
Abstract
Background
The decline in physical activity (PA) during adolescence is well-established. However, while some subgroups of adolescents follow the general pattern of decreased activity, others increase or maintain high or low activity. The correlates and determinants of different PA patterns may vary, offering valuable information for targeted health promotion. This study aimed to examine how psychosocial factors, health behaviours, and PA domains are associated with longitudinal PA patterns from adolescence to young adulthood.
Methods
This prospective study encompassed 254 participants measured at mean ages 15 and 19. Device-measured moderate-to-vigorous PA was grouped into five patterns (activity maintainers, inactivity maintainers, decreasers from moderate to low PA, decreasers from high to moderate PA, increasers) via a data-driven method, K-Means for longitudinal data. Multinomial logistic regression was used to analyse the associations between health behaviours, psychosocial factors, PA domains, and different PA patterns.
Results
A lack of sports club participation characterised inactivity maintainers throughout adolescence. Difficulties in communicating with one’s father at age 15 were associated with higher odds of belonging to inactivity maintainers and to decreasers from moderate to low PA. Lower fruit and vegetable consumption at age 19 was also related to increased odds of belonging to the groups of inactivity maintainers and decreasers from moderate to low PA. Smoking at age 19 was associated with being a decreaser from moderate to low PA.
Conclusions
Diverse factors characterise longitudinal PA patterns over the transition to young adulthood. Sports club participation contributes to maintained PA. Moreover, a father-adolescent relationship that supports open communication may be one determinant for sustained PA during adolescence. A healthier diet and non-smoking as a young adult are associated with more favourable PA development.
Similar content being viewed by others

Background
The decline in physical activity (PA) during adolescence is a global health concern [1]. Overall, PA tends to decline with increasing age [2, 3], such that as compared to younger age groups [1], more adolescents fail to meet the one-hour moderate-to-vigorous PA (MVPA) per day recommendation [4]. However, despite the overall decline in PA, considerable individual variation exists in the development of PA over adolescent years – a point illustrated by studies identifying distinct longitudinal PA patterns or trajectories [5,6,7,8,9]. There is a need for studies to determine how those adolescents who maintain favourable PA differ from those who decrease their activity, or those who maintain an inactive lifestyle. Such research would open up possibilities to guide PA interventions [2, 5, 6, 10].
PA is a complex behaviour, varying over time. Numerous theories and models have been applied to shed light on it. One of these, the (socio)ecological model, is based on the idea that PA may be influenced by (1) individual (e.g. genetic or psychological) factors, (2) social or cultural factors, (3) the built environment, and (4) policies [11, 12]. Thus, the determinants and correlates of longitudinal PA patterns may exist at many levels. Moreover, the contexts of living and of PA change over the life course [13,14,15], and this further increases the possible correlates for sustained and changed PA. The transition to young adulthood typically involves increasing autonomy. This is frequently linked to important changes (such as moving out of the childhood family home, or entering higher education or employment) that may predispose individuals to changing their health behaviours. As well as acknowledging the changes in environments and the impacts of life events during the lifespan, the life course approach considers the impact of earlier life phases on subsequent phases, and assumes that there may be ideal times for intervening in health behaviours [16,17,18].
A number of possible correlates/determinants for longitudinal PA patterns during adolescence have previously been examined, including maturity [7, 19, 20], socioeconomic status [21], other health behaviours [19, 20], support for PA [20, 21], PA domains [5], and distance to the nearest park and school [20]. However, the research base is still limited, and apart from family and peer support for PA, the psychosocial factors correlating with PA patterns have received little attention. Moreover, for the most part, only a single health behaviour has been studied in relation to longitudinal PA patterns [6, 20], even if there would be reason to examine the possible accumulation of behavioural risk and/or protective factors in relation to longitudinal PA patterns. Overall, information on the co-occurring and multidimensional characteristics of longitudinal PA patterns could be valuable for health promotion, one aim of which is to increase or maintain physical activity during adolescence.
Another limitation in previous research is that only some studies have used accelerometry in PA assessment rather than self-reported measurements; furthermore, the majority of studies have not applied data-driven methods for identifying distinct PA patterns. Data-driven methods can better identify genuinely heterogeneous PA patterns as compared to subjective methods (which can involve splitting into quartiles, or applying predetermined levels of PA).
