
Abstract
Background
Temperature fluctuations can impact the occurrence and progression of respiratory system diseases. However, the current understanding of the impact of temperature on acute exacerbation of chronic obstructive pulmonary disease (AECOPD) remains limited. Therefore, our study aims to investigate the relationship between daily mean temperature (DMT) and the risk of AECOPD hospitalizations within Panzhihua City.
Methods
We systematically collected data on AECOPD hospitalizations at Panzhihua Central Hospital from 2015 to 2020 and meteorological factors across Panzhihua City’s districts. A two-stage analysis method was used to establish a distributed lag non-linear model to elucidate the influence of DMT on the frequency of admissions for AECOPD. Subgroup analyses were conducted by gender and age to identify populations potentially susceptible to the impact of DMT.
Results
A total of 5299 AECOPD hospitalizations cases were included. The DMT and the risk of AECOPD hospitalization showed a non-linear exposure–response pattern, with low temperatures exacerbating the risk of hospitalizations. The lag effects of low temperature and relatively low temperature peaked at 2th day, with the lag effects disappearing at 16–17 days. Females and elders aged ≥ 65 years were more sensitive to effects of low and relatively low temperature at lag 0–4 days, while male AECOPD patients exhibited longer lasting lag effects.
Conclusions
Low temperatures are associated with an increased risk of AECOPD hospitalizations. Females or elders aged ≥ 65 years with chronic obstructive pulmonary disease should pay more attention to taking protective measures in cold environments. These findings are crucial for the formulation of public health policies, as they will help significantly alleviate the burden of AECOPD and improve respiratory health in the face of climate challenges.
Similar content being viewed by others

Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most common chronic respiratory disease, significantly influenced by environmental factors, and currently lacks an effective cure [1]. According to the Global Burden of Disease Study (2019), approximately 250 million people worldwide suffer from COPD [2], making it the third leading cause of death globally with 3.23 million deaths reported in 2019. Notably, nearly 90% of these deaths occur in low- and middle-income countries among individuals under the age of 70 [3]. A cross-sectional study conducted in China estimated a COPD prevalence rate of 8.6% (n = 50,991) among adults aged ≥ 20 years, and around 99.9 million individuals affected [4]. COPD poses a significant public health challenge, significantly impacting global health and imposing considerable economic strains. Smoking, obesity, malnutrition, and comorbidities have been identified as precipitants of COPD [5]. Furthermore, exposure to certain environmental factors, such as climate change, occupational exposure, and air pollution, also contribute to the development of COPD [6]. The acute exacerbation of COPD (AECOPD), characterized by an abrupt intensification of symptoms, is frequently linked to these risk factors. It serves as a principal reason for hospital admissions, escalates the likelihood of medical complications and mortality, and consequently incurs substantial healthcare expenditures [7]. In the United States, more than $3.2 billion is spent annually on COPD management [8], with AECOPD accounting for 50–75% of these expenditures [9].
In recent years, global climate change has emerged as a significant environmental public health challenge, characterized by the occurrence of global warming and frequent extreme weather events. The fluctuations in temperature and humidity, coupled an increase in extreme weather events, have been proven to affect the prevalence and severity of respiratory diseases [10]. Tran et al. emphasized the critical importance of adapting to and mitigating climate change to reduce COPD mortality rates, particularly in regions experiencing significant fluctuations in temperature and humidity [1]. Lin et al. investigated the relationship between meteorological factors and AECOPD in Changhua (Taiwan, China), revealing a positive correlation between elevated temperature and reduced atmospheric pressure with occurrences of AECOPD during warming-up seasons. Conversely, they observed a positive correlation between decreased temperature and PM10 concentration with AECOPD during cooling-down seasons [11]. Notably, there is limited research on the impact of climate change factors like temperature on AECOPD. Existing studies exhibit considerable variations across different geographical regions and populations. Therefore, further research is necessary to provide more specific and practical information for devising accurate prevention and management strategies.
Numerous studies have demonstrated that the relationship between temperature and incidence of diseases is not linear and may involve lagged effects [12, 13]. The Distributed Lag Non-Linear Model (DLNM) is a statistical tool specifically designed to investigate and quantify the delayed and non-linear relationships of variables over time. It enables the identification of both short-term and long-term impacts of environmental factors on human health, making it widely utilized [14, 15]. Hence, our study aims to assess the lag effects of temperature on hospital admissions for AECOPD in Panzhihua City, China, using the DLNM and multivariate meta-regression analysis. Our research provides a comprehensive analysis of the influence of daily mean temperatures (DMT) on AECOPD hospitalization rates in Panzhihua, China. Our study provides evidence that temperature changes are associated with COPD exacerbations, filling a significant gap that has been largely ignored in previous studies. It aims to provide a scientific basis for the development of comprehensive prevention and control strategies and measures for AECOPD.
