
Abstract
Objective
To study the historical global incidence and mortality trends of gastric cancer and predicted mortality of gastric cancer by 2035.
Methods
Incidence data were retrieved from the Cancer Incidence in Five Continents (CI5) volumes I-XI, and mortality data were obtained from the latest update of the World Health Organization (WHO) mortality database. We used join-point regression analysis to examine historical incidence and mortality trends and used the package NORDPRED in R to predict the number of deaths and mortality rates by 2035 by country and sex.
Results
More than 1,089,000 new cases of gastric cancer and 769,000 related deaths were reported in 2020. The average annual percent change (AAPC) in the incidence of gastric cancer from 2003 to 2012 among the male population, South Korea, Japan, Malta, Canada, Cyprus, and Switzerland showed an increasing trend (P > 0.05); among the female population, Canada [AAPC, 1.2; (95%Cl, 0.5–2), P < 0.05] showed an increasing trend; and South Korea, Ecuador, Thailand, and Cyprus showed an increasing trend (P > 0.05). AAPC in the mortality of gastric cancer from 2006 to 2015 among the male population, Thailand [3.5 (95%cl, 1.6–5.4), P < 0.05] showed an increasing trend; Malta Island, New Zealand, Turkey, Switzerland, and Cyprus had an increasing trend (P > 0.05); among the male population aged 20–44, Thailand [AAPC, 3.4; (95%cl, 1.3–5.4), P < 0.05] showed an increasing trend; Norway, New Zealand, The Netherlands, Slovakia, France, Colombia, Lithuania, and the USA showed an increasing trend (P > 0.05). It is predicted that the mortality rate in Slovenia and France’s female population will show an increasing trend by 2035. It is predicted that the absolute number of deaths in the Israeli male population and in Chile, France, and Canada female population will increase by 2035.
Conclusion
In the past decade, the incidence and mortality of gastric cancer have shown a decreasing trend; however, there are still some countries showing an increasing trend, especially among populations younger than 45 years. Although mortality in most countries is predicted to decline by 2035, the absolute number of deaths due to gastric cancer may further increase due to population growth.
Similar content being viewed by others
Introduction
Gastric cancer is one of the most common cancers worldwide [1]. In 2020, more than 1,089,000 new cases and 769,000 patients died of gastric cancer worldwide. Although the incidence of gastric cancer has been steadily declining over the past few decades [2], the decrease is much less marked in some populations, such as Canada, Brazil, Denmark, India, and Israel [3]. The recognized etiology of gastric cancer includes Helicobacter pylori infection (a major confirmed cause of gastric cancer) [4]; obesity [5]; smoking [6]; alcohol [7], high salt food [8]; coffee [9]; gastric ulcer disease [10]; gastroesophageal reflux disease [11, 12]; gastric surgery [13] and radiation exposure [14] are associated with the risk of gastric cancer.
Knowledge of gastric cancer’s global and regional epidemiology is essential for personalized decision-making in risk stratification, screening, and prevention. Owing to the high heterogeneity of epidemiological trends in different regions, using data from high-quality population-based cancer registries to predict future mortality trends is extremely important.
To date, few studies have assessed gastric cancer’s global incidence and mortality trends. A previous study [15] predicted the incidence rate of gastric cancer by 2035 but did not predict the mortality rate by 2035. We hypothesized that gastric cancer incidence and mortality rates have decreased over the past decade. In this study, we used the GLOBOCAN 2020 database, the latest data on cancer incidence in Five Continents Plus (CI5plus) database, and UN World Population Prospects 2019 Revision. We further investigated whether global trends varied by age, sex, and region. The global incidence and mortality trends of gastric cancer will be analyzed, and the mortality rate up to 2035 will be predicted.
Method
Data
A total of 41 countries participated in the analysis of incidence and mortality rates. The estimated global incidence and mortality for 2020 were retrieved from the GLOBOCAN database (http://globocan.iarc.fr). Incidence data were retrieved from country-specific registries based on the Cancer Incidence in Five Continents (CI5) volumes I-XI [16]. Mortality data from malignant neoplasms of the stomach (International Classification of Diseases (ICD)-10 C16) were obtained from the latest update of the World Health Organization (WHO) mortality database. We excluded databases with less than 15 calendar years of incidence/mortality, as this does not allow joinpoint regression analysis to be performed. The updated databases of incidence and mortality in the European Cancer Observatory and Nordic cancer registries will replace the data in the CI5 I-XI volume and WHO databases. The incidence and mortality rates for each country have been standardized (using the Segi's standard world population and the revised standard population issued by the WHO for 2020–2025).
