
Abstract
Background
Air pollution poses a significant health risk to the human population, especially for vulnerable groups such as the elderly, potentially discouraging their engagement in physical activity. However, there is a lack of sufficient objective and longitudinal data in current research on how air pollution affects physical activity among older adults. With these gaps, we aimed to explore the relationship between air pollution and objective measurement-based physical activity among older adults by engaging in a longitudinal study design.
Methods
A total of 184 older adults were recruited from three cities with varying levels of air quality. Mean daily minutes of physical activity were measured with 7 consecutive days of accelerometer monitoring (ActiGraph GT3X-BT). Corresponding air pollution data including daily PM2.5 (µg/m3), PM10 (µg/m3) and air quality index (AQI) were sourced from the China National Environmental Monitoring Centre at monitor locations close to older adults’ addresses. Associations between air quality and physical activity were estimated using a fixed effect model, adjusting for average daytime temperature, rain, age and weight.
Results
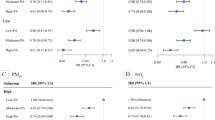
AQI and PM2.5 were observed to exhibit significant, inverse, and linear associations with mean daily walk steps, minutes of light physical activity (LPA), moderate physical activity (MPA) and moderate-to-vigorous physical activity (MVPA) in the single variable models. A one-level increase in AQI corresponded to a decline in 550.04 steps (95% [CI] = -858.97, -241.10; p < 0.001), 10.43 min (95% [CI] = -17.07, -3.79; p < 0.001), 4.03 min (95% [CI] = -7.48, -0.59; p < 0.001) and 4.16 min (95% [CI] = -7.77, -0.56; p < 0.001) in daily walking steps, LPA, MPA, and MVPA, respectively. A one-level increase in PM2.5 correlated with a decline in daily walk steps, LPA, MPA and MVPA by 361.85 steps (95% [CI] = -516.53, -207.16; p < 0.001), 8.97 min (95% [CI] = -12.28, -5.66; p < 0.001), 3.73 min (95% [CI] = -5.46, -2.01; p < 0.001,) and 3.79 min (95% [CI] = -5.59, -1.98; p < 0.001), respectively. However, PM10 displayed a significant negative association exclusively with LPA, with one-level increase in PM10 resulting in a 3.7-minute reduction in LPA (95% [CI] = -6.81, -0.59, p < 0.05).
Conclusion
Air pollution demonstrates an inverse association with physical activity levels among older adults, potentially discouraging their engagement in physical activity. Different air quality indicators may exert varying impacts on physical activity. Future studies are warranted to enhance policy interventions aimed at reducing air pollution and promoting physical activity.
Similar content being viewed by others

Introduction
Air pollution stands as a prominent global environmental health issue [1], resulting in the exacerbation of various diseases, including but not limited to decreased lung function, stroke, myocardial infarction, hypertension, asthma, bronchitis and premature mortality [2,3,4,5], especially for vulnerable groups such as the elderly [6, 7]. Some studies indicated that air pollution is associated with reduced lung function, elevated hypertension, and diverse respiratory and cardiovascular symptoms [2, 3], consequently impacting exercise capacity [8,9,10]. Despite observed declines in air pollutant levels over recent decades, the issue of poor air quality in developing countries remains a substantial public health concern [11, 12]. A study that gathered hourly air pollution data from more than 1500 monitoring stations across 32 provinces in China revealed that 92% of China’s residents encountered over 120 h of unfavorable air conditions annually [11].
Physical activity exerts an essential role in human health benefits, especially for older adults [13, 14]. Compelling evidence reveals that physical activity not only effectively reduces the risk of cardiovascular disease, obesity, stroke, type-II diabetes, osteoporosis, colon cancer and other diseases associated with air pollution among the elderly, but also enhances their mental health [15, 16]. Additionally, physical activity has been shown to increase their lifespan and healthy life expectancy [17, 18]. Research evidence has also suggested a “dose-response” connection between health status and the intensity of physical activity, indicating that engaging in higher intensity physical activities leads to greater health benefits [19,20,21,22,23,24,25]. Therefore, it is of paramount importance to enhance physical activity levels.
