
Abstract
Background
In China, the world’s largest developing country, low back pain (LBP) is a common public health issue affecting workability. This meta-analysis aimed to systematically assess the risk factors of LBP in the Chinese population.
Methods
Four English language and four Chinese databases were searched, and cross-sectional studies on the risk factors for LBP in Chinese populations were identified and collected. The search timeframe covered the period from the establishment of the database to November 2023. Two researchers independently reviewed the literature, extracted the data, and evaluated the risk of bias. Begg’s and Egger’s tests were used to evaluate publication bias.
Results
Fifteen cross-sectional studies involving 86,575 people were included. Seven risk factors for LBP were identified. Six risk factors were statistically significant: Cigarette smoking (odds ratio [OR] = 1.55; 95% confidence interval [CI]: 1.15, 2.08, P = 0.004, I2 = 72%), body mass index (BMI) ≥ 28 kg/m² (OR = 4.51; 95% CI: 3.36, 6.07, P < 0.00001, I2 = 8%), female sex (OR = 1.54; 95% CI: 1.25, 1.90, P < 0.0001, I2 = 63%), vibration exposure at work (OR = 1.65; 95% CI: 1.16, 2.34, P = 0.006, I2 = 84%), working overtime (OR = 2.57; 95% CI: 1.12, 5.91, P = 0.03, I2 = 85%), and lack of exercise (OR = 2.48; 95% CI: 1.62, 3.78, P < 0.0001, I2 = 0%). One risk factor that was not statistically significant was standing for long periods (OR = 1.02; 95% CI: 0.82, 1.26, P = 0.88, I2 = 73%).
Conclusions
This study found that smoking, a BMI ≥ 28 kg/m², female sex, vibration exposure at work, working overtime, and lack of exercise may be risk factors for LBP in the Chinese population. Because the included studies were cross-sectional and the certainty of the evidence was very low, the results need to be interpreted cautiously. Multicentre, high-quality studies should be conducted in the future. To reduce the prevalence of LBP, the Chinese government and hospitals must develop early screening programs and implement effective preventive and interventional measures.
Trial registration
This study is registered in the PROSPERO database (No. CRD42023447857).
Similar content being viewed by others

Background
Low back pain (LBP) is a common symptom of many known and unknown pathologies or diseases [1]. Pain is usually located at the lower edge of the ribs, in the lumbosacral region, or accompanied by unilateral and bilateral lower limb nervous system symptoms [2]. LBP is a health problem that can occur in all age groups. According to literature reports, approximately 90% of people worldwide experience LBP at some stage of their lives [3]. LBP ranks sixth among all disease burdens in developed and developing countries [4, 5]. Hartvigsen et al. reported [1] that the global economic burden of LBP is likely to increase further.
In China, LBP is also a major public health problem. According to Chen et al. [6], the annual prevalence of LBP in Chinese adults is 20.88–29.88%. This is closely related to China’s social and economic conditions. China is a large agricultural country with a population of more than 1.4 billion, and many people perform manual labour work. Furthermore, the level of agricultural mechanisation in China is significantly lower than that in developed countries [7], and the degree of industrial intelligence is also relatively low. As a rapidly emerging developing country, many adults in China work long hours to earn more income for their household expenses in response to escalating costs of living [8]. During their leisure time, the participation rate of Chinese people in sports activities was only 13.8%, which was significantly lower than that in Western countries [9]. The vast differences between Chinese and Western cultures and the lack of medical knowledge in the Chinese population may aggravate the occurrence of chronic pain in the Chinese population [10]. One study found that the prevalence of chronic pain in China was 31.54%, and most patients with chronic pain were in the northern and southern coastal areas [10]. Among the patients with chronic pain, 24.06% did not visit the hospital, and 36.788% did not receive any treatment [10]. Compared with developed Western countries, Chinese people have an insufficient understanding of chronic pain; the medical treatment rate of the affected population is low, and the number of patients undergoing standard treatment is also low [10]. Additionally, there are 1.14 billion smokers worldwide and an estimated 306 million adult smokers in China, the country with the largest number of smokers worldwide [11, 12]. China’s economic development, popularisation of medical knowledge, and lifestyle habits show unique characteristics. These factors jointly affect LBP prevalence and risk in the Chinese population.
