
Abstract
Background
Coronary artery diseases (CADs) are the most important non‑communicable diseases (NCDs), which cause the highest number of deaths around the world. Hypertension (HTN), dyslipidemia (DL), diabetes mellitus (DM), obesity (OB), low physical activity (LPA), smoking, opium consumption (OC) and anxiety are the most important CAD risk factors, which are more dangerously present in combination in some patients.
Methods
A total of 5835 people aged 15 to 75 years were enrolled in the phase 1 (2012) and followed up to the phase 2 (2017) of the population-based Kerman coronary artery diseases risk factors study (KERCADRS). The prevalence and pattern of different combinations of CAD risk factors (double to quintuple) and their 5-year incidence rates were assessed.
Results
The prevalence of single CAD risk factors (RFs) in phase 2 was 50.2% (DL), 47.1% (LPA), 28.1% (abdominal obesity), 21.2% (OB), 16.5% (HTN), 9.2% (smoking), 9.1% (OC), and 8.4% (DM). The most frequent combination of risk factors was LPA plus DL (23.9%), metabolic syndrome (19.6%), and DL plus OB (17.8%). The 5-year incidence rates of multiple comorbidities (in persons per 100 person-years) was DL plus LPA (2.80%), HTN plus DL (1.53%), and abdominal obesity (AOB) plus DL (1.47%). The most participants (84.4%) suffered from at least one RF, while 54.9% had at least two and 29.9% had at least three RFs.
Conclusion
The results showed that a large portion of the study population suffers from multiple CAD RFs. The findings underscore the importance of identifying multiple CAD risk factors to reduce the overall burden of these NCDs.
Similar content being viewed by others

Introduction
Coronary artery diseases (CADs) are a group of cardiovascular diseases (CVDs) that are the most common cause of death all over the world [1,2,3]. CAD is an atherosclerotic disorder with an inflammatory background that could present in different types such as: stable angina, unstable angina, myocardial infarction (MI), and sudden death [4, 5]. According to the recent studies, CAD risk factors are divided into two main categories, non-modifiable and modifiable risk factors [6, 7]. Age, gender, race, and family history are mentioned as non-modifiable risk factors [8, 9]. Modifiable risk factors include hypertension (HTN), dyslipidemia (DL), diabetes mellitus (DM), obesity (OB), abdominal obesity (AOB), low physical activity (LPA), smoking, opium consumption (OC) and anxiety [10, 11]. The Kerman coronary artery diseases risk factors (KERCADR) study is a population based epidemiological research, which studied 5900 people aged 15–75 years old in phase 1 and 10,000 people in phase 2 in Kerman aimed to investigate the prevalence of CAD risk factors. Recent studies represent strong relation between DM and CAD [12]. As a result, atherosclerotic process happens sooner and is more prevalent in diabetic patients [12,13,14]. The results of our previous studies demonstrated that the prevalence of HTN, the most common modifiable risk factor, was 19.2% of which 13.9% has already been diagnosed and 5.3% still were unaware of their disease [15]. Also, the relationship between HTN and increased risk of CADs has been proven [16].
DL is a major risk factor for CVDs specially CAD [17, 18]. 56.9% of participants were found to suffer from DL that only 16.2% were already detected and 40.7% were undiscovered [19]. Smoking is classified as one of the modifiable CAD risk factors [20]. Also, long term use of opium is known as a significant risk factor of CAD [21, 22]. On the other hand, OB and overweight can cause CAD [23]. According to KERCADR study phase 1 and 2, the prevalence of OB is 22.3% in phase 2, which increased between the two phases of the study [24, 25]. LPA can intensify the risk of atherosclerosis [26] and it has been estimated that its prevalence is 47.2 in Kerman population and more commonly in women [27].
