
Abstract
Background
Computer vision syndrome has become a significant public health problem, especially in developing countries. Therefore, this study aims to identify the prevalence of computer vision syndrome during the COVID-19 pandemic.
Methods
A systematic review and meta-analysis of the literature was conducted using the databases PubMed, Scopus, Web of Science, and Embase up to February 22, 2023, using the search terms "Computer Vision Syndrome" and "COVID-19". Three authors independently performed study selection, quality assessment, and data extraction, and the Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument was used to evaluate study quality. Heterogeneity was assessed using the statistical test I2, and the R version 4.2.3 program was used for statistical analysis.
Results
A total of 192 studies were retrieved, of which 18 were included in the final meta-analysis. The total sample included 10,337 participants from 12 countries. The combined prevalence of computer vision syndrome was 74% (95% CI: 66, 81). Subgroup analysis based on country revealed a higher prevalence of computer vision syndrome in Pakistan (99%, 95% CI: 97, 100) and a lower prevalence in Turkey (48%, 95% CI: 44, 52). In addition, subgroup analysis based on study subjects showed a prevalence of 82% (95% CI: 74, 89) for computer vision syndrome in non-students and 70% (95% CI: 60, 80) among students.
Conclusion
According to the study, 74% of the participants experienced computer vision syndrome during the COVID-19 pandemic. Given this finding, it is essential to implement preventive and therapeutic measures to reduce the risk of developing computer vision syndrome and improve the quality of life of those affected.
Trial registration
The protocol for this systematic review and meta-analysis was registered in the international registry of systematic reviews, the International Prospective Register of Systematic Reviews (PROSPERO), with registration number CRD42022345965.
Similar content being viewed by others


Introduction
Computer Vision Syndrome (CVS), or digital eye strain, is a set of visual and ocular symptoms that affect people who use electronic devices (ED) for extended periods [1]. These devices include computers, laptops, tablets, e-readers, and smartphones [2]. Symptoms related to CVS can be classified into three categories [3,4,5]: visual symptoms (blurry vision, visual fatigue or discomfort, and double vision), ocular symptoms (dry eyes, redness, eye fatigue, and irritation), and extraocular symptoms (headache and pain in the shoulders, neck, and back).
Recent studies have shown that there are two categories of risk factors associated with CVS [3]: those that are of personal origin (such as poor posture while sitting, the incorrect distance between the eyes and the screen, the wrong viewing angle, the presence of medical conditions, and prolonged computer exposure) [6] and those that are computer and environmental factors (which include inadequate workstations, insufficient lighting, poor contrast and resolution, the increased presence of screen glare, excessive brightness, and light imbalance between the screen and the surrounding work environment) [7, 8].
For the past two decades, CVS has become a highly relevant health problem that affects the entire population [1]. A systematic review and meta-analysis study found that the pooled prevalence of CVS is 66% [3]. In addition, the COVID-19 pandemic and the subsequent lockdowns have led to a significant increase in the use of ED worldwide. That massive increase in the use of ED has created a conducive environment for the development of CVS, which increases the risk of experiencing its associated visual, ocular, and extraocular symptoms [9].
During this global crisis, many people have experienced a significant increase in time spent on technology-related activities, such as working from home, participating in virtual meetings, and engaging in online entertainment [10, 11]. This change in screen use habits has led to an increased risk of developing CVS [12].
The rapid evolution of technology has made ED an essential part of our daily lives [13]. However, several studies have shown that prolonged use of these devices can negatively affect people's eye health, as evidenced during the COVID-19 pandemic [14, 15]. Therefore, this systematic review and meta-analysis aimed to determine the prevalence of computer vision syndrome during the COVID-19 pandemic. This will allow the development of strategies and preventive measures to protect and improve the eye health of the population.
Materials and methods
Study design and protocol registration
This systematic review and meta-analysis was registered on the International Prospective Register of Systematic Reviews (PROSPERO) under the registration code CRD42022345965. Available at: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=345965.
Eligibility criteria
The prevalence of CVS was identified using published peer-reviewed articles with observational study methods (nonrandomized cohort and intervention studies). The articles covered what was published through February 22, 2023, and had no language restrictions. Editorials, letters to the editor, randomized clinical trials, narrative reviews, systematic review papers, and meeting proceedings were not reviewed.