The risk factors for LBP reported in the literature can be divided into three aspects: (1) lifestyle factors such as obesity, smoking, and lack of exercise; (2) social factors such as working overtime, physical labour, education, and job satisfaction; and (3) psychological factors such as depression and anxiety [1, 13, 14]. If people have an unhealthy lifestyle, choose to eat junk food, smoke, and are unwilling to exercise, there is an increased risk of LBP. In highly competitive metropolitan cities, employees often work overtime and engage in heavy physical labour, resulting in low job satisfaction and the possibility of LBP. However, psychological factors are often overlooked. A cross-sectional study in South Korea found that the severity of depressive symptoms was associated with an increased risk of LBP [15]. A retrospective study conducted in the United States revealed that a healthy emotional state and a positive lifestyle can aid recovery from LBP [16]. In addition, regarding certain factors such as prolonged standing and education level, the research findings are inconsistent. Research conducted by Li et al. [17] and Jia et al. [18] indicate that prolonged standing may be a protective factor against LBP, whereas research conducted by Peng et al. [19] and Yue et al. [20] shows otherwise. Conflicting research is also seen in education. Xu et al. [21], Liu [22], and Jia et al. [18] reported an association between education and LBP, whereas Ye et al. [23] reported the opposite. The inconsistency in these research results may be related to the significant differences in the industries in which the research participants were located.
Although existing studies have provided valuable knowledge about LBP, few studies on the risk factors of LBP in the Chinese population exist. Investigations and research are limited by the sample size and study population. After reviewing Chinese and English language databases, we could not locate any evidence-based studies on the risk factors for LBP in the Chinese population. This finding suggests a systematic and quantitative approach is required to address this issue. As an evidence-based research method, meta-analysis can comprehensively analyse the results of multiple studies, improve the accuracy of result estimation, and identify and quantify potential risk factors. Therefore, the purpose of this study was to systematically review and integrate existing studies on the risk factors of LBP in the Chinese population through a meta-analysis. The aims were to enhance statistical precision, address inconsistencies among studies, and ensure robust conclusions, thereby providing an evidence-based foundation for formulating effective prevention and intervention strategies.
Methods
This evidence-based medical study is registered in The International Prospective Register of Systematic Reviews (PROSPERO) database (No. CRD42023447857). The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [24, 25].
Search strategy
PubMed, Web of Science, Embase, Cochrane Library, CNKI, WanFang Date, VIP, and CBM databases were searched to collect cross-sectional studies on the risk factors for LBP in the Chinese population. From the time the databases were created until 1 November 2023, eight databases were searched using MeSH Terms, index terms, and keywords. Chinese search terms: ‘low back pain’ or ‘lower back pain’, ‘risk factors’ or ‘influencing factors’ or ‘related factors’. The English language search strategy is detailed in Additional File 1.
Inclusion criteria
-
Research individuals: People with LBP (pain arising from the lower edge of the ribs in the lumbosacral and sacroiliac areas, with or without radiating pain in the lower limbs [2]) in China.
-
Exposure factors: Risk factors that may lead to the onset of LBP.
-
Outcome measure: Clinical diagnosis confirming the presence of LBP.
-
Study type: Cross-sectional studies.
-
Studies with original clear odds ratios (ORs) and 95% confidence intervals (95% CIs).
-
Language: Chinese and English.
Exclusion criteria
-
Republished studies.
-
Studies with different research participants and methods.
-
Studies on individuals with lumbar stenosis or other comorbidities.
-
Dissertations and conference papers.
-
Research lacking data or not including analytical factors.
Data extraction and quality assessment
Two researchers (Qiang Li and Yiding Wang) with extensive retrieval experience read the literature and extracted the information. The contents of the records included the first author, publication year, sample size, risk factors, and OR (95% CI). The third researcher (Leyun Peng) made the final decision whenever problems were encountered regarding data extraction; quality was evaluated. Two reviewers evaluated cross-sectional studies using the Agency for Healthcare Research and Quality methods [26]. With this method [27], 1–3 points mean low quality, 4–7 points mean medium, and 8–11 points mean high quality. In the Newcastle-Ottawa Scale, 0–4 points mean low quality, 5–6 points mean medium, and 7–9 points mean high quality.
The Grading of Recommendations, Assessment, Development, and Evaluation system [28] was employed to assess the evidence quality for the risk factors. This is based on factors such as study design, risk of bias, imprecision, inconsistency, indirectness, publication bias, and effect size [29,30,31,32,33,34]. The level of evidence was categorised as high, medium, low, or very low.
Statistical analyses
To guarantee the accuracy of the pooled effect estimates, we conducted a meta-analysis based solely on risk factors evaluated in a minimum of four studies. We used Revman 5.3 software for statistical analysis. OR (95% CI) was used as the effect analysis statistic. I² was used to test heterogeneity using P-values. Low, moderate, and high degrees of heterogeneity were indicated by the I2 statistical values of 25, 50, and 75%, respectively [35]. When I2 was > 50%, sensitivity analyses were performed to exclude each study individually to determine the stability of the findings. Funnel plot analysis was performed when at least 10 studies were included. Begg’s and Egger’s tests were used to evaluate the publication bias.
