
Abstract
Background
Neonatal asphyxia is a leading cause of early neonatal mortality, accounting for approximately 900,000 deaths each year. Assessing survival rates, recovery time and predictors of mortality among asphyxiated neonates can help policymakers design, implement, and evaluate programs to achieve the sustainable development goal of reducing neonatal mortality to 12/1,000 live births by 2030. The current study sought to ascertain the survival status, recovery time, and predictors of neonatal asphyxia.
Methods
A retrospective follow-up study conducted in Debre Berhan Comprehensive Specialized Hospital, which carried out from May 20th to June 20th, 2023 using records of asphyxiated babies in NICUs from January 1st, 2020 to December 31st, 2022, involving a sample size of 330. Pre-structured questionnaires created in Google Form were used to collect data, and STATA Version 14.0 was utilized for data entry and analysis, respectively. The Kaplan–Meier survival curve, log rank test, and median time were calculated. A multivariable Cox proportional hazards regression model was fitted in order to determine the predictors of time to recovery. Variables were statistically significant if their p-value was less than 0.05.
Results
Three hundred thirty admitted asphyxiated neonates were followed a total of 2706 neonate -days with a minimum of 1 day to 18 days. The overall incidence density rate of survival was 9.9 per 100 neonates’ days of observation (95% CI: 8.85–11.24) with a median recovery time of 9 days (95% CI: 0.82–0.93). Prolonged labor (Adjusted hazard ratio (AHR: 0.42,95%CI:0.21–0.81), normal birth weight (AHR:2.21,95% CI: 1.30–3.70),non-altered consciousness (AHR:2.52,CI:1.50–4.24),non-depressed moro reflex of the newborn (AHR:2.40,95%CI: 1.03–5.61), stage I HIE (AHR: 5.11,95% CI: 1.98–13.19),and direct oxygen administration via the nose (AHR: 4.18,95% CI: 2.21–7.89) were found to be independent predictors of time to recovery of asphyxiated neonates..
Conclusion
In the current findings, the recovery time was prolonged compared to other findings. This implies early diagnosis, strict monitoring and provision of appropriate measures timely is necessary before the babies complicated into the highest stage of hypoxic –ischemic encephalopathy(HIE) and managing complications are the recommended to hasten recovery time and increase the survival of neonates.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Neonatal asphyxia, defined as the inability to breathe on one's own from birth, is marked by a marked impairment of respiratory gas exchange (oxygen and carbon dioxide), which leads to progressive hypoxemia and hypercapnia along with a marked acidosis in the metabolism. Birth asphyxia is diagnosed in a newborn with a fifth-minute Apgar score of seven. World Health Organization (WHO) states that the APGAR score at 1 and 5 min can be used to define and categorize birth asphyxia as mild, moderate, or severe. Newborns may experience mild, moderate, or severe encephalopathy in the 72 h that follow the hypoxic-ischemic insult [1].
Globally, neonatal asphyxia is a leading cause of morbidity and mortality in newborns. Each year, approximately 4 million neonates experience severe oxygen deprivation during birth [2], with nearly 20 per 1000 deliveries requiring resuscitation due to neonatal asphyxia (biochemical and clinical evidence) [3]. Neonatal asphyxia is a leading cause of neonatal mortality, resulting in an estimated 900,000 deaths worldwide annually [5, 6]. Neonatal asphyxia causes approximately 23% of newborn deaths worldwide [7].
According to the World Health Organization reports, 3.6 million newborns (3%) in developing nations suffer from moderate to severe asphyxiation at birth, of which 23% die and roughly the same number experience severe sequelae [4].
