
Abstract
Background
Cervical cancer accounts for 7.5% of all female cancer related deaths worldwide; peaking between the ages of 35 and 65, and not only kills young women but also destroys families with young children.
Objective
This review was intended to measure national level magnitude and the most common predictors of cervical cancer related mortality in Ethiopia.
Methods
Common Public databases like Science Direct, Embase, the Cochrane Library, and PubMed were thoroughly searched. The STATA 14 and Rev-Manager 5.3 statistical software packages were used for analysis, as well as a standardized data abstraction tool created in Microsoft Excel. The Cochrane Q-test statistics and the I2 test were used to assess non-uniformity. The pooled magnitude and predictors of cervical cancer related mortality were estimated using fixed-effect and random-effect models, respectively.
Result
The pooled mortality among cervical cancer patients was estimated that 16.39% at 95% confidence level fall in 13.89–18.88% in Ethiopia. The most common predictors of cervical cancer related mortality were late diagnosed, radiation therapy alone, and Being anemic were identified by this review. Among cervical cancer treatment modalities effectiveness of surgery with adjuvant therapy was also approved in this meta-analysis.
Conclusion and recommendation
In this study high cervical cancer-related mortality was reported as compared to national strategies to alleviate cervical cancer related mortality. Advanced implementation of cervical cancer screening at the national level for early diagnosis, anaemia detection, and combination anticancer therapy during initiation, as well as combination therapy, is critical to improve cervical cancer patient survival and decreasing mortality rates.
Similar content being viewed by others

Background
In 2018, there were an estimated 570,000 cases and 311,000 deaths from cervical cancer worldwide, making it one of the top four common causes of cancer-related mortality among women [1]. Worldwide cancer-related death figures show that developed countries accounted for 85% of cervical cancer mortality, with low- and middle-income countries having an 18-fold higher death rate from the disease [2]. Cervical cancer is caused by oncogenic subtypes of the human papillomavirus [3]. The disease that kills young women and destroys families with small children also causes 7.5% of cancer-related deaths among women globally, with a peak incidence between the ages of 35 and 65 [4, 5].
As a result of population ageing and growth, as well as an increase in the prevalence of risk factors associated with economic change, such as smoking, obesity, physical inactivity, and reproductive behaviors, cancer is becoming more prevalent in Africa [6]. In Eastern, Western, Middle, and Southern Africa, women die from cancer mostly from cervical cancer [7]. Cervical cancer is expected to kill over 443,000 women worldwide by 2030, the vast majority of whom will be in Sub-Saharan Africa [8].
Each year, approximately 6,300 new cases of cervical cancer are diagnosed in Ethiopia cancer treatment centers, and approximately 4,884 women die from the disease [9]. According to data from TikurAnbesa Specialized Hospital (TASH) radiotherapy center, cervical cancer is the second most common type of cancer among patients attending the oncology center [10]. According to various sources, treatment options include surgery, chemotherapy, radiotherapy, or a combination of the three [11,12,13].
There is no study which shows country level of magnitude of cervical cancer related death and predictors of this mortality irrespective of tremendous updated cervical cancer therapies. Thus, this study was designed to measure overall magnitudes of cervical cancer related mortality and its predictors.
Conducting a review study as a strategy evaluation is so mandatory. Additionally, there is no finding that has been used to raise public awareness about predictors of death among cervical cancer patients, which paves the way for preventive and curative approaches for early detection and proper treatment.
Methods
Study protocol
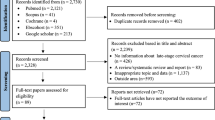
This study’s protocol was based on the PRISMA recommendations for systematic reviews and meta-analyses [14]. Three distinct researchers worked independently to finish each step. The screening was based on methodological issues, incomplete data, or full text that was not accessible from the analysis [15]. The fourth researcher resolved any disagreements by examining whether the results were consistent. Additionally articles published in English online from university repositories were also considered. Then, described by Preferred Reporting Items for Systematic Review and Meta-analysis protocol (PRISMA-P) (fig. 1). (Additional file 1)

PIRSMA flowchart diagram of included article
Objective of the study
-
To determine the national-level pooled magnitude cervical cancer related mortality.