Our aim was to study how psychosocial factors (loneliness, weight satisfaction, ease in talking to parents, exercise with parents) and health behaviours (alcohol, tobacco, and snuff use, amount of sleep, eating behaviours, toothbrushing) are associated with longitudinal PA patterns from adolescence to young adulthood (referring here to the patterns represented by activity maintainers, inactivity maintainers, decreasers from moderate to low PA, decreasers from high to moderate PA, and increasers [5]). Moreover, the associations between activity domains and PA patterns were examined together with psychosocial factors and health behaviour, the aim being to assess the most important correlates for sustained and changed PA during the transition to young adulthood. In previous analyses using the same study data, changes in sports club participation have emerged as significantly related to maintained and decreased PA, and passive commuting throughout adolescence has been found to be related to maintained inactivity [5]. Thus, we hypothesised that when analysed together with the other studied factors, we would find participation in a sports club to be related to maintained or increased PA, and passive commuting to maintained inactivity. Moreover, we hypothesised that (1) decreasing PA to a low level, and (2) maintained inactivity, would be associated with at least some health-compromising behaviours and psychosocial challenges.
Methods
Participants and study procedure
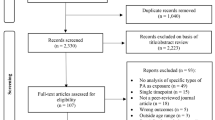
The data for this observational cohort study were drawn from the Health Promoting Sports Club study (HPSC), conducted in the years 2013–2014 and 2017–2018. At baseline, the participants (mean age 15) were recruited on the basis of power calculations [22] from 156 sports clubs and 100 schools within six large cities and surrounding communities in different parts of Finland [5, 20].
The procedure was the same at baseline and follow-up. Hence, the participants took part in electronic surveys on current health status and behaviours, and participated in medical examinations containing screening by a physician, a fasting blood sample, and instructions to use a hip-worn accelerometer (seven consecutive days during waking hours, except when bathing or doing water activities).
Nearly two thirds (64%) of the baseline participants (n = 583, mean age 15.5, SD 0.6), also took part in follow-up measurements (n = 371, mean age 19.4, SD 0.6). In total, 254 adolescents (60% females) provided valid accelerometry data for both measurements (swimmers excluded: n = 22, at least four days, 10 h/day). See [5, 20] for more study details.
Measures
Outcomes (longitudinal PA patterns)
PA was measured via a Hookie accelerometer (AM20 Activity Meter, Hookie Technologies Ltd., Helsinki, Finland), which collected and stored tri-axial data as actual g-units (100 Hz sampling frequency). The data were analysed in units of 6 seconds’ duration. The PA analysis was based on mean amplitude deviation analyses (MAD), calculated from a resultant tri-axial raw acceleration signal, and converted to metabolic equivalents (METs) [23, 24]. The epoch-wise MET values were further smoothed by calculating the 1-minute exponential moving average MET value for each epoch time point. MVPA was defined as ≥ 3.0 METs.
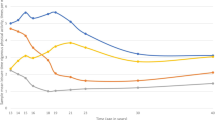
The formulation and details of the longitudinal PA patterns have been described previously [5]. In brief, by applying k-means for longitudinal data (KmL) [25] based on the two MVPA measurement periods, the participants were grouped into distinct clusters so that the clusters were as different from each other as possible. The KmL method belongs to classical algorithmic approaches (hierarchical or partitional clustering), but similar model-based methods also exist, such as mixture modelling techniques or latent class analysis [25]. In this study, the KmL was selected, as it could be run with only two measurement points. Moreover, it performs especially well when the sample size is small [26], and it is computationally less complex [27]. The longitudinal PA patterns (clusters) arrived at consisted of inactivity maintainers, activity maintainers, decreasers from moderate (to low) PA, decreasers from high (to moderate) PA (see Additional file 1).
Exposure variables
The potential correlates and determinants of interest were drawn from electronic surveys. With a few exceptions, the questions were based on the international Health Behaviour in School-aged Children (HBSC) study [1], and were repeated identically at both time points (unless otherwise stated). All the HBSC survey questions have been subject to validation and piloting at national and international levels [28], and many of the items have been assessed for their test-retest reliability [28, 29].
The questions assessing sports club participation and active commuting have been described elsewhere [5]. Dichotomous variables were used to assess participation in sports clubs and active commuting (by bike or on foot) to school (age 15), or to the study place or work (age 19). The questions assessing active commuting were modified from the Finnish schools on the Move survey [30].