Materials and methods
Data resources
The hospitalization data of 5299 AECOPD cases between January 2015 and December 2020 were obtained from the case database of Panzhihua Central Hospital. These patients resided in Panzhihua, Renhe District, Miyi County, and Yanbian County. Key data collected included admission dates, disease diagnoses, gender, age, and place of residence. The study included both initial and recurring AECOPD cases, adhering to established standards for COPD diagnosis and treatment. Exclusion criteria were applied to patients diagnosed with asthma or other known respiratory diseases, as well as those with uncontrolled severe inflammation or complications in other systems. This study was conducted in compliance with the latest revision of the Declaration of Helsinki.
The meteorological data for this study were obtained from the Panzhihua, Renhe, Yanbian, and Miyi meteorological stations (Fig. 1). The primary data included DMT, daily average relative humidity, and daily average air pressure for the four districts and counties of Panzhihua City, spanning from January 2015 to December 2020.

The location of meteorological factor monitoring stations in the study. Notes: Miyi (26°9166'N latitude and 102°1166'E longitude), Yanbian (26°6833'N latitude and 101°85'E longitude), Panzhihua (26°5833'N latitude and 101°7166'E longitude), Renhe (26°4975'N latitude and 101°7573'E longitude). Drawing using ArcGIS10.2
Research methods
Descriptive analysis of meteorological factors
In this study, meteorological factors were characterized by their minimum value (Min), 10th percentile (P10), 15th percentile (P15), 50th percentile (P50), 90th percentile (P90), 95th percentile (P95), and maximum value (Max). These percentiles were used to describe the distribution of meteorological factors. Furthermore, Spearman rank correlation analysis was conducted to examine the correlations among the meteorological factors.
Two-stage analysis method to examine the impact of DMT on AECOPD hospitalization
DLNM can flexibly characterize the relationship between exposures (such as temperature, air pollutants, etc.) and health outcomes over time [16]. The adoption of a two-stage analysis method can effectively improve the stability and reliability of effect estimates in regions with small samples, thereby enhancing the model’s adaptability [17, 18]. Given the absence of reports on the relationship between DMT and the risk of hospitalization for AECOPD patients in Panzhihua City, this study employed a two-stage analysis based on DLNM to investigate the impact of DMT on AECOPD hospitalizations across the district and counties of Panzhihua City.
In the first stage, we used the R package “dlnm” to build DLNM for each district and county. DLNM can flexibly describe the nonlinear and delayed effect relationship of exposure–response in time series data [19]. The quasi-Poisson function was employed as the link function to fit the exposure–response relationship between the DMT and the hospitalization count for AECOPD. To account for the confounding effects of other meteorological factors such as relative humidity and atmospheric pressure, natural cubic spline functions of daily average relative humidity and atmospheric pressure were included in the model. To eliminate the influence of long-term patterns on short-term associations, a cubic spline function of time was incorporated into the model. Additionally, the model considered the day of the week effects and holiday effects. The final expression is as follows:
Here, E(Yt) is the expected value of daily hospitalization count for AECOPD exacerbations on day t, α is the intercept, Tempt, l represents the cross-basis of DMT and lagged time, β is the coefficient for Tempt, l, NS denotes the natural cubic spline function, df represents degrees of freedom, pre is daily average atmospheric pressure, rh is daily average relative humidity, time is the time variable, DOW accounts for day of the week effects, and holiday represents holiday effects. Based on previous research indicating temperature lag effects, the longest lag time selected was 21 days [20]. According to the quasi-likelihood for Akaike’s information criterion (Q-AIC) and prior research results, the degrees of freedom for daily average atmospheric pressure and relative humidity were set to 3, and the annual degrees of freedom for the time trend variable were set to 7 [21].
In the second stage, the R package “mvmeta” was employed to combine the DLNM results from four districts obtained in the first stage, in order to derive the overall exposure–response relationship for Panzhihua City. The R package “mvmeta” performs random-effect meta-analysis, which can effectively handle heterogeneity by allowing for variation in effect sizes between studies and incorporating this variation into the model [22, 23]. Given the heterogeneity in population size and effect magnitude among the study regions, the Best Linear Unbiased Prediction (BLUP) analysis from the mvmeta algorithm was introduced to fit the meta-analysis results. BLUP provides the best effect estimate by weighing the overall fixed effect and the regional observed effect. When there are fewer regional research data, the total variability increases, making the estimate of the region more dependent on the overall average estimate [22, 24]. This approach results in a more reliable exposure–response relationship between DMT and AECOPD risk for Panzhihua City as a whole [25].