-
To identify predictors associated with cervical cancer related mortality.
-
To detect heterogeneity between the studies at the national level.
Sources of data and ways of search
Common Public databases like Articles conducted on pediatrics virological failure were searched in Google Scholar, PubMed, Embase, and Cochrane Library search engine using different Medical Subject Heading (MeSH). The search terms were used individually as well as in conjunction with Boolean operators such as “OR” and “AND.” Citations discovered using our search terms were imported into EndNote-X6 software, and duplicate articles were removed. (Additional file 2).
Inclusion and exclusion criteria
The review attempted to include published studies with epidemiological data on cervical cancer mortality and predictors conducted. The PICOS evidence-based medicine framework served as our basis for inclusion criteria, and nonrandomized studies met the following PICOS-standardized components [16].
PICO (population, intervention, comparator and outcome) of the study.
P: Cervical cancer patients.
I: Categories of variables those are positively associated with virological failure.
C: Categories of variables those are significantly associated with PPD.
O: Pediatrics with HIV infection and on ART experienced virological failure.
The following points were used as exclusion criteria.
-
1)
Studies with sample sizes with cervical cancer and other comorbidities..
-
2)
Studies included more than 18-year-old participants..
-
3)
Studies that reported immunological and mixed measurements..
-
4)
Studies that reported un-operationalized out come..
-
5)
Complete data, i.e., lack of variable of interest..
Assessment of quality of included studies
Newcastle-Ottawa Scale assessment of Critical Appraisal Checklist for non-randomized Studies was used to determined quality status of the article and included articles were accepted at the level of above mean score out of 14 overall score [17]. (Additional file 3)
Measurements of outcome
Death among cervical cancer was considered as cervical cancer related mortality and Predictors were factors those consistently with mortality in more than or four articles were considered in this meta- analysis.
Characteristics of included studies
This meta-analysis included 14 studies that reported on the magnitude and predictors of mortality among cervical cancer patients in Ethiopia. Totally, 9,260 cervical cancer patients were included in the study. Articles published between January 2013 and March 30, 2023 was taken into account. This study looked at the most common predictors of mortality in cervical cancer patients. Those predictors were, late diagnosis [18,19,20,21], radiation therapy only [10, 22, 23], surgery with adjuvant therapy [24,25,26] and anemic status of the patient [27,28,29] were selected based on their frequency identified as the predictors by different studies (Table 1).
Data extraction techniques
The necessary data was taken from a predetermined set of articles using a Microsoft Excel template. The name of the author, the year of publication, the location, the age range, the sample size, the response rate, the number of study subjects with the desired outcome, the prevalence rates, and the predictors significantly associated with death from cervical cancer were all contained in a Microsoft Excel spreadsheet. (Additional file 4 and Additional file 5)
Data synthesis and analysis
The heterogeneity inverse variance (I2) test was used to assess study non-uniformity, and Cochran’s Q test (P-value less than 0.1) revealed statistically significant results [30].. The I2 value ranges from 0 to 100%. I2 75% indicates that there is significant heterogeneity across studies, with a P-value of 0.05 used to declare significant heterogeneity [31]. The pooled size magnitude of cervical cancer related mortality was estimated using a random effect model because I2 = 78.50 at p = 0.00, indicating the presence of heterogeneity between studies. Furthermore, we used a random model for subgroup analysis by identified predictors to deal with the significance of their significance in cervical cancer-related mortality at I2 = 96.4%, indicating high heterogeneity across studies [32].
Publication bias assessment
A funnelplot graph was used visually to assess publication bias. The symmetry of the funnel plot revealed that there was no potential publication bias [33] (Fig. 2). Egger’s and Begg’s tests were also run at the 5% significant level; the distribution of each study, as well as a P-value greater or less than 0.05, were used to determine the presence or absence of publication bias [30] (Table 2).