Results
Study selection
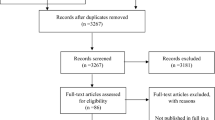
We initially searched the database and obtained 1,984 records. In total, 836 duplicate records were deleted using EndNote X9. We then reviewed the titles and abstracts of the literature and excluded 1,051 records. After reading the full texts, 82 studies were excluded. Finally, 15 studies were included for appraisal and analysis. A flow chart of the article screening is shown in Fig. 1. The studies excluded in the final step are presented in Additional File 2.

Flow chart of the search process for the studies
Study characteristics and methodologic quality
The basic characteristics and quality assessment results of the included studies are summarised in Table 1. For details of the quality assessment of the literature, please refer to Additional File 3. Fifteen papers [18,19,20, 22, 36,37,38,39,40,41,42,43,44,45,46] were published between 2006 and 2022. The sample size ranged from 96 to 57,501, with a total of 86,575 individuals. The quality assessment of the 15 cross-sectional studies yielded scores ranging from 8 to 10.
Risk factors for LBP in the Chinese population
Seven risk factors were identified: cigarette smoking, body mass index (BMI) ≥ 28 kg/m², female sex, vibration exposure at work, working overtime, lack of exercise, and standing for long periods.
The certainty of the evidence for these seven risk factors was very low. Some risk factors, such as smoking, vibration exposure at work, and standing for a long time, might have had publication bias. The comprehensive results and the certainty of evidence assessment are presented in Table 2. A detailed rating of the certainty of evidence assessment is provided in Additional File 4. Begg’s and Egger’s tests are presented in Additional File 5.
Cigarette smoking
Six studies assessing the correlation between smoking and LBP were included in this meta-analysis [18, 36,37,38, 45, 46]. Comprehensive findings suggest that individuals in China who smoke are at a heightened risk of experiencing LBP compared with those who do not smoke (OR = 1.55; 95% CI: 1.15, 2.08, P = 0.004, I2 = 72%) (Fig. 2). Sensitivity analysis indicated significant heterogeneity regardless of which study was excluded.

Forest plot of cigarette smoking
BMI ≥ 28 kg/m²
Five studies evaluating the relationship between BMI ≥ 28 kg/m² and LBP were included [36,37,38,39, 41]. The comprehensive findings suggest that individuals in the Chinese population with a BMI of 28 kg/m² or higher are at a heightened risk of experiencing LBP compared with those with a BMI below 28 kg/m² (OR = 4.51; 95% CI: 3.36, 6.07, P < 0.00001, I2 = 8%) (Fig. 3).

Forest plot of BMI ≥ 28 kg/m²
Female sex
Five studies assessing the association between women and LBP were included [19, 20, 22, 41, 46]. The comprehensive findings suggest that within the Chinese population, women are more susceptible to LBP than men (OR = 1.54; 95% CI: 1.25, 1.90, P < 0.0001, I2 = 63%) (Fig. 4). Sensitivity analysis indicated that eliminating Liu et al.’s study could reduce I2 to 0% (OR = 1.67; 95% CI: 1.44, 1.93, P < 0.00001).

Forest plot of female sex
Vibration exposure at work
Five studies evaluating the relationship between work-related exposure to vibration sources and LBP were included in the meta-analysis [18, 22, 39, 40, 43]. The findings indicated that individuals in China who were exposed to vibration sources were at a higher risk of experiencing LBP than those not exposed to vibration sources (OR = 1.65; 95% CI: 1.16, 2.34, P = 0.006, I2 = 84%) (Fig. 5). Sensitivity analysis indicated that eliminating Jia et al.’s study could reduce I2 to 8% (OR = 1.70; 95% CI: 1.42, 2.03, P < 0.00001). This may be related to Jia’s definition of risk factors, which differs from those of other studies that only mention work involving vibrations. Jia’s study mentioned the use of vibration tools.

Forest plot of vibration exposure at work
Working overtime
Four studies assessing the association between extended working hours and LBP were included in the meta-analysis [36, 38, 42, 44]. These findings suggest that individuals in China who work extended hours are more susceptible to LBP than those who work standard hours (OR = 2.57; 95% CI: 1.12, 5.91, P < 0.03, I2 = 85%) (Fig. 6). Sensitivity analysis indicated that eliminating the study by Xu et al. could reduce the I2 to 0% (OR = 3.55; 95% CI: 2.24, 5.63, P < 0.00001).

