
Abstract
Background
Epidemiological study of sex differences in incidence and risk factors of heart failure (HF), and subsequent mortality attributed to HF in the Chinese general population is lacking. This study aims to assess the sex differences in the incidence and risk factors of hospitalization for HF and evaluate the sex differences in population attributable fractions (PAFs) for the subsequent mortality among the general population.
Methods
Data were from a sub-cohort of the Patient-Centered Evaluative Assessment of Cardiac Events Million Persons Project in China. Fine and Gray models were conducted to calculate the hazard ratios (HRs) and 95% confidence intervals (CIs) accounting for the competing risk of all-cause mortality. Propensity score matching analysis and subgroup analyses were used to verify the robustness of the results. Adjusted PAFs of HF for all-cause and cardiovascular mortality were evaluated by sex.
Results
Of the 102,278 participants, 60.5% were women, and the mean age was 54.3 years. After a median follow-up of 3.52 years, 1588 cases of hospitalization for HF were identified. After adjusting for the covariates, women had 31% (95% CI: 0.61–0.79) lower risk for HF than men. The results were consistent in the propensity score matching cohort and across all subgroup analyses (all P sex-subgroups interaction > 0.05). Although women were associated with a lower risk of HF, they had a higher PAF (24.2%, 95% CI: 16.0-31.6) for subsequent cardiovascular mortality than men (16.5%, 95% CI: 11.3–21.5). Several significant differences in risk factors for HF were noted between sexes.
Conclusion
In the southern Chinese population, women had a lower risk of HF but had a higher cardiovascular mortality fraction attributed to HF than men. Sex-specific preventative strategies and management for HF should be warranted.
Similar content being viewed by others


Background
Striking sex differences in heart failure (HF) have been well-documented in Western countries, ranging from epidemiology and pathophysiological factors to therapeutic response and prognosis [1]. In Europe and the US, the prevalence of HF is fairly comparable between sexes [2,3,4], whereas women younger than 74 years of age have a significantly lower risk for incident HF than men [5]. Moreover, marked sex differences in risk factors, such as diabetes mellitus (DM) [6,7,8], hypertension [9], socioeconomic status (SES) [10, 11], tobacco smoking and alcohol consumption [12], for HF have also been well-described in western populations.
Epidemiologic studies of HF between sexes are relatively limited in Asia [13], especially in China. To date, only one previous study showed a similar weighted prevalence of HF among Chinese men and women (men versus women: 1.4% versus 1.2%) [14], and the sex difference in HF-related hospitalization in China is still unknown. Furthermore, sex differences in risk factors for HF and subsequent mortality attributed to HF in the Chinese population remain inconclusive [15]. Against the background of the high prevalence and heavy burden of HF in China [16], better clarifications of sex differences in incidence and risk factors of HF, and subsequent mortality due to HF are immediately needed, thus promoting sex-specific prevention and treatment strategies for HF.
Accordingly, leveraging a prospective sub-cohort of the China Patient-Centered Evaluative Assessment of Cardiac Events (PEACE) Million Persons Project, we aimed to (1) assess the sex differences in the incidence and risk factors of hospitalization for HF, and (2) evaluate the sex differences in population attributable fractions (PAFs) for the subsequent mortality among the Chinese general population.
Materials and methods
Study design and participant
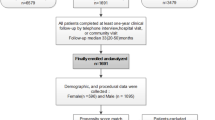
The China PEACE Million Persons Project details have been described elsewhere [17, 18]. Briefly, this project is a nationwide, community-based cardiovascular disease (CVD) screening study that is aimed at identifying high CVD-risk individuals. Our current study was conducted in a sub-cohort of the China PEACE Million Persons Project, including 102,358 participants who were enrolled in 8 sites from Guangdong Province (Southern China) between January 2016 and December 2020. At each site, eligible participants aged 35 to 75 years with local residence registration were recruited by local staff after written informed consent was obtained. In the present study, we excluded 80 individuals with prevalent HF, and a total of 102,278 subjects were finally included.