Lagged effects analysis of AECOPD hospitalization risk at different temperatures
The relative risk (RR) refers to the ratio of the risk of hospitalization for AECOPD caused by exposure to a given temperature to the risk at the minimum risk temperature [25]. The R package “dlnm” transforms the linear predictors (log[E(Yt)]) for each temperature and lag day into risk values using an exponential function. After determining the minimum risk value, RR represents the ratio of the risk value at each temperature and lag day to the lowest risk value. In this study, we observed that the risk of hospitalization for AECOPD was minimized at an DMT of 31.7°C. Using 31.7°C as the reference, the RR at each temperature was calculated and the exposure–response curve was drawn. The RR of hospitalization for AECOPD was calculated for exposure to low temperature (P5), relatively low temperature (P10), relatively high temperature (P90), and high temperature (P95) with a lag time ranging from 0 to 21 days. Lag-effect curves were plotted to elucidate the impact of high and low temperature on the risk of AECOPD hospitalizations. Finally, stratified analyses were conducted based on gender and age (< 65 years and ≥ 65 years) to identify populations more sensitive to DMT. The study employed a two-sided test with a significance level of 0.05.
Model robustness assessment
After adjusting the degrees of freedom for the time variable, the exposure–response curves of DMT and the risk of AECOPD admissions were drawn. The robustness of the model was evaluated based on the consistency of its trends.
Results
Basic characteristics of AECOPD patients
A total of 5,299 hospitalized AECOPD patients from four districts/counties in Panzhihua from 2015 to 2020 were included. Upon analyzing the baseline information of these patients, their ages ranged from 30 and 101 years. Specifically, 12.21% (647) of the patients aged < 65 years, while 87.79% (4,652) were aged ≥ 65 years. Additionally, 75.77% (4,015) of the patients were male, and 24.23% (1,284) were female (Table 1). Among the four regions, Panzhihua had the largest number of hospital admissions, accounting for 55.56% (2,944) of total admissions, while Miyi County and Yanbian County had fewer AECOPD admissions (Table 1). The daily hospitalization information across the four regions revealed that the daily hospitalization count ranged from 0 to 10 individuals (Supplementary Table 1). Furthermore, the distribution of AECOPD patients’ hospitalization time showed that the number of hospitalizations was higher in January and December and lower from April to September each year. A rising trend in hospitalizations was observed starting from September (Fig. 2). These findings suggest that AECOPD is more prevalent in winter and less prevalent in summer in Panzhihua.

Trend of monthly hospitalization number of patients with AECOPD in Panzhihua City
Analysis of meteorological factors in Panzhihua City from 2015 to 2020
Panzhihua City, situated in the southern region of Sichuan Province, China, is located at approximately 26°23'N latitude and 101°43'E longitude. The city exhibits a subtropical monsoon climate characterized by concentrated summer precipitation and relatively arid winters. It maintains a consistently warm temperature throughout the year, featuring brief, scorching summers and mild winters. The median DMT in Panzhihua City is 21.9℃ (range: 4.2–34.2℃), while the median daily average atmospheric pressure stands at 880.3 hPa (range: 857.8–902.6 hPa). Additionally, the median daily average relative humidity is 62% (range: 12%-100%) (Table 2). Spearman correlation analysis was conducted to examine the interplay between these meteorological factors, revealing significant negative correlation between DMT and both daily mean atmospheric pressure as well as daily mean relative humidity (Fig. 3). Considering that lower relative humidity and higher atmospheric pressure are associated with an increased risk of AECOPD [26], both variables were considered as confounding factors for subsequent analysis on the impact of DMT on AECOPD hospitalizations.

Spearman correlation among meteorological factors. Notes: DMT represents daily mean temperature, DMAP represents daily mean atmospheric pressure, DMRH represents daily mean relative humidity; blue indicates a positive correlation, red indicates a negative correlation, and *** represents P < 0.001
The impact of DMT on AECOPD hospitalizations
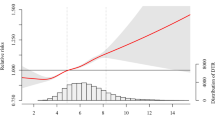
To investigate the association between DMT and AECOPD hospitalizations, we constructed an exposure–response curve to examine the relationship between DMT and the risk of AECOPD hospitalization. We found that the risk of AECOPD hospitalization was lowest when the DMT was 31.7°C. Therefore, 31.7°C was used as the reference point for calculating RR values in subsequent analyses. Our analysis revealed a nonlinear association between lower temperatures and increased risk of AECOPD hospitalization (Fig. 4). Notably, DMT above 21.7°C did not significantly impact AECOPD hospitalization risk. However, below this threshold temperature, significant differences in RR values were observed. The highest RR value was recorded at a temperature of 4.2°C, reaching 15.008 (95% CI: 7.179 ~ 31.377) (Fig. 4).

