
Abstract
Background
The evidence regarding the effect of earthquake exposure on the development of cardiovascular diseases is limited. This study evaluated the association between the 2016 Gyeongju earthquake, which had a magnitude of 5.8, and over 600 subsequent aftershocks occurring within a year in Korea, with the development of ischemic heart disease (IHD) among residents of Gyeongju.
Methods
Ten years (2010–2019) of medical records from a randomly selected cohort of residents (n = 540,858) in Gyeongju and 3 control cities were acquired from the national health insurance service. Employing difference-in-difference and meta-analyses, the risks of IHD development of Gyeongju residents before (reference: Sep 2014 to Aug 2015; period 1: Sep 2015 to Aug 2016) and after (period 2: Sep 2016 to Aug 2017; period 3: Sep 2017 to Aug 2018; period 4: Sep 2018 to Aug 2019) the earthquake were estimated.
Results
The monthly average incidence of IHD in Gyeongju was 39.5 persons (per 1,000,000) for reference period and 38.4 persons for period 1. However, the number increased to 58.5 persons in period 2, and 49.8 persons in period 3, following the earthquake. The relative risk (RR) [with a 95% confidence interval] of developing IHD among Gyeongju residents increased by 1.58 times (1.43, 1.73) in period 2, 1.33 times (1.21, 1.46) in period 3, and 1.15 times (1.04, 1.27) in period 4, in comparison to both the control cities and the pre-earthquake reference period. The increase in RR was particularly noticeable among women, adults aged 25–44, and individuals with lower incomes.
Conclusions
The major earthquake in Korea was associated with an increase in the development of IHD among local residents. Individuals exposed to earthquakes may benefit from cardiovascular health surveillance.
Similar content being viewed by others

Backgrounds
The Gyeongju earthquake, a seismic event with a moment magnitude of 5.8, occurred in Korea on September 12, 2016. This earthquake marked the most formidable seismic activity observed in Korean history [1, 2]. The estimated property loss was 10 million US dollars, and 632 aftershocks occurred over a year [3].
Disasters result in direct casualties and are known to affect mental health, especially in individuals who experience the loss of family, friends, and property [4]. Physical and mental stress following a disaster might lead to increased sympathetic tone and ultimately induce cardiovascular events [5]. Several review articles have reported increased rates of cardiovascular diseases and mortality in earthquake-affected regions [5,6,7].
Most previous studies on earthquakes and cardiovascular disease used time-series or cross-sectional study design by temporally comparing the number of hospital visits [8,9,10] or mortalities [11, 12] before and after the earthquake. Studies involving proper geographical controls have rarely been conducted [6, 13,14,15], and studies on the chronic effects of earthquakes on cardiovascular health using a cohort design were scarce [6, 8]. In addition, the lack of detailed personal medical histories in previous studies makes it difficult to elucidate the effects of earthquakes on new disease development [8, 16, 17].
The health insurance system of Korea registers all the hospital visit information of entire Koreans in a single database [18]. Earlier research employed the database to assess the immediate effects of an earthquake on the emergence of specific illnesses [3, 19]. Because hospital information is stored longitudinally, not only acute but also years of long-term effects of earthquakes and series of secondary shocks can be evaluated with the database.
Although the Gyeongju earthquake was the largest earthquake ever recorded in Korea, its magnitude and resulting damage were relatively small compared with those of the major earthquakes in history [3]. There were no direct casualties, and only 23 people were injured due to the earthquake [2]. However, its unexpected nature and the yearlong aftershocks might have led to mental and physical stress, ultimately affecting cardiovascular health [5, 6]. Therefore, it might be meaningful to evaluate whether earthquakes with limited casualties and property loss but long-lasting aftershocks can affect the cardiovascular health of residents exposed to the earthquake.
Therefore, this study examined the association between the 2016 Gyeongju earthquake and the risk of ischemic heart disease (IHD) development. The nationwide health insurance data was used to facilitate temporal and location-based comparisons of disease development.
Materials and methods
Study design
The difference-in-difference (DID) framework was used in this study [20]. If there were no external effects other than the earthquake, comparing the disease incidence rate before and after the earthquake-affected region (first difference) is considered a good estimate of the earthquake’s effect. To guard against the possibility of external effects, the same difference (second difference) in the control region (region not affected by the earthquake) was subtracted from the previous difference (first difference) to calculate the DID estimates.