In most industrialized countries, neonatal asphyxia causes less than 0.1% of infant deaths. In developing countries, the rate of neonatal asphyxia is significantly higher, with a fatality rate exceeding 40% [8]. Compared to developed countries, developing nations experience a higher global incidence of neonatal asphyxia [9]. In developing countries, asphyxiation at birth occurs ten times more frequently than in developed countries [10], which is the leading cause of neonatal death in low- and middle-income countries, as well as the primary cause of long-term neurodevelopmental disorders [11]. Improved perinatal care, continuous fetal monitoring during labor, early presentation of newborns to neonatal intensive care units (NICUs), and treatment options have increased the chance of survival for asphyxiated neonates in the western world. This was not the case in developing countries, where there are high rates of mortality and lengthy hospital stays or recovery periods [12]. In East Africa, neonatal mortality rates range from 11 to 102 per 1000 live births, with neonatal asphyxia being the leading cause of death in 2015 (31.6%) [7]. In Ethiopia, neonatal asphyxia is the second leading cause of neonatal mortality (26.7%) and the fourth leading cause of death among children under the age of five (11.3%) [13].
Neonatal asphyxia is a major contributing factor in most neonatal deaths. Consistent with this, Ethiopia has a high incidence of birth asphyxia (22.52%), which is the second most common cause of neonatal death [14]. While most asphyxiated babies recover, prolonged exposure to prenatal hypoxia–ischemia can cause multi-organ damage [4]. Prolonged hypoxia can cause financial and emotional burdens for families and communities, with both short-term and long-term complications [15].
Obstetrical or fetal disorders that develop prior to, during, or following delivery, or a combination of these, can result in neonatal asphyxia [16, 17]. Many outcomes occur in the neonate's life as a result of neonatal asphyxia, such as hypoxic-ischemic encephalopathy (HIE), multiple organ dysfunction, severe neurodevelopmental delay, motor delay, and cerebral delay [18, 19].
Despite national programs to prevent neonatal asphyxia asphyxia by providing high-quality prenatal, intra-natal, and postnatal care to all women, neonatal asphyxia remains a significant issue in Ethiopia, with limited data on recovery rates and predictive factors. This study aimed to assess the survival rate, and recovery time of asphyxiated neonates and identify predictors of recovery time during PNA treatment in public hospitals in Debre Berhan, Ethiopia.
Methods
Study design, study area and study period
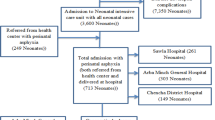
A retrospective follow-up study was carried out among neonates with asphyxia who were admitted to the Debre Berhan Comprehensive Specialised Hospital (DBCSH), located in Debre Berhan, Ethiopia. Using data from newborns who were admitted to neonatal intensive care unit (NICUs) due to asphyxia between January 1, 2020, and December 31, 2022. The study was conducted from May 20th to June 20th, 2023.
Population
The study population consisted of all asphyxiated neonates who fulfilled eligibility criteria and randomly selected from the source populations of all asphyxiated neonates admitted to the neonatal intensive care unit at Debre Berhan Comprehensive Specialised Hospital between January 1st, 2020, and December 31st, 2022.
Inclusion criteria and exclusion criteria
All newborns who were admitted to the neonatal intensive care unit at Debre Berhan Comprehensive Specialised Hospital between January 1st, 2020, and December 31st, 2022, with a confirmed diagnosis of asphyxia, were included in the study. The babies were monitored until they either experienced the event or turned 28 days postnatal. This study excluded all neonates with asphyxia who had incomplete medical records and babies with significant congenital abnormalities.
Sample size determination and sampling technique
The sample size would be determined by the log-rank test, and Freedman method using.
STATAsoftwareversion14.0.
Where:
Zα/2 = standard normal variable at 95% confidence interval level = (1.96) Zβ = power of 80% = (0.842),P = cumulative survival probability at end of study (28 days) is 0.04%, Hazard ratio = 0.5, Pr (E) = probability of event for outcome variable(recovery) and IR = incidence rate is 10% as obtained from a retrospective study done in Addis Ababa public hospitals on time to recovery and predictors of asphyxia among neonates [20]. E = number of interested events is 66 and the probability of an event (recovery) is 0.2 so the total sample size is calculated as;
The samples were taken in a way that the registration logbook was searched for medical record numbers of babies diagnosed with perinatal asphyxia. The study participants were then chosen using a computer-generated simple random sampling technique from the isolated medical record numbers in the hospital. Finally, from April to May 2023, the selected medical charts would be reviewed.