Exposure–response relationship between DMT and relative risk of AECOPD hospitalization in Panzhihua City based on BLUP adjustment. Notes: The gray dashed lines represent the exposure–response curves adjusted with BLUP corresponding to the four districts/counties in Panzhihua City. The red solid line represents the overall exposure–response curve of Panzhihua City after conducting multiple meta-regression analysis and applying BLUP adjustment. The gray shaded area indicates the 95% confidence interval
Lagged effects of DMT on AECOPD hospitalizations
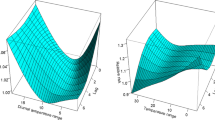
To investigate the lagged effects of DMT on the risk of hospitalization for AECOPD, we constructed a three-dimensional graph illustrating the relationship between RR and lag days, as well as variations in DMT. The findings revealed that exposure to low temperatures was associated with an increased short-term risk of hospitalization for AECOPD, reaching its peak within 0–5 days before gradually declining. Although exposure to high temperatures had a relatively smaller impact on the risk of hospitalization for AECOPD, it also exhibited a transient lagged effect (Fig. 5). Consequently, this study further analyzed the lagged effects of both low and high temperatures on the risk of hospitalization for AECOPD.

Three-dimensional graph of the risk distribution for AECOPD hospitalizations across different lag periods and DMT
Lag-response curves (Fig. 6) were employed to investigate the delayed effects of various temperature levels, including low (12.1°C), relatively low (13.3°C), relatively high (27.8°C), and high (29.5°C), on the AECOPD hospitalizations. The findings revealed that both low temperature and relatively low temperature exhibited prolonged lagged effects on AECOPD. Following exposure to low temperature, a significant and maximum RR was observed at 2th day lag period (RR = 1.101, 95% CI: 1.009 ~ 1.202). Subsequently, the RR gradually declined and disappeared entirely by the 17th day. Similarly, the impact of relatively low temperature on AECOPD hospitalizations persisted for an extended duration. with a significant RR observed at a lag 2th day following exposure to this condition (RR = 1.098, 95% CI: 1.011 ~ 1.193), disappearing by the 16th day in its entirety. However, no significant delayed effects were observed for either relatively high temperature or high temperature on the AECOPD hospitalizations (Table 3).

Lag-response curves for the impact of different DMT on AECOPD hospitalizations. Notes: Dashed lines indicate the 95% confidence interval
The impact of DMT on AECOPD hospitalizations based on gender stratified analysis
The gender-stratified revealed that both low and relatively low temperature had significant impact on AECOPD hospitalizations in both sexes. In the female population, the RR values for low and relatively low temperature reached their maximum at lag 3–4 days, surpassing those observed in males. This suggested that females faced a higher risk of AECOPD hospitalization within 0–4 days when exposure to low and relatively low temperature. In contrast, the effect of low and relatively low temperature on male AECOPD patients persisted for a longer duration, becoming significant effects from a lag at 4th day, reaching a peak at 3th day, and persisting until 16th day. No significant effects of relatively high temperature and high temperature on AECOPD hospitalizations were observed in both groups (Table 4).
The impact of DMT on AECOPD hospitalizations in different age groups
The age-stratified revealed that both low and relatively low temperature had a significant impact on AECOPD hospitalization in individuals aged ≥ 65 years. Conversely, in the age group < 65 years, temperature did not have a significant effect on the risk of AECOPD hospitalization. When compared to the temperature associated with the lowest risk, low temperature at lag of 2th day exhibited the RR for AECOPD hospitalization in individuals aged ≥ 65 years, reaching 1.128 (95% CI: 1.025–1.242). Subsequently, this Lag effect gradually diminished and became insignificant by 17–21 days. In individuals aged ≥ 65 years, the Lag effect of relatively low temperature on AECOPD hospitalization was similar to that of low temperature, albeit with RR values were relatively lower than the impact of low temperature. No significant effects of relatively high temperature on AECOPD exacerbation hospitalizations were observed across different age groups (Table 5). Interestingly, high temperature showed a slight protective effect in people aged > 65 years.
Sensitivity analysis
To evaluate the robustness of the model, we adjusted the time series degrees of freedom ranging from 6 to 9, to control the temporal trends (Fig. 7). It indicated that, under different degrees of freedom, the relationship between temperature and the RR of AECOPD hospitalizations exhibited similar trends. This suggested the reliability of the model.

Exposure–response curves of temperature and AECOPD hospitalizations under different degrees of freedom. Notes: The gray area represents the 95% confidence interval
Discussion
This study is the first comprehensive investigation and analysis of the relationship between DMT and AECOPD hospitalization in Panzhihua, a city in southwestern China. There was a non-linear exposure–response relationship between DMT and AECOPD hospitalization, and low DMT significantly increased the risk of AECOPD hospitalization. Furthermore, we elucidated the lag effects of low DMT, revealing that the Lag effect of low DMT was limited to 2–17 lag days after exposure. Notably, the extent of the lag effect of low temperature varied greatly depending on gender and age.