Current literature contains studies exploring air pollution’s impact on health behavior. Air pollution alerts can reduce fragile groups’, such as the elderly’s, outdoor activities [26, 27]. For example, warnings and alerts issued by local air pollution monitoring government institutions can reduce outdoor cycling behavior by 14–35% [28]. A study also showed that individuals mitigate pollution exposure by reducing the duration of outdoor vigorous physical activity (VPA), averaging an 18-minute reduction on days with air quality alerts [29]. Furthermore, studies have indicated varying degrees of air pollution’s impact on physical activity levels [30,31,32,33,34,35]. For example, a study from Korea reported both PM10 and PM2.5 levels presented significant negative impacts on the distances and durations of outdoor biking [36]. A meta-analysis drawing from various cross-sectional researches concluded that each unit (µg/m3) increase in ambient PM2.5 levels resulted in a 10% higher chance of physical inactivity [4]. Moreover, a merger of data from a South Korea study showed that the duration of walking decreased as the PM10 increased [37]. A previous mixed-age study exploring the correlation between physical activity and air quality index (AQI) showed that more than half of the participants adjusted the timing or frequency of their physical exercise in response to the AQI levels in their neighborhood [38]. A longitudinal cohort study of adults aged 18 years or older from California revealed that poor air quality was significantly linked to a reduction in accelerometer-based daily step counts. Specifically, when the AQI surpassed 200, step counts decreased by 18% compared to levels below 100 [39].
Although the aforementioned works have been done, three notable gaps persist in the scientific literature. First, there is a lack of studies using objective measurements to evaluate physical activity among older adults, all studies have relied on self-reported physical activity data [4, 31, 32, 40]. Second, while some studies have reported relationships between PM2.5, PM10 and physical activity levels of the elderly [9, 41], and between AQI and physical activity among mixed-age groups [38], no study has investigated the relationship between AQI and physical activity among older adults. Third, few studies have employed a longitudinal study design to explore how air pollution impacts physical activity, with most studies adopting a cross-section design [4, 32, 33, 40]. Even when longitudinal research was conducted, the primary focus was on diseased populations [42], non-elderly populations [35], or relied on self-reported methods to measure physical activity [34]. Hence, the objective of the study was to investigate how air pollution affects physical activity among older adults engaging objective measurements longitudinal study design.
Methods
Participants
The study recruited 184 participants from 46 communities in Beijing, Shijiazhuang, Hebei Province and Qinzhou, Guangxi Province during several periods (Beijing N = 116, Jan 11–18, 2018; Sep 28–Oct 11, 2019; Apr 16–27, 2021; May 6–17, 2021; Qinzhou N = 20, June 8–21, 2021; Shijiazhuang N = 48, July 14–23, 2021; July 23–31, 2021). Three cities present different air environments. According to a report from the Ministry of Ecology and Environment, Shijiazhuang is ranked in the bottom 20 nationwide regarding air quality, whereas Qinzhou is situated in the top 20, and Beijing falls in the middle range. All participants were healthy without diseases that could affect physical activity and were retired individuals aged 60 years or older. Recruitment information was disseminated through the Community Committee Office prior to this study. Individuals who were interested in our study provided written informed consent and completed a paper-pencil demographical information questionnaire including age, gender, weight and height. During each measurement period, participants were told to fasten accelerometers on their non-dominant waist. Air pollution data for the corresponding periods were collected from China National Environmental Monitoring Centre. Four participants who did not complete measurements were excluded because of three devices without data and one device with invalid data (wearing duration less than three days). Consequently, 180 participants with valid data were included in our study. Approval for the study was granted by Tsinghua University Institutional Review Board (IRB 20110170).
Air pollution exposure
We obtained air pollution data including hourly PM2.5, PM10, and AQI from the China National Environmental Monitoring Centre. AQI is an air quality index, comprising five components: carbon monoxide, ozone, particle pollution (PM), nitrogen dioxide, and sulfur dioxide. One of the PM components is classified into PM2.5 and PM10 on the basis of particle diameter, which are defined as < 2.5 µg and < 10 µg respectively (available from: https://www.epa.gov/criteria-air-pollutants/naaqs-table).