An Australian study demonstrated that people who had more risk factors were also more likely to report a heart attack, stroke, angina, or atherosclerosis, independent of age and sex [28]. Although only one risk factor is sufficient to increase the risk of a disease, the risk is augmented when another risk factor is added [29]. In a recent cohort study in Shahrekord in southwest Iran, only 39.5 percent of the participants have no non‑communicable diseases (NCD) risk factors; while the people with a co-existence of two, and ≥ 3 NCDs were 16.6 and 15.9 percent respectively [30]. In phase 1 of KERCADRS five years earlier, almost 60% of the people living in Kerman had at least 2 CAD risk factors, and these were more frequent among women and older people [29]. As Iran's predominantly young population approaches middle Ages, there is a growing concern about the burden of CADs in the country in future. To develop effective preventive and management strategies, it is crucial to have accurate and up-to-date information about the trends in the prevalence and incidence of these risk factors, particularly in individuals who have multiple of them. Therefore, the aim of this study was assessing the prevalence of multiple CAD risk factors to find endangered groups of population and comparing the prevalence and assessing the incidence rate of these in a 5-year interval between phases 1 and 2 of KERCADRS. The results can help the health policy makers to have a better insight into the society health status and make plans to decrease the incidence rate of CVDs and the burden of these diseases.
Methods
Population and sampling
The first phase of KERCADRS, a population-based, prospective cohort study, was performed in the physiology research center of Kerman from 2009 to 2012 with 5835 participants (having completed data) aged 15 to 75 years old. A total number of 9993 people aged 15 to 80 years old (having completed data) with the mean age of 46.2 ± 15.7 participated in the second phase of the study from 2014 to 2017. The inclusion criteria were: Iranian with at least a 1-year period of residency in Kerman and signing the informed consent form.
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and in conformity with the national guidelines for conducting human studies. It was approved by the Ethics Committee of Kerman university of medical science, Kerman, Iran (Ethical code: IR.KMU.AH.REC.1400.21).
Written informed consent was obtained from all subjects. For those who were between 15 and 18 years old, the consent was obtained from both the participant and his/her legal guardian.
A skilled physician examined all participants, took their blood pressure, pulse rates and their medical history. A questionnaire consisted of the history of underlying diseases such as DM, HTN, DL, and others, was also completed by the physician. Other necessary data comprising demographic information, height, weight, history of cigarette smoking, OC, and level of physical activity were collected by trained interviewers. 10–12 h fasting blood samples were taken from participants and fasting blood sugar (FBS), total cholesterol, triglyceride (TG), low-density lipoprotein (LDL), and high-density lipoprotein (HDL) were measured using traditional laboratory kits.
Definition of coronary artery disease risk factors
Participants who had FBS ≥ 126 mg/dL at the time of recruitment or were previously diagnosed with DM or were injecting insulin or taking anti-diabetes medications, were considered as diabetic patients [31]. According to the American heart association (AHA), HTN was defined as a systolic blood pressure ≥ 140 mm Hg or a diastolic blood pressure ≥ 90 mm Hg [32]. Also, people with a history of taking any antihypertensive drug before participating in the study were considered as hypertensive patients.
DL was characterized by total cholesterol ≥ 240 mg/dL or LDL ≥ 160 mg/kg, or HDL < 40 mg/kg in men or HDL < 50 mg/kg in women, or triglyceride (TG) level of ≥ 150 mg/dl, or who were under treatment with lipid-lowering drugs [19].
Physical activity (PA) refers to all activities which were measured by World Health Organization global physical activity questionnaire (GPAQ). Metabolic equivalents of task (METs) were calculated based on the daily activity of the participants to express the intensity of physical activity. MET is the use of energy in an adult while sitting [33]. Low, moderate, and severe physical activity levels were defined based on weekly METs values. A weekly MET value of less than 600 is considered as LPA, while a value between 600 and 3000 is considered moderate. Severe physical activity is defined as a weekly MET value of greater than 3000 [34]. Current cigarette smoking referred to smoke of at least one cigarette per day. OC was referred to regularly consumption of opium by inhalation or orally more than 3 times per week as defined according to the diagnostic and statistical manual of mental disorders-IV (DSM-IV) criteria.