Variables
Outcome variable (dependent) is time to recovery dichotomized as (recovered = 1, censored = 0). Independent variables includes socio-demographic and obstetrics –maternal age, place of residency, antenatal follow-up, maternal hypertension, prolonged labor, mode of labor, meconium-stained amniotic fluid, prolonged rupture of membrane, Neonatal related predictors- sex of neonate, gestational age, postnatal age at presentation, birth weight, fetal presentation, Treatment related predictors- bag mask ventilation, calcium gluconate, aminophylline, fluid and electrolyte management, oxygenation, Clinical and laboratory predictors-APGAR score, clinical status at admission, stage of hypoxic –ischemic encephalopathy(HIE), vital sign change and comorbidities.
Operational definition
Neonatal asphyxia- failure to initiate and sustain spontaneous breathing, and will diagnosed based on a clinical conditions made by a healthcare provider and documented on the charts. Time to recovery- the average time that the patient will take to recover from an illness or disease Hypoxic-ischemic encephalopathy (HIE) stages –will determined based on saranat's classification of a clinical diagnosis made by a healthcare provider (stage 1, stage 2, stage 3). Survival time-The number of days it takes from admission to the recovery of a neonate from asphyxia (measured by incidence density rate and median recovery time). The incidence density rate- will be determined by dividing the number of events by the total follow-up time in person-days. Follow-up time- is the time that the patient begins to follow up from 0 to 28 days of observation. Major congenital anomalies (malformation) – a physical defect present in a newborn at birth that results in central nerve system depression. Survival- In this study, survival refers to newborns who are recovered and/or been discharged from the NICUs after completing their treatment and are no longer displaying clinical signs of asphyxia. Censored- newborns who have referral sheets, death summary sheets, incomplete medical records and medical against (caregivers sign on behalf of the newborn) were censored. Died- those newborns who passed away and whose death report is recorded on the charts. Co-morbidities- newborns with perinatal asphyxia and other medical problems Event- Infants who recovered from perinatal asphyxia. Out born – give birth out of hospital in this study Inborn – give birth in the hospital in this study. Two-third of fluid management- the total amount of fluid calculated based on weight and for the maintenance purpose, two-third were given. Total fluid- the amount of fluid fully calculated based on weight and given.
Data collection tool and procedure
Using the FMOH standardized log, registration book, perinatal follow-up chart, neonatal evaluation sheet, neonatal referral paper, and additional reviewed articles, a structured questionnaire was created[10]. To standardize the data collection process, supervisors and data collectors received training on the importance of the study, how to complete the checklist, and ethical considerations. Next, all available data on patient records was examined, and the records of each study participant were chosen in accordance with the inclusion criteria. Using a structured data extraction form, all relevant variables that satisfy the study's objectives were taken out of the patient charts. Examining the patient's chart allowed confirmation of the treatment outcomes. A pretest involving 5% (17 charts) of the study participants was conducted to guarantee the quality of the data. Before the analysis, errors discovered during the verification process were fixed and adjusted to guarantee that the data abstraction format complied with the study's goals. When data was being managed, stored, cleaned, and analyzed, all completed data collection forms were checked for consistency and completeness. The principal investigator also randomly selected medical records and cross-checked them to ensure consistency.
Data processing and analysis
After being coded, amended, and cleaned, the data were imported into a Google Spreadsheet and then exported to the statistical program STATA version 14.0 for additional examination. Descriptive and inferential statistics would be used to present the data. The necessary assumptions of the Cox-proportion hazard regression models would be validated using Schoenfeld's residual test. The Kaplan–Meier survival curve would be used to estimate survival time, and the survival curves between categorical predictors would be compared using the Log-rank test. For each explanatory variable, a bivariate Cox-proportional hazards regression model would be fitted. To identify independent predictors of asphyxiated neonate survival, variables with p-values less than 0.2 would next be fitted to a multivariable Cox regression analysis. The statistical significance of the predictor associations was evaluated using a hazard ratio at a 95% confidence level. In the multivariable Cox regression analysis, variables are significant predictors of asphyxiating neonate survival if the p-value is less than 0.05. Finally, text, tables, and graphs would be included, along with a summary of the findings.