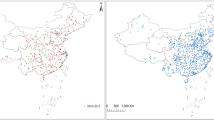
Considering the impact area of the Gyeongju earthquake (Fig. 1), residents in Gyeongju were identified as the earthquake-exposed group, while inhabitants of Gimpo, Jeonju, and Southern Pohang served as control groups, unaffected by the earthquake. Gimpo, with a population size comparable to Gyeongju, is situated 300 km away. Southern Pohang, being the nearest administrative division to Gyeongju, also shares a similar population size. Jeonju, larger in population than Gyeongju, lies approximately 186 km distant. The general characteristics, including the population size, ambient temperature, gross regional domestic product per capita, number of vehicles, number of hospitals, and the numbers of medical doctors per 1,000 population, for Gyeongju and the control cities have been extracted from the Korean Statistical Office and the Korea Meteorological Administration. Details are summarized in Table S1 (refer to Additional file 1). If there is a link between experiencing earthquakes and the development of IHD, it was anticipated that Gyeongju residents would demonstrate a higher occurrence of IHD after the earthquake, even when considering the temporal changes in the control cities.

Map of the study region. Color-coded dots represent the extent of the Gyeongju earthquake exposure, calculated according to property damage, ranging from moment magnitude V (yellow) to VIII (red)
Data
South Korea operates a comprehensive single-payer health insurance system through the National Health Insurance Service (NHIS), offering healthcare coverage to the entire nation. For administrative purposes, hospital use information (including date, diagnostic code, details of treatment and prescription) and personal information (including birth year, sex, death, household health insurance premium, residential location) of the insured residents are archived in the National Health Insurance database [18].
The NHIS constructs a customized dataset based on researchers’ requests using data from the health insurance database. Prior epidemiological research utilized customized datasets to assess the impacts of air pollution, industrial operations, and natural calamities on public health [3, 19, 21, 22].
Due to the personal information protection policy, only a subset of entire population was allowed to be retrieved from the National Health Insurance database. For this study, 50% of individuals who resided in Gyeongju, Gimpo, Southern Pohang, and Jeonju in 2014 were randomly selected (n = 732,554). Sampling was conducted by the NHIS statistical service team based on sex and birth year. To avoid population migration-related problems [23], individuals who did not change their place of residence from 2014 to 2019 or from 2014 to death were selected (n = 540,858). The records of the individuals included in the study sample were screened for all IHD-related hospital visits using primary diagnostic code information of each hospital visits (International Classification of Disease 10th revision codes, I20.X to I25.X). From 2010 to 2019, 460,582 hospital visits for IHD were identified. The incidence was calculated based on the first hospital visit in which diagnostic codes were recorded as in previous studies [24]. The monthly number of patients newly diagnosed with IHD was calculated for various age brackets, spanning five-year ranges from 0 to 4 to 80–84 years and those aged 85 years and above. The monthly age-standardized incidence rate was calculated to determine the overall IHD incidence patterns during the study period and to compare the patterns across the evaluated cities with different populations and age structures [25, 26]. The number of the study population by each city is presented in Supplementary Table S2 (see Additional file 1). The regional ambient temperature data used in the sensitivity analysis was obtained from the Korea Meteorological Administration’s Automated Synoptic Observing System.
Statistical analysis
The following DID model was used:
In this model, \( {\mu }_{t, x} \)represents the number of IHD incidence patients in year-month t and age group x, \( R\) represents the study region (R = 1: Gyeongju city, R = 0: control city), and \( {T}_{t}\) represents the time (in months) since Sep 2014. \( {P}_{n}\) represents the period before and after the Gyeongju earthquake (\( {P}_{1} \)= Sep 2015-Aug 2016, \( {P}_{2} \)= Sep 2016-Aug 2017, \( {P}_{3} \)= Sep 2017-Aug 2018, \( {P}_{4} \)= Sep 2018-Aug 2019), M refers to months, A represents age categories, and\( { Pop}_{t, x }\) represents the population qualified for health insurance within the specific age group x and during the t year-month. A natural spline term for the time variable was utilized to account for long term temporal patterns in IHD incidence over time, as indicated by the variable \( ns ({T}_{t}, df=6)\). Month indicator variable (M) and age category variable (A) were included to adjust seasonality and age structure. The \( {{\upbeta }}_{7}\) to \( {{\upbeta }}_{10}\) values were used to calculate the risk of disease development in Gyeongju residents in each time period by setting the period from Sep 2014 to Aug 2015 as a reference. The estimates between Gyeongju and the control cities were meta-analyzed using a random-effects model in order to calculate the pooled estimates [27]. A similar DID model was used in a previous study that evaluated the mental health effects of an induced earthquake in Korea [19].