Data collection and variables
Information on sociodemographic characteristics (sex, age, resident area, married status, smoking and drinking status, education, occupation, annual household income, health insurance) and comorbid conditions (hypertension, DM, dyslipidemia, coronary artery disease (CAD), coronary revascularization, stroke, chronic obstructive pulmonary disease (COPD)) were collected by trained medical staff during face-to-face interviews. Each participant then received a physical examination to measure blood pressure, height, weight, and waist circumference using standard protocols. Seated blood pressure and pulse were measured on the participants’ right arm using an electronic blood pressure monitor (Omron HEM-7430; Omron Corporation, Kyoto, Japan) after 5 min of rest. Each subject’s blood pressure and pulse were measured twice at a 1-minute interval, and the mean value of 2 measurements was used. Height, weight, and waist circumference were measured by trained technicians, and individuals were required to wear light clothes without shoes and a cap. Body mass index (BMI) was calculated by dividing the weight in kilograms by the square of height in meters. Fingertip blood samples were used to test lipid profile (CardioChek PA Analyzer; Polymer Technology Systems, Indianapolis, Indiana, USA) and fasting blood glucose (FBG) (BeneCheck BK6–20 M MultiMonitoring System, Suzhou Pu Chun Tang Biotechnology, China).
Study outcome
The primary outcome of the current study was hospitalization for HF. Using the code of the Tenth Revision of the International Classification of Diseases (ICD-10) [19], participants’ HF-related hospitalization (I50) records were reviewed and identified from the Inpatients Registry by trained staff who were blinded to their baseline characteristics. HF was ascertained based on the presence of symptoms or signs (e.g., dyspnea, jugular vein distention, ankle swelling), the elevation of natriuretic peptide level, and the abnormality of cardiac function or structure on echocardiography. Finally, a panel of experienced experts consisting of 2 cardiologists and 1 statistician independently verified and ascertained all HF events. In addition, we calculated the PAFs for subsequent all-cause mortality and cardiovascular (CV) mortality due to HF among men and women. The events of death were collected from the China’s Centre for Disease Prevention and Control’s National Mortality Surveillance System and Vital Registration, and the ICD-10 was also used to code the all-cause and CV mortality records (I00-I99). The date of HF-related hospitalization, the death date, or the last follow-up date (December 31, 2021) was used to calculate the follow-up time, whichever came first.
Statistical analysis
Continuous and categorical variables were presented as mean ± standard deviation (SD) and number (proportion) respectively. Differences in the baseline characteristics of participants between sexes were tested using Student’s t-test and χ2 test, accordingly. The Fine and Gray estimator was conducted to compute cumulative incidence curves for HF-related hospitalization and all-cause mortality before hospitalization for HF as a competing risk, and hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated with adjustment for demographic and socioeconomic information, including age, smoking and drinking status, residential area, education, annual household income, and insurance (Model 1); Model 1 plus physical examination and laboratory, including systolic blood pressure (SBP), pulse, BMI, waist circumference, lipid profiles, and FBG (Model 2); Model 2 plus comorbidities, including hypertension, DM, dyslipidemia, CAD, coronary revascularization, stroke, and COPD (Model 3). Multiple imputations by chained equations with 20 imputations were used to fill in the missing values (< 1%). Several subgroup analyses were conducted and the sex-by-subgroup interactions were tested in Fine and Gray models based on likelihood ratio tests. Seven subgroups, including age (< 60 and ≥ 60 years), residential area (urban and rural), smoking status (current and non-current), education attainment (< high school and ≥ high school), annual household income (< 50,000 and ≥ 50,000 China Yuan), hypertension (yes and no), and DM (yes and no), were selected based on the following criteria: (1) A certain number of participants in each group; (2) Potential effect modifiers of the association between sex with hospitalization for HF.
To verify the robustness of the results, a 1:1 ratio propensity-matched analysis with a caliper value of 0.01 was performed. All 26 variables presented in Table 1 were selected for the propensity model to ensure the comparability of baseline characteristics between sexes. The propensity to men versus women was predicted by the multivariable logistic regression model, and post-estimations for propensity score-matched were evaluated by standardized bias and propensity score density [20]. Individuals were matched to the nearest available propensity score without replacement, and the procedure was repeated until all male participants were matched. The Fine and Gray models were then conducted in the propensity score-matched cohort.