Psychosocial variables: Loneliness was measured by one question: ‘Do you ever feel lonely?’ In further categorisation, the response options very often and often were combined, as were sometimes and never. A question estimating satisfaction with one’s own current weight included two response options (yes/no), and it was created for the purposes of the present study.
Communication with parents: The study participants were asked how easy it was for them to talk to their mother about things that really bothered them. The response options were: very easy, easy, difficult, and very difficult, with the additional response option I don’t have or see this person. Identical questions were posed regarding communication with the father and (if applicable) stepfather and stepmother. Separate dichotomised variables (easy vs. difficult) were formed for communication with (1) the mother and (2) the father. The latter also included talking over difficulties with one’s stepfather in cases where the respondent did not have a father (baseline n = 3, follow-up n = 5). Cases were excluded where there was neither mother nor stepmother (baseline n = 3, follow-up n = 8) (and similarly neither father nor stepfather, baseline n = 14, follow-up n = 16).
The frequency of exercising together with a parent was assessed via a question: ‘During a typical week: How often does your mother (or your stepmother if your mother does not live in your primary home)…. exercise or do sport with you?’ A corresponding question assessed exercising together with the father. Two categories were formed, encompassing (1) sometimes to very often, and (2) never to occasionally. Category 2 also included not having the parent in question, or not seeing that parent.
Health behaviour: The frequency of alcohol consumption was based on a question used in the Finnish School Health Promotion (SHP) study [31]: ‘On the whole, how often do you consume alcohol, for example a half-bottle of beer or more?’. The response options ranged from Once a week or more often to I don’t drink alcoholic beverages. A dichotomised variable was formed: (1) at least once a month, (2) less frequently or no consumption at all.
Lifetime drunkenness was based on a question asking adolescents whether they had ever had so much alcohol that they were really drunk. The response alternatives ranged from never to more than 10 times. A dichotomised variable was formed for lifetime drunkenness: (1) two times or more vs. (2) never or once.
Snuff use was assessed via the following question ‘Do you currently use snuff?’ The responses were categorised into two groups encompassing (1) less frequently to every day, (2) non-users. A correspondingly dichotomised variable was used to assess smoking frequency. Here, the categories less than weekly, weekly, and daily smokers were combined, due to the overall small proportion of current daily smokers at age 15.
Toothbrushing frequency was determined via a question: ‘How often do you brush your teeth?’. The answer options were dichotomised (< twice daily vs. twice daily) according to the international recommendation of twice-daily toothbrushing. Furthermore, the responses on frequency of eating breakfast on weekdays and frequency of eating school meals were dichotomised to (5 days vs. 4 days or less per week).
The fruit and vegetable index and the sweets and sugared soft drinks index were based on a question assessing the consumption of listed foods and drinks. The response options ranged from never to every day, more than once. The vegetable index ranged from 0 to 14, where value 0 represented no fruit and vegetable consumption, and value 14 consumption of both fruit and vegetables at least once a day. Correspondingly, value 0 indicated consuming both sweets and sugared soft drinks at least once a day, while value 14 indicated never eating sweets and sugared soft drinks (for more details see 32, 33). Energy drinks (with examples given such as Battery, RedBull) were also among the listed foods and drinks, and adolescents’ responses indicating energy drink consumption were categorised into two groups: (1) at least weekly, (2) never or less than weekly.
The amount of sleep was asked by a question created for the purposes of the present study: ‘How many hours do you sleep on average on weekdays?’. Respondents reported the amount by a number.
Data analysis
The cross-sectional differences between PA patterns were assessed with cross-tabulations and Chi-square test/Fisher’s exact test for categorial variables, and with the Kruskall-Wallis test (with post hoc Dunn’s test, adjusted by the Bonferroni correction for multiple tests) for continuous variables.
Multinomial logistic regression analyses were conducted to calculate odds ratios (ORs) with 95% confidence intervals (CIs) for the associations between the exposure variables and membership of PA patterns. For these analyses, the categories of activity maintainers and increasers were combined due to the relatively small number of increasers (n = 20), and because both categories represented a favourable evolution of PA in terms of health. This combined group was used as a reference in the analyses. Multiple different models were tested with the forced entry method, until the best-fitting ones were reached separately for (1) the baseline (mean age 15) and (2) the follow-up (mean age 19). Thus, the models (1) predicted membership of each pattern by determinants from the baseline (mean age 15), and (2) characterised the patterns at mean age 19 (longitudinal correlates). The models were adjusted for the measurement interval (age at the 2nd measurement minus age at the 1st measurement) and for the change in device wear-time. Missing cases (n = 1–14) were excluded from the analyses. The data analysis was performed using SPSS version 26, and the significance level was set at p < 0.05 in all the statistical tests.