Forest plot of working overtime
Lack of exercise
Four studies assessing the association between exercise and LBP were included in the meta-analysis [37,38,39,40]. The comprehensive findings suggest that individuals in China who insufficiently engage in physical activity are at a greater risk of developing LBP than those who exercise regularly (OR = 2.48; 95% CI: 1.62, 3.78, P < 0.0001, I2 = 0%) (Fig. 7).

Forest plot of lack of exercise
Standing for long periods
Four studies assessing the association between prolonged standing and LBP were included [18,19,20, 44]. The comprehensive findings indicate that prolonged standing is not a risk factor for LBP in the Chinese population (OR = 1.02; 95% CI: 0.82, 1.26, P = 0.88, I2 = 73%) (Fig. 8). Sensitivity analysis indicated that eliminating Jia’s study could reduce the I2 to 0% (OR = 1.10; 95% CI: 0.94, 1.30, P = 0.24).

Forest plot of standing for long periods
Discussion
LBP is a common clinical problem in the Chinese population. Limited studies on LBP risk factors exist in China, and their results vary widely. Most studies have only explored the risk factors for LBP in specific occupational and regional populations. For instance, the study participants of Yue et al. [20] and Yao et al. [53] focused on Chinese teachers and adolescents, while Barrero et al. [43] only focused on individuals from rural areas. The risk factors they present have inherent limitations and do not apply to the entire Chinese population. Therefore, we conducted a systematic review to identify the risk factors that may cause LBP in the Chinese population. Seven risk factors were identified: smoking, BMI ≥ 28 kg/m², female sex, vibration exposure at work, working overtime, lack of exercise, and prolonged standing. Among them, prolonged standing was not related to the occurrence of LBP, which may be owing to different occupations and research studies conducted. Wong et al. found that female sex, obesity, and smoking were risk factors for LBP [54]. A LBP study among African school teachers found that lack of exercise and female sex are risk factors for LBP [55]. Jia et al.’s study found that vibration exposure at work and working overtime were risk factors for LBP [18]. These results are consistent with those of the present study.
Smoking and LBP are global public health concerns. Numerous studies [56,57,58] indicate that smoking increases the risk of LBP. Using a passive smoking model in rats, Nemoto et al. [56] found cracks, tears, and dislocations in the intervertebral discs. A recent study [58] has also shown that smoking and tetramer tryptase accelerate intervertebral disc degeneration by inducing methyltransferase 14-mediated dishevelled-axin domain-containing 1 m6 modifications. Smokers experience significantly greater levels of lumbar pain and dysfunction than non-smokers [57]. The greater the daily tobacco intake, the more pronounced the LBP. Therefore, to prevent the onset of LBP, Chinese individuals are advised to quit smoking or reduce the frequency of smoking.
BMI ≥ 28 kg/m2 is a risk factor for LBP in the Chinese population. Adipose tissue due to obesity can release several adipokines (including leptin, resistin, and adiponectin) as well as proinflammatory cytokines such as interleukin-1β, interleukin-6, and tumour necrosis factor-α [59]. Leptin can accelerate the calcification of hyaline cartilage in the cartilaginous endplate, interfering with the transport of nutrients to disc cells [60]. Resistin expression in normal intervertebral discs is low but increases during intervertebral disc degeneration. In intervertebral disc tissues, resistin can activate nuclear factor-κB and p38 mitogen-activated protein kinase, followed by resistin binding to toll-like receptor 4 and increasing chemokine ligand 4 expression. This promotes the infiltration of macrophages [61]. However, the correlation between adiponectin level and LBP remains unclear. All these molecules may cause low-grade inflammation and have been shown to exert detrimental effects on nucleus pulposus and annulus fibrosus cells in vitro [62]. Fortunately, obesity can be modified through exercise and dietary management. Individuals with obesity should consider appropriate weight management strategies. Moreover, there are variations in the risk of LBP across sex groups. Women are at a higher risk of developing LBP than men, and patients with LBP exhibit poor dynamic postural control [63]. This may be attributed to the additional housework that women perform and their relatively low muscle strength. Women, as a group susceptible to LBP, should prioritise enhancing self-management awareness and mitigating LBP stemming from intrinsic factors.
A previous study showed that whole-body vibration can lead to compression, stretching, rotation, and spine flexion, all of which involve back muscles and cause fatigue [64]. Studies of the erector spinae found that electromyography signals increased during whole-body vibration, resulting in a decrease in the signal frequency of muscle fatigue, mainly at the resonance frequency of 5 Hz [65,66,67]. Kim et al. and Burström et al. concluded that irregular whole-body vibrations are closely associated with musculoskeletal disorders, particularly LBP onset [68, 69]. Moreover, our previous research [70] indicated that vibration therapy remains a viable treatment for LBP, which may be closely related to vibration frequency and amplitude.