To detect the risk factors for HF-related hospitalization among men and women, multivariate Cox regression analyses were performed between sexes, and the sex-by-factor interactions were also tested. To compute the PAFs for the subsequent all-cause and CV mortality attributed to HF, the ‘punaf’ command in STATA software was employed with further adjustment for the identical covariables included in the Fine and Gray model. This command implements the method for estimating PAFs for cross-section and cohort studies as recommended by Greenland S and Drescher K [21].
All analyses were performed using Stata MP version 17.1 (StataCorp LLC, College Station, TX, USA). Two-sided p-values < 0.05 were considered statistically significant.
Results
Baseline characteristics of participants
A total of 102,278 participants were enrolled, and 60.5% were women. The mean age was 54.3 years old, and the most prevalent comorbidity was hypertension (22.7%), followed by DM (7.6%) and dyslipidemia (5.6%). Compared with men, women were younger and less likely to smoke and drink and had lower SES (i.e., women had lower educational levels, lower annual household income, and were less likely to have health insurance). By contrast, men had higher comorbid burdens compared to women. (Table 1)
The baseline characteristics of participants with and without hospitalization for HF were also presented in Supplemental Table 1. Briefly, compared with individuals without HF-related hospitalization, those with HF were older and more likely to be smokers, had lower SES, had higher levels of baseline blood pressure and pulse, were more obese, and had higher comorbid burdens.
Sex differences in hospitalization for heart failure
After a median follow-up of 3.52 years (343,758 person-years), 1588 cases of hospitalization for HF (4.62 (95% CI: 4.40–4.85) per 1000 person-year) were identified. The incidence rate for men and women was 6.37 (95% CI: 5.95–6.80) and 3.49 (95% CI: 3.24–3.75) per 1000 person-year, respectively (p for incidence rate comparison < 0.001). The cumulative rate of HF-related hospitalization was lower in women than in men (Fig. 1 Panel A), with an adjusted HR of 0.69 (95% CI: 0.61–0.79). (Table 2)

Cumulative Incidence Curves of Hospitalization for Heart failure in Overall (A) and Propensity Scores Matched (B) Cohort. HF, heart failure, HR, hazard ratio
Due to the significant differences in baseline characteristics between sexes, we performed the propensity-matched analysis. We matched 17,075 men to women in a 1:1 ratio, and the differences and the standardized bias significantly reduced between groups after propensity matching. (Supplemental Figs. 1 and 2, Supplemental Table 2) The lower risk of hospitalization for HF observed in women remained consistent in the propensity matching analysis (HR: 0.72, 95% CI: 0.61–0.86). (Fig. 1 Panel B, Table 2)
In the several subgroup analyses, including age (higher or lower than 60 years old), residence area (urban or rural), smoking status (current or non-current), education attainment (higher or lower than high school), annual household income (higher or lower than 50,000 Chinese Yuan), hypertension (yes or no), and DM (yes or no), women consistently had a lower risk of HF in comparison with men (all p-interaction > 0.05). (Fig. 2)

Subgroup analyses. CNY, China Yuan
Sex differences in risk factors for heart failure
SBP, pulse, waist circumference, hypertension, DM, CAD, COPD, and FBG were the significant independent risk factors for HF in both men and women. Among these risk factors, higher age, waist circumference, and triglyceride had a more pronounced impact on HF development in women than in men (p for sex-factor interactions < 0.05). Additionally, urban residence, higher annual household income, and prevalent stroke were also associated with a higher risk of HF in women. (Table 3)
Sex difference in population attributable fraction for mortality attributed to heart failure
The overall PAFs for subsequent all-cause mortality and CV mortality attributed to HF were 15.1% (95% CI: 13.7–17.0) and 19.3% (95% CI: 14.9–23.4), respectively. Specifically, the PAFs for all-cause mortality were comparable between men (14.7%, 95% CI: 12.2–17.1) and women (15.3%, 9%% CI: 12.2–18.3), while the PAF for CV mortality was higher in women (24.2%, 95% CI: 16.0-31.6) than in men (16.5%, 95% CI: 11.3–21.5). (Fig. 3)

Population Attributable Fraction of Heart Failure for All-cause and Cardiovascular Death Stratified by Sex
Discussion
In this large, prospective, population-based cohort study, women had a lower risk of hospitalization for HF than men, and the results remained consistent in the conventional risk factors that were adjusted, in the propensity-matched analysis as well as in the subgroup analyses. Majorities of modifiable risk factors were associated with HF both in men and women, several sex differences in risk factors (e.g., age, waist circumference) were also found. Although female sex was associated with a lower HF risk, women had a higher PAF for subsequent CV mortality than men.