Participant’s height was measured by a tape stadiometer with a minimum measurement of 0.2 cm in a standing position, without shoes, and their weight was measured by a calibrated standard weighing balance (Seca, model 707, Germany). The body mass index (BMI) was calculated through dividing their weight in kilograms by height in meters squared. Participants were categorized as overweight if their BMI was between 25 and 29.9 kg/m2 and categorized as obese if their BMI was ≥ 30 kg/m2.
Metabolic syndrome is a cluster of conditions that occur together leading to increase the risk of CADs. The syndrome defines as the presence of 3 or more of the criteria of waist circumference ≥ 102 cm in men and ≥ 88 cm in women, TG > 150, HDL < 40 in men and < 50 in women, blood pressure > 130/85 or taking medication for HTN, FBS > 100 mg/dl or taking medications for hyperglycemia [35, 36].
Statistical analysis
All analyzes were performed using SPSS version 14.1, and P < 0.05 was considered as statistically significant. Multiple CADRFs included a combination of two or more factors of HTN, DL, DM, OB, AOB, LPA, smoking, and OC. The reference population was Kerman census population data in 2016. All prevalence rates were presented as percentage frequencies and compared using the chi-squared test among sexes and age groups.
Incidence rate of multiple CAD risk factors
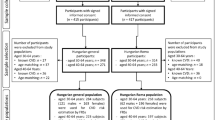
For multiple CAD incidence rate calculation those people who participated in phase 1 and followed to phase 2 were considered. Here as an example the incidence rate calculation for LPA plus DL is presented. Out of 5835 participants with complete data in phase 1, 2158 individuals who were already with LPA plus DL, excluded from this analysis. The remaining 3677 participants were physically active enough and had normal lipid levels (were at risk for becoming LPA plus DL) during follow-up. During the follow-up period, 1892 participants died or were lost to follow-up, while 1785 participants (with normal lipids and enough physical activity at baseline) visited phase 2. Of these, 363 individuals developed LPA and DL, yielding an incidence rate of 2.8 per 100 person-years (Fig. 1). To calculate the person-years at risk for those who did not have any CAD risk factors (CADRFs) at the phase 1 visit, the time difference (in years) between the phase 1 and phase 2 visits was calculated. For those lost to follow-up, an average of 2.5 years (half of the overall follow-up time) was assumed to be the person at risk [37].

The flow chart of the study for those who participated in both phases of the study (here for calculation of DL plus LPA). DL Dyslipidemia, IR Incidence rate, LPA Low physical activity
Using the above information, the incidence rate (expressed as person per 100 person-years) was calculated using the following formula [37]:
where Time is the exact duration (in years) between the two attending of each participant in phases 1 and 2.
Results
Prevalence of multiple coronary artery disease risk factors
Totally 9993 people were enrolled in phase 2 study of which 4055 (40.6%) were male. The mean age of the participants at enrollment was 46.2 ± 15.7 years. 4669 (46.7%) were jobless or housewife while the other participants had governmental or non-governmental jobs.
The prevalence of DM, HTN, DL, OC, and metabolic syndrome significantly decreased in phase 2 compared with the phase 1 (5 years earlier). The prevalence of OB, AOB, LPA and cigarette smoking increased (Table 1).
The prevalence of type 2 diabetes was 6.7% in men that was lower than women (10%). The prevalence of HTN in phase 2 was not statistically different between females (16.7%) and males (16.3%) (P = 0.571). The prevalence of DL was significantly higher in women (56.9%) than men (43.8). About 26.6% of female participants were obese while the prevalence of OB was lower in men (15.9%). Also, AOB was more frequent in women (41.3%) than men (15.4%). Moreover, the prevalence of cigarette smoking, and OC was more frequent in men than women (P < 0.001). The most frequent level of LPA was observed among women and its prevalence was higher (48%) than men (46.3%).
Different combinations of risk factors (two or more simultaneous risk factors) were assessed but the prevalence of most important ones in phases 1 and 2 are reported in Table 2.