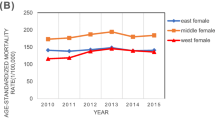
To confirm the parallel-trend assumption in the DID analysis, monthly age-standardized incidence rates in the analyzed cities were visually inspected (Fig. 2). In addition, the reference (Sep 2014-Aug 2015) and \( {P}_{1}\) (Sep 2015-Aug 2016) periods before the earthquake were compared with the expectation of null results. To show that the increase in disease development was confined to Gyeongju, comparisons were performed between the control cities.

Monthly age-standardized ischemic heart disease incidence rate (1,000,000 persons)
A stratification analysis was conducted based on gender, age categories (25–44, 45–64, and 65 and above), and income groups and potential effect modification was evaluated with the Cochrane Q test [28]. Patients aged < 24 years were excluded from the stratification analysis because only a small number developed IHD. Age categories (25–44, 45–64, and 65 and above) were selected based on previous cardiovascular epidemiological studies [29, 30]. Health insurance premiums (categorized from 1 to 20) vary according to household income in Korea. As in previous studies, income groups were defined by using the categorized health insurance premium levels (low: 0 to 10, high: 11–20) [21]. For the sensitivity analysis, monthly average temperature for each region was included in the difference-in-difference model to adjust for region specific climate differences. SAS (version 9.4) and R statistical software (version 4.2.1) were used in our analysis. The significance level for statistical analysis was established as p < 0.05.
Results
Ten years (2010–2019) of medical records from a randomly selected cohort of residents (n = 540,858) in Gyeongju and 3 control cities were evaluated. A total of 11,039 newly diagnosed IHD patients were identified between September 2014 and August 2019.
Table 1; Fig. 2 show the monthly IHD incidence in Gyeongju and in the control cities before (reference: Sep 2014-Aug 2015, period 1: Sep 2015-Aug 2016) and after the earthquake (period 2: Sep 2016-Aug 2017, period 3: Sep 2017-Aug 2018, period 4: Sep 2018-Aug 2019). A monthly average incidence of IHD in Gyeongju was 39.5 (per 1,000,000) for reference and 38.4 for period 1. However, this number increased to 58.5 in period 2, and 49.8 in period 3, following the earthquake. There was a clear increase in the age-standardized incidence rate (/1,000,000 persons) in Gyeongju city after the earthquake (period 2: 267.1 persons, period 3: 231.2 persons/1,000,000 persons), while no difference was observed in the control cities.
The relative risk [RR, 95% confidence interval (CI)] of developing IHD among Gyeongju residents increased by 1.58 times (1.43, 1.73) in period 2, 1.33 times (1.21, 1.46) in period 3, and 1.15 times (1.04, 1.27) in period 4, in comparison to both the control cities and the pre-earthquake reference period (Table 1). As expected, no increase was observed before the earthquake (period 1) [RR (95% CI): 0.97 (0.86, 1.11)]. Figure 2 also shows similar monthly disease incidence patterns across the cities before the earthquake.
A monthly average incidence of IHD in Gyeongju was 21.3 (per 1,000,000; reference) and 19.8 (period 1) in men and 18.2 (reference) and 18.7 (period 1) in women. However, this number increased to 29.2 and 29.3 after the earthquake in both men and women (period 2). The increase was greater in women [RR (95% CI): men, 1.38 (1.20, 1.60); women, 1.85 (1.60, 2.13), p-value for heterogeneity: < 0.01] (Table S3, see Additional file 1).
Table 2 presents the results of the stratification analysis by age and income groups. A monthly average incidence of IHD in Gyeongju for reference period was 1.9, 15.5, and 21.7 (per 1,000,000) in age 25–44, age 45–64, and age 65- group, respectively. However, this number increased to 2.8 (age 25–44), 24.6 (age 45–64), and 30.8 (age 65-) after the earthquake (period 2). The DID estimates for IHD development were greater in young adults (25–44 years) than in other age groups (45–64 and ≥ 65 years) [RR (95% CI) for period 2: age 25–44, 2.36 (1.50, 3.73); age 45–64, 1.65 (1.42, 1.91); age ≥ 65, 1.48 (1.25, 1.74): p-value for heterogeneity: 0.05] (Table S4, see Additional file 1).