Sex differences in the incidence of HF have been well-documented in Western countries. A recent study including over 70,000 Europeans from 4 community-based cohorts found women had a lower risk for incident HF than men, with fewer HF cases noted in women (5.9%) than in men (7.3%) after a median follow-up of 12.7 years [22]. Another pooled study consisting of 12,417 community-dwelling adults from the U.S. also showed a higher lifetime risk for HF in men (27.4%) than in women (23.8%) [23]. Interestingly, more and more studies demonstrated that men developed HF earlier than women in middle-aged (< 75 years) whereas women had a higher incidence rate of HF in old-aged [5, 24]. However, little evidence exists regarding the sex difference in hospitalization for HF in China. Our current study is the first to describe the incidence of HF-related hospitalization by sexes in southern China. Consistent with the prior studies from Western countries, our study showed a lower risk for HF was observed in women aged 35 to 75 years, and the conclusion remained robust in the propensity-matched analysis, suggesting intensive and improved preventative strategies should be warranted in middle-aged men.
In line with previous studies [12, 25], the majority of conventional risk factors were related to HF-related hospitalization in both sexes in the present study, including age, lower education attainment, higher levels of SBP, resting pulse, and waist circumference, hypertension, DM, CAD, and COPD. Of note, advanced age had a more pronounced impact on HF development in women than men, and this could be a reasonable explanation for why women have a higher incidence rate of HF than men in older age [5], indicating improved management of CV health should be considered in elderly women. In addition to age, women with greater waist circumference were predisposed to HF compared to men. A previous study also showed that obese women harbored a greater risk of future HF than men, especially in HF with preserved ejection fraction (HFpEF) [7], and the underlying mechanism may be due to the differential effect of abdominal obesity on longitudinal changes in left ventricular mass among women than men [26]. All in all, the current study demonstrated that the majority of modifiable risk factors tended to have more pronounced impacts on HF in women than men, although women had a lower risk of HF development.
Another previous study from the Western population demonstrated the differential association between SBP [22] and DM [12] with incident HF among men and women. In contrast to these studies, the current study showed that SBP, hypertension, and DM portended similar risks of HF between sexes in the Chinese general population. The difference might be mainly due to the distinct races enrolled in each study, and further studies including different racial groups are warranted to investigate the sex differences in risk factors for HF development. Nevertheless, immediate efforts are needed to ease the burden of the high incidence of HF in China [16] by emphasizing the management and prevention of chronic diseases (i.e., hypertension, DM, CAD).
Sex differences in mortality risk after incident HF are complicated and mixed. In the Framingham Heart Study (FHS) from 1990 to 1999, men with HF (59%) were associated with a higher 5-year all-cause mortality risk than their female counterparts (45%) [27]. By contrast, in the Olmsted County study from 2000 to 2010, the age-adjusted all-cause mortality risk was comparable between men and women (men vs. women: HR: 1.09, 95% CI: 0.99–1.20), whereas the lower CV mortality rate was noted in women (men vs. women: HR: 1.19, 95% CI: 1.03–1.37) [28]. In a study consisting of Asian individuals, women with acute HF had a 14% (95% CI: 0.79–0.94) lower mortality risk than men at 1-year follow-up [29]. Nevertheless, another study from the ASIAN-HF cohort showed that women with HF with reduced heart failure (HFrEF) patients and DM had a higher risk of 1-year all-cause mortality and HF hospitalization than men [30]. Our current study supports and extends the prior findings. In the general population, although female sex was associated with a lower risk of hospitalization for HF, women had a similar PAF for subsequent all-cause mortality and significantly higher PAF for subsequent CV mortality than men, indicating a worse prognosis in women with HF. The poor outcomes observed in women might be the consequence of the huge sex gap in standardized therapy of CV diseases [31,32,33,34]. More attention should be paid to female HF patients for the prevention of mortality.