We selected monitoring sites closest to individuals’ residential addresses in the three cities for data collection (Fig. 1). These sites are Wanliu of the Haidian district, Beijing (air quality monitoring station ID:1007A), Century Park, Shijiazhuang (air quality monitoring station ID:1033A) and Qinzhou Environmental Monitoring Center, Qinzhou (air quality monitoring station ID:2502A), with an average distance of 4.71 km from the individual’s residential addresses. The AQI value ranges from 0 to 500 and is divided into six levels: Good AQI (0–50), Moderate AQI (51–100), Unhealthy for sensitive groups AQI (101–150), Unhealthy AQI (151–200), Very unhealthy AQI (201–300), Hazardous AQI (> 300). Similar to AQI, PM2.5 and PM10 are also categorized into six levels: very good, good, moderate, unhealthy for sensitive, unhealthy and very unhealthy.

Map of air quality monitoring stations and individual’s addresses. Notes: a: Map of China; b: Map of Beijing; c: Map of Qinzhou; d: Map of Shijiazhuang; Map shows the locations of individual’s residential address and surrounding air quality monitoring sites
Physical activity measurement
We collected physical activity data concurrently with air pollution data. Physical Activity data were measured using an accelerometer (ActiGraph GT3X-BT), which is a reliable and valid objective measure [43]. The volunteers were asked to wear GT3X-BT accelerometer for over 7 continuous days, for at least 10 h a day. The monitors’ recording epoch was set for collecting data at 60 Hz. Individuals were told to remove the accelerometer only during showering, swimming, or other water-related activities. Data included in the analysis required a minimum wearing duration of at least three days, with ten hours of wear each day. We processed the walking steps, kcals in energy expenditure, metabolic equivalents (METs), daily light physical activity (LPA), VPA, very vigorous physical activity (VVPA), moderate-to-vigorous physical activity (MVPA) and sedentary behavior using ActiLife software (version 6.13.3). The physical activity intensity in all data is graded based on the Counts Per Minute (CPM), which is divided using the Freedon’s classical accelerometer model: sedentary behavior (0-99CPM), LPA (100–1951 CPM), MPA (1952–5724 CPM), MVPA (1952–9498 CPM), VPA (5725–9498 CPM) and VVPA (9499–16,000 CPM) [44].
Statistical analysis
Statistical analysis was undertaken utilizing Stata 25.0. Descriptive statistics, including means, standard deviation (SD), and percentages of the 180 samples were calculated. Conducting a T-test was for evaluating whether the differences between the characteristics of male and female were significant. When p < 0.05, it was considered to be statistically significant. Fixed effect models adjusted for average daytime temperature, rain, age and weight were utilized for examining how air pollution, including PM2.5, PM10, and AQI, was related to physical activity variables.
Results
Participant characteristics
Table 1 displays the demographic characteristics of the 180 participants. Females made up nearly two-thirds (63.9%) of the participants. All participants wore GT3X-BT accelerometer for an average of 6.43 continuous days, totaling 1157days. Compliance with wearing the accelerometers was 5.85 days (SD = 1.46) for male and 6.76 (SD = 3.10) for female. The mean age, weight and BMI were 70.31 years old, 63.82 kg and 24.11 kg/m2 respectively. Additionally, male participants exhibited significantly greater height than their female counterparts (p < 0.05).
The air pollution variations
Table 2 and Fig. 2 illustrate variations in air pollution measurements throughout the research period. There were 44.68%, 46.85%, 5.7% and 2.77% average AQI values at “Good” AQI (0–50), “Moderate” AQI (51–100), “Unhealthy for sensitive groups” AQI (101–150), “Unhealthy” AQI (151–200), respectively. Both the average daily PM2.5 and PM10 were at “Good” levels for over 40% of the study period.

Dot plot of AQI (a), PM2.5 (b) and PM10 (c) percentage during the study period
The physical activity variations
Table 3 presents descriptive statistics for physical activity. The mean daily steps were 6663.97 steps. Participants on average engaged daily LPA, MPA, VPA, VVPA, MVPA and sedentary behavior was 159.22 (SD = 107.04), 59.26 (SD = 68.80), 1.59 (SD = 6.18), 0.64 (SD = 4.21), 61.49 (SD = 73.36) and 587.59 (SD = 279.42) minutes, respectively. The mean daily kcals and score of METs were 230.51 and 1.25.