The most pravalent double combination risk factor in both phases was LPA/DL (37.8% and 23.9% respectively), which its prevalence was significantly decreased in phase 2 compared with phase 1 (P < 0.001). The prevalence of combined DM/AOB and DM/OB increased in phase 2 compared with phase 1. Combination of HTN and OB also appeared to be more frequent in phase 2 (6.4%) than phase 1 (3.4%). Because of significant diminution in the prevalence of DL, the prevalence of DM/DL, smoking/DL, HTN/DL and LPA/DL decreased in phase 2 compared to phase 1. The prevalence of DL/AOB was higher in phase 2 (17.8%) than phase 1 (14.1%). The prevalence of LPA/DM, LPA/OB, LPA/DM/OB, and DM/DL/OB increased in phase 2. Metabolic syndrome appeared to be less frequent in phase 2 than in phase 1 (Table 2).
Due to the existence of more than three CAD risk factors in some of the participants, the prevalence of quadruple and quintuple risk factors in phase 2 are also reported (in clinically important- then in more prevalent combinations order) (Table 3).
The prevalence of almost all combined risk factors except those combinations that include smoking and OC, was significantly higher in women in both phases (P < 0.001) (Table 4).
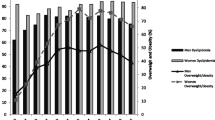
The prevalence of some of the multiple CAD risk factors increased in the second phase of the study in the gender subcategories. The data shows that 2.1% of men had DM plus AOB in phase 2 which was significantly higher than phase 1 (1.3%). The prevalence of DM plus AOB was 7.2% among women in phase 2, which was 2.7% higher than its prevalence in phase one. Also, the overall prevalence rates of HTN/OB, LPA/DM, LPA/OB and DM/LPA/OB were more frequent in both genders in phase 2 compared to phase 1. Although the combination of HTN/DL was more prevalent among women in phase 2 than in phase 1, its prevalence decreased from 9.7% to 8% among men. The prevalence of LPA/DL was significantly lower in the phase 2 in both genders. complementary information about the prevalence of multiple CAD risk factors in phases 1 and 2 based on gender are shown in Fig. 2.

Comparison of the prevalence of multiple CADRFs in phase 1 and 2 of KERCADRS based on gender. In the legend, P1 means phase 1 and P2 means phase 2. TP1, Total phase 1; TP2, Total phase 2; MP1, Male phase1; MP2, Male phase2; FP1, Female phase1; FP2, Female phase2. AOB Abdominal obesity, DL Dyslipidemia, DM Diabetes mellitus, HTN Hypertension, LPA Low physical activity, OB Obesity, OC Opium consumption
Furthermore, age plays a significant role in the occurrence of cardiometabolic diseases. The standardized prevalence of multiple CAD risk factors based on differrent age groups are shown in Table 5. The data strongly support that the prevalence of multiple CAD risk factors increases with aging. The most prevalent combination risk factor in young (15–24 years) participants was LPA/DL with 18.7%.
Incidence rate of multiple coronary artery disease risk factors
The data of 2818 people who participated in both phases 1 and 2 were used for incidence rate (IR) calculation. The IR of multiple CADRFs are summarized in Table 6. The highest incidence rate was observed among the patients who suffered from DL and had LPA (2.80 persons/100 person-years). The IR for HTN plus DL was 1.53 and for DL plus AOB was 1.48 persons/100 person-years, ranking them in the second and third positions.
The results of the distribution of the prevalence of multiple CAD risk factors showed that most of the participants (84.4%) had at least one risk factor of CAD, indicating a high burden of cardiovascular risk in the study population. Moreover, 54.9% had at least two, 29.9% had at least three, and 13.8% had at least four of the studied risk factors. This suggests a high clustering of risk factors in some individuals (Table 7).
Discussion
Our study is the first cohort for CADRFs in the southeast of Iran in which we examined the prevalence and trend of multiple CADRFs and their 5-year incidence rate among 15–80-year old population. The study's main result was that the majority of the participants (84.4%), had at least one CADRF leaving only 15.6% without any risk factor. More than half (54.9%) of the participants had two or more risk factors for CAD. In a study conducted by Mamudu et al., in USA, it was found that almost all of their participants (98.3%) had at least one risk factor for developing CAD. Furthermore, 23.5% exhibited two risk factors, 26.4% had three, 19.6% had four, and 14% had five or more risk factors [38]. According to another study conducted by Yamada Harada and colleagues in Japan, the research revealed that the highest proportion of risk factor combination was observed when two risk factors were present. Among individuals without DM, this combination accounted for 39.6% of cases and among those with DM, it accounted for 36.4% of cases [39].