Understanding the sex differences in risk factors for HF and subsequent mortality has significant public health implications for cardiovascular health promotion. First, most conventional risk factors were significantly associated with HF in both sexes, underlining the early intervention of these risk factors is of great significance to HF prevention at the population level. Second, an urgent call to action is needed to promote CV health in elderly women, not only the higher incidence of HF among older women [5, 24] but also the worse life quality observed in female HF patients [35]. Third, the majority of modifiable harbored a hazardous impact on hospitalization for HF in women than men, highlighting that primary care physicians should pay more attention to improving the management of common and conventional risk factors for women. Fourth, lower SES (i.e., rural residence, lower annual household income) has a stronger strength of association with female CV health than males. Nevertheless, gender inequality consistently exists and women always tend to have a poor SES, resulting in under-management of CVDs [31] as well as under-recognition of cardiovascular risk factors [36], eventually leading to a poor prognosis among women. Therefore, our study underscores the improvement of female SES, which might be a potential approach and an extremely important step to promote the CV health of women.
Limitations
The present study has several noteworthy limitations. First, the current study was conducted in a sub-cohort of the China PEACE Million Persons Project from southern China, and the results should be extrapolated with caution to other regions with different lifestyles and genetic backgrounds. Second, due to the observational nature, unmeasured and missing confounding factors may still exist and influence the current results, such as the important laboratory indicators relative to cardiac injury and function, although we have adjusted for multiple conventional covariates and conducted the propensity-matched analysis. Third, the China PEACE Million Persons Project only performs echocardiography with high-CVD risk individuals, we cannot classify HF subtypes based on left ventricular ejection fraction (LVEF). Because patients with HFpEF are often undetected, particularly in the outpatient [37], and because women are susceptible to HFpEF [38], an underdiagnosis of HFpEF in women might be possible. Nevertheless, HF as an endpoint obtained from administrative registers has been demonstrated can be used in a cohort study with high specificity [39]. Fourth, given the epidemiologic nature of the current study, the underlying pathophysiological mechanisms of the sex differences in HF and risk factors cannot be fully explained.
Future research
Future research could analyze the sex disparities in the incidence and risk factors of different HF subtypes according to LVEF (i.e., HFrEF, heart failure with mildly reduced LVEF, and HFpEF) using the nationally represented population. In addition, sex differences in mortality among Western HF patients have been reported [38], however, sex differences in prognosis of HF are still inconclusive and remain to be elucidated. What’s more, comparisons of the above sex differences between different regional and racial groups need to be considered, as significant regional and ethical differences in HF have been recently recorded [40, 41]. Lastly, as mentioned above, the underlying mechanisms of the sex differences in HF cannot be completely explained due to the observational and epidemiologic nature of the present study, which merits further study.
Conclusions
Our large, population-based data provide evidence showing that female sex was associated with a lower risk of HF than men in the general population from southern China, and the results remained consistent in the propensity-matched analysis and across all the subgroups. Majorities of conventional risk factors were related to HF development in both sexes, whereas several significant sex differences in modifiable risk factors for HF were also noted, suggesting sex-specific preventative strategies for HF should be warranted. Although female sex was associated with a lower risk of HF-related hospitalization, women had a similar PAF for subsequent all-cause mortality and significantly higher PAF for subsequent CV mortality than men, indicating more attention should be paid to female HF patients for standardized management.
Data Availability
The deidentified participant data will be shared on a request basis. Please directly contact the corresponding author to request data sharing.