The relationship between air pollution and physical activity
Table 4 illustrates the estimated impacts of AQI, PM2.5 and PM10 on individual-level daily physical activity through the fixed-effect model. Our findings indicate a converse correlation between air pollution variables and various aspects of daily physical activity, including total steps walked per day, total minutes of daily LPA, MPA and MVPA.
Total steps of daily walk demonstrated a significant negative association with AQI. A one-level increase in AQI corresponded to a decrease of 550.04 steps (95% [CI] = -858.97, -241.10; p < 0.001). Similarly, for all participants, AQI showed a significant negative association with total daily minutes of LPA, MPA, and MVPA. A one-level increase in AQI was noticed with a decline in LPA, MPA and MVPA by 10.43 min (95% [CI] = -17.07, -3.79; p < 0.001), 4.03 min (95% [CI] = -7.48, -0.59; p < 0.001) and 4.16 min (95% [CI] = -7.77, -0.56; p < 0.001), respectively.
PM2.5 demonstrated a significant negative association with total daily walking steps, LPA, MPA and MVPA among total participants. Notably, a one-level increase in PM2.5 was observed with a decrease of daily walking steps, LPA, MPA and MVPA by 361.85steps (95% [CI] = -516.53, -207.16; p < 0.001), 8.97 min (95% [CI] = -12.28, -5.66; p < 0.001), 3.73 min (95% [CI] = -5.46, -2.01; p < 0.001,) and 3.79 min (95% [CI] = -5.59, -1.98; p < 0.001), respectively.
PM10 displayed a significant negative association with total minutes of daily light physical activity, with a one-level increase in PM10, corresponding to a decline of 3.7 min in LPA (95% [CI] = -6.81, -0.59; p < 0.05). However, no significant negatively association with daily walking steps, MPA and MVPA (p > 0.05) was noticed.
Discussion
This study examined the impact of air pollution levels on physical activity among older adults in China using objective measurements. Additionally, this study is notable for being the first longitudinal study to employ objective physical activity measurements in older adults to estimate relationship between air pollution and physical activity. Moreover, it was the pioneering study to explore whether a relationship existed between AQI and physical activity among older adults.
We found that AQI, PM2.5 and PM10 were related to decreased physical activity in older adults. AQI demonstrated a strong negative association with daily walking steps, daily LPA, MPA and MVPA among all participants. This study stands as a pioneering contribution to the existing literature on elderly populations, marking the first utilization of the AQI indicator for exploring whether a relationship existed between air pollution and physical activity. Our findings align with earlier research on non-elderly age groups [39, 45,46,47]. A study on Chinese middle-aged populations showed that a one-unit increase in AQI led to a 20% decrease in physical inactivity [45]. In a longitudinal cohort study encompassing adults aged 18 years and older in California, a statistically substantial decline in accelerometer-based daily walking steps was observed with poor air quality, resulting in an 18% decrease in step counts when the AQI exceeded 200 in comparison to levels below 100 [39]. Furthermore, a cluster randomized controlled trial among Australian children showed that AQI was significantly negatively associated with physical activity, with an increase in AQI by one SD linked to a decline in MPA, VPA and MVPA by 0.86, 0.35 and 1.21 min per day, respectively [47]. It is worth noting that the AQI is defined and measured differently in different countries, making comparisons challenging. Therefore, future studies should consider conducting further research in this area.
Similar to AQI, PM2.5 was noticed to have a significantly negatively association with physical activity. A one-level increase in PM2.5 led to reduced daily walking steps, LPA, MPA and MVPA among all participants, resulting in declines of 361.85 steps, 8.97 min, 3.73 and 3.79 min per week, respectively. This association aligned with findings from subjectively measured studies undertaken in China and other countries. For example, a study reported that elderly residents in cities with PM2.5 higher concentration exhibited elevated levels of physical inactivity [48]. Our longitudinal study conducted among Beijing retirees yielded consistent conclusions [34]. Furthermore, a U.S. cross-sectional study indicated that each PM2.5 exposure class increase corresponded to a statistically substantial 16 to 35% increase in probability of physical inactivity [32]. Another cross-sectional study of elderly individuals in the United States found that for each 10-unit (µg/m3) increase in PM2.5 concentration, the odds of physical inactivity increased by 16% [33]. Furthermore, consistent conclusions have also been reached in studies involving other age groups. A longitudinal study of Chinese freshmen in our previous study demonstrated a reverse correlation between PM2.5 level and walking time and VPA [35]. Another cross-sectional study among 18–76 years of age adults also demonstrated a negative correlation between PM2.5 concentration and outdoor physical activities [49]. However, the study among adults revealed that PM2.5 exerted no effects on the average hourly physical activity, which was inconsistent with our findings [50]. One possible explanation for this inconsistency is that the ages of the participants differed from those in our study.