In the database, the incidence rates for most countries range from 2003 to 2012 (with some countries' data from 1998 to 2012), and the mortality rates for most countries range from 2006 to 2015 (with some countries' data from 2001 to 2015). Therefore, in order to present a more comprehensive view of the historical trends in incidence rates and mortality rates, the data did not only show the overlapping time period (2006–2012) for both incidence and mortality rates.
Joinpoint regression analysis to examine incidence and mortality trends
We used joinpoint regression analysis (https://surveillance.cancer.gov/joinpoint/) to examine the historical incidence and mortality trends. We specified the maximum number of three joinpoints as the analysis options. To determine the direction and magnitude of recent trends, the average annual percent change (AAPC) and the corresponding 95% confidence interval (CI) were evaluated for the most recent 10-year period available. The trends of incidence and mortality rates in this study both follow a Poisson distribution. Therefore, a logarithmic linear model analysis was used.
NORDPRED predicted mortality in 2035
Age-standardized mortality rates per 100 000 person-years were calculated using the world standard population. To predict the number of deaths and mortality rates by 2035 by country and sex, an age–period–cohort model was fitted to recent trends in mortality rates. The model, implemented in R through the NORDPRED package, has been shown to perform well empirically in projecting current trends in cancer mortality in the future [17]. The three or four most recent 5-year observed periods (depending on data availability) were extrapolated using a power function to level off the growth, with a projection of the recent linear trend for the last 10 years that was attenuated (or accentuated in the case of negative trends) by 25% and 50% in the second and third prediction periods, respectively, and by 75% for both the fourth and fifth prediction periods. The number of deaths was predicted up to 2035 by taking a weighted average of the projected mortality rates for the last two prediction periods, centering on 2035, and then applying the rates to the UN World Population Prospects 2019 Revision forecasts available for each country for that year. Predicted ASRs (Age-standardised rate) were then analyzed in light of the mortality threshold of 6 per 100 000 person-years, below which cancer can have low mortality.
Ethic
As this was a retrospective study involving the examination of secondary cancer data only, patients were not involved in the design and conduct of this research. This study was approved by the Ethics Committee of Fujian Union Hospital of Fujian Medical University.
Statistical analysis
Stata.14 was used for data management and plotting observed and modeled trends. Modeling analyses were performed using R 4.10, and the functions available in the Epi package version 1.1.36, R Studio, and the NORDPRED package (http://www.kreftregisteret.no/en/Research/ Projects/ Nordpred/Nordpred-software/).
Results
New cases and deaths of gastric cancer in 2020
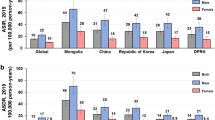
In 2020, there were more than 1,089,000 new cases of gastric cancer and 769,000 related deaths. China, Japan, India, Russia, and South Korea were the top five countries for new cases of gastric cancer. The top five countries in terms of deaths were China, India, Japan, Russia, and Brazil. (Fig. 1A, B).

A in 2020, there were 1,089,000 new cases of gastric cancer worldwide. B in 2020, there were 769,000 deaths of gastric cancer worldwide
Global incidence and mortality in 2020
The estimated incidence of gastric cancer in Asia was the highest (Fig. 2A). Regarding the total population, Mongolia, Japan, South Korea, Tajikistan and China had the highest incidence rate.

A Map of incidence rate of gastric cancer. B Map of mortality rate of gastric cancer
The estimated mortality rate of gastric cancer was the highest in Asia (Fig. 2B). Regarding the total population, Mongolia, Pakistan, Bhutan, China and Kyrgyzstan have the highest mortality rate.
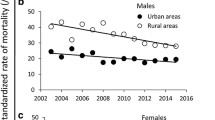
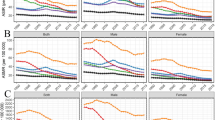
The estimated incidence and mortality rates of gastric cancer also differed between the sexes. In the total population, gastric cancer incidence and mortality rates were higher in men than women. Stratified analysis showed that gastric cancer incidence and mortality rates in men aged 45–74 and 70–85 + were higher than those in women; in the population aged 20–44, the incidence and mortality rates in men were similar to those in women (Fig. 3).

