
Abstract
Background
HIV molecular epidemiology (HIV ME) can support the early detection of emerging clusters of new HIV infections by combining HIV sequence data routinely obtained during the clinical treatment of people living with HIV with behavioral, geographic, and sociodemographic information. While information about emerging clusters promises to facilitate HIV prevention and treatment efforts, the use of this data also raises several ethical concerns. We sought to assess how those working on the frontlines of HIV ME, specifically public health practitioners (PHPs) and researchers, prioritized these issues.
Methods
Ethical issues were identified through literature review, qualitative in-depth interviews, and stakeholder engagement. PHPs and researchers using HIV ME prioritized the issues using best–worst scaling (BWS). A balanced incomplete block design was used to generate 11 choice tasks each consisting of a sub-set of 5 ethical concerns. In each task, respondents were asked to assess the most and least concerning issue. Data were analyzed using conditional logit, with a Swait-Louviere test of poolability. Latent class analysis was then used to explore preference heterogeneity.
Results
In total, 57 respondents completed the BWS experiment May–June 2023 with the Swait-Louviere test indicating that researchers and PHPs could be pooled (p = 0.512). Latent class analysis identified two classes, those highlighting “Harms” (n = 29) (prioritizing concerns about potential risk of legal prosecution, individual harm, and group stigma) and those highlighting “Utility” (n = 28) (prioritizing concerns about limited evidence, resource allocation, non-disclosure of data use for HIV ME, and the potential to infer the directionality of HIV transmission). There were no differences in the characteristics of members across classes.
Conclusions
The ethical issues of HIV ME vary in importance among stakeholders, reflecting different perspectives on the potential impact and usefulness of the data. Knowing these differences exist can directly inform the focus of future deliberations about the policies and practices of HIV ME in the United States.
Similar content being viewed by others


Background
HIV ME (HIV ME) is currently used in both research and public health activities related to HIV prevention, treatment, and surveillance in the United States. Molecular HIV surveillance (MHS) promises to facilitate the early detection of HIV transmission clusters, thereby allowing public health practitioners (PHPs) to implement targeted interventions. HIV ME has also been used to describe emerging epidemics [1, 2], drug-resistance dynamics [3,4,5,6,7], and to predict risk factors associated with transmission [8,9,10]. Furthermore, MHS is a key component in the Ending the HIV Epidemic in the U.S. (E.H.E.) initiative, which aims to reduce new HIV infections by 90% by 2030 [11, 12]. In the United States, MHS relies upon partial HIV gene sequence data obtained through HIV drug resistance testing, which is a common component of routine clinical care of individuals living with HIV.
While the U.S. Centers for Disease Control and Prevention (CDC) has stated that MHS has assisted in the detection of hundreds of growing transmission clusters across the country [13], its use in HIV surveillance has raised social and ethical concerns related to consent, privacy and confidentiality leading some to call for a moratorium on its use in public health [14, 15]. Some critics fear that MHS data may intersect with laws that criminalize HIV transmission or non-disclosure, while others express concern that identification and public disclosure of HIV transmission clusters may lead to increased risk of stigma and discrimination in affected communities [16,17,18,19,20,21,22,23,24]. In 2023, the Presidential Advisory Council on HIV/AIDS (PACHA) passed a resolution calling on public health agencies and others to take a variety of actions in response to such concerns [15]. These include meaningfully engaging with communities regarding MHS, gathering evidence on its use, obtaining consent from individuals for use of their HIV viral sequence data in public health, and addressing HIV criminalization laws [15].
Evidence is needed on the direct benefits of using HIV ME for public health purposes, including on interrupting or preventing HIV transmission, on intermediate outcomes (e.g., HIV testing, pre-exposure prophylaxis uptake, and viral suppression), and on outcomes for vulnerable populations [19, 24, 25]. The lack of evidence makes it challenging for stakeholders to weigh the benefits and risks of the practice. Moreover, no systematic evaluation has been done on how different stakeholders, such as researchers, public health practitioners (PHPs), persons living with HIV and persons living without HIV at increased risk of acquiring it, perceive the use of HIV ME and its implications. To begin to address this knowledge gap, one study explored the views and attitudes of persons living with HIV and persons living without HIV at risk of acquiring it towards HIV ME and recommended further systematic data collection from key stakeholders to inform policymaking and practice in HIV ME [26].
We sought to assess how PHPs and researchers using HIV ME in the United States prioritize the associated ethical issues. There is value in understanding how stakeholders prioritize ethical concerns as they can and should promote a more informed discussion between researchers, PHPs, and other stakeholders about the future policies and practices on the appropriate uses of HIV ME. Similarly, there is value in understanding how different methods such as emerging choice experiment methods can be used to assess ethical concerns and to study differences among various types of professionals using molecular epidemiology.