Data sources and search strategy
The databases PubMed, Scopus, Web of Science, and Embase were searched extensively. The search terms used were "COVID-19" and "Computer Vision Syndrome". The search strategy is available at: https://doi.org/https://doi.org/10.6084/m9.figshare.22141715.v1. The searches were completed on February 22, 2023, and the results were independently evaluated by three different investigators (J.J.B., DALF, and R.S.).
Study selection
A database was created from the results of electronic searches using Endnote reference management software. Duplicate articles, irrelevant titles, and abstracts were removed. Then, three investigators (DALF, A.S., and MJVG) independently evaluated the article titles and abstracts to select those that appeared to meet the inclusion criteria. Finally, three other investigators (J.J.B., R.S., and AJRM) carefully reviewed the full-text reports and assessed whether they met the inclusion criteria before deciding whether to include them. In any disagreement, a fourth investigator (AJRM) helped resolve the differences and reach a solution. A PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram was used to present the study selection procedures.
Data extraction
Three investigators (DALF, MJVG, and J.J.B.) worked independently to extract data from the selected articles and record them in an Excel spreadsheet. Essential details of the selected studies were collected, such as author, date of publication, study design, country, sample size, response rate, prevalence of computer vision syndrome, study subjects, age, and sex. If disagreements arose over the inclusion of studies, a fourth investigator (EAM) resolved them and verified that the list of publications and extracted data did not contain duplicate articles or irrelevant information.
Quality assessment
"The Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI-MAStARI)" [16] was used to assess the quality of articles before their inclusion in the final meta-analysis. The evaluation was based on various aspects, such as the research context, outcome and explanatory variables, explicit inclusion criteria, measurement standards, subject description, and precise statistical analysis. DALF, AJRM, and JJB independently evaluated the quality of the studies. It was classified as "high", "moderate", or "low" based on their score, with more than 7 points for high quality, 4 to 6 points for moderate quality, and less than 4 points for low quality. Any discrepancies among the researchers during the quality evaluation were resolved through discussion (Table 1).
Data analysis
The extracted Excel data was imported into the R program version 4.2.3 for analysis. The studies that were included were presented narratively using tables and graphs. A meta-analysis was conducted using the random-effects model to calculate the overall effect size, and the results were displayed using a forest plot. The I2 index was used to analyze heterogeneity, where I2 = 30% indicated low heterogeneity, I2 = 30–60% represented moderate heterogeneity, and I2 > 60% showed high heterogeneity. The R meta-package was utilized for conducting the meta-analyses. A visual evaluation was performed using a funnel plot and Egger's test for asymmetry to assess publication bias, but only if the number of included papers exceeded 10.
Results
Study selection
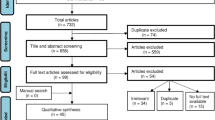
The search strategy allowed for the retrieval of 192 articles, whose selection process can be visualized in the PRISMA flowchart (Fig. 1). After removing duplicates (n = 100), 92 articles were examined by the researchers. Subsequently, after filtering the titles and abstracts, 64 articles were selected for full-text reading, and 18 were considered eligible for inclusion in this systematic review and meta-analysis [13, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33].

PRISMA flowchart describing the selection of studies for the systematic review and meta-analysis of the prevalence of computer vision syndrome during the COVID-19 pandemic
Characteristics of the included studies
Eighteen cross-sectional studies examining the prevalence of CVS during the COVID-19 pandemic, published between 2021 and 2022, were included [13, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33] (Table 2). The total sample included 10,337 participants from 12 countries (n = 18) [13, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]: India (n = 3) [17, 24, 31], Saudi Arabia (n = 3) [18, 23, 32], Ethiopia (n = 1) [19], Pakistan (n = 1) [20], China (n = 2) [21, 29], Egypt (n = 1) [22], Paraguay (n = 1) [25], Peru (n = 1) [26], South Africa (n = 1) [27], Bangladesh (n = 1) [28], Thailand (n = 2) [13, 30], and Turkey (n = 1) [33]. The sample size varied from 74 in a study of Chinese medical students at the University of Sichuan [21] to 2476 in a survey of high school students in Thailand [13]. Of the participants, 39% were men, and 61% were women. The student population was the primary participant in most included studies [13, 17, 20, 21, 23, 25,26,27,28,29,30, 32, 33]. This systematic review and meta-analysis provide a broad overview of the prevalence of CVS in various countries during the COVID-19 pandemic [13, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33] (Table 2).