Incidence and mortality of gastric cancer by gender and age
Average annual percent change in the incidence of gastric cancer from 2003 to 2012
The average annual percent change in incidence in 41 countries from 2003 to 2012 is shown in Table 1.
Among the male population, South Korea, Japan, Malta, Canada, Thailand, Cyprus, and Switzerland showed an increasing trend (P > 0.05). Brazil, Iceland, Chile, Sweden, Denmark, Ecuador, Turkey, India, and Ireland showed a decreasing trend (P > 0.05), while the other 25 countries showed a decreasing trend (P < 0.05) (Fig. 4A).

A AAPC of the Incidence of Gastric Cancer in Individuals 0 to 85 Years or Older in male (*: P < 0.05). B AAPC of the Incidence of Gastric Cancer in Individuals 0 to 85 Years or Older in female (*: P < 0.05). C AAPC of the Mortality of Gastric Cancer in Individuals 0 to 85 Years or Older in male (*: P < 0.05). D AAPC of the Mortality of Gastric Cancer in Individuals 0 to 85 Years or Older in female (*: P < 0.05)
Among the female population, Canada [AAPC, 1.2; (95%Cl, 0.5–2), P < 0.05] showed an increasing trend; South Korea, Ecuador, Thailand, and Cyprus showed an increasing trend (P > 0.05); Iceland, Lithuania, Poland, Germany, Malta, Turkey, Ireland, Chile, the USA, and Japan showed a decreasing trend (P > 0.05), while the other 23 countries showed a decreasing trend (P < 0.05) (Fig. 4B).
Average annual percent change in the mortality of gastric cancer from 2006 to 2015
The average annual percent change in the mortality of the 41 countries from 2006 to 2015 is shown in Table 2.
Among the male population, Thailand [3.5 (95%Cl, 1.6–5.4), P < 0.05] had an increasing trend; Malta Island, New Zealand, Turkey, Switzerland, and Cyprus had an increasing trend (P > 0.05); 35 countries had a decreasing trend (P < 0.05) (Fig. 4C).
Among the female population, Thailand [4.7 (95%Cl, 3.6–5.9], P < 0.05) had an increasing trend (Iceland, Ireland, Turkey, Slovenia, Switzerland, Croatia, Denmark, Lithuania, Malta, and Cyprus had an increasing trend (P > 0.05); and 30 countries had a decreasing trend (P < 0.05) (Fig. 4D).
Predicting mortality trends and absolute number of deaths by 2035
Among the male population, it is predicted that the mortality rate in 29 countries will show a decreasing trend by 2035(Fig. 5A). Among the female population, it is predicted that the mortality in 27 countries will show a decreasing trend in 2035, and the mortality in two countries (Slovenia and France) will show an increasing trend until 2035 (Fig. 5B).

A Age standardized mortality rate per 100,000 in male. B Age standardized mortality rate per 100,000 in female
Using a mortality threshold of 6 per 100 000, 20 of 29 countries will have reached this threshold by 2035 (Fig. 5A). Using the mortality threshold of 6 per 100 000, 27 out of 29 countries will reach this threshold by 2035 (Fig. 5B). Generally, the mortality rate in male patients is higher than in female patients.
Although mortality rates continue to decrease, the absolute number of deaths is expected to increase further in some countries. Among the male population, it is predicted that the number of deaths in 28 countries will decrease by 2035, but the absolute number of deaths in Israel will increase by 2035 (Table 3). Among the female population, it is predicted that the absolute number of deaths in 26 countries will decrease by 2035, but the absolute number of deaths in Chile, France, and Canada will increase by 2035 (Table 4).
Discussion
This study aimed to further investigate the global incidence and mortality trend of gastric cancer and predict the mortality by 2035 using global data. Several key findings were obtained in this cohort study. First, East Asia has the highest incidence and mortality rates of gastric cancer. Second, in the past decade, gastric cancer incidence and mortality in major countries have decreased; however, the decreasing trend in populations younger than 45 years is not obvious. Third, mortality in Thailand has been increasing over the past decade. Finally, the absolute number of deaths due to gastric cancer in some countries is predicted to increase by 2035.