However, there is no significant relationship between PM10 and walking steps, MPA, or MVPA. This result may indicate that the impact of different air quality indicators on physical activity may vary: LPA is associated with AQI, PM10, and PM2.5, while walking steps, MPA and VPA are only linked to AQI and PM2.5. This finding contradicts previous results indicating a direct relationship between an increase in PM10 and increased odds of physical inactivity. A U.S. cross-sectional study demonstrated that an increasing concentration of PM10 led to heightened odds of physical inactivity [32]. A merger of data from South Korea study showed that walking time decreased by 0.22 h as PM10 increased [37]. A cohort study from London in patients with COPD reported that PM10 significantly independently associated with reduced pedometer-based daily step counts [42]. The inconsistent of results across studies may be due to factors such as the use of self-reported data in cross-sectional studies [32, 51] or study design related to short-term and long-term pollution exposures [31]. At the same time, a cross-sectional study conducted in the United States suggested that ozone, like PM2.5 and PM10, is one of the factors affecting physical activity [32], and future research should consider including this variable. This study is preliminary and replication among older adults is warranted.
Some studies advocate that physical activity can still be carried out in air polluted environments. Several health assessments support this viewpoint, indicating that the advantages of physical activity outweigh potential risks linked to air pollution [52, 53]. Public health modeling has also contributed to this perspective by examining the balance of risks and benefits between physical activity and exposure to polluted environments [54]. On the other hand, a minority of studies failed to provide evidence that air pollution exposure offsets the positive effects of physical activities [55,56,57]. In summary, the comprehensive effects of participating in physical activity in an air-polluted environment remain unclear. Future research should prioritize an examination of their risk-benefit relationship. This study has several strengths. First, we employ accelerometers to objectively measure physical activity of older adults. Many prior investigations into the correlation between air pollution and physical activity relied on subjective measurement methods, potentially introducing biases. As far as we know, this is the pioneering study employing objective physical activity data in delving into the connection of air pollution and physical activity among China’s older adults. Second, our study adopts a longitudinal design, employing an individual fixed effects model during data analysis. This approach effectively mitigates biases that can persist within participants over time. Third, our findings reveal a significant negative correlation between AQI and physical activity within the elderly population. Nevertheless, this study is not without its limitations. Firstly, we were unable to distinguish between outdoor and indoor physical activities, which could introduce variability in air pollution exposure. Secondly, it is worth noting that air pollution exposure may contribute to lagged or cumulative effects, which our study did not account for. Thirdly, our participants were recruited through convenience sampling, potentially not fully representative of all elderly individuals. Hence, further investigations are warranted to address these limitations with other information such as education and socio-economic status.
Conclusions
This study examined how air pollution is related to base-accelerometer physical activity among older adults. AQI and PM2.5 demonstrate an inverse association with physical activity levels among older adults, potentially discouraging their engagement in physical activity. Different air quality indicators may affect physical activity differently. Future studies are warranted to enhance policy interventions aimed at reducing air pollution and promoting physical activity.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to confidentially reason, but are available from the corresponding author on reasonable request.
References
Færgeman O. Climate change, disease and public health. Ugeskr Laeger. 2008;170(35):2667–8.
Cakmak S, Dales R, Leech J, Liu L. The influence of air pollution on cardiovascular and pulmonary function and exercise capacity: Canadian Health measures Survey (CHMS). Environ Res. 2011;111(8):1309–12.
Auchincloss AH, Diez Roux AV, Dvonch JT, Brown PL, Barr RG, Daviglus ML, Goff DC Jr, Kaufman JD, O’Neill MS. Associations between recent exposure to ambient fine particulate matter and blood pressure in the multi-ethnic study of atherosclerosis (MESA). Environ Health Perspect. 2008;116(4):486–91.