Quality of the included studies and publication bias
The included cross-sectional studies were characterized by their high level of quality, which was assessed using the JBI-MAStARI tool (Table 1). In the analyses aimed at assessing the prevalence of CVS during the COVID-19 pandemic, it was observed that when applying Egger's test to assess publication bias, a value of p = 0.7046 (t = 0.39, df = 16) was obtained. This result suggests that the null hypothesis of symmetry is accepted, indicating that there is no evidence of publication bias in the studies examined (Fig. 2).

Funnel plot and Egger's test illustrate the publication bias of the included studies
Pooled prevalence of computer vision syndrome
The pooled prevalence of CVS was 74% (95% CI: 66, 81) [13, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. The study with the lowest proportion was conducted in Saudi Arabia, with a prevalence of 35% (95% CI: 31, 40) [23], while the highest was conducted in Pakistan, with a prevalence of 99% (95% CI: 97, 100) [20]. The I2 test showed that there was heterogeneity among the included studies (I2 = 99%, p-value < 0.01) (Fig. 3) [13, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33].

Forest plot showing the pooled prevalence of computer vision syndrome during the COVID-19 pandemic
Subgroup analysis by country
Subgroup analysis was performed based on country, and the prevalence of CVS was highest in Pakistan (99%, 95% CI: 97, 100) [20] and lowest in Turkey (48%, 95% CI: 44, 52) [33]. The studies that showed significant heterogeneity were studies in India (I2 = 99%, p-value < 0.01), Saudi Arabia (I2 = 99%, p-value < 0.01), China (I2 = 94%, p-value < 0.01), and Thailand (I2 = 96%, p-value < 0.01) (Fig. 4).

Subgroup analysis by country on computer vision syndrome during the COVID-19 pandemic
Subgroup analysis by study subjects
A subgroup analysis was performed according to the study subjects, which revealed a prevalence of 82% (95% CI: 74, 89) for computer vision syndrome in non-students [18, 19, 22, 24, 31] and 70% (95% CI: 60, 80) among students [13, 17, 20, 21, 23, 25,26,27,28,29,30, 32, 33]. However, heterogeneity was observed among the studies included in both groups for both non-student and student subjects (I2 = 95%, p-value < 0.01; I2 = 99%, p-value < 0.01) (Fig. 5).

Subgroup analysis by study subjects on computer vision syndrome during the COVID-19 pandemic
Discussion
Since the onset of the COVID-19 pandemic, numerous countries around the world have implemented restrictions on physical activity and mobility as part of their social isolation and quarantine measures. These measures have had a significant impact on daily life, transforming the reality in which interactions have become predominantly virtual, whether for work, education, shopping, or other activities [34]. Several studies have shown a reduction in physical activity and an increase in sedentary time during the period of confinement due to the COVID-19 pandemic [35,36,37,38].
Therefore, the present study aimed to determine the prevalence of CVS during the COVID-19 pandemic, considering the increase in the use of electronic devices and the change in lifestyle towards greater virtualization in areas such as work, education, communications, and various daily activities [39]. Our meta-analysis reveals that during the COVID-19 pandemic, the overall prevalence of CVS increased by 74%, significantly exceeding the overall prevalence estimated in a recent systematic review by Anbesu EW et al. of 66% [3]. However, these results are consistent with the high prevalence rate of CVS in Ethiopia, which reaches 73.21%, as reported in a systematic review conducted by Adane et al. [3, 40]. That difference in prevalence between our study and the other one performed by Anbesu et al. is consistent with the shift in lifestyle during the period of COVID-19 to be more virtual and with the increase in the usage of electronic devices for multiple needs [39, 41]. In addition, several studies have been conducted to assess the impact of digital device usage during the COVID-19 pandemic on eye health, such as the study conducted by Bahkir et al., which found an increase in screen time, and 95% of the participants experienced at least one symptom of digital device use, such as dry eye, eye pain, eye redness, headache, double vision, and others [42]. Furthermore, another study conducted by Alabdulkader et al. reported that the incidence of digital eye strain was 78%, which is positively correlated with duration and the number of devices that are used [18], aside from another study conducted by Usgaonkar et al., which found that 89% of the participants were spending most of the time on social media using electronic devices. Hence, they experienced symptoms such as dry eyes, headaches, and back pain [14].