Funnel plot for test of publication bias
The Egger’s test output also indicates that there is no publication bias at (P = 0.825). However, the result of Begg’s test was notable in the presence of minimal publication bias (P = 0.047). Trim and fill analysis was thus performed following pooled effect analysis (Fig. 2)
Result
Pooled effect size of mortality among cervical cancer patients in Ethiopia
The pooled mortality among Ethiopian cervical cancer patients was 16.39% (95% confidence level; 13.89-18.88%). Because of heterogeneity was observed between the included primary studies at I2 = 90.50% and P = 0.00, we used random effect model to compute the pooled effect size of mortality among cervical cancer patients as described by figure of forest plot below (Fig. 3).

Forest plot showing pooled effect size of cervical cancer in Ethiopia
Regression analysis of study uniformity
Meta-regression was used to identify the source of non-uniformity, and p-values greater than 0.1 revealed that there was no statistically significant non-uniformity between the studies (Table 3).
A sensitivity analysis was also performed to determine the effect size of each study on the pooled effect size. Two investigators carried out the statistical analysis independently, and the results were cross-checked for reliability, (Fig. 4).

Sensitivity analysis of included studies
Trim and fill analysis
The pooled magnitude was changed from [16.39% (95% CI, 13.89%, 18.88%)] to [16.39% (13.23%, 19.42%)] after trim and fill analysis. The egger test only detected minimal publication bias; however, since the later confidence interval includes the first pooled size, there is no conspicuous difference between them which affects the final effect sizes (Fig. 5).

Trim and fill analysis for correcting publication bias of 14 studies
Predictors of mortality among cervical cancer patients in Ethiopia
After thoroughly literature review, we selected four commonly significant predictors of mortality among cervical cancer patients based on the frequency of being considered by different studies. Late diagnosed [RR = 2.65, 95% CI: (2.16, 3.26)], radiation therapy only [RR = 2.21, 95% CI: 1.65, 2.96], and being anemic [RR = 3.20, 95% CI: 1.73, 5.91] are the most common aggregate predictors of mortality for cervical cancer patients. Each of them was discussed by more than three studies.
Another goal was to realize how recombinant therapy could decrease cervical cancer related mortality and improve survival rate of the patients had been identified from four studies conducted on survival of patients with cervical cancer. Survival status of cervical cancer patients can be increased as a result of surgery with adjuvant therapy when compared with cervical cancer patients treated by radiation therapy only [RR = 0.55, 95% CI: (0.41, 0.73)]. Thus, the output of our Meta analysis forwarded that 45% of mortality from cervical cancer can be averted by combination therapy than non-recombinant therapy (Fig. 6).

Forest plot briefing predictors of cervical cancer related mortality in Ethiopia
Discussion
It was crucial to carry out a systematic review and meta-analysis in order to offer national strategic designers of the health sector advice. Despite the development of new cervical cancer therapies, significant mortality rates are still reported in low and middle-income countries [34, 35]. This could be due to the use of non-preferred methods and the limitations of care provisions, as well as the inability of patients in developing countries to cover the cost of therapy [34].
We carried out this review using data from 14 studies which included 9,260 cervical cancer patients. In accordance with the current meta-analysis, the pooled magnitude of cervical cancer patients’ mortality was reported as 16.39% with 95% confidence interval. This finding is consistent with the findings of a study done in America among non-Hispanic African American and white women, which reported a 14.2% death rate and a 13.3% review of LMIC, but more than the 5.49% found in urban China studies [5] and the two studies conducted in USA 7.9–11.9% and 4% respectively [35]. However our finding is less than review conducted in Thailand Bhutan 22.7% [36] and interventional study done in India which reports 25.32% died in the chemotherapy plus surgery group and 25.24% died in the concomitant chemotherapy plus radiotherapy group [37]. The reasons of this variation might be the difference between study design, characteristics of study population, treatment modalities and sociodemographic characteristics of the patients.