A monthly average incidence of IHD in Gyeongju was 13.9 (per 1,000,000; reference) and 14.2 (period 1) in low income group and 25.6 (reference) and 24.3 (period 1) in high income group. However, this number increased to 23.8 and 34.7 in both low- and high-income groups after the earthquake (period 2) (Table 2). Although the risk of IHD development was greater in the low-income group than in the high-income group [RR (95% CI) for period 2: low-income group, 1.77 (1.52, 2.07); high-income group: 1.47 (1.31, 1.65)], the difference was marginally significant (p-value for heterogeneity: 0.06) (Table S5, see Additional file 1). The DID estimates between the control cities are shown in Supplementary Table S6 (see Additional file 1). No increase was observed across the control cities during the study period. The sensitivity analysis additionally adjusting for monthly average ambient temperature showed similar results to the main analysis (Supplementary Table S7, see Additional file 1).
Discussion
The residents affected by the earthquake showed an increased risk of IHD development. The risk of IHD development in Gyeongju residents increased by 50% during the year following the earthquake compared to residents in cities unaffected by the earthquake. This increase in risk was particularly noticeable among women, adults aged 25–44, and individuals with lower incomes. Based on the study findings, close monitoring of long-term cardiovascular health is recommended for earthquake-exposed residents.
Several research studies have documented a connection between the earthquake and cardiovascular health [5,6,7]. For instance, an increase in cardiac-related deaths and IHD admissions was reported on the day or within a week after the 1994 Northridge earthquake (magnitude: 6.7) in the US [10,11,12]. A rise in hospital admissions due to acute myocardial infarction and cardiomyopathy was observed five weeks after a sequence of major earthquakes took place in Christchurch, New Zealand, in 2010 (magnitude: 7.1) and 2011 (magnitude: 6.3) [16]. Research utilizing medical records demonstrated an increased risk of cardiovascular events occurring within a span of three weeks following the Great East Japan Earthquake in 2011, which had a magnitude of 9.0 [8, 9].
The long-term consequences of earthquakes on the cardiovascular health of residents have received limited attention in earlier studies [6]. An increase mortality due to cardiovascular disease and in the development of other morbidities (hypertension, heart disease, diabetes, and arthritis) were reported in a cohort study involving residents exposed to the 1988 Armenia earthquake, which had a magnitude of 6.8 [15]. Comparing the 5 years preceding and the 3 years following the Niigata-Chuetsu earthquake in Japan (magnitude: 6.8) in 2004, a 14% rise in acute myocardial infarction-related mortality was noted after the earthquake [13].
Within 1 year after the Great East Japan earthquake, an increase in out-of-hospital cardiac arrest cases was observed among residents who suffered significant earthquake damage [17]. A rise in fatal myocardial infarction occurrences was identified in the area impacted by the tsunami triggered by the Great East Japan earthquake, and this increase persisted for 3 years [14]. However, when studying a group of heart failure patients, stable mortality patterns were observed throughout the 3-year monitoring period after the Great East Japan earthquake, even though there was a notable surge shortly after the earthquake [31].
Various epidemiological studies report that earthquakes affect not only cardiovascular diseases but also infectious and respiratory diseases and psychological disorders [6, 32,33,34]. A systematic literature review of 160 documents evaluating the health impact of the Great East Japan Earthquake in 2011 found that medical utilization increased for patients with pre-existing respiratory and mental disorders after the earthquake [32]. Additionally, there was a rise in the incidence of new mental disorders, including post-traumatic stress disorder, suicidal tendencies, and depression, among residents in earthquake-affected areas [32].
Considering the anticipated increase in earthquake intensity and frequency due to the impact of climate change in regions such as Korea [35], it is crucial to quantitatively assess not only the direct injuries and fatalities resulting from earthquakes but also the diverse health impact on community residents using the well-designed epidemiological studies. However, most of previous studies use cross-sectional and questionnaire based evaluation for a small number of participants without using temporal or geographical location based compaisons [6, 32,33,34]. In addition, major earthquakes with high number of death tolls were mainly considered.