The proportion of male AECOPD hospitalizations was significantly higher than that of females. This disparity can largely be attributed to a markedly higher prevalence of smoking among males. Analysis by Liu et al. of the nationally representative 2018 China Health Literacy Survey revealed a significantly higher smoking rate among males than females in the population aged 20–69 (47.6% vs. 1.9%) [27]. Considering that smoking is a primary cause of COPD [28], this may be one of the reasons for the differences in AECOPD hospitalizations in different gender subgroups. Additionally, there was a significant increase in the number of AECOPD hospitalized AECOPD patients aged ≥ 65 years compared to those ≤ 65 years. Which can be attributed to age-related decline in physical function exacerbating their conditions and necessitating hospitalization.
To date, several studies have suggested a correlation between temperature and the incidence and mortality of COPD [6, 29]. However, limited epidemiological research has specifically focused on the association between DMT and AECOPD. A significant finding of our study was the identification of a non-linear relationship between DMT and hospital admissions for AECOPD. We observed that low DMT increasing the risk of AECOPD hospitalization, with no effect observed when DMT exceeded 21.7℃. Interestingly, our results were inconsistent with previous studies conducted in Taiwan, China [11], which reported an elevated risk of AECOPD with both increasing and decreasing temperature. Several mechanisms have been proposed to explain the increase in pulmonary diseases during colder temperature. Firstly, low temperature increased the risk of respiratory infections [30]. Secondly, cold conditions exacerbated airway inflammation, a pivotal factor in the genesis and progression of COPD [31, 32]. Additionally, cold air can induce bronchoconstriction leading to breathing difficulties and worsening condition, thereby increasing the risk of hospitalization and mortality [33]. Nevertheless, it is important to note that the impact of temperature on COPD varies significantly across different regions [11, 34,35,36].
A study in Hangzhou, China, revealed a non-linear association between temperature and COPD mortality, characterized by an inverse J-shaped pattern. both extreme low and high temperature increased the risk of COPD deaths, with the impact of low temperature being greater than that of high temperature [34]. Similarly, two studies in the United States also found that during hot summers, an increase in temperature was associated with a rise in hospital admissions for COPD and increased mortality rates among elderly COPD patients [37, 38]. The specific mechanisms underlying the heightened risks of COPD due to high temperature remain unclear. One possible explanation is that high temperature may increase the concentration of air pollutants, such as particulate matter, nitrogen oxides, sulfur oxides, and ozone precursors. The synergistic effect between high temperature and air pollution could potentially increase the risk of respiratory diseases [39]. Moreover, certain pathogens including viruses and bacteria may thrive more effectively in high-temperature environments leading to the development or exacerbating respiratory diseases [40].
However, we observed that high temperature had no effect on the overall risk of AECOPD hospitalization, but showed a slight protective effect in the group ≥ 65 years old, which may be related to the mild climate of Panzhihua City. The highest temperature in Panzhihua City during the observation period did not exceed 34.2℃. Therefore, this result does not contradict previous studies. Zhang et al. assessed the impact of environmental temperature on AECOPD in Beijing, China, and found a significant positive correlation with low temperature, not high temperature [41]. This variation could be attributed to a combination of factors including geographical and climatic differences. Numerous studies have demonstrated the influence of seasons on the mortality rates of respiratory diseases, with the heightened mortality observed during the hot summer months and cold winter periods warranting significant attention [42, 43]. Douglas et al. compared latitude with seasonal variations in all-cause mortality, highlighting the significant and intricate roles of climatic conditions, sunlight duration, and other environmental factors in the fluctuations of respiratory diseases [44]. Additionally, population adaptability might also contribute to these differences. A study investigating temporal changes in population adaptability to heat and cold revealed a decrease in susceptibility to high temperatures and heatwaves; however, no significant reduction in mortality due to cold was observed [45]. Our study only observed a slight protective effect of high temperature on AECOPD hospitalization, possibly because residents have a better adaptability to summer temperature.
The impact of temperature on disease incidence is not instantaneous and often exhibits a lag effect. Previous studies have shown that the lag effect of low temperature usually lasts longer, while high temperature either have no lag effect or a shorter one [15, 37]. The impact of low DMT on AECOPD was stronger than that of high DMT, both in terms of the number of hospital admissions and the duration of the lag effect in this study. Specifically, low DMT exhibited a more enduring lag effect. Multiple studies have reported higher numbers of AECOPD admissions during winter [11, 46]. These studies suggested that in colder months, more proactive monitoring and treatment of COPD patients should be implemented. Public awareness should also be raised with measures provided to reduce the risk of AECOPD. Additionally, medical resource allocation should be adjusted according to temperature trends to provide adequate healthcare services for the potential increase in AECOPD patients.