Among the common predictors of cervical cancer related mortality, late diagnosis of the disease was identified by this review. Four articles in which late diagnosis commonly discussed as the predictor were selected and analyzed, as seen from the above forest plot. From this finding, the risk of dying among late diagnosed cervical cancer patients were 2.65 times more likely when compared to those diagnosed early. The reason might be lack of cervical cancer screening awareness in developing countries increases progression of pre-cervical cancer lesion into invasive malignant stages which can metastasis to vital organs and have poor prognosis of the diseases, thus increases cervical cancer related mortality [38]. Furthermore, evidence of this suggests that five year survival rate for early diagnosed cervical cancer is 70% when compared to stage IIB to stage IV in which they have less than 20% survival rate [39]. As cancer stage increases, malignant metastasis also increase, which leads to compromising patient’s immunity to resist other infections, difficulty of treating the cases and these factors in aggregate increases the probability of death. This determinant was also reported by different literatures [40, 41].
This study also measured the contribution of combination of surgery with adjuvant therapy to alleviate cervical cancer related mortality. According to the pooled protective effect of recombinant therapy from these studies, 45% of cervical cancer related mortality can be averted by surgery with adjuvant therapy modality. The reason for this could be that, while surgical therapy is determined by tumour size and cancer stage, different evidence strongly suggests surgery to reduce tumour size and remove partial if all impossible. Adjuvant therapy is then used to reduce the rate of anaplasia and thus the cancer cell’s invasive capacity [42, 43].
The reports of four studies focused on contribution of radiation therapy only treatment modality to cervical cancer related mortality also selected in this review. The reports of those studies were examined at 95% confidence level. Thus the odds of cervical cancer related mortality among patient treated by radiation alone were 2 times more likely when compared with the patient treated by other treatment modalities. The reason for this could be that immunotherapy can achieve a synergistic effect with radiotherapy by directly inducing immunogenic death of tumour cells [44] reestablishing tumour vessels and regulating tumour cell phenotype [45], allowing immune cell infiltration and systemic therapeutic drug local infiltration [42, 46]. Acute and Long term toxicity of radiation therapy alone also supported by another study [47].
Being anemic was identified as the fourth most predictor of the cervical cancer related mortality from the four studies. The risk of death by cervical cancer patient increases three times as compared to normal hematocrit patients. This result implies that the risk of dying from cervical cancer was 3.2 times higher in patients with anaemia than in the control group. This could be because low hemoglobin levels in the blood cause oxygen deprivation in both cancerous and normal cells, resulting in tissue necrosis and exacerbating malignancy and cancer cell invasive capacity [48, 49]. The current finding is supported by the studies conducted in Canada [50] and Japan [51]. Synergic effect of anemia to cervical cancer related mortality is so preventable with effective implementation of its managements [52]. However, in this meta-analysis, anemia was highly significant to increase cervical cancer related mortality, but correction of anemia is so first priority to improve survival of cervical cancer patients while initiation of direct cancer patient therapy [53].
Conclusion
The finding of this systematic review and meta-analysis reported high cervical cancer-related mortality at national level. Cervical cancer mortality was found to be strongly linked with late diagnosis and anaemia. However, this meta-analysis found that combining surgery with adjuvant therapy was associated with a significant decrease in cervical cancer-related mortality. This review also discovered that radiation therapy alone without combination therapy is less effective to improve cervical cancer patient survival than recombinant chemotherapy.
The report of our meta-analysis recommends that early diagnosis of tumor stage through cervical cancer screening program improves survival of cervical cancer. Furthermore, surgery with adjuvant therapy more encouraged to increase survival rate of cervical cancer patients. This meta-analysis disproves radiation therapy alone as a treatment modality for cervical cancer, as it did not improve patient survival. Accordingly, this finding supports the use of combination treatment modalities for cervical cancer. It is expected that future research better focus on comorbid treatment of cervical cancer patients to increase drug efficacy and to develop better treatment modalities.