Methods
Methods of identification
The identification of ethical issues surrounding the use of HIV ME in public health and research was informed by the peer-reviewed and grey literature, engagement with HIV ME experts in in public health and research, and the results of earlier qualitative interviews with persons living with HIV and persons living without HIV at increased risk of acquiring it [26]. Six expert stakeholders were selected based on their leadership, and active roles in publishing and providing guidance on the methods, application, and ethical considerations related to using HIV ME in both research and public health contexts. These stakeholders provided input on the relevant ethical issues to be considered in our study. This process resulted in a list and brief description of 11 candidate ethical issues to include in the BWS experiment. Table 1 presents the final list of objects included in the BWS experiment.
Method for prioritization
Best–worst scaling (BWS) was used to prioritize the ethical issues [30]. BWS uses an experimental design to generate choice tasks comprised of subsets of objects (i.e., ethical issues) [31, 32]. Then respondents assess what is the best and worst object in a choice set. BWS experiments have advantages over other prioritization methods such as Likert scales [32,33,34] and was chosen because of its simplicity, low respondent burden, and strengths in measuring priorities [35, 36]. BWS is increasingly used to assess the priorities of a wide array of stakeholders in medicine [37] and in other fields [38].
Survey instrument
The survey instrument followed good research practices [39] and began with an introductory section that provided relevant contextual information. The introduction informed participants of the study’s purpose, that their participation was voluntary, and that their individual responses would be kept confidential. The introduction also provided a definition of HIV ME and its uses in research or public health for HIV prevention, treatment, or surveillance in the United States. The next section of the survey collected information about participants, including about their field of work, number of years working in their field, and institutional location.
The BWS instrument within the survey was developed specifically for this study and included two parts (Supplementary material). The first was an orientation exercise used to explain each ethical issue and to ask about which issues were a relevant concern (yes/no). The purpose of the orientation exercise was to encourage respondents to read the descriptions for each issue and not to provide data for analysis. The second part elicited priorities of the ethical issues using a series of 11 BWS choice tasks, each of which consisted of a sub-set of 5 ethical issues. All the ethical issues were phrased in the negative to avoid response bias due to directionality of phrasing. The underlying latent, subjective continuum was degree of concern, where each choice set was introduced by the statement: “Please choose the most concerning and then the least concerning ethical issue when using HIV ME for research or public health in the United States.” The choice tasks were introduced using an example task (Fig. 1). A balanced incomplete block design was used to generate the 11 choice tasks where each ethical issue occurred and co-occurred with other issues the same number of times.

Example BWS choice task
Survey development
The survey development process included pre-testing and piloting to assess the instrument’s burden as well as to ensure content validity and relevance to potential respondents [39]. The expert stakeholders were further engaged in virtual pre-testing interviews that included the think-aloud technique and lasted an average of 60 min. Stakeholders reviewed the survey overall and the descriptions of the ethical issues specifically. Interviewers probed the salience of each ethical issue as well as the accuracy and clarity of their descriptions during pretesting. Pre-testers were asked about the amount of time participants would need to complete the survey and whether other information should be collected about the respondents or whether other ethical issues should be considered. The survey instrument was revised based on pre-testers’ insights and perspectives, including revisions to the labels and descriptions of ethical issues.
A pilot survey was then designed and programmed in Qualtrics (Qualtrics, Provo, Utah). Ten individuals from the study team and the expert stakeholder group piloted the survey to assess its functionality and feasibility. Based on qualitative feedback and quantitative analysis of results from the pilot, the survey was revised to improve its functionality on mobile devices and to improve the clarity of two descriptions. The final survey was programmed in Qualtrics.
Fielding the survey
We targeted respondents who conduct HIV ME research, and PHPs from U.S. public health departments who are: (1) leaders with oversight of HIV cluster detection and response programs that include molecular cluster detection, and (2) staff members responsible for implementing HIV molecular cluster detection and/or response.
Potential respondents were identified by their: (1) authorship of peer reviewed publications; (2) presentations at major HIV conferences; (3) leadership roles in national societies/centers; (4) publicly available lists of HIV-focused public health officials (e.g., lists from the National Alliance of State and Territorial AIDS Directors; and through (5) the project’s Expert Advisory Board members.