Abbreviations
- HF:
-
heart failure
- DM:
-
diabetes mellitus
- SES:
-
socioeconomic status
- PEACE:
-
Patient-Centered Evaluative Assessment of Cardiac Events
- PAF:
-
population attributable fraction
- CVD:
-
cardiovascular disease
- CAD:
-
coronary artery disease
- COPD:
-
chronic obstructive pulmonary disease
- BMI:
-
body mass index
- FBG:
-
fasting blood glucose
- ICD-10:
-
the Tenth Revision of International Classification of Diseases
- CV:
-
cardiovascular
- SD:
-
standard deviation
- HR:
-
hazard ratio
- CI:
-
confidence interval
- SBP:
-
systolic blood pressure
- HFpEF:
-
heart failure with preserved ejection fraction
- FHS:
-
Framingham Heart Study
- HFrEF:
-
heart failure with reduced heart failure
References
Lam CSP, Arnott C, Beale AL, Chandramouli C, Hilfiker-Kleiner D, Kaye DM, Ky B, Santema BT, Sliwa K, Voors AA. Sex differences in Heart Failure. Eur Heart J. 2019;40(47):3859–3868c.
Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, et al. Heart Disease and Stroke Statistics-2020 update: a Report from the American Heart Association. Circulation. 2020;141(9):e139–e596.
Störk S, Handrock R, Jacob J, Walker J, Calado F, Lahoz R, Hupfer S, Klebs S. Epidemiology of Heart Failure in Germany: a retrospective database study. Clin Res Cardiology: Official J German Cardiac Soc. 2017;106(11):913–22.
Smeets M, Vaes B, Mamouris P, Van Den Akker M, Van Pottelbergh G, Goderis G, Janssens S, Aertgeerts B, Henrard S. Burden of Heart Failure in flemish general practices: a registry-based study in the Intego database. BMJ open. 2019;9(1):e022972.
Christiansen MN, Køber L, Weeke P, Vasan RS, Jeppesen JL, Smith JG, Gislason GH, Torp-Pedersen C, Andersson C. Age-Specific trends in Incidence, Mortality, and comorbidities of Heart Failure in Denmark, 1995 to 2012. Circulation. 2017;135(13):1214–23.
Ohkuma T, Komorita Y, Peters SAE, Woodward M. Diabetes as a risk factor for Heart Failure in women and men: a systematic review and meta-analysis of 47 cohorts including 12 million individuals. Diabetologia. 2019;62(9):1550–60.
Savji N, Meijers WC, Bartz TM, Bhambhani V, Cushman M, Nayor M, Kizer JR, Sarma A, Blaha MJ, Gansevoort RT, et al. The Association of Obesity and cardiometabolic traits with Incident HFpEF and HFrEF. JACC Heart Failure. 2018;6(8):701–9.
Eaton CB, Pettinger M, Rossouw J, Martin LW, Foraker R, Quddus A, Liu S, Wampler NS, Hank Wu WC, Manson JE et al. Risk factors for Incident Hospitalized Heart Failure with preserved Versus reduced ejection fraction in a Multiracial Cohort of Postmenopausal Women. Circulation Heart Failure 2016, 9(10).
Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK. The progression from Hypertension to Congestive Heart Failure. JAMA. 1996;275(20):1557–62.
Averbuch T, Mohamed MO, Islam S, Defilippis EM, Breathett K, Alkhouli MA, Michos ED, Martin GP, Kontopantelis E, Mamas MA, et al. The Association between Socioeconomic Status, Sex, race / ethnicity and In-Hospital mortality among patients hospitalized for Heart Failure. J Card Fail. 2022;28(5):697–709.
Dewan P, Rørth R, Jhund PS, Ferreira JP, Zannad F, Shen L, Køber L, Abraham WT, Desai AS, Dickstein K, et al. Income inequality and outcomes in Heart Failure: A Global between-country analysis. JACC Heart Failure. 2019;7(4):336–46.
Sillars A, Ho FK, Pell GP, Gill JMR, Sattar N, Gray S, Celis-Morales C. Sex differences in the association of risk factors for Heart Failure incidence and mortality. Heart. 2020;106(3):203–12.
Shimokawa H, Miura M, Nochioka K, Sakata Y. Heart Failure as a general pandemic in Asia. Eur J Heart Fail. 2015;17(9):884–92.
Hao G, Wang X, Chen Z, Zhang L, Zhang Y, Wei B, Zheng C, Kang Y, Jiang L, Zhu Z, et al. Prevalence of Heart Failure and left ventricular dysfunction in China: the China Hypertension Survey, 2012–2015. Eur J Heart Fail. 2019;21(11):1329–37.