In the present study, the most prevalent combination of multiple risk factors was LPA plus DL (23.9%), followed by metabolic syndrome (19.6%() and DL plus AOB (17.8%). Compared to the first phase of the study, the first two combinations has shown a significant decrease, but the prevalence of DL plus AOB increased. This reduction of first two combination can be attributed to a notable decline in DL between the two phases [19]. However, the increase in the prevalence of AOB has masked the decreasing effect of DL, resulting in an increase in the prevalence of DL plus AOB.
The most prevalent single risk factors are DL, LPA, AOB, and OB which are significant public health concerns. DL was found in half of the study participants (50.2%), LPA in 47.1%, AOB in 28.1% and OB in 21.2% of them.
In the Golestan cohort study in northern Iran, Ahmadi et al. (2016) found that a significant proportion of participants had low levels of physical activity (68.2%), which is higher than its prevalence in our study. Also the prevalence of OB was comparatively higher in Golestan study (25.4%) [40]. In the Shahrekord cohort study in Southwest Iran, also a higher prevalence of several risk factors of CAD was found. These included DM (9.8%), OB (27.1%), LPA (57%), and HTN (17.1%). Additionally, the study found that opium use and smoking were more prevalent in Shahrekord as 12.5% and 24.7%, respectively [30].
In the Azar cohort study, conducted by Farhang et al. in 2019 a higher prevalence of OB, (31.4%), DM (13.9%) and HTN (19.6%) was also found [41]. In an Iranian.
national survey in 2016 a higher prevalence of LPA (51.3%), HTN (25%), smoking (14.2%) was Found. These differences may be due to the age range of the population studied or the regional variations in lifestyle and environmental exposures [42,43,44,45]. In the Golestan, Shahrekord and Azar cohorts the population under the studies were in the age of 35 years or higher up to 80 years, which could be one of the reasons for higher prevalence of mentioned CADRFs in their studied population. These findings highlight the significant burden of cardiovascular risk factors in the country and emphasize the need for effective prevention and management strategies nationaly. Fortunately, DL and multiple RFs including DL showed reduction in the prevalence in phase 2 compared to phase 1 of the present study. The reason for reduction of DL in the 5 years between the two phases may be due to the provision of more treatment facilities by the government during this period In Iran [34, 46]. In recent years, the government has performed a health promotion plan that includes covering the treatment costs by providing more efficient health insurance to almost all Iranians. The tendency for replacement of saturated fats with unsaturated oil in cooking may also have played a role. Despite the control of laboratory factors such as blood sugar and plasma lipids, there is still a need for more follow-up for appropriate methods in primary prevention in terms of factors related to physical fitness (including BMI and accumulated body fat level) and lifestyle.
The trends in the prevalence of CAD risk factors over a 5-year period indicate a significant increase in the prevalence of OB, AOB, and low physical activity in the community. Consequently, the combined factors including these risk factors, have also exhibited a noticeable increase in the prevalence. This emphesizes an overall rise in health risks associated with sedentary lifestyles and unhealthy dietary habits [25, 34].
The high incidence rate of multiple CADFRs among the participants of the present study is also of great concern. Among the double clusters LPA/DL with 2.81, HTN/DL with 1.53, and DL/OB with 1.48 person/hundred person-years, and among the triple clusters, DM/HTN/OB with 0.55, DM/HTN/DL with 0.45 and DM/DL/OB with 0.32 person/hundred person-years, have the fastest incidence rate in our studied population. These are probably due to urbanization, sedentary jobs and lifestyle and shortage of time and motivation for having more physical activity [47]. Carrying excess weight in obese subjects can significantly increase the risk of developing mobility issues, such as joint pain and reduced flexibility, which can make it challenging for individuals to engage in physical activity [48]. Furthermore, OB is frequently linked with low self-esteem and body image concerns, which may discourage individuals from participating in physical activity due to fear of judgment or discomfort [49]. As a result, addressing OB and LPA through appropriate lifestyle changes, such as healthy eating habits and regular exercise, can help improve mobility, increase self-esteem, and promote a more active lifestyle. Otherwise the co-occurrence of multiple risk factors increases the likelihood of developing CAD and its associated complications, such as heart attack and stroke.