These results suggest that CVS significantly affected a large portion of the population during this period of health crisis. This underscores the importance of understanding and addressing the potential negative effects of prolonged exposure to electronic device screens.
The sub-group analysis based on the country revealed different prevalence estimates based on the number of studies available per country and justifying the inclusion criteria. The prevalence of CVS in India was estimated at 78%; similar results indicated a prevalence of digital eyestrain in the pre-isolation period of 64.3% [43]. That indicates the impact of increased digital device usage during the lockdown period. Our subgroup analysis revealed a CVS prevalence in Saudi Arabia of 72% based on the three included studies. However, this estimate differs from one setting to another. It varies based on the target population, as CVS prevalence was estimated at 43.5% in another Al Subaie et al. study among the Al-Ahsa population. Besides, another study conducted among radiologists revealed an overall prevalence of 65.4% [44, 45]. Our sub-group analysis revealed that the highest prevalence of CVS was in Pakistan (99%) based on only one included study, and the lowest prevalence was in Turkey (48%) based on only one study. This significant difference between them is based on the difference in the population's culture, behavior, and habits [46, 47].
It was estimated that the prevalence of CVS among students was 70%, which is consistent with their increased usage of computers and learning tools during the COVID-19 lockdown as most educational institutions and universities transformed their learning to be more virtual during the pandemic [48,49,50].
Our results revealed the variation in the CVS prevalence from one country to another, as shown in the sub-group analysis, and besides other studies conducted, such as the study conducted by Ranasinghe et al. among Sri Lankan computer workers, which reported a CVS prevalence of 67.4%, a survey conducted among the instructors in Ethiopia (70.4%), and a study conducted among undergraduate students in Pakistan (90.5%) [19, 51, 52]. The difference in the prevalence estimates may be attributed to the differences in the study setting, study period, socioeconomic characteristics, awareness of the target population about the preventive measures of using computers and digital devices, and the tool used in the estimation of the prevalence, which mainly depends on subjective questions and differs from one study to another.
Subgroup analysis revealed that the prevalence of CVS was higher in the non-student group (82%), compared to the student group (70%). These results can be attributed to the face-to-face restrictions that the COVID-19 pandemic imposed on educational and work activities, generating a massive transition to virtual environments. This shift resulted in a significant increase in time spent using electronic devices, such as computers, tablets, and cell phones. The non-student population, who were employed in jobs that did not require regular use of electronic devices or who lacked access to formal educational resources, possibly experienced greater exposure to digital screens without the same guidance and eye protection measures. This lack of guidance could have contributed to the higher prevalence of CVS in this group. In contrast, the student population may have demonstrated greater awareness of and access to eye protection measures, such as regular breaks, ergonomic adjustments, and the use of blue light filters. This is due to the guidance provided by educational institutions and the increased attention paid to eye health in the educational environment [53, 54].
The increased prevalence of CVS indicates poor education about this syndrome and the proper ways of using computers and digital devices. Therefore, educational programs should be designed for the general population to increase their awareness of CVS symptoms, the risk factors of this syndrome, the different causes of it, and safety measures to prevent it [55]. We should also promote research to identify the prevalence of CVS in other countries lacking data to have a more precise estimate of the prevalence of this syndrome globally.
This is the first meta-analysis conducted to describe the prevalence of CVS in the context of the COVID-19 pandemic. The results obtained in this study will provide a solid basis on which policymakers can design new policies and follow-up programs to address this syndrome. In addition, this analysis contributed significantly to the identification of gaps in research on the prevalence of CVS, which, in turn, will help guide future measures aimed at preventing its occurrence. Importantly, this study focused on the negative impact on ocular health due to the COVID-19 pandemic. It is important to mention that the present work was carried out following PRISMA guidelines. However, it is relevant to recognize certain limitations in our research. In particular, the limited availability of studies on the prevalence of CVS in a small number of countries limited our analysis. Furthermore, given that the included studies were cross-sectional in nature, we cannot establish a definitive causal relationship. Finally, it is important to keep in mind that our investigation was based on data collected in individual studies during a specific period, implying that circumstances might have changed over time.