Results
Descriptive information
Detailed descriptive information on the study participants has been provided previously [5], see also Additional file 2. Briefly, at baseline, nearly two-thirds (62%) of the participants lived in families with high affluence. At follow-up, most of the participants (69%) were still living with their parents. Half of the sample (49%) were studying in upper secondary education, while 13% were studying in higher education, and 21% were working (not studying) during the follow-up measurement. The inactivity maintainers were mostly females (73%), while the decreasers from high to moderate were mostly males (vs. 19% females). There were no other differences in sociodemographic characteristics between the PA patterns (see Additional file 2).
A previous study found no differences in baseline MVPA, family affluence, or perceived health between the baseline participants and those lost to follow-up [5]. However, males, and those who reported lower school achievement, were more likely not to participate in the post-measurement (p < 0.001).
Psychosocial and health behavioural characteristics of the PA patterns: univariable analysis
As shown in Tables 1 and 2, there were differences between PA patterns in multiple psychosocial variables (loneliness, communication difficulties with father, exercise with parents, and weight satisfaction) and in some health behaviours (smoking, dietary habits, and sleep). For example, exercising together with a parent at least occasionally was less frequent among inactivity maintainers (57%) and decreasers from moderate to low (59%) at age 15 as compared to increasers (95%) (Table 1). Health behaviours did not differ between PA patterns at age 15, apart from a slightly lower average sleep amount among inactivity maintainers as compared to decreasers from high to moderate PA and increasers (Table 2).
Correlates and determinants (multivariable analysis)
The most significant correlates and determinants for belonging to PA patterns were detected via multinomial logistic regression, using the combined group of activity maintainers and increasers as a reference (Figs. 1 and 2, Additional file 3). Both of the best-fitting models included sports club participation and gender as the most significant exposure variables, together with talking about difficulties with one’s father (using a model consisting of only baseline predictors) and fruit and vegetable consumption (using a model consisting of only exposure variables from follow-up measurements).

Analysis stemming from exposure variables presented at baseline (mean age 15)

Analysis stemming from exposure variables presented at follow-up (mean age 19)
Not participating in a sports club (OR: 4.6; CI: 2.2–9.6) and communication difficulties with one’s father (OR: 2.4; CI: 1.1–5.1) at age 15 were associated with increased odds of being an inactivity maintainer as compared to membership of a group with favourable PA development. Correspondingly, communication difficulties with one’s father at age 15 (OR: 3.3; CI: 1.6–7.1) was related to belonging to decreasers from moderate to low PA. Male gender was the only significant determinant for belonging to the decreasers from high PA.
Female gender (OR: 2.4; CI: 1.03–5.4), lower fruit and vegetable consumption (OR: 0.8; CI: 0.7–0.9), and not participating in a sports club at age 19 (OR: 6.4; CI: 2.6–14.7) were associated with increased odds of being an inactivity maintainer as compared to belonging to the combined group of activity maintainers and increasers. A lower fruit and vegetable consumption index at age 19 (OR: 0.9; CI: 0.8–0.97) was also related to being a decreaser from moderate PA. The same was true of smoking (OR: 3.0; 1.005–8.8).
Discussion
The study aimed to determine the psychosocial, health behavioural and PA domain-related characteristics of different longitudinal PA patterns from adolescence to young adulthood. The patterns (i.e. groups with different PA development over time) were based on device-measured MVPA and formed via a novel data-driven method. Multilevel factors were found to characterise the PA patterns. At age 15, gender, sports club participation, and communication difficulties with one’s father were the most important predictors for PA patterns. Correspondingly, at age 19, gender, sports club participation, and fruit and vegetable consumption were associated with longitudinal PA patterns.
A lack of sports club participation characterised inactivity maintainers throughout adolescence. Indeed, such non-participation showed the strongest association for belonging to this PA pattern. The result is in line with previous studies showing the relation between sports participation and maintained PA during adolescence [5, 9, 19]. Sports clubs have an important role in supporting maintained PA, including during early young adulthood, even if dropout from organised sports is common during adolescence [5, 34]. In Finland, sports clubs are typically based on voluntary civic activities at local level.