Results
Socio-demographic and Obstetrics characteristics of the study participants
Following the review of 330 asphyxiated neonatal charts, 330 (100%) of them qualified for this investigation. 238 (72%) of the mothers were in the 20–34 age range. Nearly all of the 319(97%) pregnant women had prenatal care visits, and over half of the 205(62%) mothers gave birth for the first time. In terms of delivery mode, 204 (62%) and 54 (16%) were spontaneous vaginal deliveries and caesarean sections (C-sections), respectively. 211 (64%) cases of pre/eclampsia, 87 (26%) cases of meconium-stained amniotic fluid (MSAF), 19 (6% cases) of oligohydramnios, and 13 (4% cases) of pregnant women with obstetrics and medical complications documented during their pregnancies were among the pregnant women with these conditions. Out of the 330 newborns admitted in total, 60% of them were born in Debre Berhan Comprehensive Specialized Hospital (inborn) (Table 1).
Neonatal characteristics of the study participants
Of the cohort, 134 (60%) of the participants were infant males. Out of the cohort, 264 (80%) were term, 22 (7%), were post term, and 44 (13%) were preterm. Based on the postnatal age, 268 (81.21%) of the patients were admitted to the neonatal ward before 24 h, while 62 (18.79%) required more than 24 h to be admitted to the NICU. A quarter of the neonates cried and had normal APGAR scores of (> = 7) in the first minute of their lives in both survival and censored scenarios, whereas nearly three-fourths of the neonates did not cry at all at birth. When it came to the APGAR score at the five-minute mark, 218 (66.06%) of the participants had an APGAR score of less than seven, and 112 (32.94%) of them had an APGAR score of more than seven.
Clinical and Laboratory characteristics of the study participants
Hypothermia is 82 (24.85%), respiratory distress syndrome 198 (60%) and meconium-stained amniotic fluid among asphyxiated newborns, 50(15.15%) were the most commonly observed additional medical issues at admission and during their hospital stays. Of the newborns with stage II HIE, 36 (or 15%) had censored. Of the total neonates that survived, 210 (64%) and 60 (18%) were still alive when they were released from stage II and stage I, respectively. 77 (23.33%) and 54 (20%) of the neonates who made it through the ordeal and appeared in NICUs with altered consciousness were censored due to having a depressed moro reflex. Upon admission, 218 (66.06%) were hypothermic, 153 (46.36%) had low oxygen saturation, and 59 (17.88%) had gasping breathing or a respiratory rate of less than 30 breaths per minute. Among all the neonates who survived, 104 (38.5%) had a normal heart rate, 170 (52%), 80 (24.2%) had a normal temperature, and 143 (43%), with normal oxygen saturation levels within the first 24 h of postnatal life. 8 (2.42%) and 44 (13.33%) had respiration rates of less than 30 b/min and more than 60 b/min, respectively, after 24 h of admission. 18 (5.45%) and 124 (37.58%) of the patients with heart rates greater than 160 beats per minute were hypothermic (below 36.5 degrees Celsius), and 25 (7.58%) of them were desaturated in room air or had saturation levels below 85%.
Treatment related characteristics of the study participants
At birth, more than half (67.58%) of the babies received resuscitation, 64.7% were given intra nasal oxygen, and 13.23% were given continuous positive airway pressure (CPAP), Aminophylline (10.3%) and anticonvulsant (12%) were taken, respectively. Two thirds of the maintenance fluid were given to the majority of asphyxiated newborns (77.58%).
Overall proportion and incidence rate of survival of asphyxiated neonates
Among the study participants, 60 (18.2%) were censored, and 270 (81.8%) asphyxiated neonates were recovered and discharged from NICUs alive. It was discovered that, overall, the incidence density rate of survival for asphyxiated neonates was 9.9 per 100 neonatal days of observation (95% CI: 8.85–11.24).
Time to recovery of neonates with asphyxia
A total of 2706 neonate-days were monitored for 330 admitted asphyxiated babies, ranging from a minimum of 1 day to a maximum of 18 days. The median survival period was 9 days (95% CI: 0.82–0.93). For the 1, 3, 7, 14, and 18 days, the estimated cumulative probability of survival was 1.0, 1.0, 0.69, 0.03, and 0.0, respectively. Figure 1.