Qiu W, Cai A, Li L, Feng Y. Lagging behind the western countries: the knowledge gaps of gender differences in Heart Failure in Asia. ESC Heart Failure. 2023;10(5):2797–806.
Zhang Y, Zhang J, Butler J, Yang X, Xie P, Guo D, Wei T, Yu J, Wu Z, Gao Y, et al. Contemporary Epidemiology, management, and outcomes of patients hospitalized for Heart Failure in China: results from the China Heart Failure (China-HF) Registry. J Card Fail. 2017;23(12):868–75.
Li X, Wu C, Lu J, Chen B, Li Y, Yang Y, Hu S, Li J. Cardiovascular risk factors in China: a nationwide population-based cohort study. The Lancet Public Health. 2020;5(12):e672–81.
Lu J, Xuan S, Downing NS, Wu C, Li L, Krumholz HM, Jiang L. Protocol for the China PEACE (patient-centered evaluative Assessment of Cardiac events) million persons Project pilot. BMJ open. 2016;6(1):e010200.
Sattar N, Rawshani A, Franzén S, Rawshani A, Svensson AM, Rosengren A, McGuire DK, Eliasson B, Gudbjörnsdottir S. Age at diagnosis of type 2 Diabetes Mellitus and associations with Cardiovascular and Mortality risks. Circulation. 2019;139(19):2228–37.
Brookhart MA, Wyss R, Layton JB, Stürmer T. Propensity score methods for confounding control in nonexperimental research. Circulation Cardiovasc Qual Outcomes. 2013;6(5):604–11.
Greenland S, Drescher K. Maximum likelihood estimation of the attributable fraction from logistic models. Biometrics. 1993;49(3):865–72.
Magnussen C, Niiranen TJ, Ojeda FM, Gianfagna F, Blankenberg S, Vartiainen E, Sans S, Pasterkamp G, Hughes M, Costanzo S, et al. Sex-specific epidemiology of Heart Failure risk and mortality in Europe: results from the BiomarCaRE Consortium. JACC: Heart Failure. 2019;7(3):204–13.
Pandey A, Omar W, Ayers C, LaMonte M, Klein L, Allen NB, Kuller LH, Greenland P, Eaton CB, Gottdiener JS, et al. Sex and race differences in lifetime risk of Heart Failure with preserved ejection fraction and Heart Failure with reduced ejection fraction. Circulation. 2018;137(17):1814–23.
Meyer S, Brouwers FP, Voors AA, Hillege HL, de Boer RA, Gansevoort RT, van der Harst P, Rienstra M, van Gelder IC, van Veldhuisen DJ, et al. Sex differences in new-onset Heart Failure. Clin Res Cardiology: Official J German Cardiac Soc. 2015;104(4):342–50.
Yusuf S, Rangarajan S, Teo K, Islam S, Li W, Liu L, Bo J, Lou Q, Lu F, Liu T, et al. Cardiovascular risk and events in 17 low-, middle-, and high-income countries. N Engl J Med. 2014;371(9):818–27.
Lieb W, Xanthakis V, Sullivan LM, Aragam J, Pencina MJ, Larson MG, Benjamin EJ, Vasan RS. Longitudinal tracking of left ventricular mass over the adult life course: clinical correlates of short- and long-term change in the framingham offspring study. Circulation. 2009;119(24):3085–92.
Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with Heart Failure. N Engl J Med. 2002;347(18):1397–402.
Gerber Y, Weston SA, Redfield MM, Chamberlain AM, Manemann SM, Jiang R, Killian JM, Roger VL. A contemporary appraisal of the Heart Failure epidemic in Olmsted County, Minnesota, 2000 to 2010. JAMA Intern Med. 2015;175(6):996–1004.
Motiejūnaitė J, Akiyama E, Cohen-Solal A, Maggioni AP, Mueller C, Choi DJ, Kavoliūnienė A, Čelutkienė J, Parenica J, Lassus J, et al. The association of long-term outcome and biological sex in patients with acute Heart Failure from different geographic regions. Eur Heart J. 2020;41(13):1357–64.