Conclusions
This study discovered a high prevalence of computer vision syndrome, affecting 74% of the participants. These results suggest that many individuals may experience prolonged electronic screen usage symptoms, including visual fatigue, headaches or neck pain, dry eyes, and blurred vision, among others. Therefore, it is crucial to emphasize the importance of implementing preventive and therapeutic measures to reduce the risk of developing CVS and improve the affected individuals' quality of life.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
References
Pavel IA, Bogdanici CM, Donica VC, Anton N, Savu B, Chiriac CP, et al. Computer Vision Syndrome: An Ophthalmic Pathology of the modern era. Med Kaunas Lith. 2023;59(2):412. https://doi.org/10.3390/medicina59020412.
Galindo-Romero C, Rodríguez-Zamora CL, García-Ayuso D, Di Pierdomenico J, Valiente-Soriano FJ. Computer vision syndrome-related symptoms in presbyopic computer workers. Int Ophthalmol. 2023;1–9. https://doi.org/10.1007/s10792-023-02724-z.
Anbesu EW, Lema AK. Prevalence of computer vision syndrome: a systematic review and meta-analysis. Sci Rep. 2023;13(1):1801. https://doi.org/10.1038/s41598-023-28750-6.
Lema AK, Anbesu EW. Computer vision syndrome and its determinants: a systematic review and meta-analysis. SAGE Open Med. 2022;10:20503121221142400. https://doi.org/10.1177/20503121221142402.
Iqbal M, Said O, Ibrahim O, Soliman A. Visual sequelae of computer vision syndrome: a cross-sectional case-control study. J Ophthalmol. 2021;2021:6630286. https://doi.org/10.1155/2021/6630286.
Long J, Cheung R, Duong S, Paynter R, Asper L. Viewing distance and eyestrain symptoms with prolonged viewing of smartphones. Clin Exp Optom 1 de marzo de. 2017;100(2):133–7. https://doi.org/10.1111/cxo.12453.
Tesfaye AH, Alemayehu M, Abere G, Mekonnen TH. Prevalence and Associated Factors of Computer Vision Syndrome among Academic Staff in the University of Gondar, Northwest Ethiopia: an Institution-based cross-sectional study. Environ Health Insights. 2022;16:11786302221111864. https://doi.org/10.1177/11786302221111865.
Cantó-Sancho N, Porru S, Casati S, Ronda E, Seguí-Crespo M, Carta A. Prevalence and risk factors of computer vision syndrome—assessed in office workers by a validated questionnaire. PeerJ 3 de marzo de. 2023;11:e14937. https://doi.org/10.7717/peerj.14937.
Almalki AM, Alblowi M, Aldosari AM, Khandekar R, Al-Swailem SA. Population perceived eye strain due to digital devices usage during COVID-19 pandemic. Int Ophthalmol 5 de diciembre de. 2022;1–9. https://doi.org/10.1007/s10792-022-02593-y.
Karl KA, Peluchette JV, Aghakhani N. Virtual work meetings during the COVID-19 pandemic: the good, bad, and ugly. Small Group Res junio de. 2022;53(3):343–65. https://doi.org/10.1177/10464964211015286.
Pandya A, Lodha P. Social connectedness, excessive screen time during COVID-19 and Mental Health: a review of current evidence. Front Hum Dyn. 2021;3. https://doi.org/10.3389/fhumd.2021.684137. https://www.frontiersin.org/articles/.
Mrayyan MT, Alseid ARH, Ghoolah TS, Al-Shaikh Ali MH, Mrayan M. Investigating the prevalence of computer vision syndrome (CVS) among undergraduate nursing students: a cross-sectional study. SAGE Open Nurs. 2023;9:23779608231191884. https://doi.org/10.1177/23779608231191883.
Seresirikachorn K, Thiamthat W, Sriyuttagrai W, Soonthornworasiri N, Singhanetr P, Yudtanahiran N, et al. Effects of digital devices and online learning on computer vision syndrome in students during the COVID-19 era: an online questionnaire study. BMJ Paediatr Open. 2022;6(1): e001429. https://doi.org/10.1136/bmjpo-2022-001429.