Overall Kaplan -Meier survival estimate of asphyxiated neonates admitted in DBCSH, Ethiopia from 2020-2022, Debre Berhan, Ethiopia, 2023
Predictors of survival status of asphyxiated neonates
According to the findings of a multivariable Cox regression analysis, women who gave birth to their children after a protracted labor had a 58% lower chance of recovering from asphyxia than women who did not (AHR: 0.42, 95% CI: 0.21–0.81). Normal-weight babies had a 2.2-fold higher chance of recovering from asphyxia compared to low-weight babies (AHR: 2.21, 95% CI: 1.30–3.76). Compared to their counterparts, newborns who had not changed their level of consciousness were 2.5 times more likely to recover from asphyxia (AHR:2.52, 95%CI:1.50–4.24), and those who had not experienced a decline in their moro reflexes were 2.4 times more likely to do so (AHR: 2.4, 95%CI:1.03–5.61). The recovery process either slowed down or lengthened as the HIE stage rose. Infants given continuous positive airway pressure (CPAP) were 4.2 times less likely to recover from asphyxia than those given direct oxygen (intranasal) (AHR: 4.18, 95 CI: 2.21–7.89).Vital signs were a critical sign of whether a newborn was improving or worsening. The multivariable Cox regression analysis revealed that babies who were asphyxiated had respiratory rates of 30 to 60 breaths per minute at 24 h, which indicated an 8.6-fold increased likelihood of recovering from asphyxia compared to their counterparts (AHR:8.68, 95%CI: 3.78–19.90). Compared to their counterparts, babies with heart rates less than 100 beats per minute at 24 h had an 82% lower chance of recovering earlier (AHR: 0.18, 95% CI: 0.37–0.93). And compared to their counterparts, babies whose hearts beat faster than 160 beats per minute had a 79% lower chance of recovering from asphyxia (AHR: 0.21, 95% CI: 0.08–0.50). Since asphyxia involves the brain being deprived of oxygen, it was necessary to measure the saturation level. According to the multivariable, babies with an oxygen saturation level of less than 85% upon admission had a 44% lower chance of recovering from asphyxia sooner than their peers. In terms of comorbidities, neonates with random blood sugar (RBS) at 24 h (> 60 mg/dl) were 42 times more likely than their peers to recover from asphyxia more quickly (AHR: 6.2, 95%CI: 3.54–15.56) (Fig. 2) (Table 2).

Log-rank survival estimate for time to recovery of asphyxiated neonates by postnatal gestational age presented & admitted at NICU of DBCSH, Debre Berhan, Ethiopia from 2020–2022
Discussion
In the current study, asphyxiated neonates admitted to Debre Berhan Comprehensive Specialised Hospital had their recovery time from asphyxiated neonates presented, along with its predictors. According to this study, asphyxiated newborns recovered on average after nine days. This result was similar to the research conducted in Dire Dawa (7 days) [21] and Addis Ababa (8 days) [20]. This study's statistically significant finding is that neonates who are preterm or have low birth weight have a decreased chance of surviving than their counterparts. The scientific and clinical explanation for this is that babies born low birth weight or preterm frequently have poor immune systems, feeding problems, and immature respiratory and thermoregulation centers. They may also have poor prognoses and require longer hospital stays if standard NICU care is not given. Because of the prematurity of the respiratory center, nervous system, immune system, and thermoregulation mechanism, the gestational age, birth weight, and age of the neonates at the time of presentation to the NICU affected the survival rates and recovery times of the asphyxiated newborns. The results were in line with research done in Jimma and Kenya [22, 23].
According to the study's findings, the likelihood of a newborn recovering from asphyxia varied based on the stage of hypoxic-ischemic encephalopathy (HIE), and stage I HIE patients have a slightly better chance than their counterparts of surviving and recovering from asphyxia. Additional research results [24,25,26,27,28] corroborated this conclusion. The central nervous system and the kidneys are the next most seriously impacted systems, after asphyxia, according to scientific explanations for this finding. The prognosis of infants who are asphyxiated is reduced due to the primary and secondary energy failure that often occurs as HIE progresses, which also leads to the emergence of various neurologic sequelae [29]. Second, when a neonate has multiple organ damage and prolonged hypoxia, management and care are often insufficient and ineffective. Finally, because necrotizing enterocolitis exacerbated thrombocytopenia and malnutrition, infants with advanced HIE were often kept on NPO (nothing by mouth) and had unstable blood sugar levels. This could make things more difficult and require more time and resources to deal with the problems that arise.