Potential respondents were invited to opt-in to participate via email from the project team directly or on behalf of the team through members of its Expert Advisory Board. The invitation to participate described the survey and its purpose as well as how the results would be used to inform future deliberations about the policies and practices of HIV ME. Potential respondents could opt-in to participate by providing their email address via a brief online survey. Individuals who opted-in to participate in the study were subsequently sent an individual online survey link administered via Qualtrics. The survey was fielded from May 16, 2023 to June 28, 2023. Respondents were not compensated for participating.
Data analysis
BWS scores were calculated by subtracting the number of times an object was selected as least concerning from the number of times it was selected as most concerning and then dividing each count by the total number of times the object appeared during the experiment. Conditional logistic analysis was conducted using a sequential best–worst choice assumption and stratified by researcher versus PHP. Effects coding was used for the conditional logit analysis. Importance scores were then calculated by rescaling coefficients from the conditional logit to a probability ratio scale that ranges from 0 to 100 [40]. The rescaled importance scores follow ratio scaling where, for example, an item with a score of 10 can be interpreted as being twice as concerning as an item with a score of 5. A Swait-Louviere test was used to test for the poolability of respondents [41].
Preference heterogeneity was assessed using latent class analysis [42], an approach that is increasingly used [43]. We used latent class conditional logit models to identify different groups or “classes” of individuals, with each class having distinct preferences. This involves estimating parameters that determine which class a given individual is likely to be a member of [44]. For each class, a separate conditional logit model is estimated. Wald tests were used to test differences in specific coefficients between the classes. We also used chi-square tests to examine the association between class membership and respondent characteristics. A key aspect of this exploration included assessing whether the location of participants’ institutions, specifically in states with HIV or sexually transmitted infection (STI) criminalization laws, had an association with class membership. To facilitate this, we sourced data from the U.S. CDC regarding state-specific criminalization laws related to HIV and STIs [45]. Next participants were categorized into two groups: (i) those in states without specific criminalization laws; and (ii) those in states with laws that either criminalize STIs or infectious diseases that might include HIV, or specifically target HIV exposure or actions that could potentially expose another person to HIV [45]. All data analysis was conducted with Stata SE version 17 (StataCorp LLC).
Oversight
The expert stakeholder engagement that guided survey development was deemed non-human subjects research by the Johns Hopkins School of Medicine (JHM #IRB IRB00354016). The survey was deemed non-human subject research by the Ohio State University College of Medicine Institutional Review Board (OSU IRB #2022E1207). As such, explicit informed consent was not required. However, the survey introduction provided information about the nature of the survey questions, the expected time required to answer them, that participation was voluntary, that individual responses would be treated confidentially, and the survey could be stopped at any time. Next, was a statement: “If you are willing to participate, please click the ‘Next’ button at the bottom of this page.” An advisory board also provides oversight to the project overall.
Results
In total, 90 professionals opted-in to receive the survey; 57 completed it, including 29 researchers and 28 PHPs. The respondents differed in the number of years they reported working in their respective field; one half (50.0%) of PHPs had worked in their field more than 10 years while over two-thirds (69%) of researchers had worked in their field for over 10 years. All researchers had experience with HIV ME in the U.S. and most (60.7%) conducted research with a focus solely on the U.S. setting. PHPs represented 22 public health jurisdictions from across the United States.
The results of the Swait-Louviere test failed to reject the null hypothesis (p = 0.512) that the estimated parameters between researchers and PHPs were the same. This indicated that the data from these two groups could be pooled. In the pooled analysis, respondents prioritized legal prosecution, group stigma, and individual harm the most, and limited resources, data re-use, and lack of an opt-out option the least (Table 2).
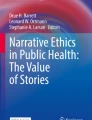
Latent class analysis revealed heterogeneity of priorities (as reported by importance scores) clustered in two groups: a “Harms” group (n = 29) who prioritized concerns about potential risk of legal prosecution (p < 0.001), individual harms (p < 0.001), and group stigma (p = 0.002); and a “Utility” group (n = 28) who prioritized concerns about limited evidence of benefits (p < 0.001), uncertain impact on resource allocation (p < 0.001), lack of routinely disclosing use of data (p = 0.045), and the potential to infer the directionality of HIV transmission (p = 0.022). The two groups differed significantly in how they prioritized seven ethical issues (Fig. 2). There were no statistically significant differences in the characteristics of members across classes (Table 3).

