10.1186/s12889-024-19683-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19683-4