In the subgroup analysis, we observed a higher susceptibility to the effects of low DMT in patients aged ≥ 65, which is consistent with previous research findings [26, 47]. This increased vulnerability can be attributed to age-related declines in bodily functions, respiratory function, weakened immunity, and a higher likelihood of comorbidities, rendering them more sensitive to low DMT [48]. Additionally, we noted that under low DMT conditions, females exhibited a higher RR. However, conflicting studies suggest that females are more affected by high temperatures and less affected by low temperatures compared to males [49, 50]. The gender differences in response to temperature changes might be associated with social and behavioral factors, study design, and population choices, but the precise reasons require further investigation. Interestingly, the lag effect of low DMT persisted longer in males than in females. This could be due to men being more prone to cardiovascular diseases, with low DMT increasing cardiovascular stress and thus exerting a more extended impact on men [51].
In summary, this study had the following two key highlights. Firstly, we employed the advanced statistical method of a distributed lag non-linear model, enabling us to conduct a comprehensive analysis of the impact of different temperature and lag times on the risk of hospitalization due to AECOPD. Secondly, the statistical analysis was based on a substantial dataset from 2015–2020, and encompassing four districts in Panzhihua City. This extensive data coverage enhances the reliability and generalizability of our findings. However, there are certain limitations in this study. Firstly, the scope of our research was limited to Panzhihua City; therefore, its applicability to other regions with distinct climatic characteristics may be constrained. Secondly, there might be unidentified or uncontrolled factors that could affect the accuracy of the results. Additionally, existing literature suggested interactions among diurnal temperature range, relative humidity, and atmospheric pressure, which heighten COPD risk [26, 52]. In our study, we only analyzed relative humidity and atmospheric pressure as confounding factors. Future research should aim at further investigate the correlation between humidity, atmospheric pressure and AECOPD.
Conclusion
This study revealed an association between lower DMT and increased AECOPD hospitalizations in Panzhihua, China. The lag effects of low (12.1°C) and relatively low (13.3°C) DMTs were evident from the second day and persist for over two weeks. Furthermore, our findings indicate that females and patients aged over 65 are particularly susceptible to the adverse effects of low DMT on AECOPD. This study not only provide new insights into how low temperatures impact AECOPD hospitalization rates but also highlight the vulnerability of specific groups, which is crucial for the formulation of public health strategies. Our findings highlight the importance of environmental factors in the management of chronic diseases, urging future research to explore the broader impact of environmental health.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COPD:
-
Chronic obstructive pulmonary disease
- AECOPD:
-
Acute exacerbation of COPD
- DLNM:
-
Distributed Lag Non-Linear Model
- RR:
-
Relative risk
- DMT:
-
Daily mean temperature
References
Tran HM, Chuang TW, Chuang HC, et al. Climate change and mortality rates of COPD and asthma: a global analysis from 2000 to 2018. Environ Res. 2023;233:116448.
Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–22. https://doi.org/10.1016/S0140-6736(20)30925-9, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7567026/?report=printable.
Vogelmeier CF, Criner GJ, Martínez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Arch Bronconeumol. 2017;53(3):128–49.
Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–17.
Jenkins CR, Celli B, Anderson JA, et al. Seasonality and determinants of moderate and severe COPD exacerbations in the TORCH study. Eur Respir J. 2012;39(1):38–45.
Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–73.
Hurst JR, Han MK, Singh B, et al. Prognostic risk factors for moderate-to-severe exacerbations in patients with chronic obstructive pulmonary disease: a systematic literature review. Respir Res. 2022;23(1):213.
Guarascio AJ, Ray SM, Finch CK, et al. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–45.
Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–46.
McDermott-Levy R, Scolio M, Shakya KM, et al. Factors that influence climate change-related mortality in the United States: an integrative review. Int J Environ Res Public Health. 2021;18(15):8220.
Lin MT, Kor CT, Chang CC, et al. Association of meteorological factors and air NO(2) and O(3) concentrations with acute exacerbation of elderly chronic obstructive pulmonary disease. Sci Rep. 2018;8(1):10192.
Fong FC, Smith DR. Exposure-lag response of air temperature on COVID-19 incidence in twelve Italian cities: a meta-analysis. Environ Res. 2022;212(Pt A):113099.
Baek K, Choi J, Park JT, et al. Influence of temperature and precipitation on the incidence of hepatitis A in Seoul, Republic of Korea: a time series analysis using distributed lag linear and non-linear model. Int J Biometeorol. 2022;66(9):1725–36.
Almendra R, Loureiro A, Silva G, et al. Short-term impacts of air temperature on hospitalizations for mental disorders in Lisbon. Sci Total Environ. 2019;647:127–33.