Differences in endorsing ethical issues by latent class membership (2-class model). aImportance scores calculated by rescaling coefficients from conditional logit on a ratio scale from 0 to 100. With ratio scaling an item with a score of 10, for example, can be interpreted as being twice as concerning as an item with a score of 5
Discussion
We have explored the ethical issues related to HIV ME by using BWS to elicit the priorities of PHPs and researchers who use HIV ME in their work. Our results revealed two distinct perspectives on the ethical issues: one emphasizing the potential harms to individuals and groups, and the other emphasizing the utility and effectiveness of the approach. These findings relate directly to the increased attention on addressing the ethical issues of using HIV ME in research and public health in the United States. This includes recently revised guidelines from the CDC [46] as well as four proposals presented for federal stakeholders to consider regarding molecular HIV surveillance programs, including recommendations about incorporating opt-outs and plain-language notifications about the use of HIV viral sequence information for public health purposes [29]. Despite these recommendations, other researchers have reported general support and limited concerns about the use of HIV ME in public health and research among persons living with HIV and persons living without HIV at increased risk of acquiring it [26] – evidence that contrasts with the concerns raised by some critics of HIV ME. These findings highlighted the importance of engaging with a diversity of stakeholders, including those who may not have been previously engaged as widely.
Our study contributes to this important and ongoing conversation by presenting the preferences of two groups of professionals not previously engaged systematically. Our results indicated that the preferences of the two groups – researchers and PHPs – were similar enough to be pooled and analyzed using a joint model. The aggregated importance scores showed that the potential added risk of legal prosecution was the most concerning ethical issue and was more than five times as influential as the uncertain impact on the allocation of limited resources, which was the least concerning issue. The prioritization of added risk of legal prosecution is consistent with prior work that has identified this issue as a main ethical concern of using HIV ME [16, 17, 24, 27, 29]. Legal prosecution refers to the risk of using HIV genetic data as evidence in criminal cases against people living with HIV who are accused of transmitting or exposing others to HIV. This practice has been widely criticized for being discriminatory, stigmatizing, and undermining public health efforts to prevent and treat HIV [27]. It was unexpected that the uncertain impact of HIV ME on the allocation of limited resources was the least prioritized issue given that this issue has been discussed at PACHA meetings [15]. One possible explanation is that our participants did not perceive this issue as directly relevant to their work or interests, or that they assumed that HIV ME would not significantly affect the resource allocation decisions.
While we did not expect the preferences of researchers and PHPs to be poolable, there was significant heterogeneity among respondents, where latent class analysis identified two distinct classes of participants. While the classes were not associated with profession or other observable characteristics, the ethical issues prioritized by each class seemed to reflect a coherent and consistent set of values and concerns. The “Harms” class focused on the issues that could cause social harm to individuals or groups who are affected by the actions – inadvertent or not – that result from the use of HIV ME. The Harms class may have a stronger sense of responsibility to the people living with HIV or at risk of HIV infection and may be more sensitive to the potential negative consequences of HIV ME on their rights and well-being. The Utility class focused on issues that could affect the scientific quality and credibility of HIV ME – issues related to principles of scientific integrity, transparency, and accountability, which are essential for ensuring the validity and reliability of research and public health interventions. The Utility class members may have a higher expectation and demand for HIV ME to demonstrate its value and utility for improving HIV prevention and care outcomes; they may be more skeptical of the benefits of HIV ME and more critical of the limitations and uncertainties of HIV ME.
It is critical to understand how stakeholders prioritize relevant ethical concerns to enable the weighing of benefits versus risks and related tasks of formulating and revising research and public health guidelines. By aligning new and updated guidelines with stakeholders’ priorities and preferences, we stand to enhance their effectiveness. For instance, insights from our study relate to the efforts undertaken by interdisciplinary working groups to improve the ethical conduct of HIV phylogenetic research [47]. These working groups identified critical issues such as study design, data security, access, and sharing; community engagement; and communication and dissemination. Studies such as ours can help recognize which of these issues matter most to stakeholders and can inform the decisions that address them. Similarly, insights from our study could further inform the CDC’s guidance for health departments conducting cluster detection and response, which the CDC updated in February 2024 [46]. The CDC indicated that its new guidance incorporates input from HIV and human rights organizations who sent a letter about their concerns with molecular HIV surveillance [48], including concerns considered by our study such as individual consent and opt-out. In summary, stakeholders’ priorities play a pivotal role in shaping policy decisions and the ethical landscape of HIV-related research.