D’Oliveira A, Dominski FH, De Souza LC, Branco JHL, Matte DL, da Cruz WM, Andrade A. Impact of air pollution on the health of the older adults during physical activity and sedentary behavior: a systematic review. Environ Res. 2023;234:116519–116519.
Brook RD, Rajagopalan S, Pope CA, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong YL, Luepker RV, Mittleman MA et al. Particulate Matter Air Pollution and Cardiovascular Disease An Update to the Scientific Statement From the American Heart Association. Circulation: 2010, 121(21):2331–2378.
Di Novi C. The influence of traffic-related pollution on individuals’ life-style: results from the BRFSS. Health Econ. 2010;19(11):1318–44.
Anowar S, Eluru N, Hatzopoulou M. Quantifying the value of a clean ride: how far would you bicycle to avoid exposure to traffic-related air pollution? Transp Res Part A: Policy Pract. 2017;105:66–78.
Cutrufello PT, Rundell KW, Smoliga JM, Stylianides GA. Inhaled whole exhaust and its effect on exercise performance and vascular function. Inhalation Toxicol. 2011;23(11):658–67.
Marr LC, Ely MR. Effect of air pollution on marathon running performance. Med Sci Sports Exerc. 2010;42(3):585–91.
Rundell KW, Caviston R. Ultrafine and Fine Particulate Matter Inhalation decreases Exercise performance in healthy subjects. J Strength Conditioning Res. 2008;22(1):2–5.
Rohde RA, Muller RA. Air Pollution in China: mapping of concentrations and sources. PLoS ONE. 2015;10(8):1.
Greenstone M, Hanna R. Environmental regulations, air and water pollution, and infant mortality in India. Am Econ Rev. 2014;104(10):3038–72.
U.S. Department of Health and Human Services. Physical Activity Guidelines (2nd edition). In.: U.S. Department of Health and Human Services; 2018.
Chodzko-Zajko WJ. Exercise and physical activity for older adults. Kinesiol Rev. 2014;3(1):101–6.
Colman R, Walker S. The cost of physical inactivity in British Columbia. GPI Atlantic; 2004.
Seefeldt V, Malina RM, Clark MA. Factors affecting levels of physical activity in adults. Sports Med 2002, 32(3):143–68.
Ferrucci L, Izmirlian G, Leveille S, Phillips CL, Corti M-C, Brock DB, Guralnik JM. Smoking, physical activity, and active life expectancy. Am J Epidemiol. 1999;149(7):645–53.
Wang BWE, Ramey DR, Schettler JD, Hubert HB, Fries JF. Postponed development of disability in elderly runners: a 13-year longitudinal study. Arch Intern Med. 2002;162(20):2285–94.
Bruce B, Fries JF, Hubert H. Regular vigorous physical activity and disability development in healthy overweight and normal-weight seniors: a 13-year study. Am J Public Health. 2008;98(7):1294–9.
Ebrahim S, Wannamethee SG, Whincup P, Walker M, Shaper AG. Locomotor disability in a cohort of British men: the impact of lifestyle and disease. Int J Epidemiol. 2000;29(3):478–86.
Kim LG, Adamson J, Ebrahim S. Influence of life-style choices on locomotor disability, arthritis and cardiovascular disease in older women: prospective cohort study. Age Ageing. 2013;42(6):696–701.
Wannamethee SG, Ebrahim S, Papacosta O, Shaper AG. From a postal questionnaire of older men, healthy lifestyle factors reduced the onset of and may have increased recovery from mobility limitation. J Clin Epidemiol. 2005;58(8):831–40.
Swain DP, Franklin BA. Comparison of cardioprotective benefits of vigorous versus moderate intensity aerobic exercise. Am J Cardiol. 2006;97(1):141–7.
Paterson DH, Warburton DER. Physical activity and functional limitations in older adults: a systematic review related to Canada’s Physical Activity guidelines. Int J Behav Nutr Phys Act. 2010;7(1):1–22.
Roh K-H, Park H-A. A meta-analysis of the effect of walking exercise on lower limb muscle endurance, whole body endurance and upper body flexibility in elders. J Korean Acad Nurs. 2013;43(4):536–46.