Limitation of the study
Most of the studies conducted in developing countries are non-randomized, as the cost-effectiveness of the studies for resources is limited. Thus, this meta-analysis included only non-randomized studies. Therefore, in the future, researchers should better focus on laboratory-based studies to identify predictors of cervical cancer-related mortality.
Data availability
The datasets used and/or analyzed during the current study are available freely and openly accessed in this article is supplemented.
Abbreviations
- AFT:
-
Accelerated failure time
- CIN:
-
Cervical intraepithelial neoplastic
- HIV:
-
Human immunodeficiency virus
- HPV:
-
Human papillomavirus infection
- CI:
-
Confidence interval
- I2 :
-
Inverse variance
- OR:
-
Odds ratio
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-analysis
- SE:
-
Standard error
- SNNPR:
-
Southern Nations and Nationalities of Ethiopia
- WHO:
-
World Health Organization
References
Bray F, Ferlay J, Soerjomataram I, Siegel R, Torre L, et al. Erratum: global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca Cancer J Clin. 2020;70:313.
Hull R, Mbele M, Makhafola T, Hicks C, Wang SM, et al. Cervical cancer in low and middle-income countries. Oncol Lett. 2020;20:2058–74.
Olusola P, Banerjee HN, Philley JV, Dasgupta S. (2019) Human Papilloma Virus-Associated Cervical Cancer and Health disparities. Cells 8.
Jalil, Aat epidemiology of cervical cancer and high risk of human papilloma virus in patient. ББК 286 З 85.
Chen T, Wei M, Liu Y, Wang H, Zhou W, et al. Rising mortality rate of cervical cancer in younger women in urban China. J Gen Intern Med. 2020;35:593–3.
Burt LM, McCormak M, Lecuru F, Kanyike DM, Bvochora-Nsingo M, et al. Cervix Cancer in Sub-saharan Africa: an Assessment of Cervical Cancer Management. JCO Glob Oncol. 2021;7:173–82.
Jordaan S, Michelow P, Richter K, Simoens C, Bogers J. A review of cervical cancer in South Africa: previous, current and future. Health Care Curr Rev. 2016;4:2.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71:209–49.
Abate SM. Trends of Cervical Cancer in Ethiopia. Gynecology & Obstetrics s3; 2017.
Moelle U, Mathewos A, Aynalem A, Wondemagegnehu T, Yonas B, et al. Cervical Cancer in Ethiopia: the Effect of Adherence to Radiotherapy on Survival. Oncologist. 2018;23:1024–32.
Hoffman BL. Williams Gynecology. THIRDEDITION: McGraw-Hill Education; 2016.
Health OW. (2007) Cancer Control: Knowledge into Action: WHO Guide for Effective Programmes: Module 2: Prevention. Geneva: © World Health Organization 2007.
Green JA, Kirwan JJ, Tierney J, Vale CL, Symonds PR, et al. Concomitant chemotherapy and radiation therapy for cancer of the uterine cervix. Cochrane database of systematic reviews; 2005.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–89.
Roever L. Critical appraisal of cohort studies. Evid Based Med Pract. 2015;1:e108.
Amir-Behghadami M, Janati A. Population, intervention, comparison, outcomes and study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emergency Medicine Journal; 2020.
Peterson J, Welch V, Losos M, Tugwell P. (2011) The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute 2: 1–12.
Aguade AE, Gashu C, Jegnaw T. The trend of change in cervical tumor size and time to death of hospitalized patients in northwestern Ethiopia during 2018–2022: retrospective study design. Health Sci Rep. 2023;6:e1121.
Argefa TG, Roets L. Malnutrition and the survival of cervical cancer patients: a prospective cohort study using the PG-SGA tool. Nutr Cancer. 2022;74:605–12.
Begoihn M, Mathewos A, Aynalem A, Wondemagegnehu T, Moelle U, et al. Cervical cancer in Ethiopia–predictors of advanced stage and prolonged time to diagnosis. Infect Agents cancer. 2019;14:1–7.