Chandramouli C, Teng TK, Tay WT, Yap J, MacDonald MR, Tromp J, Yan L, Siswanto B, Reyes EB, Ngarmukos T, et al. Impact of Diabetes and sex in Heart Failure with reduced ejection fraction patients from the ASIAN-HF registry. Eur J Heart Fail. 2019;21(3):297–307.
Ezekowitz JA, Savu A, Welsh RC, McAlister FA, Goodman SG, Kaul P. Is there a sex gap in surviving an Acute Coronary syndrome or subsequent development of Heart Failure? Circulation. 2020;142(23):2231–9.
Hsich EM. Sex differences in Advanced Heart Failure therapies. Circulation. 2019;139(8):1080–93.
Bucholz EM, Butala NM, Rathore SS, Dreyer RP, Lansky AJ, Krumholz HM. Sex differences in long-term mortality after Myocardial Infarction: a systematic review. Circulation. 2014;130(9):757–67.
Chang WC, Kaul P, Westerhout CM, Graham MM, Fu Y, Chowdhury T, Armstrong PW. Impact of sex on long-term mortality from acute Myocardial Infarction vs unstable angina. Arch Intern Med. 2003;163(20):2476–84.
Truby L, O’Connor C, Fiuzat M, Stebbins A, Coles A, Patel C, Granger B, Pagidipati N, Agarwal R, Rymer J, et al. Sex differences in quality of life and clinical outcomes in patients with Advanced Heart Failure: insights from the PAL-HF trial. Circulation Heart Failure. 2020;13(4):e006134.
Rodriguez F. Sex disparities in Prevention of Atherosclerotic Cardiovascular Disease across the Life Course. Circulation. 2023;147(7):523–5.
van Riet EE, Hoes AW, Limburg A, Landman MA, van der Hoeven H, Rutten FH. Prevalence of unrecognized Heart Failure in older persons with shortness of breath on exertion. Eur J Heart Fail. 2014;16(7):772–7.
Stolfo D, Uijl A, Vedin O, Strömberg A, Faxén UL, Rosano GMC, Sinagra G, Dahlström U, Savarese G. Sex-based differences in Heart Failure across the Ejection Fraction Spectrum: phenotyping, and prognostic and therapeutic implications. JACC Heart Failure. 2019;7(6):505–15.
Mähönen M, Jula A, Harald K, Antikainen R, Tuomilehto J, Zeller T, Blankenberg S, Salomaa V. The validity of Heart Failure diagnoses obtained from administrative registers. Eur J Prev Cardiol. 2013;20(2):254–9.
Lam CS, Teng TK, Tay WT, Anand I, Zhang S, Shimizu W, Narasimhan C, Park SW, Yu CM, Ngarmukos T, et al. Regional and ethnic differences among patients with Heart Failure in Asia: the Asian Sudden Cardiac Death in Heart Failure registry. Eur Heart J. 2016;37(41):3141–53.
Tromp J, Claggett BL, Liu J, Jackson AM, Jhund PS, Køber L, Widimský J, Boytsov SA, Chopra VK, Anand IS, et al. Global differences in Heart Failure with preserved ejection fraction: the PARAGON-HF trial. Circulation Heart Failure. 2021;14(4):e007901.
Funding
This current review was supported by the Climbing Plan of Guangdong Provincial People’s Hospital (DFJH2020022), Guangdong Provincial Clinical Research Center for Cardiovascular disease (2020B111117011), Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention (2017B030314041), and the Key Area R&D Program of Guangdong Province (No.2019B020227005).
Author information
Authors and Affiliations
Contributions
Q.W.D contributed to the data acquisition, analysis and drafted the manuscript. A.P.C provided study concept and design, and revised the manuscript. Z.Q.N contributed to the data acquisition and analysis. J.B.W contributed to the data acquisition. Y.Q.O contributed to funding obtained and provide administrative, technical, or material support. Y.Q.F contributed to funding obtained and provide administrative, technical, or material support. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Guangzhou Provincial People’s Hospital (No. GDREC2016438H(R2)). All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Qiu, W., Cai, A., Nie, Z. et al. Sex difference in incidence and risk factors of hospitalization for heart failure, and subsequent mortality: findings from the China PEACE million persons project. BMC Public Health 23, 2356 (2023). https://doi.org/10.1186/s12889-023-17286-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-17286-z