This study found that the incidence rate in East Asia was the highest, whereas that in Western Europe and Northern America was lower. This finding is consistent with those of previous studies [3, 18]. Different risk factors related to gastric cancer result in this phenomenon. Gastric cancer is divided into non-cardiac cancer (NCGC) and cardiac cancer (CGC). Cardiac cancer is related to obesity and reflux esophagitis in the Western population, whereas most non-cardiac cancers are related to Helicobacter pylori infection. The World Health Organization classifies H pylori as a class I carcinogen, which is the most important risk factor for gastric cancer [19]. Nearly 90% of distal gastric cancers can be attributed to H pylori infection [20]. Countries with a high incidence of gastric cancer are related to high H pylori seroprevalence rates, such as South Korea [21], China [22] and Japan [23]. The incidence rate of gastric cancer is relatively low in some countries, such as South Asia and Africa, whereas the seroprevalence of H pylori is very high [3]. Better food preservation practices and refrigeration during the transportation and storage of food have decreased the risk of developing gastric cancer [24]. Other risk factors for gastric cancer include smoking, low intake of fruits and vegetables, and a high intake of salt-preserved foods and possibly alcohol [25, 26].
In contrast to the overall declining incidence, an increasing incidence has been observed in populations younger than 50 years in the USA [27, 28] and the UK [29]. The historical incidence trends in these countries are mainly affected by cardiac cancer. The increase in cardiac cancer is related to an increase in the obesity level. The USA and UK are high-income countries with the highest obesity rates in adults, children, and adolescents, which is a public health concern [30]. This study found that, contrary to the declining trend of the overall incidence rate, the incidence rate of people younger than 45 years in some countries showed an increasing trend, especially in countries with a low incidence rate, including the UK, USA, and the Netherlands.
A recent global study showed that the mortality rate decreased faster than the incidence rate owing to improved socioeconomic status and better access to diagnostics and treatment [31]. Early gastric cancer rarely causes symptoms, and early screening still faces many challenges. Although Japan and South Korea are two high-risk countries, their survival rates are relatively high (> 60%) owing to their great efforts in early screening. Although the implementation of population-based screening in high-risk areas has shown some benefits, whether it will translate into a real reduction in mortality need to be further confirmed [32, 33]. We observed an increasing trend in populations younger than 45 years in some countries, including the USA, the UK, and other developed countries. Moreover, the mortality rate in Thailand has increased significantly in the past decade, which may be related to the low level of economic development and screening rate for early gastric cancer. Therefore, more attention should be paid to the population with gastric cancer in Thailand and those younger than 45 years of age.
A previous study [15] has used global high-quality data to predict whether gastric cancer may become a "rare" disease. This rare cancer threshold was defined in previous studies as cervical cancer (set at less than six cases per 100,000 population) [34]. To our knowledge, this study is also the first attempt to characterize future trends in gastric cancer mortality from a global perspective. Based on the mortality threshold of 6 cases per 100,000 population, those above this threshold can be regarded as high-mortality cancer. Although it is predicted that mortality will continue to decrease in most countries until 2035, gastric cancer is still a high mortality cancer in some countries. The absolute number of deaths is expected to further increase by 2035 as a result of population growth and aging, making gastric cancer a major public health challenge in some world regions.
The prevention of gastric cancer mainly focused on primary prevention and secondary prevention. Primary prevention strategies that can reduce the risk of gastric cancer include dietary modification such as decreasing the intake of salty foods, increasing the intake of fruits and vegetables, avoiding smoking, high alcohol consumption [1, 35,36,37,38], and refrigeration or chemical preservation of foods [36]. Identifying Helicobacter pylori-infected individuals at high risk for gastric cancer presents an opportunity for primary prevention. A meta-analysis of twenty-four studies [39] demonstrated that Helicobacter pylori eradication reduces gastric cancer incidence by 47%. A randomized controlled trial in South Korea [40] demonstrated a 55% reduction in incidence of gastric cancer after Helicobacter pylori eradication. Secondary prevention mainly involves endoscopic screening. Four studies [41,42,43,44] demonstrated endoscopic screeningr educe gastric cancer-specific mortality ranging from 42–67%.Two studies [42, 43] from Japan found endoscopic screening were superior in reducing gastric cancer-specific mortality compared with radiographic screening. The odds ratio (OR) of gastric cancer specific mortality among screened subjects compared to never-screened individuals was 0.53 (95% CI: 0.51–0.56) in a South Korea study [33].