This study focusing on 2016 Gyeongju earthquake and series of aftershocks used both temporal and geographical control groups based on the health insurance database, and the findings suggest an association between earthquake exposure and an increase in IHD incidence. Disease incidence after an earthquake can be determined without bias only if a community-based cohort already existed at the earthquake site [31, 36, 37]. Because an earthquake occurs randomly, the possibility of a such pre-existing cohort is very low. Therefore, a previous study recruited subjects after an earthquake and investigated previous histories and new disease onset using a structured questionnaire [15]. In contrast, this research managed to determine the connection between earthquake exposure and disease occurrence post-earthquake by examining the medical records of residents through hospital visit data. Utilizing hospital-based or health insurance data, which often include comprehensive disease outcomes, enables the assessment of the diverse impact of earthquakes on different disease [3, 19].
Physical and emotional stress caused by earthquake exposure affects the sympathetic nervous and endocrine systems, which may precipitate cardiovascular events [5, 6]. The experience of life-threatening events or the loss of family or close friends during such an event may be the main drivers of emotional stress [4]. Reports indicate that increased psychological stress levels or biomarkers, such as glycated hemoglobin, have lasted for a year after earthquake exposure [5, 6]. Studies in Korea showed an increase in anxiety-related disorders and mood disorders within the days and weeks after the earthquake [3, 19]. Therefore, the sudden earthquake experience and yearlong aftershocks may have affected the cardiovascular health of Gyeongju residents.
Another plausible mechanism explaining the increased risk of cardiovascular disease after a disaster is an interruption in medical services [9]. Loss of medications or destruction of medical facilities after a disaster may cause such interruptions. However, the estimated property damage was relatively small after the Gyeongju earthquake compared to the damage caused by major earthquakes in previous studies [3]. In addition, as far as author is aware, no disruption of medical services was reported in Gyeongju after the earthquake. Therefore, the effects of healthcare disruption on the findings of this study may be minimal.
Occupational studies have shown an association between whole-body vibration and cardiovascular disease [38]. Vibration exposure is associated with vasoconstriction, endothelial dysfunction, and increased heart rate and blood pressure [38]. An experimental study showed that exposure to simulated train vibration increased heart rate [39]. Although over 96% of the aftershocks following the Gyeongju earthquake were below a magnitude of 3 (most people inside buildings were not able to feel the vibration) [40], chronic long-term minor exposure to sudden vibration may have affected the residents’ cardiovascular health. However, additional laboratory and epidemiological evidence is required to confirm this hypothesis.
Studies focusing on a vulnerable population against the effects of earthquake on IHD incidence are still limited. In this study, subjects from the low household income group and women exhibited an increased risk of IHD development after the earthquake. Although the biological mechanisms are unclear, women and individuals from low-income groups exhibit a heightened risk of adverse health effects after disasters [3, 41, 42]. A prospective cohort study conducted in Japan revealed an elevated risk of cardiovascular deaths in women who reported high perceived stress compared to those in the low-stress, while the association was found to be less pronounced among men [43]. Subjects with a low socioeconomic status may have a vulnerable health status or infrastructure, which can make them susceptible to external stresses [44, 45]. Similar findings were noted in previous studies investigating the health effects of earthquakes. The standardized incident ratio of fatal myocardial infarction comparing the incidence before (2009–2010) and after 2011 Great East Japan earthquake showed higher rates in women after the earthquake (2011: 1.72; 2012; 2.59) than men (2011: 1.85; 2012; 1.58) [14]. By comparing acute myocardial infarction mortality rate 5 years before and 3 years after the Niigata-Chuetsu earthquake, the increase was greater in women (14.9% increase after the earthquake) compared to men (13.4% increase after the earthquake) [13]. Risk of developing heart disease after the 1988 Armenia earthquake was 1.5 times higher in low education group (education years ≤ 10 years) compared to high education group in gender matched case-control analysis [15]. It is important to identify vulnerable groups to natural disasters in disaster research studies. Based on such studies, it will be possible to determine priority targets for the healthcare management of disaster victims [46].
The results of age stratification analysis showed a higher estimate for the age 25–44 group compared to the age 45–64 and age ≥ 65 groups during the year following the Gyeongju earthquake. However, the results from 25 to 44 age group should be carefully interpreted due to the low monthly incidence rate of IHD (ranging from 1.9 to 5.0 persons per month) in both the Gyeongju and control regions. In addition, previous earthquake studies comparing the effects of earthquake across different age categories did not show significant differences [14, 15].