Yang RQ, Wang YR, Dong JY, et al. Association between ambient temperature and cause-specific respiratory outpatient visits: a case-crossover design with a distributed lag nonlinear model in Lanzhou, China. Urban Clim. 2022;46:46.
Gasparrini A, Armstrong B, Kenward MG. Distributed lag non-linear models. Stat Med. 2010;29(21):2224–34.
Zhao R, Gao Q, Hao Q, et al. The exposure-response association between humidex and bacillary dysentery: a two-stage time series analysis of 316 cities in mainland China. Sci Total Environ. 2021;797:148840.
Li Y, Xia Y, Zhu H, et al. Impacts of exposure to humidex on cardiovascular mortality: a multi-city study in Southwest China. BMC Public Health. 2023;23(1):1916.
Gasparrini A. Distributed lag linear and non-linear models in R: the package dlnm. J Stat Softw. 2011;43(8):1–20.
Luo Y, Li H, Huang F, et al. The cold effect of ambient temperature on ischemic and hemorrhagic stroke hospital admissions: a large database study in Beijing, China between years 2013 and 2014-utilizing a distributed lag non-linear analysis. Environ Pollut. 2018;232:90–6.
Bhaskaran K, Gasparrini A, Hajat S, et al. Time series regression studies in environmental epidemiology. Int J Epidemiol. 2013;42(4):1187–95.
Gasparrini A, Armstrong B, Kenward MG. Multivariate meta-analysis for non-linear and other multi-parameter associations. Stat Med. 2012;31(29):3821–39.
Sera F, Armstrong B, Blangiardo M, et al. An extended mixed-effects framework for meta-analysis. Stat Med. 2019;38(29):5429–44.
van Aert RCM, Schmid CH, Svensson D, et al. Study specific prediction intervals for random-effects meta-analysis: a tutorial: prediction intervals in meta-analysis. Res Synth Methods. 2021;12(4):429–47.
Chen R, Yin P, Wang L, et al. Association between ambient temperature and mortality risk and burden: time series study in 272 main Chinese cities. BMJ. 2018;363:k4306.
Jo EJ, Choi MH, Kim CH, et al. Patterns of medical care utilization according to environmental factors in asthma and chronic obstructive pulmonary disease patients. Korean J Intern Med. 2021;36(5):1146–56.
Liu Z, Li YH, Cui ZY, et al. Prevalence of tobacco dependence and associated factors in China: findings from nationwide China Health Literacy Survey during 2018–19. Lancet Reg Health West Pac. 2022;24:100464.
Wheaton AG, Liu Y, Croft JB, et al. Chronic obstructive pulmonary disease and smoking status - United States, 2017. MMWR Morb Mortal Wkly Rep. 2019;68(24):533–8.
Lu BB, Gu SH, Wang AH, et al. [Study on influence of air temperature on daily chronic obstructive pulmonary disease mortality in Ningbo]. Zhonghua Liu Xing Bing Xue Za Zhi. 2017;38(11):1528–32.
Donaldson GC, Seemungal T, Jeffries DJ, et al. Effect of temperature on lung function and symptoms in chronic obstructive pulmonary disease. Eur Respir J. 1999;13(4):844–9.
McCormack MC, Paulin LM, Gummerson CE, et al. Colder temperature is associated with increased COPD morbidity. Eur Respir J. 2017;49(6):1601501.
Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27.
Davie GS, Baker MG, Hales S, et al. Trends and determinants of excess winter mortality in New Zealand: 1980 to 2000. BMC Public Health. 2007;7:263.
Gu S, Wang X, Mao G, et al. The effects of temperature variability on mortality in patients with chronic obstructive pulmonary disease: a time-series analysis in Hangzhou, China. Environ Sci Pollut Res Int. 2022;29(47):71502–10.
Krachunov II, Kyuchukov NH, Ivanova ZI, et al. Impact of air pollution and outdoor temperature on the rate of chronic obstructive pulmonary disease exacerbations. Folia Med (Plovdiv). 2017;59(4):423–9.
Tian H, Zhou Y, Wang Z, et al. Effects of high-frequency temperature variabilities on the morbidity of chronic obstructive pulmonary disease: evidence in 21 cities of Guangdong, South China. Environ Res. 2021;201:111544.
Lin S, Luo M, Walker RJ, et al. Extreme high temperatures and hospital admissions for respiratory and cardiovascular diseases. Epidemiology. 2009;20(5):738–46.
Zanobetti A, O’Neill MS, Gronlund CJ, et al. Summer temperature variability and long-term survival among elderly people with chronic disease. Proc Natl Acad Sci U S A. 2012;109(17):6608–13.
Liu C, Liu C, Zhang P, et al. Association of greenness with the disease burden of lower respiratory infections and mediation effects of air pollution and heat: a global ecological study. Environ Sci Pollut Res Int. 2023;30(40):91971–83.