The reality many people face is the long working hours they must endure. Individuals are susceptible to musculoskeletal disorders in prolonged and high-intensity work environments, leading to an increased risk of LBP. People who frequently work overtime should be vigilant in preventing and managing this condition. In addition, extended working hours can lead to sedentary behaviour, a fixed posture at work, and prolonged neck forward tilt among professionals working in offices and drivers. A positive correlation exists between sedentary time and two common acute phase reactants, C-reactive protein and fibrinogen [71, 72]. Sedentary behaviour also has a detrimental impact on systemic inflammation [71, 72]. Compared with men, the level of inflammation in women is more influenced by sedentary behaviour [71, 72]. Sedentary behaviour may also reduce bone density, decrease flexibility, and promote weight gain [59]. Furthermore, all participants in this study were adults, and no consideration was given to children. An Iranian meta-analysis [73] suggests that various forms of sedentary behaviour (such as prolonged TV viewing or electronic device use) may also contribute to LBP in children.
This study suggests that a lack of exercise may be a risk factor for LBP. As work and life pressures grow in China, ensuring regular physical activity for industry workers, such as factory employees, office staff, and healthcare professionals, has become challenging. A meta-analysis in China also suggested that Taijiquan, Pilates, sling and core stability exercises can improve LBP symptoms [74]. Taijiquan, a traditional Chinese sport, can enhance joint flexibility and mobility, boost muscle strength and endurance, increase the tensile strength of ligaments and bursae, improve cardiopulmonary function, and alleviate stress and anxiety [75]. In addition, Taijiquan can decrease the expression of serum B-type linalool peptides, enhance blood circulation, increase the metabolism of the lumbar spine, improve the absorption of calcium and other minerals by bone cells, and increase bone density in the lumbar region [76]. We recommend engaging in physical activity as a treatment or preventive measure for LBP.
Strengths and limitations
To our knowledge, this is the first meta-analysis to explore the risk factors for LBP in the Chinese population. We quantitatively assessed multiple studies on the risk factors for LBP in the Chinese population. With enhanced statistical precision and the resolution of inconsistencies found in previous studies, we arrived at more robust conclusions.
However, this study had inherent limitations. First, the included participants had various occupations and were from different regions of China, leading to heterogeneity in the results. Second, the included studies were cross-sectional, making it impossible to establish a causal relationship between the exposure factors and outcomes. Recall bias was also highly probable. Third, the limited literature included in this study on certain risk factors might have introduced bias into the research outcomes. Lastly, only Chinese and English language literature were included, with no gray literature retrieved, leading to a limited number of articles in the final analysis.
Conclusion
This study employed evidence-based medical research methods to analyse and explore the risk factors for LBP in the Chinese population. We found that smoking, BMI ≥ 28 kg/m², female sex, vibration exposure at work, working overtime, and lack of exercise may be risk factors for LBP in this population. However, because of the limited number of included studies and their cross-sectional design, causality could not be determined. The certainty of the evidence is also very low. Therefore, these findings should be interpreted with caution. Multicentre, high-quality studies should be conducted in the future. To reduce the prevalence of LBP, the Chinese government and hospitals must develop early screening programs and implement effective preventive and interventional measures.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- LBP:
-
Low back pain
- BMI:
-
Body mass index
- OR:
-
Odds ratio
- 95% CI:
-
95% Confidence interval
References
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–67.
Dionne CE, Dunn KM, Croft PR, Nachemson AL, Buchbinder R, Walker BF, et al. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine. 2008;33:95–103.
Freburger JK, Holmes GM, Agans RP, Jackman AM, Darter JD, Wallace AS, et al. The rising prevalence of chronic low back pain. Arch Intern Med. 2009;169(3):251–8.
Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, et al. The global burden of low back pain: estimates from the global burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–74.
Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the global burden of Disease Study 2013. Lancet. 2015;386(9995):743–800.
Chen D, Chen CH, Hu ZC, Shao ZX, Lin JL, Wu AM. Prevalence of low back pain in adult population in China: a systematic review. Chin J Evid Based Med. 2019;19(6):651–5.
Shang SQ, Wang JS, Wang DW. Development of agricultural mechanization in China and its current Strategic Focus. Agricultural Mach Technol. 2019. https://doi.org/10.22314/2073-7599-2019-13-3-4-7. 13.4-7.
Liang Y, Li Z, Wang X, Liu P, Ma L, Wang X. Association between overtime and depressive symptoms among Chinese employees. Front Public Health. 2023;11:1241994.