Study limitations
The KERCADR study has several limitations that should be considered when interpreting the results. First, the study included only urban population in Kerman, and the results may not be generalizable to rural population. Second, the study relied on self-reported data for some risk factors, such as smoking, opium consumption and physical activity, which may be subject to recall bias, under or over reporting.
Conclusion
Overall, more than half of the study population have at least two and about one thierd have at least three CAD risk factors. These are valuable information for policymakers and healthcare providers to develop and implement effective strategies for reducing the burden of CADs in Kerman. The high prevalence of CAD risk factors and the clustering of them in mojority of individuals highlight the urgent need for effective preventive strategies, early detection, and management of these risk factors. The decreasing trend in DL and opium consumption prevalences is encouraging, but more efforts are needed to decrease the prevalence and incidence rate of more important metabolic risk factors, such as HTN, DM, OB, AOB, and LPA.
Availability of data and material
The datasets used and/or analysed during the present study are available from the corresponding author on reasonable request.
References
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–322.
Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143(8):CIR0000000000000950.
Wang H, Naghavi M, Allen C, Barber R, Bhutta Z, Carter A. A systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459–544.
Ross R. Atherosclerosis—an inflammatory disease. N Engl J Med. 1999;340(2):115–26.
Álvarez-Álvarez MM, Zanetti D, Carreras-Torres R, Moral P, Athanasiadis G. A survey of sub-Saharan gene flow into the Mediterranean at risk loci for coronary artery disease. Eur J Hum Genet. 2017;25(4):472–6.
Libby P, Ridker PM, Hansson GK. Progress and challenges in translating the biology of atherosclerosis. Nature. 2011;473(7347):317–25.
Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart views: the official journal of the Gulf Heart Association. 2017;18(3):109.
Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. The lancet. 2014;383(9921):999–1008.
Jousilahti P, Laatikainen T, Peltonen M, Borodulin K, Männistö S, Jula A, et al. Primary prevention and risk factor reduction in coronary heart disease mortality among working aged men and women in eastern Finland over 40 years: population based observational study. BMJ. 2016;352:i721.
Lind L. Population-based cardiovascular cohort studies in Uppsala. Upsala J Med Sci. 2019;124(1):16–20.
Pencina MJ, Navar AM, Wojdyla D, Sanchez RJ, Khan I, Elassal J, et al. Quantifying importance of major risk factors for coronary heart disease. Circulation. 2019;139(13):1603–11.
Patsouras A, Farmaki P, Garmpi A, Damaskos C, Garmpis N, Mantas D, et al. Screening and risk assessment of coronary artery disease in patients with type 2 diabetes: an updated review. In Vivo. 2019;33(4):1039–49.
Glovaci D, Fan W, Wong ND. Epidemiology of diabetes mellitus and cardiovascular disease. Curr Cardiol Rep. 2019;21:1–8.
Albers AR, Krichavsky MZ, Balady GJ. Stress testing in patients with diabetes mellitus: diagnostic and prognostic value. Circulation. 2006;113(4):583–92.
Williams B, Lindholm LH, Sever P. Systolic pressure is all that matters. The lancet. 2008;371(9631):2219–21.
Dawber TR, Moore FE, Mann GV II. Coronary heart disease in the Framingham study. Int J Epidemiol. 2015;44(6):1767–80.
Reiner Ž. Statins in the primary prevention of cardiovascular disease. Nat Rev Cardiol. 2013;10(8):453–64.
Graham I, Cooney M-T, Bradley D, Dudina A, Reiner Z. Dyslipidemias in the prevention of cardiovascular disease: risks and causality. Curr Cardiol Rep. 2012;14:709–20.