Graff Zivin J, Neidell M. Days of haze: environmental information disclosure and intertemporal avoidance behavior. J Environ Econ Manag. 2009;58(2):119–28.
Noonan DS. Smoggy with a chance of Altruism: the effects of ozone alerts on Outdoor Recreation and driving in a tlanta. Policy Stud J. 2014;42(1):122–45.
Saberian S, Heyes A, Rivers N. Alerts work! Air quality warnings and cycling. Resour Energy Econ. 2017;49:165–85.
Sexton AL. Responses to air quality alerts: Do Americans spend less time outdoors? 2011.
Andrade A, Dominski FH, Coimbra DR. Scientific production on indoor air quality of environments used for physical exercise and sports practice: bibliometric analysis. J Environ Manage. 2017;196:188–200.
Tainio M, Jovanovic Andersen Z, Nieuwenhuijsen MJ, Hu L, de Nazelle A, An R, Garcia LMT, Goenka S, Zapata-Diomedi B, Bull F, et al. Air pollution, physical activity and health: a mapping review of the evidence. Environ Int. 2021;147:105954.
Roberts JD, Voss JD, Knight B. The Association of Ambient Air Pollution and Physical Inactivity in the United States. PLoS ONE. 2014;9(3):e90143.
Wen X-J, Balluz L, Mokdad A. Association between Media alerts of Air Quality Index and Change of Outdoor Activity among Adult Asthma in Six States, BRFSS, 2005. J Community Health. 2009;34(1):40–6.
Yu H, An R, Andrade F. Ambient fine particulate Matter Air Pollution and physical activity: a longitudinal study of University retirees in Beijing, China. Am J Health Behav 2017, 41(4):401–10.
An R, Yu H. Impact of ambient fine particulate matter air pollution on health behaviors: a longitudinal study of university students in Beijing, China. Public Health. 2018;159:107–15.
Kim H. Seasonal impacts of particulate matter levels on Bike sharing in Seoul, South Korea. In: Int J Environ Res Public Health 17; 2020.
Kim M-G, Lee S-J, Park D, Kim C-h, Lee K-h. Hwang J-m: relationship between the actual fine dust concentration and media exposure that influenced the changes in outdoor activity behavior in South Korea. Sci Rep. 2020;10(1):12006.
Xiong L, Li J, Xia T, Hu X, Wang Y, Sun M, Tang M. Risk reduction behaviors regarding PM2.5 exposure among Outdoor exercisers in the Nanjing Metropolitan Area, China. In: Int J Environ Res Public Health 15; 2018.
Rosenthal DG, Vittinghoff E, Tison GH, Pletcher MJ, Olgin JE, Grandis DJ, Marcus GM. Assessment of Accelerometer-based physical activity during the 2017–2018 California Wildfire Seasons. JAMA Netw Open 2020, 3(9):e2018116–2018116.
Kim Y-B, McCurdy AP, Lamboglia CG, Hakimi S, Kuzik N, Lee E-Y, Lindeman C, Sivak A, Spence JC. Ambient air pollution and movement behaviours: a scoping review. Health Place. 2021;72:102676.
Carlisle AJ, Sharp NCC. Exercise and outdoor ambient air pollution. Br J Sports Med. 2001;35(4):214–22.
Alahmari AD, Mackay AJ, Patel ARC, Kowlessar BS, Singh R, Brill SE, Allinson JP, Wedzicha JA, Donaldson GC. Influence of weather and atmospheric pollution on physical activity in patients with COPD. RESPIRATORY RESEARCH; 2015. p. 16.
Butte NF, Ekelund U, Westerterp KR. Assessing physical activity using wearable monitors: measures of physical activity. Med Sci Sports Exerc. 2012;44(Suppl 1):S5–12.
Freedson PS, Melanson E, Sirard J. Calibration of the computer science and applications, Inc. accelerometer. Med Sci Sports Exerc. 1998;30(5):777–81.
Chen D-R, Lin Y-C. Social identity, perceived urban neighborhood quality, and physical inactivity: a comparison study of China, Taiwan, and South Korea. Health Place. 2016;41:1–10.