Zou Q, Wang H, Du W, Su C, Ouyang Y, Wang Z, et al. Trends in leisure-time physical activity among Chinese adults - China, 2000–2015. China CDC Wkly. 2020;2(9):135–9.
Zheng YJ, Zhang TJ, Yang XQ, Feng ZY, Qiu F, Xin GK, et al. A survey of chronic pain in China. Libyan J Med. 2020;15(1):1730550.
GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the global burden of Disease Study 2019. Lancet. 2021;397(10292):2337–60.
Chinese Center for Disease Control and Prevention. The results of Chinese adult Tobacco Survey in 2018 [R]. Beijing: Chinese Center for Disease Control and Prevention; 2020.
Fatoye F, Gebrye T, Odeyemi I. Real-world incidence and prevalence of low back pain using routinely collected data. Rheumatol Int. 2019;39(4):619–26.
Liu Y, Tang G, Li J. Causations between obesity, diabetes, lifestyle factors and the risk of low back pain. Eur Spine J. 2023. https://doi.org/10.1007/s00586-023-08069-6.
Park SM, Kim HJ, Jang S, Kim H, Chang BS, Lee CK, et al. Depression is closely Associated with Chronic Low Back Pain in patients over 50 years of age: a cross-sectional study using the Sixth Korea National Health and Nutrition Examination Survey (KNHANES VI-2). Spine (Phila Pa 1976). 2018;43(18):1281–8.
Roberts KE, Beckenkamp PR, Ferreira ML, Duncan GE, Calais-Ferreira L, Gatt JM, et al. Positive lifestyle behaviours and emotional health factors are associated with low back pain resilience. Eur Spine J. 2022;31(12):3616–26.
Li JY, Wang S, He LH, Wu SS, Yang L, Yu SF, et al. Risk factors of low back pain among the Chinese occupational population: a case-control study. Biomed Environ Sci. 2012;25(4):421–9.
Jia N, Zhang MB, Zhang HD, Ling RJ, Liu YM, Li G et al. Prevalence and risk factors analysis for low back pain among occupational groups in key industries of China. BMC Public Health, 2022(22):1493.
Peng BL, Wu JB, Qi C, Zhao CH, Lin RJ, Yang L. Prevalence and influence factors of low back pain among workers in an automobile industry corporation. Chin J Public Health. 2017;33(4):663–7.
Yue PY, Liu FY, Li LP. Neck/shoulder pain and low back pain among school teachers in China, prevalence and risk factors. BMC Public Health,2012; (12):789.
Xu XY, Qiu SJ, An SL, Jin AM, Min SX. Analysis of risk factors of nonspecific low back pain in a community population: a case-control study. J South Med Univ. 2014;34(12):1794–8.
Liu F. Analysis of the related factors of chronic nonspecific low back pain in community population. J Cervic Lumb. 2020;41(05):568–71.
Ye SY, Jing QL, Chen W, Lu J. Risk factors of non-specific neck pain and low back pain in computer- using office workers in China: a cross- sectional study. BMJ Open, 2017(7):e014914.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hofmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Page MJ, Moher D, Bossuyt PM, Boutron I, Hofmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160.
Agency for Healthcare Research and Quality (US). AHRQ methods for effective health care. Methods guide for effectiveness and comparative effectiveness reviews. Rockville: 2008.
Rostom A, Dubé C, Cranney A, Celiac, Disease. Rockville (MD): Agency for Healthcare Research and Quality (US); 2004 Sep. (Evidence Reports/Technology Assessments, No. 104.) Appendix D. Quality Assessment Forms. http://www.ncbi.nlm.nih.gov/books/NBK35156/.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1.Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64:383–94.
Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–6.
Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines: 4. Rating the quality of evidencedstudy limitations (risk of bias). J Clin Epidemiol. 2011;64:407–15.
Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidencedimprecision. J Clin Epidemiol. 2011;64:1283–93.
Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 7. Rating the quality of evidencedinconsistency. J Clin Epidemiol. 2011;64:1294–302.
Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality of evidencedindirectness. J Clin Epidemiol. 2011;64:1303–10.
Guyatt GH, Oxman AD, Montori V, Vist G, Kunz R, Brozek J, et al. GRADE guidelines: 5. Rating the quality of evidence-publication bias. J Clin Epidemiol. 2011;64:1277–82.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Zhang Y, Liu J, Chen G, Liu CJ. Risk factors of nonspecific low back pain in cadre health care population. J North Sichuan Med Coll. 2021;36(11):1424–7.
Wu G. Analysis of disease situation and risk factors of non-specific low back pain in taxi drivers in a city. J Cervic Lumb. 2019;40(6):770–2.