Usgaonkar U, Shet Parkar SR, Shetty A. Impact of the use of digital devices on eyes during the lockdown period of COVID-19 pandemic. Indian J Ophthalmol. 2021;69(7):1901–6. https://doi.org/10.4103/ijo.IJO_3500_20.
Zheng X, Shi L, Ou W, Xue Y, Xu Y, Xue B, et al. Effects of physical activity and use of digital devices on visual acuity in children and adolescents during the COVID-19 pandemic: a cross-sectional study. Front Public Health. 2022;10: 1017479. https://doi.org/10.3389/fpubh.2022.1017479.
Munn Z, Tufanaru C, Aromataris E. JBI’s systematic reviews: data extraction and synthesis. Am J Nurs. 2014;114(7):49–54. https://doi.org/10.1097/01.NAJ.0000451683.66447.89.
Mohan A, Sen P, Shah C, Jain E, Jain S. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: Digital eye strain among kids (DESK study-1). Indian J Ophthalmol. 2021;69(1):140–4. https://doi.org/10.4103/ijo.IJO_2535_20.
Alabdulkader B. Effect of digital device use during COVID-19 on digital eye strain. Clin Exp Optom. 2021;104(6):698–704. https://doi.org/10.1080/08164622.2021.1878843.
Zenbaba D, Sahiledengle B, Bonsa M, Tekalegn Y, Azanaw J, Kumar Chattu V. Prevalence of computer vision syndrome and associated factors among instructors in Ethiopian universities: a web-based cross-sectional study. ScientificWorldJournal. 2021;2021:3384332. https://doi.org/10.1155/2021/3384332.
Noreen K, Ali K, Aftab K, Umar M. Computer vision syndrome (CVS) and its associated risk factors among undergraduate medical students in midst of COVID-19. Pak J Ophthalmol. 2021. https://doi.org/10.36351/pjo.v37i1.1124.
L W, X W, Y D. Computer Vision Syndrome during SARS-CoV-2 outbreak in University students: a comparison between Online courses and Classroom lectures. Front Public Health. 2021. https://doi.org/10.3389/fpubh.2021.696036.
Zayed HAM, Saied SM, Younis EA, Atlam SA. Digital eye strain: prevalence and associated factors among information technology professionals, Egypt. Environ Sci Pollut Res Int. 2021;28(20):25187–95. https://doi.org/10.1007/s11356-021-12454-3.
Abuallut I, Ajeebi RE, Bahari AY, Abudeyah MA, Alyamani AA, Zurayyir AJ, et al. Prevalence of computer vision syndrome among school-age children during the COVID-19 pandemic, Saudi Arabia: a cross-sectional survey. Child Basel Switz. 2022;9(11):1718. https://doi.org/10.3390/children9111718.
Basnet A, Pathak SB, Marasini A, Pandit R, Pradhan A. Digital eye strain among adults presenting to tertiary care hospital in the era of COVID-19 pandemic: a descriptive cross-sectional study. JNMA J Nepal Med Assoc. 2022;60(245):22–5. https://doi.org/10.31729/jnma.7092.
Coronel-Ocampos J, Gómez J, Gómez A, Quiroga-Castañeda PP, Valladares-Garrido MJ. Computer visual syndrome in medical students from a private University in Paraguay: a survey study. Front Public Health. 2022;10: 935405. https://doi.org/10.3389/fpubh.2022.935405.
Estrada Araoz EG, Paricahua Peralta JN, Zuloaga Araoz MC, Gallegos Ramos NA, Valverde YP, Herrera RQ, et al. Prevalence of computer vision syndrome in Peruvian university students during the COVID-19 health emergency. Arch Venez Farmacol Ter. 2022;264:70.
Munsamy AJ, Naidoo S, Akoo T, Jumna S, Nair P, Zuma S, et al. A case study of digital eye strain in a university student population during the 2020 COVID-19 lockdown in South Africa: evidence of an emerging public health issue. J Public Health Afr. 2022;13(3): 2103. https://doi.org/10.4081/jphia.2022.2103.