The results of this study also demonstrated that there is a statistically significant change in the babies' vital signs both during and after their 24-h admission (respiratory rate, heart rate, temperature, saturation, random blood sugar at admission, random blood sugar at 24 h). This alteration in vital signs happens when newborns don't get enough oxygen, which causes lifelong harm to the heart, brain, lung, kidney, intestines, and other organs. This finding implies that the babies' recovery times would have shortened if they hadn't received care sooner. Studies conducted in Nigeria produced similar results [30].
The patient's clinical state upon admission—a changed state of consciousness and a depressed moro reflex—was statistically significant and had an effect on the patient's recovery, according to the study's statistics. Two countries with limited resources, South Africa and Nigeria [28, 31], endorsed the results as well. Additionally, asphyxiated newborns who were given aminophylline (AHR = 2.05, 95 CI: 1.06–3.96) and direct oxygen through the nose (AHR = 4.18, 95 CI: 2.21–7.89) recovered from asphyxia more quickly than their counterparts. Research done in Tanzania [32, 33] refuted this conclusion. If intranasal oxygen is given to the babies, it can be scientifically explained that the organ insult is mild, easily reversible, and helps to maintain a normal state. On the other hand, if infants were given continuous positive airway pressure, or CPAP, the injury would be severe and potentially hard to recover from.
This study found that prolonged labor period is associated with asphyxia recovery time (AHR: 0.42, 95% CI: 0.2–0.81). The longer the labor, the greater the risk of asphyxia for the babies and the lower the chance of asphyxia recovery. A meta-analysis study conducted in Ethiopia provides support for this finding [34]. And clarified by saying that too much contraction causes meconium to leak, the baby may suck, and the compressed umbilical cord may bleed or become ischemic. Finally, the neonate ends up with asphyxia.
Although the statistical results of the current study are not statistically significant in this regard, the administration of calcium gluconate during the first few days of life in conjunction with intravenous fluid therapy may enhance the baby's chances of survival and offer potential benefits over those who do not take prophylactic calcium gluconate. Low calcium intake, hyperphosphatemia, excessive bicarbonate, and functional hypoparathyroidism are the most frequent scientific causes of hypocalcemia in newborns with asphyxia [35]. The need for managing hypocalcemia was less in newborns who received intravenous calcium infusions in a Tanzanian randomized control trial evaluating the efficacy of prophylactic calcium gluconate administration in the first five days of life [36].
Conclusion
The overall recovery rate was 9.9 per 100 neonates-day observations, with a median recovery time of 9 days. This demonstrated that the recovery time was prolonged. Neonatal survival time for asphyxiated neonates was predicted by low birth weight, prolonged labor, gestational age, postnatal age at presentation, altered consciousness at admission, depressed Moro reflex at admission, stage of HIE, and oxygen management. As a result, early diagnosis, strict monitoring, and timely implementation of appropriate measures are required before babies reach the highest stage of hypoxic-ischemic encephalopathy (HIE), and prevention and managing complications is recommended to speed up recovery time and increase neonate survival.
Availability of data and materials
Upon a reasonable request, the corresponding author will make the data utilized and/or analyzed for this study available.
References
Geme, J.W.S., Nelson textbook of pediatrics. 2020: Elsevier.
Padayachee N, Ballot DE. Outcomes of neonates with perinatal asphyxia at a tertiary academic hospital in Johannesburg, South Africa. South African Journal of Child Health. 2013;7(3):89–94.
Ahearne CE, Boylan GB, Murray DM. Short and long term prognosis in perinatal asphyxia: An update. World journal of clinical pediatrics. 2016;5(1):67.
Gupta SK, et al. Clinical profile of neonates with perinatal asphyxia in a tertiary care hospital of central Nepal. JNMA J Nepal Med Assoc. 2014;52(196):1005–9.