Our study had several limitations. First, it is very important to distinguish non-cardiac cancer (NCGC) and cardiac cancer (CGC) from etiology; however, the existing data do not support a stratified analysis of incidence and mortality trends. Second, as the database lacks data on the risk factors associated with gastric cancer, we are unable to provide one table of risk factors that are associated with the emergence of gastric cancer.The influence of Helicobacter pylori infection, obesity, smoking, and other risk factors on gastric cancer incidence and mortality were not analyzed. Finally, the model used in this study to predict mortality was based on past data; therefore, there was a certain degree of uncertainty.
In the past decade, gastric cancer incidence and mortality have shown a decreasing trend, but there are still some countries showing an increasing trend, especially among populations younger than 45 years of age. Although mortality in most countries is predicted to decline by 2035, the absolute number of deaths due to gastric cancer may further increase due to population growth, making gastric cancer a major public health challenge in some countries. Changes in the epidemiology of gastric cancer require further analysis for cancer control. This study will also aid in the planning and decision-making related to gastric cancer control strategies.
Availability of data and materials
All data were retrieved from country-specific registries based on the Cancer Incidence in Five Continents (CI5) volumes I-XI (16)(https://gco.iarc.fr/overtime/en) and the World Health Organization (WHO) mortality database (https://platform.who.int/mortality).
This public database is open, and the use of data does not require additional consent.
Abbreviations
- WHO:
-
World Health Organization
- CI5plus:
-
Five Continents Plus
- AAPC:
-
The average annual percent change
- WHO:
-
World Health Organization
References
Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. https://doi.org/10.3322/caac.21660.
Sitarz R, Skierucha M, Mielko J, et al. Gastric cancer: epidemiology, prevention, classification, and treatment. Cancer Manag Res. 2018;10:239–48. https://doi.org/10.2147/CMAR.S149619.
Luo G, Zhang Y, Guo P, et al. Global patterns and trends in stomach cancer incidence: Age, period and birth cohort analysis. Int J Cancer. 2017;141(7):1333–44. https://doi.org/10.1002/ijc.30835.
Ahmed N. 23 years of the discovery of Helicobacter pylori: is the debate over? Ann Clin Microbiol Antimicrob. 2005;4:17. https://doi.org/10.1186/1476-0711-4-17.
Rawla P, Barsouk A. Epidemiology of gastric cancer: global trends, risk factors and prevention. Prz Gastroenterol. 2019;14(1):26–38. https://doi.org/10.5114/pg.2018.80001.
Ladeiras-Lopes R, Pereira AK, Nogueira A, et al. Smoking and gastric cancer: systematic review and meta-analysis of cohort studies. Cancer Causes Control. 2008;19(7):689–701. https://doi.org/10.1007/s10552-008-9132-y.
Tramacere I, Negri E, Pelucchi C, et al. A meta-analysis on alcohol drinking and gastric cancer risk. Ann Oncol. 2012;23(1):28–36. https://doi.org/10.1093/annonc/mdr135.
Tsugane S. Salt, salted food intake, and risk of gastric cancer: epidemiologic evidence. Cancer Sci. 2005;96(1):1–6. https://doi.org/10.1111/j.1349-7006.2005.00006.x.
Liu H, Hua Y, Zheng X, et al. Effect of coffee consumption on the risk of gastric cancer: a systematic review and meta-analysis of prospective cohort studies. PLoS One. 2015;10(5):e0128501. https://doi.org/10.1371/journal.pone.0128501.
Hansson LE, Nyren O, Hsing AW, et al. The risk of stomach cancer in patients with gastric or duodenal ulcer disease. N Engl J Med. 1996;335(4):242–9. https://doi.org/10.1056/NEJM199607253350404.
Wu AH, Tseng CC, Bernstein L. Hiatal hernia, reflux symptoms, body size, and risk of esophageal and gastric adenocarcinoma. Cancer. 2003;98(5):940–8. https://doi.org/10.1002/cncr.11568.