Roy S, Sharif AB, Chowdhury S, Iktidar MA. Unavoidable online education due to COVID-19 and its association to computer vision syndrome: a cross-sectional survey. BMJ Open Ophthalmol. 2022;7(1): e001118. https://doi.org/10.1136/bmjophth-2022-001118.
Uwimana A, Ma C, Ma X. Concurrent rising of dry eye and eye strain symptoms among university students during the COVID-19 pandemic era: a cross-sectional study. Risk Manag Healthc Policy. 2022;15:2311–22. https://doi.org/10.2147/RMHP.S388331.
Wangsan K, Upaphong P, Assavanopakun P, Sapbamrer R, Sirikul W, Kitro A, et al. Self-reported computer vision syndrome among Thai University students in virtual classrooms during the COVID-19 pandemic: prevalence and associated factors. Int J Environ Res Public Health. 2022;19(7): 3996. https://doi.org/10.3390/ijerph19073996.
Agarwal R, Tripathi A, Khan IA, Agarwal M. Effect of increased screen time on eyes during COVID-19 pandemic. J Fam Med Prim Care. 2022;11(7):3642–7. https://doi.org/10.4103/jfmpc.jfmpc_2219_21.
Almousa AN, Aldofyan MZ, Kokandi BA, Alsubki HE, Alqahtani RS, Gikandi P, et al. The impact of the COVID-19 pandemic on the prevalence of computer vision syndrome among medical students in Riyadh, Saudi Arabia. Int Ophthalmol. 2022;1–9. https://doi.org/10.1007/s10792-022-02525-w.
Demirayak B, Yılmaz Tugan B, Toprak M, Çinik R. Digital eye strain and its associated factors in children during the COVID-19 pandemic. Indian J Ophthalmol. 2022;70(3):988–92. https://doi.org/10.4103/ijo.IJO_1920_21.
Shahidi SH, Stewart Williams J, Hassani F. Physical activity during COVID-19 quarantine. Acta Paediatr Oslo nor 1992. 2020;109(10):2147–8. https://doi.org/10.1111/apa.15420.
Bertrand L, Shaw KA, Ko J, Deprez D, Chilibeck PD, Zello GA. The impact of the coronavirus disease 2019 (COVID-19) pandemic on university students’ dietary intake, physical activity, and sedentary behaviour. Appl Physiol Nutr Metab. 2021;46(3):265–72. https://doi.org/10.1139/apnm-2020-0990.
Tison GH, Avram R, Kuhar P, Abreau S, Marcus GM, Pletcher MJ, et al. Worldwide Effect of COVID-19 on physical activity: a descriptive study. Ann Intern Med. 2020;173(9):767–70. https://doi.org/10.7326/M20-2665.
Zaccagni L, Toselli S, Barbieri D. Physical activity during COVID-19 lockdown in Italy: a systematic review. Int J Environ Res Public Health. 2021;18(12): 6416. https://doi.org/10.3390/ijerph18126416.
Castañeda-Babarro A, Arbillaga-Etxarri A, Gutiérrez-Santamaría B, Coca A. Physical activity change during COVID-19 confinement. Int J Environ Res Public Health. 2020;17(18): 6878. https://doi.org/10.3390/ijerph17186878.
Vargo D, Zhu L, Benwell B, Yan Z. Digital technology use during COVID-19 pandemic: a rapid review. Hum Behav Emerg Technol. 2021;3(1):13–24. https://doi.org/10.1002/hbe2.242.
Adane F, Alamneh YM, Desta M. Computer vision syndrome and predictors among computer users in Ethiopia: a systematic review and meta-analysis. Trop Med Health. 2022;50:26. https://doi.org/10.1186/s41182-022-00418-3.
Singhal R, Kumar A, Singh H, Fuller S, Gill SS. Digital device-based active learning approach using virtual community classroom during the COVID-19 pandemic. Comput Appl Eng Educ. 2021;29(5):1007–33. https://doi.org/10.1002/cae.22355.
Bahkir FA, Grandee SS. Impact of the COVID-19 lockdown on digital device-related ocular health. Indian J Ophthalmol. 2020;68(11):2378–83. https://doi.org/10.4103/ijo.IJO_2306_20.
Khan S, Khan S, Midya MZ, Khan IJ, Raghib M. Comparison of prevalence data about digital eye strain (DES), pre-lockdown versus post-lockdown period in India: a systematic review study. Children. 2021;17:18.