This study has several limitations. First, the validity of the DID analysis can be threatened by external factors specifically affecting Gyeongju. The DID analysis may not separate the effects of the earthquake and other external factors changing in Gyeongju at the same time as the earthquake. Although such changes were not noticed, the possibility cannot be ruled out. Second, individual factors other than sex, age, and household income were not considered in this study because of data availability. The availability of information regarding routine health examinations or personal habits could have enabled individual-level matching, which may have increased the comparability between the case (individuals from Gyeongju) and control (individuals from the control cities) groups compared to the geographical and stratification-based analyses used in this study. Third, specific subtypes of IHD or assessments for other cardiovascular diseases were not feasible due to data constraints. In addition, due to the personal information protection policy, only 50% of entire population was evaluated in this study. Further analysis including detailed assessments of disease subtypes and the entire population will help to shape overall disease burden of 2016 Gyeongju earthquake on residents.
Conclusions
Analyzing the nationwide health insurance data showed a marked increase in the incidence of IHD in earthquake-exposed residents. The DID analysis showed a 58% increase in the risk of IHD development, and this increased risk was found to last for over 2 years. Although the damage to life and property was limited after the Gyeongju earthquake, this study revealed an association between long-lasting seismic activities and the development of IHD.
Data availability
The data that support the findings of this study are available from the National Health Insurance Service, Korea. Restrictions apply to the availability of these data, which were used under license for this study. Data are available from the authors (contact C.H.) with the permission of the National Health Insurance Service, Korea.
References
Korea Meteorological Administration.: 9.12 earthquake response report (in Korean), (https://www.weather.go.kr/w/download/earthquake_912.pdf, assessed 20 December 2022). 2017.
Lee T, Koo W, Baek M. A study on the consciousness survey of residents in Gyeong-Ju to improve earthquake disaster prevention measures after the occurrence of 9.12 earthquake. J Korean Soc Hazard Mitigation. 2018;18(4):261–70.
Han C. Seismic activity and development of mood disorders: findings from the 2016 Kyungju earthquake. Sci Total Environ. 2023;867:161328.
Goldmann E, Galea S. Mental health consequences of disasters. Annu Rev Public Health. 2014;35:169–83.
Kloner RA. Lessons learned about stress and the heart after major earthquakes. Am Heart J. 2019;215:20–6.
Ripoll Gallardo A, Pacelli B, Alesina M, Serrone D, Iacutone G, Faggiano F, Della Corte F, Allara E. Medium- and long-term health effects of earthquakes in high-income countries: a systematic review and meta-analysis. Int J Epidemiol. 2018;47(4):1317–32.
Bazoukis G, Tse G, Naka KK, Kalfakakou V, Vlachos K, Saplaouras A, Letsas KP, Korantzopoulos P, Thomopoulos C, Michelongona P. Impact of major earthquakes on the incidence of acute coronary syndromes–a systematic review of the literature. Hellenic J Cardiol. 2018;59(5):262–7.
Nozaki E, Nakamura A, Abe A, Kagaya Y, Kohzu K, Sato K, Nakajima S, Fukui S, Endo H, Takahashi T. Occurrence of cardiovascular events after the 2011 Great East Japan Earthquake and tsunami disaster. Int Heart J. 2013;54(5):247–53.
Nakamura A, Nozaki E, Fukui S, Endo H, Takahashi T, Tamaki K. Increased risk of acute myocardial infarction after the Great East Japan Earthquake. Heart Vessels. 2014;29(2):206–12.
Leor J, Kloner RA. The Northridge earthquake as a trigger for acute myocardial infarction. Am J Cardiol. 1996;77(14):1230–2.
Kloner RA, Leor J, Poole WK, Perritt R. Population-based analysis of the effect of the Northridge Earthquake on cardiac death in Los Angeles County, California. J Am Coll Cardiol. 1997;30(5):1174–80.
Leor J, Poole WK, Kloner RA. Sudden cardiac death triggered by an earthquake. N Engl J Med. 1996;334(7):413–9.
Nakagawa I, Nakamura K, Oyama M, Yamazaki O, Ishigami K, Tsuchiya Y, Yamamoto M. Long-term effects of the Niigata-Chuetsu earthquake in Japan on acute myocardial infarction mortality: an analysis of death certificate data. Heart. 2009;95(24):2009–13.