Najafipour H, Yousefzadeh G, Baneshi MR, Gohari MA, Shahouzehi B, Farokhi MS, et al. Prevalence and 5-year incidence rate of dyslipidemia and its association with other coronary artery disease risk factors in Iran: Results of the Kerman coronary artery disease risk factors study (Phase 2). J res med sci. 2021;26:99.
Iversen B, Jacobsen BK, Løchen M-L. Active and passive smoking and the risk of myocardial infarction in 24,968 men and women during 11 year of follow-up: the Tromsø Study. Eur J Epidemiol. 2013;28:659–67.
Najafipour H, Beik A. The impact of opium consumption on blood glucose, serum lipids and blood pressure, and related mechanisms. Front Physiol. 2016;7:436.
Yousefzadeh G, Shokoohi M, Najafipour H, Eslami M, Salehi F. Association between opium use and metabolic syndrome among an urban population in Southern Iran: Results of the Kerman Coronary Artery Disease Risk Factor Study (KERCADRS). ARYA atherosclerosis. 2015;11(1):14.
Wilson PW, D’Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med. 2002;162(16):1867–72.
Najafipour H, Yousefzadeh G, Forood A, Karamouzian M, Shadkam M, Mirzazadeh A. Overweight and obesity prevalence and its predictors in a general population: A community-based study in Kerman, Iran (Kerman coronary artery diseases risk factors studies). ARYA atherosclerosis. 2016;12(1):18.
Bagheri M, Najafipour H, Saberi S, Farokhi M, Amirzadeh R, Mirzazadeh A. Epidemiological update on prevalence and incidence of overweight and obesity in adults in Southeastern Iran: findings from KERCADRS. East Mediterranean Health J. 2021;27(9):874–83.
Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. The lancet. 2012;380(9838):219–29.
Najafipour H, Moazenzadeh M, Afshari M, Nasri HR, Khaksari M, Forood A, et al. The prevalence of low physical activity in an urban population and its relationship with other cardiovascular risk factors: Findings of a community-based study (KERCADRS) in southeast of Iran. ARYA atherosclerosis. 2016;12(5):212.
Li M, McCulloch B, McDermott R. Metabolic syndrome and incident coronary heart disease in Australian indigenous populations. Obesity. 2012;20(6):1308–12.
Najafipour H, Afshari M, Rostamzadeh F. Prevalence of multiple coronary artery disease risk factors in Kerman: A population-based study in southeast Iran. Iranian journal of medical sciences. 2018;43(2):140.
Ahmadi A, Shirani M, Khaledifar A, Hashemzadeh M, Solati K, Kheiri S, et al. Non-communicable diseases in the southwest of Iran: profile and baseline data from the Shahrekord PERSIAN Cohort Study. BMC Public Health. 2021;21(1):1–14.
Khan RMM, Chua ZJY, Tan JC, Yang Y, Liao Z, Zhao Y. From pre-diabetes to diabetes: diagnosis, treatments and translational research. Medicina. 2019;55(9):546.
Flack JM, Adekola B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc Med. 2020;30(3):160–4.
Franklin BA, Brinks J, Berra K, Lavie CJ, Gordon NF, Sperling LS. Using metabolic equivalents in clinical practice. Am J Cardiol. 2018;121(3):382–7.
Najafipour H, Kahnooji M, Baneshi MR, Yeganeh M, Gohari MA, Farokhi MS, et al. The prevalence and 5-year incidence rate of low physical activity in an urban population of 10,000 in southeastern Iran: relationship with other cardiovascular risk factors. J Phys Act Health. 2020;17(4):435–42.
Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9:1–13.
Eckel RH, Alberti KG, Grundy SM, Zimmet PZ. The metabolic syndrome. The lancet. 2010;375(9710):181–3.
Principles of epidemiology in public health practice. An introduction to applied epidemiology and biostatistics, 3rd ed. Lesson 3: Measures of risk. Atlanta: Centers for Disease Control and Prevention (CDC); 2006.