This study presented some unique challenges. There is a small and finite number of researchers and PHPs involved in HIV ME. This is a particular issue with the U.S. public health workforce, especially in the context of the COVID-19-related burnout [49]. A recent study found that nearly half of all public health workers in state and local agencies left their jobs between 2017 and 2021, creating many vacancies [50]. Moreover, there are limited ways to identify PHPs who work in U.S. public health departments. These factors influenced our approach to recruitment. We carefully considered expanding the scope of our survey by inviting a broader range of participants. However, after thoughtful deliberation, we decided against it. Our concern was that doing so could introduce too much heterogeneity and bias the results to the null. Instead, we intentionally focused on a specific population of professionals who possessed the technical skills for conducting HIV ME or applying it in public health. Importantly, we recognize that this population is both small and finite. Our survey, however, posed questions about ethical issues that may not necessarily be apparent to all those with the technical skills to conduct or apply it. The professionals who participated in our survey therefore constitute a unique population. They not only possess the technical skills and knowledge to conduct or apply HIV ME, but also demonstrate the expertise to consider its broader context. By engaging this population, our survey is among the first to systematically and comprehensively capture the perspectives of professionals who can meaningfully contribute to discussions on ethical matters within this field.
We faced interesting questions in determining the appropriate survey framework. Initially, our focus was centered on the technologies used for HIV ME. However, through engaging with expert stakeholders we realized that this approach was too narrow in scope. Additionally, we deliberated on how to effectively present the ethical issues associated with HIV ME, enabling researchers and PHPs to thoroughly consider these issues. This was particularly important when the issues highlighted differences in existing rules, norms, and practices between the groups such as around disclosing use of information, obtaining individual consent, and providing opt-out options. For example, research use of HIV ME typically involves enrolling individuals into research studies via informed consent and provides opportunities to opt-out. In contrast, individual consent and opt-out is not typical in public health practice. Input from our expert stakeholders was critical for refining how these issues were described while supporting our intention to understand similarities and divergences in perspectives that could inform, and shape future discussions related to the policies and practices of HIV ME.
Another challenge related to the staged implementation of molecular HIV surveillance where public health departments have not implemented molecular HIV surveillance at the same time. For instance, some public health departments implemented it several years ago when the CDC first piloted the initiative and others are only beginning the implementation process. Therefore, PHPs have varied experiences with HIV ME depending on their public health jurisdiction. Our survey was not designed to account for these types of variations in PHPs’ experience.
When contemplating whether to compensate survey respondents, our team accounted for the fact that individuals employed at U.S. public health departments are ineligible to receive incentives for their participation. We recognized that compensating only some participants while excluding others based on their workplace would be inequitable. So, after thoughtful deliberation, we decided not to provide compensation to any of the participants. Ethical considerations surrounding participant compensation are of critical importance in research and survey studies. Offering compensation is a common practice to acknowledge the time and effort invested by participants and promote a fair exchange between researchers and the individuals contributing their valuable insights. While our decision excluded compensation for all participants, we had a decent response rate and believe the approach reduced any perceived favoritism or unequal treatment and reinforced the integrity of the study.
This study demonstrates the usefulness of BWS to systematically explore the ethical issues associated with the use of HIV ME in the United States. We found heterogeneity among respondents in their prioritization of ethical issues reflecting their different perspectives and priorities on the potential social harms and scientific utility of the data. Knowing these differences exist can shape future deliberations on policies and practices of HIV ME to address these ethical issues. Future studies should use BWS to examine the perspectives of additional stakeholders, including persons living with HIV and persons living without HIV at increased risk of acquiring it, to ensure their voices are represented in all discussions about the policies and practices of HIV ME.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Khanani MR, Somani M, Rehmani SS, Veras NM, Salemi M, Ali SH. The spread of HIV in Pakistan: bridging of the epidemic between populations. PLoS One. 2011;6(7):e22449. https://doi.org/10.1371/journal.pone.0022449.
Wang X, Wu Y, Mao L, et al. Targeting HIV prevention based on molecular epidemiology among deeply sampled subnetworks of men who have sex with men. Clin Infect Dis. 2015;61(9):1462–8. https://doi.org/10.1093/cid/civ526.
Brooks JI, Niznick H, Ofner M, Merks H, Angel JB. Local phylogenetic analysis identifies distinct trends in transmitted HIV drug resistance: implications for public health interventions. BMC Infect Dis. 2013;13:509. https://doi.org/10.1186/1471-2334-13-509.
Kühnert D, Kouyos R, Shirreff G, et al. Quantifying the fitness cost of HIV-1 drug resistance mutations through phylodynamics. PLoS Pathog. 2018;14(2):e1006895. https://doi.org/10.1371/journal.ppat.1006895.
Panichsillapakit T, Smith DM, Wertheim JO, Richman DD, Little SJ, Mehta SR. Prevalence of transmitted HIV drug resistance among recently infected persons in San Diego, CA 1996–2013. J Acquir Immune Defic Syndr. 2016;71(2):228–36. https://doi.org/10.1097/qai.0000000000000831.