Nakamura M, Tanaka K, Tanaka F, Matsuura Y, Komi R, Niiyama M, Kawakami M, Koeda Y, Sakai T, Onoda T, et al. Long-Term effects of the 2011 Japan Earthquake and Tsunami on incidence of fatal and nonfatal myocardial infarction. Am J Cardiol. 2017;120(3):352–8.
Armenian HK, Melkonian AK, Hovanesian AP. Long term mortality and morbidity related to degree of damage following the 1988 earthquake in Armenia. Am J Epidemiol. 1998;148(11):1077–84.
Chan C, Elliott J, Troughton R, Frampton C, Smyth D, Crozier I, Bridgman P. Acute myocardial infarction and stress cardiomyopathy following the Christchurch earthquakes. PLoS ONE. 2013;8(7):e68504.
Sado J, Kiyohara K, Iwami T, Kitamura Y, Ando E, Ohira T, Sobue T, Kitamura T. Three-year follow-up after the Great East Japan Earthquake in the incidence of out-of-hospital cardiac arrest with Cardiac Origin. Circ J. 2018;82(3):919–22.
Seong SC, Kim Y-Y, Khang Y-H, Heon Park J, Kang H-J, Lee H, Do C-H, Song J-S, Hyon Bang J, Ha S. Data resource profile: the national health information database of the National Health Insurance Service in South Korea. Int J Epidemiol. 2017;46(3):799–800.
Han C. Induced Seismicity and Acute Development of anxiety and stress-related Mental disorders: findings from the 2017 Pohang Earthquake. Environ Health Perspect. 2022;130(6):067701.
Wooldridge JM. Introductory econometrics: a modern approach. Cengage learning; 2015.
Han C, Oh J, Lee D-W, Kim S, Bae H-J, Jang Y, Hong Y-C, Lim Y-H. Particulate air pollution and survival after stroke in older adults: a retrospective cohort study in Korea. Environ Res. 2021;197:111139.
Han C, Hong Y-C. Adverse health effects of ferronickel manufacturing factory on local residents: an interrupted time series analysis. Environ Int. 2018;114:288–96.
Galea S, Maxwell AR, Norris F. Sampling and design challenges in studying the mental health consequences of disasters. Int J Methods Psychiatr Res. 2008;17(S2):21–S28.
Lee D-W, Han C-w, Hong Y-C, Oh J-M, Bae H-J, Kim S, Lim Y-H. Long-term exposure to fine particulate matter and incident asthma among elderly adults. Chemosphere. 2021;272:129619.
Boyle P, Parkin D. Statistical methods for registries. Cancer Registration: Principles and Methods. 1991;95:126–58.
Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJ, Lozano R, Inoue M. Age standardization of rates: a new WHO standard. Geneva: World Health Organization. 2001;9(10):1–14.
Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Introduction to meta-analysis. John Wiley & Sons; 2021.
Kaufman JS, MacLehose RF. Which of these things is not like the others? Cancer 2013, 119(24):4216–22.
Antikainen R, Jousilahti P, Tuomilehto J. Systolic blood pressure, isolated systolic hypertension and risk of coronary heart disease, strokes, cardiovascular disease and all-cause mortality in the middle-aged population. J Hypertens. 1998;16(5):577–83.
Chen J, Wu K, Lin Y, Huang M, Xie S. Association of triglyceride glucose index with all-cause and cardiovascular mortality in the general population. Cardiovasc Diabetol. 2023;22(1):320.
Miyata S, Sakata Y, Miura M, Yamauchi T, Onose T, Tsuji K, Abe R, Oikawa T, Kasahara S, Sato M. Long-term prognostic impact of the Great East Japan Earthquake in patients with cardiovascular disease–report from the CHART-2 study. J Cardiol. 2017;70(3):286–96.
Murakami A, Sasaki H, Pascapurnama DN, Egawa S. Noncommunicable diseases after the Great East Japan Earthquake: systematic review, 2011–2016. Disaster Med Pub Health Prep. 2018;12(3):396–407.
Dai W, Chen L, Lai Z, Li Y, Wang J, Liu A. The incidence of post-traumatic stress disorder among survivors after earthquakes: a systematic review and meta-analysis. BMC Psychiatry. 2016;16(1):1–11.
Najafi S, Akahavan Rezayat A, Beyzaei SF, Shahriari Z, Taheri tabar M, Ghasemi Nour M, Mosaed R, Khadem-Rezaiyan M, Hamidi Farahani R. Incidence of infectious diseases after earthquakes: a systematic review and meta-analysis. Public Health. 2022;202:131–8.