Weiner GM, et al. Respiratory and Cardiovascular Support in the Delivery Room. In: The Newborn Lung. Elsevier; 2019. p. 173–95.
Spector JM, Daga S. Preventing those so-called stillbirths. Bull World Health Organ. 2008;86:315–6.
Grady, S.C., et al., Neonatal mortality in East Africa and West Africa: a geographic analysis of district-level demographic and health survey data. Geospatial health, 2017;12(1).
Yitayew YA, Yalew ZM. Survival status and predictors of mortality among asphyxiated neonates admitted to the NICU of Dessie comprehensive specialized hospital, Amhara region, Northeast Ethiopia. PLoS ONE. 2022;17(12): e0279451.
Odd D, et al. Hypoxic-ischemic brain injury: Planned delivery before intrapartum events. Journal of neonatal-perinatal medicine. 2017;10(4):347–53.
Getaneh FB, et al. Survival and predictors of asphyxia among neonates admitted in neonatal intensive care units of public hospitals of Addis Ababa, Ethiopia, 2021: a retrospective follow-up study. BMC Pediatr. 2022;22(1):1–13.
Wallander JL, et al. Brain research to ameliorate impaired neurodevelopment-home-based intervention trial (BRAIN-HIT). BMC Pediatr. 2010;10:1–9.
Usman, F., et al., Newborn mortality in Sub-Saharan Africa: why is perinatal asphyxia still a major cause? Annals of global health, 2019;85(1).
Mekonnen, W., et al., Under five causes of death in Ethiopia between 1990 and 2016: Systematic review with meta-analysis. Ethiopian Journal of Health Development, 2020;34(2).
Bayih, W.A., et al., The state of birth asphyxia in Ethiopia: An umbrella review of systematic review and meta-analysis reports, 2020. Heliyon, 2021;7(10).
Eunson P. The long-term health, social, and financial burden of hypoxic–ischaemic encephalopathy. Dev Med Child Neurol. 2015;57:48–50.
Igboanugo, S., A. Chen, and J.G. Mielke, Maternal risk factors for birth asphyxia in low-resource communities. A systematic review of the literature. Journal of Obstetrics and Gynaecology, 2020;40(8):1039–1055.
Wosenu L, et al. Determinants of birth asphyxia among live birth newborns in University of Gondar referral hospital, northwest Ethiopia: A case-control study. PLoS ONE. 2018;13(9): e0203763.
Babu BVA, Devi SS, Kumar BK. Birth asphyxia–Incidence and immediate outcome in relation to risk factors and complications. Int J Res Health Sci. 2014;2(4):1064–71.
Ellenberg JH, Nelson KB. The association of cerebral palsy with birth asphyxia: a definitional quagmire. Dev Med Child Neurol. 2013;55(3):210–6.
Getaneh FB, et al. Survival and predictors of asphyxia among neonates admitted in neonatal intensive care units of public hospitals of Addis Ababa, Ethiopia, 2021: a retrospective follow-up study. BMC Pediatr. 2022;22(1):262.
Derese, T., Y. Belay, and Z. Tariku, The Median Survival Recovery Time and Associated Factors Among Admitted Neonate in Intensive Care Units of Dire Dawa Public Hospitals, East Ethiopia, 2019. 2020.
Aragaw Y. Perinatal mortality and associated factor in Jimma university specialized hospital. South West Ethiopia Gynecol Obstet (Sunnyvale). 2016;6(409):2161–932.
Shikuku DN, et al. Practice and outcomes of neonatal resuscitation for newborns with birth asphyxia at Kakamega County General Hospital, Kenya: a direct observation study. BMC Pediatr. 2018;18:1–11.
Shireen N, Nahar N, Mollah A. Risk factors and short-term outcome of birth asphyxiated babies in Dhaka Medical College Hospital. Bangladesh Journal of Child Health. 2009;33(3):83–9.
Meshram RM, Bokade C. Risk factors for mortality in birth asphyxia of outborn neonates: a prospective observational study. Sri Lanka Journal of Child Health. 2019;48(1):26–32.
Siva Saranappa S, et al. Clinical profile and outcome of perinatal asphyxia in a tertiary care centre. Curr Pediatr Res. 2015;19(1–2):9–12.