Ye W, Chow WH, Lagergren J, et al. Risk of adenocarcinomas of the esophagus and gastric cardia in patients with gastroesophageal reflux diseases and after antireflux surgery. Gastroenterology. 2001;121(6):1286–93. https://doi.org/10.1053/gast.2001.29569.
Takeno S, Hashimoto T, Maki K, et al. Gastric cancer arising from the remnant stomach after distal gastrectomy: a review. World J Gastroenterol. 2014;20(38):13734–40. https://doi.org/10.3748/wjg.v20.i38.13734.
Henderson TO, Oeffinger KC, Whitton J, et al. Secondary gastrointestinal cancer in childhood cancer survivors: a cohort study. Ann Intern Med. 2012;156(11):757–66, W−260. https://doi.org/10.7326/0003-4819-156-11-201206050-00002.
Arnold M, Park JY, Camargo MC, et al. Is gastric cancer becoming a rare disease? A global assessment of predicted incidence trends to 2035. Gut. 2020;69(5):823–9. https://doi.org/10.1136/gutjnl-2019-320234.
Bray F, Ferlay J, Laversanne M, et al. Cancer Incidence in Five Continents: Inclusion criteria, highlights from Volume X and the global status of cancer registration. Int J Cancer. 2015;137(9):2060–71. https://doi.org/10.1002/ijc.29670.
Moller B, Fekjaer H, Hakulinen T, et al. Prediction of cancer incidence in the Nordic countries: empirical comparison of different approaches. Stat Med. 2003;22(17):2751–66. https://doi.org/10.1002/sim.1481.
Ang T L, Fock K M. Clinical epidemiology of gastric cancer [J]. Singapore Med J, 2014, 55(12): 621–8. https://doi.org/10.11622/smedj.2014174.
World Health Organization International Agency For Research On Cancer. Schistosomes, liver flukes and Helicobacter pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 7–14 June 1994. IARC Monogr Eval Carcinog Risks Hum. 1994;61:1–241
Plummer M, Franceschi S, Vignat J, et al. Global burden of gastric cancer attributable to Helicobacter pylori. Int J Cancer. 2015;136(2):487–90. https://doi.org/10.1002/ijc.28999.
Yim JY, Kim N, Choi SH, et al. Seroprevalence of helicobacter pylori in South Korea. Helicobacter. 2007;12(4):333–40. https://doi.org/10.1111/j.1523-5378.2007.00504.x.
Wang KJ, Wang RT. Meta-analysis on the epidemiology of Helicobacter pylori infection in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2003;24(6):443–6.
Fujisawa T, Kumagai T, Akamatsu T, et al. Changes in seroepidemiological pattern of Helicobacter pylori and hepatitis A virus over the last 20 years in Japan. Am J Gastroenterol. 1999;94(8):2094–9. https://doi.org/10.1111/j.1572-0241.1999.01283.x.
Boeing H. Epidemiological research in stomach cancer: progress over the last ten years. J Cancer Res Clin Oncol. 1991;117(2):133–43. https://doi.org/10.1007/BF01613137.
Praud D, Rota M, Pelucchi C, et al. Cigarette smoking and gastric cancer in the Stomach Cancer Pooling (StoP) Project [J]. Eur J Cancer Prev. 2018;27(2):124–33. https://doi.org/10.1097/CEJ.0000000000000290.
Rota M, Pelucchi C, Bertuccio P, et al. Alcohol consumption and gastric cancer risk-A pooled analysis within the StoP project consortium. Int J Cancer. 2017;141(10):1950–62. https://doi.org/10.1002/ijc.30891.
Anderson WF, Rabkin CS, Turner N, et al. The changing face of noncardia gastric cancer incidence among US non-hispanic whites. J Natl Cancer Inst. 2018;110(6):608–15. https://doi.org/10.1093/jnci/djx262.
Camargo MC, Anderson WF, King JB, et al. Divergent trends for gastric cancer incidence by anatomical subsite in US adults. Gut. 2011;60(12):1644–9. https://doi.org/10.1136/gut.2010.236737.
Hooi JKY, Lai WY, Ng WK, et al. Global prevalence of helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology. 2017;153(2):420–9. https://doi.org/10.1053/j.gastro.2017.04.022.
Collaboration N C D R F. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults [J]. Lancet, 2017, 390(10113): 2627–42. https://doi.org/10.1016/S0140-6736(17)32129-3.