Kantelhardt EJ, Moelle U, Begoihn M, Addissie A, Trocchi P, et al. Cervical cancer in Ethiopia: survival of 1,059 patients who received oncologic therapy. Oncologist. 2014;19:727–34.
Gurmu SE. Assessing survival time of women with cervical cancer using various parametric frailty models: a case study at Tikur anbessa specialized hospital, Addis Ababa, Ethiopia. Annals Data Sci. 2018;5:513–27.
Mebratie AE, Moges NA, Meselu BT, Melesse MF. Time to death from cervical cancer and predictors among cervical cancer patients in Felege Hiwot Comprehensive Specialized Hospital, North West Ethiopia: facility-based retrospective follow-up study. PLoS ONE. 2022;17:e0269576.
Gashu C, Tasfa B, Alemu C, Kassa Y. (2023) Assessing survival time of outpatients with cervical cancer: at the university of Gondar referral hospital using the bayesian approach. BMC Womens Health 23.
Deressa BT, Assefa M, Tafesse E, Kantelhardt EJ, Soldatovic I, et al. Contemporary treatment patterns and survival of cervical cancer patients in Ethiopia. BMC Cancer. 2021;21:1–7.
Fikeraddis T, Tigistu G, DHUGASA B. Treatment outcome and associated factors among cervical cancer patients treated at Tikur Anbesa Specializsed hospital Addis Ababa, Ethiopia a retrospective study. Oncology. 2018;3:12–29.
Gizaw M, Addissie A, Getachew S, Ayele W, Mitiku I, et al. Cervical cancer patients presentation and survival in the only oncology referral hospital, Ethiopia: a retrospective cohort study. Infect Agents cancer. 2017;12:1–7.
Seifu B, Fikru C, Yilma D, Tessema F. Predictors of time to death among cervical cancer patients at Tikur Anbesa specialized hospital from 2014 to 2019: a survival analysis. PLoS ONE. 2022;17:e0264369.
Wassie M, Argaw Z, Tsige Y, Abebe M, Kisa S. Survival status and associated factors of death among cervical cancer patients attending at Tikur Anbesa Specialized Hospital, Addis Ababa, Ethiopia: a retrospective cohort study. BMC Cancer. 2019;19:1–11.
Israel H, Richter RR. A guide to understanding meta-analysis. J Orthop Sports Phys Therapy. 2011;41:496–504.
Egger M, Smith GD, Phillips AN. Meta-analysis: principles and procedures. BMJ. 1997;315:1533–7.
Perera R, Heneghan C. Interpreting meta-analysis in systematic reviews. BMJ Evidence-Based Med. 2008;13:67–9.
Hoy D, Brooks P, Woolf A, Blyth F, March L, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012;65:934–9.
Althabe F, Belizán JM, McClure EM, Hemingway-Foday J, Berrueta M, et al. A population-based, multifaceted strategy to implement antenatal corticosteroid treatment versus standard care for the reduction of neonatal mortality due to preterm birth in low-income and middle-income countries: the ACT cluster-randomised trial. Lancet. 2015;385:629–39.
Basso O, Wilcox A. Mortality risk among preterm babies: immaturity vs. underlying pathology. Epidemiol (Cambridge Mass). 2010;21:521.
Tshewang U, Satiracoo P, Lenbury Y. Survival analysis of Cervical Cancer patients: a case study of Bhutan. Asian Pac J Cancer Prevention: APJCP. 2021;22:2987.
Balasubramaniam G, Gaidhani RH, Khan A, Saoba S, Mahantshetty U, et al. Survival rate of cervical cancer from a study conducted in India. Indian J Med Sci. 2021;73:203–11.
Waxman AG. Guidelines for cervical cancer screening: history and scientific rationale. Clin Obstet Gynecol. 2005;48:77–97.
Carneiro SR, Fagundes MdA, do Rosário PdJO, Neves LMT, Souza GS et al. (2017) Five-year survival and associated factors in women treated for cervical cancer at a reference hospital in the Brazilian Amazon. PLoS One 12: e0187579.