Xie MY, Ni H, Zhao DS, et al. Effect of diurnal temperature range on the outpatient visits for acute bronchitis in children: a time-series study in Hefei. China Public Health. 2017;144:103–8.
Zhang Y, Liu X, Kong D, et al. Effects of ambient temperature on acute exacerbations of chronic obstructive pulmonary disease: results from a time-series analysis of 143318 hospitalizations. Int J Chron Obstruct Pulmon Dis. 2020;15:213–23.
Ho ATN, Shmelev A, Charbek E. Trends and seasonal variation of hospitalization and mortality of interstitial lung disease in the United States from 2006 to 2016. Respir Res. 2020;21(1):152.
Achebak H, Garcia-Aymerich J, Rey G, et al. Ambient temperature and seasonal variation in inpatient mortality from respiratory diseases: a retrospective observational study. Lancet Reg Health Eur. 2023;35:100757.
Douglas S, Rawles J. Latitude-related changes in the amplitude of annual mortality rhythm. The biological equator in man. Chronobiol Int. 1999;16(2):199–212.
Arbuthnott K, Hajat S, Heaviside C, et al. Changes in population susceptibility to heat and cold over time: assessing adaptation to climate change. Environ Health. 2016;15 Suppl 1(Suppl 1):33.
Sun S, Cao W, Mason TG, et al. Increased susceptibility to heat for respiratory hospitalizations in Hong Kong. Sci Total Environ. 2019;666:197–204.
Luan G, Yin P, Wang L, et al. Association between ambient temperature and chronic obstructive pulmonary disease: a population-based study of the years of life lost. Int J Environ Health Res. 2019;29(3):246–54.
Zou E, Worsham C, Miller NH, et al. Emergency visits for thunderstorm-related respiratory illnesses among older adults. JAMA Intern Med. 2020;180(9):1248–50.
Yang J, Ou CQ, Ding Y, et al. Daily temperature and mortality: a study of distributed lag non-linear effect and effect modification in Guangzhou. Environ Health. 2012;11:63.
Stafoggia M, Forastiere F, Agostini D, et al. Vulnerability to heat-related mortality: a multicity, population-based, case-crossover analysis. Epidemiology. 2006;17(3):315–23.
Armeni E, Lambrinoudaki I. Androgens and cardiovascular disease in women and men. Maturitas. 2017;104:54–72.
Bao HR, Liu XJ, Tan EL, et al. [Effects of temperature and relative humidity on the number of outpatients with chronic obstructive pulmonary disease and their interaction effect in Lanzhou, China]. Beijing Da Xue Xue Bao Yi Xue Ban. 2020;52(2):308–16.
Acknowledgements
Not applicable.
Informed consent
We confirmed that informed consent was obtained from all subjects and their legal guardians.
Funding
This work was funded by the Research Programmer of Panzhihua Science and Technology Bureau (grant number 2021CY-S-4), Special Basic Cooperative Research Programs of Yunnan Provincial Undergraduate Universities’ Association (grant numbers 202101AO070272, 202101BA070001-220), Sichuan Science and Technology Program (grant numbers 21ZYZF-S-01) and Research Programmer of Panzhihua Science and Technology Bureau (grant number 2021ZX-5-1).
Author information
Authors and Affiliations
Contributions
Y.Y. was responsible for conceptualization, formal analysis, funding acquisition, project administration, writing-original draft, writing-review & editing. X.L. was responsible for data curation, formal analysis, visualization. S.W. was responsible for data curation, formal analysis, project administration, resources. Y.L. & Y.L. were responsible for resources, methodology. W.X. was responsible for project administration, supervision. L.Y. was responsible for investigation, methodology. J.M. & W.W. were responsible for supervision, writing-review & editing. L.Y. was responsible for funding acquisition, project administration, methodology. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study complied with the latest revision of the Declaration of Helsinki. This study was approved by the research Ethics Committee of Panzhihua Central Hospital (NO: pzhszxyyll-2021-63).
Consent for publication
All presentations of case reports have obtained from the patient’s consent.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
12889_2024_19677_MOESM1_ESM.xlsx
Supplementary Material 1: Supplementary Table 1. Daily hospitalization information of AECOPD patients in four regions. Notes: Station represents the region where the patient belongs, DOW represents the day of the week, DMT represents daily mean temperature, DMAP represents daily mean atmospheric pressure, DMRH represents daily average relative humidity. Holiday, 1 represents yes and 0 represents no.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yang, Y., Li, X., Wang, S. et al. Assessing the impact of temperature on acute exacerbation of chronic obstructive pulmonary disease hospitalizations in residents of Panzhihua City: a multi-districts study using a distributed lag non-linear model. BMC Public Health 24, 2151 (2024). https://doi.org/10.1186/s12889-024-19677-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19677-2