Poon AF, Aldous JL, Mathews WC, et al. Transmitted drug resistance in the CFAR network of integrated clinical systems cohort: prevalence and effects on pre-therapy CD4 and viral load. PLoS One. 2011;6(6):e21189. https://doi.org/10.1371/journal.pone.0021189.
Poon AF, Joy JB, Woods CK, et al. The impact of clinical, demographic and risk factors on rates of HIV transmission: a population-based phylogenetic analysis in British Columbia, Canada. J Infect Dis. 2015;211(6):926–35. https://doi.org/10.1093/infdis/jiu560.
Lewis F, Hughes GJ, Rambaut A, Pozniak A, Leigh Brown AJ. Episodic sexual transmission of HIV revealed by molecular phylodynamics. PLoS Med. 2008;5(3):e50. https://doi.org/10.1371/journal.pmed.0050050.
Ragonnet-Cronin M, Jackson C, Bradley-Stewart A, et al. Recent and rapid transmission of HIV among people who inject drugs in Scotland revealed through phylogenetic analysis. J Infect Dis. 2018;217(12):1875–82. https://doi.org/10.1093/infdis/jiy130.
Ratmann O, van Sighem A, Bezemer D, et al. Sources of HIV infection among men having sex with men and implications for prevention. Sci Transl Med. 2016;8(320):320ra2. https://doi.org/10.1126/scitranslmed.aad1863.
Beyrer C, Adimora AA, Hodder SL, et al. Call to action: how can the US Ending the HIV Epidemic initiative succeed? Lancet. 2021;397(10279):1151–6. https://doi.org/10.1016/s0140-6736(21)00390-1.
Fauci AS, Redfield RR, Sigounas G, Weahkee MD, Giroir BP. Ending the HIV epidemic: a plan for the United States. JAMA. 2019;321(9):844–5. https://doi.org/10.1001/jama.2019.1343.
US Centers for Disease Control and Prevention. HIV cluster and outbreak detection and response. https://www.cdc.gov/hiv/programresources/guidance/cluster-outbreak/index.html#:%7E:text=Molecular%20data%20analysis%20can%20help%20detect%20HIV%20clusters%20and%20outbreaks,had%20not%20been%20previously%20recognized. Accessed 20 Sept 2023.
US PLHIV Caucus. Open letter to the CDC networks of people living with HIV demand a moratorium on molecular HIV surveillance. https://actionnetwork.org/forms/open-letter-to-the-cdc-we-demand-a-moratorium-on-molecular-hiv-surveillance. Accessed 20 Sept 2023.
Presidential Advisory Council on HIV/AIDS (PACHA). Molecular HIV surveillance and cluster detection and response resolution. https://files.hiv.gov/s3fs-public/2022-11/PACHA-resolution-on-Molecular-HIV-Surveillance-Cluster-Detection-and-Response-10-17-22.pdf. Accessed 20 Sept 2023.
Molldrem S, Smith AKJ. Reassessing the ethics of molecular HIV surveillance in the era of cluster detection and response: toward HIV data justice. Am J Bioeth. 2020;20(10):10–23. https://doi.org/10.1080/15265161.2020.1806373.
Schairer C, Mehta SR, Vinterbo SA, Hoenigl M, Kalichman M, Little S. Perceptions of molecular epidemiology studies of HIV among stakeholders. J Public Health Res. 2017;6(3):992. https://doi.org/10.4081/jphr.2017.992.
Schairer CE, Mehta SR, Vinterbo SA, Hoenigl M, Kalichman M, Little SJ. Trust and expectations of researchers and public health departments for the use of HIV molecular epidemiology. AJOB Empir Bioeth. 2019;10(3):201–13. https://doi.org/10.1080/23294515.2019.1601648.
Mehta SR, Schairer C, Little S. Ethical issues in HIV phylogenetics and molecular epidemiology. Curr Opin HIV AIDS. 2019;14(3):221–6. https://doi.org/10.1097/coh.0000000000000538.
Bernard EJ, McClelland A, Cardell B, et al. We are people, not clusters! Am J Bioeth. 2020;20(10):1–4. https://doi.org/10.1080/15265161.2020.1809550.
Rennie S, Sullivan K, Dennis A. HIV molecular epidemiology: tool of oppression or empowerment? Am J Bioeth. 2020;20(10):44–7. https://doi.org/10.1080/15265161.2020.1806392.
Watson M, Sweeney P. Furthering discussion of ethical implementation of HIV cluster detection and response. Am J Bioeth. 2020;20(10):24–6. https://doi.org/10.1080/15265161.2020.1806398.