Yang QC. Investigation and analysis of risk factors of nonspecific low back pain in teachers from a high school. J Cervic Lumb. 2020;41(4):452–4.
Wang X, Liu YQ, Tian XC, Li XH, Wu T, Xu FZ, et al. Analysis of the influence factors of non-specific low back pain in urban population. J Cervic Lumb. 2019;40(6):740–2.
Wang JQ, Chen T, Zhang X. Analysis of risk factors of non- specific low back Pain in Young People. J Med Res. 2022;51(3):80–2.
Zhang Q, Dong HY, Zhu CJ, Liu JZ. Low back pain in emergency ambulance workers in tertiary hospitals in China and its risk factors among ambulance nurses: a cross-sectional study. BMJ Open. 2019;9(9):e029264.
Wang M, Yu J, Liu N, Liu Z, Wei X, Yan F, et al. Low back pain among taxi drivers: a cross-sectional study. Occup Med. 2017;67:290–5.
Barrero LH, Hsu YH, Terwedow H, Perry MJ, Dennerlein JT, Brain JD, et al. Prevalence and physical determinants of low back pain in a rural Chinese population. Spine. 2006;31(23):2728–34.
Xu G, Pang D, Liu F, Pei D, Wang S, Li L. Prevalence of low back pain and associated occupational factors among Chinese coal miners. BMC Public Health. 2012;12:149.
Wei G, Li H, Wang B, Wu J, Wu F, Lin Z. A retrospective cross-sectional survey of non-specific lower back pain among a cohort of Chinese army soldiers. Int J Surg. 2018;56:288–93.
Liu X, Wang L, Stallones L, Wheeler KK, Zhao W, Smith GA, et al. Back pain among farmers in a northern area of China. Spine (Phila Pa 1976). 2012;37(6):508–14.
Expert Group of the Spinal Cord Professional Committee of the Chinese Rehabilitation Medicine Association. Expert consensus on acute/chronic nonspecific low back pain in China. Chin J Spine Spinal Cord. 2016;26(12):1134–8.
Salvendy. Handbook of Human Factors and Ergonomics. 4th ed; 2012.
Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–7.
Hildebrandt VH, Bongers PM, Van Dijk FJ, Kemper HC, Dul J. Dutch musculoskeletal questionnaire: description and basic qualities. Ergonomics. 2001;44:1038–55.
Li J, Yang W, Liu P, Xu Z, Cho SI. Psychometric evaluation of the Chinese(mainland) version of job content questionnaire: a study in university hospitals. Ind Health. 2004;42:260–7.
de Barros EN, Alexandre NM. Cross-cultural adaptation of the nordic Musculoskeletal Questionnaire. Int Nurs Rev. 2003;50:101–8.
Yao W, Luo C, Ai F, Chen Q. Risk factors for nonspecific low-back pain in Chinese adolescents: a case-control study. Pain Med. 2012;13(5):658–64.
Wong CK, Mak RY, Kwok TS, Tsang JS, Leung MY, Funabashi M, et al. Prevalence, incidence, and factors Associated with non-specific chronic low back Pain in Community-Dwelling older adults aged 60 years and older: a systematic review and Meta-analysis. J Pain. 2022;23(4):509–34.
Tesfaye AH, Abere G, Mekonnen TH, Jara AG, Aragaw FM. A systematic review and meta-analysis of low back pain and its associated factors among school teachers in Africa. BMC Musculoskelet Disord. 2023;24(1):499.
Nemoto Y, Matsuzaki H, Tokuhasi Y, Okawa A, Uematu Y, Nishimura T, et al. Histological changes in intervertebral discs after smoking cessation: experimental study using a rat passive smoking model. J Orthop Sci. 2006;11(2):191–7.
Yang QH, Zhang YH, Du SH, Wang YC, Wang XQ. Association between smoking and pain, functional disability, anxiety and depression in patients with chronic low back pain. Int J Public Health. 2023;68:1605583.
Tu J, Li W, Hansbro PM, Yan Q, Bai X, Donovan C, et al. Smoking and tetramer tryptase accelerate intervertebral disc degeneration by inducing METTL14-mediated DIXDC1 m6 modification. Mol Ther. 2023;31(8):2524–42.
Ambrosio L, Mazzuca G, Maguolo A, Russo F, Cannata F, Vadalà G, et al. The burden of low back pain in children and adolescents with overweight and obesity: from pathophysiology to prevention and treatment strategies. Ther Adv Musculoskelet Dis. 2023;15:1759720X231188831.
Han YC, Ma B, Guo S, Yang M, Li LJ, Wang SJ, et al. Leptin regulates disc cartilage endplate degeneration and ossification through activation of the MAPK-ERK signalling pathway in vivo and in vitro. J Cell Mol Med. 2018;22:2098–109.