GBDSC Collaborators. The global, regional, and national burden of stomach cancer in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):42–54. https://doi.org/10.1016/S2468-1253(19)30328-0.
Hamashima C, Systematic Review G. Guideline development group for gastric cancer screening G. Update version of the Japanese guidelines for gastric cancer screening. Jpn J Clin Oncol. 2018;48(7):673–83. https://doi.org/10.1093/jjco/hyy077.
Jun J K, Choi K S, Lee H Y, et al. Effectiveness of the Korean National Cancer Screening Program in Reducing Gastric Cancer Mortality [J]. Gastroenterology, 2017, 152(6): 1319–28 e7.https://doi.org/10.1053/j.gastro.2017.01.029.
Simms KT, Steinberg J, Caruana M, et al. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020–99: a modelling study. Lancet Oncol. 2019;20(3):394–407. https://doi.org/10.1016/S1470-2045(18)30836-2.
Catalano V, Labianca R, Beretta GD, et al. Gastric cancer. Crit Rev Oncol Hematol. 2009;71(2):127–64. https://doi.org/10.1016/j.critrevonc.2009.01.004.
Nagini S. Carcinoma of the stomach: A review of epidemiology, pathogenesis, molecular genetics and chemoprevention. World J Gastrointest Oncol. 2012;4(7):156–69. https://doi.org/10.4251/wjgo.v4.i7.156.
Karimi P, Islami F, Anandasabapathy S, et al. Gastric cancer: descriptive epidemiology, risk factors, screening, and prevention. Cancer Epidemiol Biomarkers Prev. 2014;23(5):700–13. https://doi.org/10.1158/1055-9965.EPI-13-1057.
Cheng XJ, Lin JC, Tu SP. Etiology and prevention of gastric cancer. Gastrointest Tumors. 2016;3(1):25–36. https://doi.org/10.1159/000443995.
Lee Y C, Chiang T H, Chou C K, et al. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis [J]. Gastroenterology, 2016, 150(5): 1113–24 e5.https://doi.org/10.1053/j.gastro.2016.01.028.
Choi IJ, Kim CG, Lee JY, et al. Family history of gastric cancer and helicobacter pylori treatment. N Engl J Med. 2020;382(5):427–36. https://doi.org/10.1056/NEJMoa1909666.
Hosokawa O, Miyanaga T, Kaizaki Y, et al. reased death from gastric cancer by endoscopic screening: association with a population-based cancer registry. Scand J Gastroenterol. 2008;43(9):1112–5. https://doi.org/10.1080/00365520802085395.
Hamashima C, Ogoshi K, Narisawa R, et al. Impact of endoscopic screening on mortality reduction from gastric cancer. World J Gastroenterol. 2015;21(8):2460–6. https://doi.org/10.3748/wjg.v21.i8.2460.
Hamashima C, Shabana M, Okada K, et al. Mortality reduction from gastric cancer by endoscopic and radiographic screening. Cancer Sci. 2015;106(12):1744–9. https://doi.org/10.1111/cas.12829.
Kim H, Hwang Y, Sung H, et al. Effectiveness of gastric cancer screening on gastric cancer incidence and mortality in a community-based prospective cohort. Cancer Res Treat. 2018;50(2):582–9. https://doi.org/10.4143/crt.2017.048.
Acknowledgements
We thank all members of WHO.
Funding
This study was supported by Fujian Research and Training Grants for Young and Middle-aged Leaders in Healthcare (No.【2022】954) and Fujian third batch of "Innovation star" talent project (No.【2022】22.
Author information
Authors and Affiliations
Contributions
Concept and design: Ju-Li Lin, Ping Li. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Ju-Li Lin, Ping Li. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: Ju-Li Lin, Jian-Xian Lin, Guang-Tan Lin. Administrative, technical, or material support: Ju-Li Lin, Chao-Hui Zheng, Ping Li, Jian-Wei Xie, Jia-bin Wang, Jun Lu, Qi-Yue Chen, Chang-Ming Huang.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Our study did not involve humans or experiments, and it therefore required no ethical approvals.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Lin, JL., Lin, JX., Lin, GT. et al. Global incidence and mortality trends of gastric cancer and predicted mortality of gastric cancer by 2035. BMC Public Health 24, 1763 (2024). https://doi.org/10.1186/s12889-024-19104-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-19104-6