Whitehead S. Critics worry government surveillance of HIV may hurt more than it helps. https://kffhealthnews.org/news/article/government-surveillance-hiv-criminalization-privacy-data-concerns/. Accessed 23 Sept 2023.
Nelson B. Questioning the benefits of molecular surveillance. https://www.poz.com/article/questioning-benefits-molecular-surveillance. Accessed 20 Sept 2023.
Oster AM, Lyss SB, McClung RP, et al. HIV cluster and outbreak detection and response: the science and experience. Am J Prev Med. 2021;61(5 Suppl 1):S130-s142. https://doi.org/10.1016/j.amepre.2021.05.029.
Bollinger JM, Geller G, May E, Brewer J, Henry LM, Sugarman J. Brief report: challenges in obtaining the informed perspectives of stakeholders regarding HIV molecular epidemiology. J Acquir Immune Defic Syndr. 2023;93(2):87–91. https://doi.org/10.1097/qai.0000000000003179.
McClelland A, Guta A, Gagnon M. The rise of molecular HIV surveillance: Implications on consent and criminalization. Crit Public Health. 2020;30(4):487–93. https://doi.org/10.1080/09581596.2019.1582755.
Lee LM, Heilig CM, White A. Ethical justification for conducting public health surveillance without patient consent. Am J Public Health. 2012;102(1):38–44. https://doi.org/10.2105/ajph.2011.300297.
Molldrem SS, Anthony KJ, McClelland A. Advancing dialogue about consent and molecular HIV surveillance in the United States: four proposals following a federal advisory panel’s call for major reforms. Milbank Q. 2023;101:1033–46. https://doi.org/10.1111/1468-0009.12663.
Guerrini CJ, Crossnohere NL, Rasmussen L, Bridges JFP. A best-worst scaling experiment to prioritize concern about ethical issues in citizen science reveals heterogeneity on people-level v. data-level issues. Sci Rep. 2021;11(1):19119. https://doi.org/10.1038/s41598-021-96743-4.
Louviere JJ, Flynn TN, Marley AAJ. Best-worst scaling: theory, methods and applications. Cambridge: Cambridge University Press; 2015.
Flynn TN, Louviere JJ, Peters TJ, Coast J. Best–worst scaling: what it can do for health care research and how to do it. J Health Econ. 2007;26(1):171–89.
Erdem S, Rigby D. Investigating heterogeneity in the characterization of risks using best worst scaling. Risk Anal. 2013;33(9):1728–48. https://doi.org/10.1111/risa.12012.
Mühlbacher AC, Kaczynski A, Zweifel P, Johnson FR. Experimental measurement of preferences in health and healthcare using best-worst scaling: an overview. Heal Econ Rev. 2016;6(1):1–14.
van Dijk JD, Groothuis-Oudshoorn CG, Marshall DA, IJzerman MJ. An empirical comparison of discrete choice experiment and best-worst scaling to estimate stakeholders’ risk tolerance for hip replacement surgery. Value Health. 2016;19(4):316–22. https://doi.org/10.1016/j.jval.2015.12.020.
Krucien N, Watson V, Ryan M. Is best-worst scaling suitable for health state valuation? A comparison with discrete choice experiments. Health Econ. 2017;26(12):e1–16. https://doi.org/10.1002/hec.3459.
Hollin IL, Paskett J, Schuster ALR, Crossnohere NL, Bridges JFP. Best-worst scaling and the prioritization of objects in health: a systematic review. Pharmacoeconomics. 2022;40(9):883–99. https://doi.org/10.1007/s40273-022-01167-1.
Schuster ALR, Crossnohere NL, Campoamor NB, Hollin IL, Bridges JFP. The rise of best-worst scaling for prioritization: a transdisciplinary literature review. J Choice Model. 2024;50:100466. https://doi.org/10.1016/j.jocm.2023.100466.
Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health–a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–13. https://doi.org/10.1016/j.jval.2010.11.013.
The MaxDiff System: Technical Paper. Sawtooth software. 2020.
Swait J, Louviere J. The role of the scale parameter in the estimation and comparison of multinomial logit models. J Mark Res. 1993;30(3):305–14. https://doi.org/10.1177/002224379303000303.
Pacifico D, Yoo HI. lclogit: a stata command for fitting latent-class conditional logit models via the expectation-maximization algorithm. Stata J. 2013;13(3):625–39.
Zhou M, Thayer WM, Bridges JFP. Using latent class analysis to model preference heterogeneity in health: a systematic review. Pharmacoeconomics. 2018;36(2):175–87. https://doi.org/10.1007/s40273-017-0575-4.
Deal K. Segmenting patients and physicians using preferences from discrete choice experiments. Patient. 2014;7(1):5–21. https://doi.org/10.1007/s40271-013-0037-9.