Hu L, Zhu L, Xu Y, Lyu J, Imm K, Yang L. Relationship between Air Quality and Outdoor Exercise Behavior in China: a Novel Mobile-based study. Int J Behav Med 2017, 24(4):520–7.
del Pozo Cruz B, Hartwig TB, Sanders T, Noetel M, Parker P, Antczak D, Lee J, Lubans DR, Bauman A, Cerin E, et al. The effects of the Australian bushfires on physical activity in children. Environ Int. 2021;146:106214.
Wells EM, Dearborn DG, Jackson LW. Activity change in response to Bad Air Quality, National Health and Nutrition Examination Survey, 2007–2010. PLoS ONE. 2012;7(11):e50526.
Wang R, Liu Y, Xue D, Yao Y, Liu P, Helbich M. Cross-sectional associations between long-term exposure to particulate matter and depression in China: the mediating effects of sunlight, physical activity, and neighborly reciprocity. J Affect Disord. 2019;249:8–14.
Wang G, Li B, Zhang X, Niu C, Li J, Li L, Speakman JR. No seasonal variation in physical activity of Han Chinese living in Beijing. Int J Behav Nutr Phys Activity. 2017;14(1):48.
Zwolinsky S, McKenna J, Pringle A, Widdop P, Griffiths C. Physical activity assessment for public health: efficacious use of the single-item measure. Public Health. 2015;129(12):1630–6.
De Hartog JJ, Boogaard H, Nijland H, Hoek G. Do the health benefits of cycling outweigh the risks? Environmental health perspectives 2010, 118(8):1109–16.
Buekers J, Dons E, Elen B, Panis LI. Health impact model for modal shift from car use to cycling or walking in Flanders: application to two bicycle highways. J Transp Health. 2015;2(4):549–62.
Tainio M, de Nazelle AJ, Götschi T, Kahlmeier S, Rojas-Rueda D, Nieuwenhuijsen MJ, de Sá TH, Kelly P, Woodcock J. Can air pollution negate the health benefits of cycling and walking? Preventive medicine 2016, 87:233–6.
Laeremans M, Dons E, Avila-Palencia I, Carrasco-Turigas G, Orjuela JP, Anaya E, Cole-Hunter T, De Nazelle A, Nieuwenhuijsen M, Standaert A. Short-term effects of physical activity, air pollution and their interaction on the cardiovascular and respiratory system. Environ Int. 2018;117:82–90.
Avila-Palencia I, Laeremans M, Hoffmann B, Anaya-Boig E, Carrasco-Turigas G, Cole-Hunter T, de Nazelle A, Dons E, Götschi T, Panis LI. Effects of physical activity and air pollution on blood pressure. Environ Res. 2019;173:387–96.
Kubesch NJ, De Nazelle A, Westerdahl D, Martinez D, Carrasco-Turigas G, Bouso L, Guerra S, Nieuwenhuijsen MJ. Respiratory and inflammatory responses to short-term exposure to traffic-related air pollution with and without moderate physical activity. Occupational and environmental medicine 2015, 72(4):284–93.
Acknowledgements
We express our appreciation to all the participants in the study. Also thanks to Diqiao Chen (pass away in 2022), Suozhu Hao for helping us to recruit Beijing participants, Weiqing zhang, Huizhong Chen, and Zhiqiang Feng recruited Shijiazhuang participants, and Chenxiao Zhang for Qinzhou participants.
Funding
This study was supported by the Beijing Municipal Social Science Foundation of China (No. 21YTA009), the Science Foundation of Hebei Normal University (No. L2024B45), the Tsinghua University “Shuang Gao” Scientific Research Program (No. 2021TSG08208), and the National Social Science Foundation of China (No. 19VXK10).
Author information
Authors and Affiliations
Contributions
JL.C.: Data collection, data analysis, writing original draft and review the original and final draft. HJ.Y.: Conceptualization, data analysis, review the original and final draft. Y.W. and XX.W.: Data collection. All authors have reviewed and endorsed the final version of the manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Tsinghua University Institutional Review Board (IRB 20110170). Written informed consent was obtained from all participants involved in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cheng, J., Wu, Y., Wang, X. et al. Objectively measured the impact of ambient air pollution on physical activity for older adults. BMC Public Health 24, 821 (2024). https://doi.org/10.1186/s12889-024-18279-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18279-2