Li Z, Wang X, Pan H, Yang H, Li X, Zhang K, et al. Resistin promotes CCL4 expression through toll-like receptor-4 and activation of the p38-MAPK and NF-κB signaling pathways: implications for intervertebral disc degeneration. Osteoarthr Cartil. 2017;25:341–50.
Molinos M, Almeida CR, Caldeira J, Cunha C, Gonçalves RM, Barbosa MA. Inflammation in intervertebral disc degeneration and regeneration. J R Soc Interface. 2015;12:20141191.
Wu XH, Yu H, Yang XJ, Wu YM, Yang P. Gender differences in postural control in patients with nonspecific chronic low back pain. J Cervic Lumb. 2020;41(2):135–9.
Patterson F, Miralami R, Tansey KE, Prabhu RK, Priddy LB. Deleterious effects of whole-body vibration on the spine: a review of in vivo, ex vivo, and in vitro models. Anim Model Exp Med. 2021;4(2):77–86.
Pope MH, Wilder DG, Magnusson M. Possible mechanisms of low back pain due to whole-body vibration. J Sound Vib. 1998;215(4):687–97.
Blüthner R, Hinz B, Menzel G, Seidel H. Back muscle response to transient whole-body vibration. Int J Ind Ergon. 1993;12(1–2):49–59.
Hansson T, Magnusson M, Broman H. Back muscle fatigue and seated whole body vibrations: an experimental study in man. Clin Biomech Elsevier Ltd. 1991;6:173–8.
Burström L, Nilsson T, Wahlström J. Whole-body vibration and the risk of low back pain and sciatica: a systematic review and meta-analysis. Int arch Occup Environ Health. 2015;88(4):403–18.
Kim JH, Zigman M, Aulck LS, Ibbotson JA, Dennerlein JT, Johnson PW. Whole body vibration exposures and health status among professional truck drivers: a cross-sectional analysis. Ann Occup Hyg. 2016;60(8):936–48.
Li Q, Liu P, Wang ZB, Li X. Vibration therapy to improve pain and function in patients with chronic low back pain: a systematic review and meta-analysis. J Orthop Surg Res. 2023;18(1):1–12.
Howard BJ, Balkau B, Thorp AA, Magliano DJ, Shaw JE, Owen N, et al. Associations of overall sitting time and TV viewing time with fibrinogen and C reactive protein: the AusDiab study. Br J Sports Med. 2015;49(4):255–8.
Yates T, Khunti K, Wilmot EG, Brady E, Webb D, Srinivasan B, et al. Self-reported sitting time and markers of inflammation, insulin resistance, and adiposity. Am J Prev Med. 2012;42(1):1–7.
Baradaran Mahdavi S, Riahi R, Vahdatpour B, Kelishadi R. Association between sedentary behavior and low back pain; a systematic review and meta-analysis. Health Promot Perspect. 2021;11(4):393–410.
Li Y, Yan L, Hou L, Zhang X, Zhao H, Yan C, et al. Exercise intervention for patients with chronic low back pain: a systematic review and network meta-analysis. Front Public Health. 2023;11:1155225.
Kong LJ, Lauche R, Klose P, Bu JH, Yang XC, Guo CQ, et al. Tai Chi for Chronic Pain conditions: a systematic review and Meta-analysis of Randomized controlled trials. Sci Rep. 2016;6:25325.
Yeh GY, Wood MJ, Lorell BH, Stevenson LW, Eisenberg DM, Wayne PM, et al. Effects of Tai Chi mind-body movement therapy on functional status and exercise capacity in patients with chronic heart failure: a randomized controlled trial. Am J Med. 2004;117(8):541–8.
Acknowledgements
Not applicable.
Funding
1. Yang Yonghui Famous Traditional Chinese Medicine Studio of Anhui Province; 2. Anhui provincial-level regional Chinese medicine rehabilitation center construction project (Anhui Chinese medicine service secretary [2022] 34); 3. The fourth batch of national regional medical center construction project (Development and Reform Office of Society [2022] 887).
Author information
Authors and Affiliations
Contributions
QL and LYP conceived and designed the study. QL and YDW searched and selected relevant studies. QL and YDW extracted and interpreted data. QL and YDW analyzed the data. QL and LYP wrote the paper. QL, YHY, and ZBW revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Q., Peng, L., Wang, Y. et al. Risk factors for low back pain in the Chinese population: a systematic review and meta-analysis. BMC Public Health 24, 1181 (2024). https://doi.org/10.1186/s12889-024-18510-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18510-0