Centers for Disease Control and Prevention. HIV and STD criminalization laws. https://www.cdc.gov/hiv/policies/law/states/exposure.html. Accessed 1 Nov 2023.
U.S. Centers for Disease Control and Prevention. HIV CDR guidance for health departments. https://www.cdc.gov/hiv/programresources/guidance/hiv-cluster-detection-and-response-guidance/index.html. Accessed 16 Feb 2024.
Dawson L, Benbow N, Fletcher FE, et al. Addressing ethical challenges in US-based HIV phylogenetic research. J Infect Dis. 2020;222(12):1997–2006. https://doi.org/10.1093/infdis/jiaa107.
Ryan B. H.I.V. groups warn of privacy risks in how C.D.C tracks virus samples. The New York Times. https://www.nytimes.com/2024/02/09/health/hiv-molecular-surveillance-cdc.html?unlocked_article_code=1.UE0.kMYw.9KUUF4mLi9QU&smid=url-share. Accessed 16 Feb 2024.
Stone KW, Kintziger KW, Jagger MA, Horney JA. Public health workforce burnout in the COVID-19 response in the U.S. Int J Environ Res Public Health. 2021;18(8):4369. https://doi.org/10.3390/ijerph18084369.
Leider JPCB, Robbins M, Hare Bork R, Fraser M, Savoia E, Piltch-Loeb R, Koh HK. The exodus of state and local public health employees: separations started before and continued throughout COVID-19. Health Aff. 2023;42(3):338–48. https://doi.org/10.1377/hlthaff.2022.01251.
Acknowledgements
The authors thank our Project Team member, Sheethal Jose, for her helpful input and assistance with recruitment. We also thank our External Advisory Board for sharing their technical expertise with us: Antoine Chaillon, PhD, MD, MSc; Michael Kalichman, PhD, MApSc; Davey Smith, MD, MAS; Laramie Smith, PhD, URM Scholar, MA; Joel Wertheim, PhD; Danielle German, PhD, MPH; Kate Grabowski, PhD, MS; Oliver Laeyendecker, PhD, MBA, MS; Carl Latkin, PhD, MS; Joseph Margolick, PhD, MD; Shruti Mehta, PhD, MPH; and Alexandra Oster, MD.The authors especially thank our expert stakeholders and all of the study participants for sharing their time and perspectives with us.
Funding
Work on this project was supported by grant R01MH124590 (National Institutes of Mental Health). John FP Bridges also holds an Innovation in Regulatory Science Award from the Burroughs Wellcome Fund.
Author information
Authors and Affiliations
Contributions
SJL and JS conceived the study. ALRS and JFPB led development of the survey; all authors (ALRS, JB, GG, SJL, SRM, TS, JS, JFPB) contributed to critical revisions of the survey. ALRS fielded the survey, conducted data analyses, prepared tables and figures, and led writing of the manuscript. JFPB provided oversight of survey fielding, data analyses and interpretation, and visualization. JB, JS, and JFPB made major contributions to writing the manuscript. All authors (ALRS, JB, GG, SJL, SRM, TS, JS, JFPB) made critical revisions to the manuscript. All authors (ALRS, JB, GG, SJL, SRM, TS, JS, JFPB) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The expert stakeholder engagement that guided survey development was deemed non-human subjects research by the Johns Hopkins School of Medicine (JHM #IRB IRB00354016). The survey was deemed non-human subject research by the Ohio State University College of Medicine Institutional Review Board (OSU IRB #2022E1207). As such, explicit informed consent was not required; consent was implied based on individuals’ agreement to participate in the survey.
Consent for publication
Not applicable.
Competing interests
JS is a member of Merck KGaA’s Ethics Advisory Panel and Stem Cell Research Oversight Committee; a member of IQVIA’s Ethics Advisory Panel; a member of Aspen Neurosciences Clinical Advisory Panel; a member of a Merck Data Monitoring Committee; and a consultant to Biogen. None of these activities are related to the material discussed in this article. SJL receives funding to her institution from Gilead Sciences and served as a consultant to Hookipa Biotech. None of these activities are related to the material discussed in this article. TS has a research grant with ViiV Healthcare, but that research is not related to the material discussed in this article. ALRS, JMB, GG, SRM, JFPB have no disclosures.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schuster, A.L.R., Bollinger, J., Geller, G. et al. Prioritization of ethical concerns regarding HIV molecular epidemiology by public health practitioners and researchers. BMC Public Health 24, 1436 (2024). https://doi.org/10.1186/s12889-024-18881-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18881-4