Mehta N, Desai SM, Dhakad V, Patel D, Saldanha E. Treatment and outcomes of early and operable recurrent cervical Cancer: a prospective study. Niger J Surg. 2021;27:28–32.
Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R. Cancer of the cervix uteri: 2021 update. Int J Gynecol Obstet. 2021;155:28–44.
Karimi H, Soleimanjahi H, Abdoli A, Banijamali RS. Combination therapy using human papillomavirus L1/E6/E7 genes and archaeosome: a nanovaccine confer immuneadjuvanting effects to fight cervical cancer. Sci Rep. 2020;10:1–15.
Yang X, Ren H, Fu J. Combinations of radiotherapy with immunotherapy in cervical cancer. J Cancer. 2022;13:1480–9.
Nakamura H, Taguchi A, Kawana K, Baba S, Kawata A, et al. Therapeutic significance of targeting survivin in cervical cancer and possibility of combination therapy with TRAIL. Oncotarget. 2018;9:13451.
Eckert F, Jelas I, Oehme M, Huber SM, Sonntag K, et al. Tumor-targeted IL-12 combined with local irradiation leads to systemic tumor control via abscopal effects in vivo. Oncoimmunology. 2017;6:e1323161.
Fang M, Kan Y, Dong D, Yu T, Zhao N, et al. Multi-habitat based radiomics for the prediction of treatment response to concurrent chemotherapy and radiation therapy in locally advanced cervical cancer. Front Oncol. 2020;10:563.
Maduro JH, Pras E, Willemse PHB, de Vries EGE. Acute and long-term toxicity following radiotherapy alone or in combination with chemotherapy for locally advanced cervical cancer. Cancer Treat Rev. 2003;29:471–88.
Dunst J, Kuhnt T, Strauss HG, Krause U, Pelz T, et al. Anemia in cervical cancers: impact on survival, patterns of relapse, and association with hypoxia and angiogenesis. Int J Radiation Oncology* Biology* Phys. 2003;56:778–87.
Lim S, Lee C-M, Park J-M, Jung S-Y, Lee K-B. An association between preoperative anemia and poor prognostic factors and decreased survival in early stage cervical cancer patients. Obstet Gynecol Sci. 2014;57:471–7.
Koulis TA, Kornaga EN, Banerjee R, Phan T, Ghatage P, et al. Anemia, leukocytosis and thrombocytosis as prognostic factors in patients with cervical cancer treated with radical chemoradiotherapy: a retrospective cohort study. Clin Translational Radiation Oncol. 2017;4:51–6.
Yanazume S, Karakida N, Higashi R, Fukuda M, Togami S, et al. Tumor bleeding requiring intervention and the correlation with anemia in uterine cervical cancer for definitive radiotherapy. Jpn J Clin Oncol. 2018;48:892–9.
Candelaria M, Cetina L, Dueñas-González A. Anemia in cervical cancer patients: implications for iron supplementation therapy. Med Oncol. 2005;22:161–8.
Moreno–Acosta P, Carrillo S, Gamboa O, Romero–Rojas A, Acosta J, et al. Novel predictive biomarkers for cervical cancer prognosis. Mol Clin Oncol. 2016;5:792–6.
Acknowledgements
We thank all the authors of the articles we used as our inputs and our colleges for the guidance and encouragement they gave us.
Funding
No fund was given for this study.
Author information
Authors and Affiliations
Contributions
Conceptualization: HDH, BTA, BA, and AG. Data curation: HDH, BTA, AG and BA. Formal analysis: HDH and BTA. Methodology: HDH and BA. Writing original draft: HDH and AG. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable for this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hambisa, H.D., Asfaha, B.T., Ambisa, B. et al. Common predictors of cervical cancer related mortality in Ethiopia. A systematic review and meta-analysis. BMC Public Health 24, 852 (2024). https://doi.org/10.1186/s12889-024-18238-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-18238-x