Mamudu HM, Paul TK, Wang L, Veeranki SP, Panchal HB, Alamian A, et al. The effects of multiple coronary artery disease risk factors on subclinical atherosclerosis in a rural population in the United States. Prev Med. 2016;88:140–6.
Yamada-Harada M, Fujihara K, Osawa T, Yamamoto M, Kaneko M, Kitazawa M, et al. Relationship between number of multiple risk factors and coronary artery disease risk with and without diabetes mellitus. J Clin Endocrinol Metab. 2019;104(11):5084–90.
Ahmadi B, Alimohammadian M, Yaseri M, Majidi A, Boreiri M, Islami F, et al. Multimorbidity: epidemiology and risk factors in the Golestan cohort study, Iran: a cross-sectional analysis. Medicine. 2016;95(7):e2756.
Farhang S, Faramarzi E, Amini Sani N, Poustchi H, Ostadrahimi A, Alizadeh BZ, et al. Cohort profile: The AZAR cohort, a health-oriented research model in areas of major environmental change in Central Asia. Int J Epidemiol. 2019;48(2):382-h.
Nejadghaderi SA, Ahmadi N, Rashidi M-M, Ghanbari A, Noori M, Abbasi-Kangevari M, et al. Physical activity pattern in Iran: Findings from STEPS 2021. Front Public Health. 2023;10:1036219.
Esteghamati A, Etemad K, Koohpayehzadeh J, Abbasi M, Meysamie A, Noshad S, et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005–2011. Diabetes Res Clin Pract. 2014;103(2):319–27.
Oori MJ, Mohammadi F, Norozi K, Fallahi-Khoshknab M, Ebadi A, Gheshlagh RG. Prevalence of HTN in Iran: meta-analysis of published studies in 2004–2018. Curr Hypertens Rev. 2019;15(2):113–22.
Varmaghani M, Sharifi F, Mehdipour P, Sheidaei A, Djalalinia S, Gohari K, et al. Prevalence of smoking among Iranian adults: findings of the national STEPs survey 2016. Arch Iran Med. 2020;23(6):369–77.
Najafipour H, Abdollahi F, Khatibi M, Amirzadeh R. Dietary status with demographic and anthropometric variables and some health affecting risk factors in people of Southeastern Iran: A population-based study (KERCADRS). Caspian J Intern Med. 2021;12(4):551.
Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? The lancet. 2012;380(9838):258–71.
Vincent HK, Lamb KM, Day TI, Tillman SM, Vincent KR, George SZ. Morbid obesity is associated with fear of movement and lower quality of life in patients with knee pain-related diagnoses. PM&R. 2010;2(8):713–22.
Creese H, Saxena S, Nicholls D, Sanchez AP, Hargreaves D. The role of dieting, happiness with appearance, self-esteem, and bullying in the relationship between mental health and body-mass index among UK adolescents: a longitudinal analysis of the Millennium Cohort Study. eClinicalMedicine. 2023;60(10036):101992.
Acknowledgements
The authors are grateful to the interviewers, physicians, and study participants for their valuable contributions and cooperation.
Funding
The Deputy of Research and Technology at Kerman University of Medical Sciences funded the study (grant No KMU.REC.1393/310).
Author information
Authors and Affiliations
Contributions
Nazanin. ZN. collected the data from KERCADRS. Nazanin. ZN. and Hamid. N. wrote the main manuscript text. Mitra. Sh. prepared tables and figures. Rashed. P. analyzed the collected data. All authors reviewed the manuscript and have approved the submitted version. All authors agreed to be personally accountable for their own contribution and ensure that all questions related to the accuracy or integrity of any part of the work are appropriately investigated, resolved, and the resolution documented in the literature.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent has been obtained from all participants in the KERCADR study. Ethics Committee of Kerman University of Medical Sciences approved the study (ethics code: IR.KMU.REC.1401.017).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zeinali-Nezhad, N., Najafipour, H., Shadkam, M. et al. Prevalence and trend of multiple coronary artery disease risk factors and their 5-year incidence rate among adult population of Kerman: results from KERCADR study. BMC Public Health 24, 25 (2024). https://doi.org/10.1186/s12889-023-17504-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-17504-8