Panthee K, et al. Clinical profile and outcome of asphyxiated newborn in a Medical College Teaching Hospital. Journal of Lumbini Medical College. 2016;4(1):1–3.
Ogunkunle, T.O., et al., Postnatal outcomes and risk factors for in-hospital mortality among asphyxiated newborns in a low-resource hospital setting: experience from North-Central Nigeria. Annals of Global Health, 2020;86(1).
Allen KA, Brandon DH. Hypoxic ischemic encephalopathy: pathophysiology and experimental treatments. Newborn Infant Nurs Rev. 2011;11(3):125–33.
Ekwochi U, et al. Incidence and predictors of mortality among newborns with perinatal asphyxia: a 4-year prospective study of newborns delivered in health care facilities in Enugu. South-East Nigeria Clinical Medicine Insights: Pediatrics. 2017;11:1179556517746646.
Ilah BG, et al. Prevalence and risk factors for perinatal asphyxia as seen at a specialist hospital in Gusau, Nigeria. Sub-Saharan African Journal of Medicine. 2015;2(2):64.
Gobezie WA, et al. Readiness to treat and factors associated with survival of newborns with breathing difficulties in Ethiopia. BMC Health Serv Res. 2019;19(1):1–10.
Cavallin F, et al. Factors associated with mortality among asphyxiated newborns in a low-resource setting. J Matern Fetal Neonatal Med. 2022;35(6):1178–83.
Desalew A, Semahgn A, Tesfaye G. Determinants of birth asphyxia among newborns in Ethiopia: A systematic review and meta-analysis. Int J Health Sci. 2020;14(1):35.
Kliegman, R., Nelson Textbook of Pediatrics, Edition 21. 2020: Hunan ke xue ji shu chu ban she.
Khan, M.A.G., et al., Efficacy of prophylactic intravenous calcium administration in first 5 days of life in high risk neonates to prevent early onset neonatal hypocalcaemia: A randomised controlled trial. Archives of Disease in Childhood-Fetal and Neonatal Edition, 2010.
Acknowledgements
The clinical staff and administrators at Debre Berhan Comprehensive Specialised Hospital, particularly Mr. Asmare Samuel, the hospital's chief executive officer, were greatly appreciated by the authors for their cooperation and unwavering assistance during the data collection process.
Funding
No funding was used for this study.
Author information
Authors and Affiliations
Contributions
SGY: conceptualization, methodology, writing proposal and original draft, software analysis, formal analysis, Manuscript writing. ET: supervised the design of the study, validation, data curation, writing, and editing critically. TMD: supervised the design of the study, validation, data curation, writing, and editing critically. ZAG: participate in software analysis, data extraction, and analysis. Finally, all authors approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethical approval was obtained from Debre Berhan University, Asrat Woldeyes Health.
Science Campus Institutional Review Board (IRB- 102, and approval period from May 8/2023 to May 8/2024.) before its commencement. In addition, an official.
letter of permission was obtained with from Debre Berhan Compressive Specialized Hospital before the data collection begins. The data collectors gave the interviewees an explanation of the study's purpose, benefits, risks, discomfort, and right to withdraw or refuse at any time for any reason before the interview commenced. Due to the secondary nature of the data, we were unable to obtain direct informed consent from each participant and the nature of the study is not clinical trial; however, we attempted to obtain consent from the hospital administration, and participants' privacy and confidentiality were protected during data collection. Because the individual's identity was kept hidden, the survey responses were anonymous. There was no consent given from the institution review board committee for waving. Unfortunately the hospital was given an oral consent to waive it and it was done.
Consent of publication
Not applicable.
Competing interests
Regarding the research, writing, and/or publication of this article, the author(s) have declared that they have no potential conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yehouala, S.G., Tesfahun, E., Dejene, T.M. et al. Time to recovery of asphyxiated neonates and its’ predictors among newborns admitted to neonatal intensive care unit at Debre Berhan Comprehensive Specialized Hospital, Ethiopia. BMC Public Health 24, 2006 (2024). https://doi.org/10.1186/s12889-024-19520-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19520-8