Kim M-J, Lee H-K. Long-term patterns of earthquakes influenced by climate change: insights from earthquake recurrence and stress field changes across the Korean Peninsula during interglacial periods. Q Sci Rev. 2023;321:108369.
Fergusson DM, Horwood LJ, Boden JM, Mulder RT. Impact of a major disaster on the mental health of a well-studied cohort. JAMA Psychiatry. 2014;71(9):1025–31.
Kino S, Aida J, Kondo K, Kawachi I. Long-term trends in Mental Health disorders after the 2011 Great East Japan Earthquake and Tsunami. JAMA Netw open. 2020;3(8):e2013437–7.
Liu T, Huang H, Zhang W, Hu G. What are some physical factors in Occupational Environment Associated with Coronary Heart Disease? J Occup Environ Med. 2022;64(10):e656–60.
Croy I, Smith MG, Waye KP. Effects of train noise and vibration on human heart rate during sleep: an experimental study. BMJ Open 2013, 3(5).
Ministry of the interior and safety.: Statistical yearbook of natural disaster (in Korean), (https://www.mois.go.kr/frt/bbs/type001/commonSelectBoardArticle.do?bbsId=BBSMSTR_000000000014&nttId=59551, assessed 17 March 2022). 2016.
Gan CCR, Oktari RS, Nguyen HX, Yuan L, Yu X, Kc A, Hanh TTT, Phung DT, Dwirahmadi F, Liu T, et al. A scoping review of climate-related disasters in China, Indonesia and Vietnam: disasters, health impacts, vulnerable populations and adaptation measures. Int J Disaster Risk Reduct. 2021;66:102608.
Marshall J, Wiltshire J, Delva J, Bello T, Masys AJ. Natural and manmade disasters: vulnerable populations. Global health security. edn.: Springer; 2020. pp. 143–61.
Iso H, Date C, Yamamoto A, Toyoshima H, Tanabe N, Kikuchi S, Kondo T, Watanabe Y, Wada Y, Ishibashi T. Perceived mental stress and mortality from cardiovascular disease among Japanese men and women: the Japan Collaborative Cohort Study for evaluation of Cancer Risk Sponsored by Monbusho (JACC Study). Circulation. 2002;106(10):1229–36.
Chou Y-J, Huang N, Lee C-H, Tsai S-L, Chen L-S, Chang H-J. Who is at risk of death in an earthquake? Am J Epidemiol. 2004;160(7):688–95.
Newnham EA. 2.5 identifying and engaging high-risk groups in disaster research. WHO Guidance on Research Methods for Health Emergency and Disaster risk Management 2021:88.
Benevolenza MA, DeRigne L. The impact of climate change and natural disasters on vulnerable populations: a systematic review of literature. J Hum Behav Social Environ. 2019;29(2):266–81.
Acknowledgements
This study used the customized database of the National Health Insurance Service for policy and academic research. The aim and conclusion of this study are irrelevant to the National Health Insurance Service, Republic of Korea. The research number of this study is NHIS-2021-1-275.
Funding
This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT) (RS-2023-00210534) and by Korea Environment Industry &Technology Institute (KEITI) through Digital Infrastructure Building Project for Monitoring Surveying and Evaluating the Environmental Health, funded by Korea Ministry of Environment (MOE) (RS-2021-KE001615). The funding sources had no role in the study design, collection, analysis, interpretation of data, writing of the report, or the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
C.H. is a sole author. C.H. conceived and designed the study. C.H. performed the statistical analysis and C.H interpreted the results and wrote the initial manuscript. C.H. reviewed the manuscript. All author provided input to the preparation of the manuscript. All author read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study used the de-identified secondary data provided by the Statistics Korea and the National Health Insurance Service with no direct involvement of the participants. The data used in this study were anonymized before provision to the authors. Therefore, the patient informed consent procedure is waived by the Institutional Review Board of the Chungnam National University (IRB no. 202106-SB-084-01). All methods were carried out following relevant guidelines and regulations.
Statement on guidelines
This study complies with relevant guidelines and regulations. All the data were provided by the National Health Insurance Service (NHIS). This study used the de-identified data provided by the Statistics Korea and the NHIS.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Han, C. Exposure to earthquakes and development of ischemic heart disease. BMC Public Health 24, 446 (2024). https://doi.org/10.1186/s12889-024-17835-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17835-0