Subaie MA, Al-Dossari S, Bougmiza MI. Computer vision syndrome among mobile phone users in Al-Ahsa, Kingdom of Saudi Arabia. Al-Basar Int J Ophthalmol. 2017;4(4):99. https://doi.org/10.4103/bijo.bijo_13_18.
Alhasan AS, Aalam WA. Magnitude and determinants of computer vision syndrome among radiologists in Saudi Arabia: a national survey. Acad Radiol. 2022;29(9):e197-204. https://doi.org/10.1016/j.acra.2021.10.023.
Guan H, Okely AD, Aguilar-Farias N, Cruz B, del Draper P, Hamdouchi CE. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc Health. 2020;4(6):416–8. https://doi.org/10.1016/S2352-4642(20)30131-0.
Robinson E, Boyland E, Chisholm A, Harrold J, Maloney NG, Marty L, et al. Obesity, eating behavior and physical activity during COVID-19 lockdown: a study of UK adults. Appetite. 2021;156: 104853. https://doi.org/10.1016/j.appet.2020.104853.
Mukhtar K, Javed K, Arooj M, Sethi A. Advantages, limitations and recommendations for online learning during COVID-19 pandemic era. Pak J Med Sci. 2020;36(4):27–31. https://doi.org/10.12669/pjms.36.COVID19-S4.2785. (COVID19-S).
Pokhrel S, Chhetri R. A literature review on impact of COVID-19 pandemic on teaching and learning. High Educ Future. 2021;8(1):133–41. https://doi.org/10.1177/2347631120983481.
Kapasia N, Paul P, Roy A, Saha J, Zaveri A, Mallick R, et al. Impact of lockdown on learning status of undergraduate and postgraduate students during COVID-19 pandemic in West Bengal, India. Child Youth Serv Rev. 2020;116: 105194. https://doi.org/10.1016/j.childyouth.2020.105194.
Ranasinghe P, Wathurapatha WS, Perera YS, Lamabadusuriya DA, Kulatunga S, Jayawardana N, et al. Computer vision syndrome among computer office workers in a developing country: an evaluation of prevalence and risk factors. BMC Res Notes. 2016;9(1):150. https://doi.org/10.1186/s13104-016-1962-1.
Hassan A, Mmk B. Prevalence of computer vision syndrome (CVS) amongst the Students of Khyber Medical University, Peshawar. En: Islamabad Congress of Ophthalmology. 2017. p. 59.
Rao S, et al. Addressing computer vision syndrome among different sections of society working digitally amidst prevailing COVID-19 pandemic: a cross-sectional study. Al Ameen J Med Sci. 2021;14(4):305–13.
Neti N, Prabhasawat P, Chirapapaisan C, Ngowyutagon P. Provocation of dry eye disease symptoms during COVID-19 lockdown. Sci Rep. 2021;11(1):24434. https://doi.org/10.1038/s41598-021-03887-4.
Tribley J, McClain S, Karbasi A, Kaldenberg J. Tips for computer vision syndrome relief and prevention. Work Read Mass. 2011;39(1):85–7. https://doi.org/10.3233/WOR-2011-1183.
Acknowledgements
We express our gratitude to Milagros Díaz-Torres, Olga Campos-Santa Cruz, and Ana Paula Mesta-Pintado for their valuable contributions to the study protocol development and for their efforts in selecting and extracting the initial data. Their assistance has been instrumental in ensuring the success of this study.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, JJB, DALF, and MJVG; methodology, MJVG, AS, RS, SA, SS, and RS; software, DALF; validation, JJB; formal analysis, DALF; investigation, AS; resources, AJRM; data curation, DALF; writing—original draft preparation, DALF, EAM, and RS; writing—review and editing, DALF, AS, SA, SS, JJB, EAM, AJRM, and RS; visualization, AS; supervision, AJRM and RS. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
León-Figueroa, D.A., Barboza, J.J., Siddiq, A. et al. Prevalence of computer vision syndrome during the COVID-19 pandemic: a systematic review and meta-analysis. BMC Public Health 24, 640 (2024). https://doi.org/10.1186/s12889-024-17636-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17636-5