Surprisingly, communication difficulties with the father (but not with the mother) were related to increased odds of being a decreaser from moderate to low PA and also of being an inactivity maintainer. This implies that a father-adolescent relationship that supports open communication might be one determinant for sustained PA behaviour during adolescence. Note that we used only one question to assess the broad phenomenon, and that the association disappeared at age 19. One can suggest that analysis of the communication and relationship with parents would be a topic for future research on PA development during adolescence, since previous research has shown that parent-adolescent communication predicts adolescent MVPA one year later [35], and that communication difficulties pose a risk for decreased life-satisfaction [36,37,38]. Generally speaking, there has been a positive increasing trend in ease of communication with both parents over the 2000s, although communication with the mother has appeared to be easier than with the father [39, 40]. Future studies should examine whether communication with friends (including girl-/boyfriend) and siblings compensates for poorer communication with parents, especially during young adulthood. Further research could also encompass the extent to which a parent’s divorce (and subsequent residential arrangements) and the adolescent’s individual temperament alter the association between communication problems and PA patterns.
Feelings of loneliness at age 19 were more commonly reported by inactivity maintainers (14%) and by decreasers from moderate to low PA (16%) as compared to increasers (0%) and decreasers from high to moderate PA (0%). Because frequent loneliness was non-existent in some PA patterns, the loneliness variable did not fit into the logistic regression models. The association we found in cross tabulation is logical also when placed alongside a review study which provided evidence for the potential diminishing effect of loneliness on PA – but conversely, the potential value of PA in reducing loneliness [41].
From the multiple health behaviours analysed only fruit and vegetable consumption and smoking appeared among the multilevel correlates for PA patterns at age 19. Lower fruit and vegetable consumption was related to increased odds of belonging to both inactivity maintainers and decreasers from moderate to low PA, with smoking also being related to the decreaser group. These findings are more or less as expected, since both unhealthy and harmful behaviours tend to accumulate [42]. Moreover, the results here are in line with previous research indicating that fruit and vegetable consumption is higher among adolescents who are persistently active [43]. In another study exploring multiple health behaviours (but not dietary habits), smoking, and being drunk (the latter only for girls) at baseline (i.e. among 13- to 15-year-olds) were associated with increased odds of being an inactivity maintainer rather than an activity maintainer [19]. Similarly, smoking at a young adult age was more common among persistently sedentary participants than among their persistently active counterparts [44]. In our study, neither alcohol consumption nor binge drinking differed between the PA patterns, but the results are similar to previous studies insofar as smoking seems to be related to unfavourable PA development over time. According to a recent review study – which did not consider different longitudinal PA patterns – PA is positively associated with alcohol use among emerging adults (aged 18–25) but less consistently among adolescents [45]. However, methodological and contextual differences hinder comparison between the studies in question.
The decreasers from high to moderate PA constituted a relatively small group that could be characterised only by male gender. Maintained participation in sports clubs and also withdrawal from sports clubs (as opposed to ‘never-participation’, i.e. non-participation at either age 15 or 19) have previously been related to increased odds of being in this group of decreasers [5]. However, as compared to the other PA patterns detected, this decreaser group is less homogeneous, as shown by the relatively wide standard deviation in PA levels. These limit the possibility to form conclusions on the characteristics of this pattern. A similar pattern, involving a substantial decrease from high MVPA, has been found in a previous study by Kwon et al. [21], in which the male gender was more prevalent.
With regard to the other studied background variables, a lack of active commuting at either baseline or follow-up did not significantly differentiate between the PA patterns, even if sustained passive commuting has been related to maintained inactivity in the same study population (when inactive maintainers were compared to all the other groups together) [5]. This finding is a reminder that the time-varying nature of possible correlates should be also taken into account, and not just the associations at a single time point (see also [18, 46]).
Strengths and limitations
The main strengths of this study are the use of relatively large prospective data from a less-studied period of life (see also [2, 3, 6]), combining information from both survey and accelerometry to assess determinants and correlates for changed and maintained PA. Instead of grouping participants on the basis of predetermined PA levels, we used a novel data-driven method to identify genuinely heterogeneous PA patterns. The survey questions were mainly drawn from the international HBSC study, and the questions have thus been subject to validation [28].
The study encompassed multilevel predictors and correlates. However, it remains possible that certain other factors, operating for instance at the environmental level, might determine the differences between PA patterns. The data were limited to two measurements, and additional time points might have revealed more fluctuations in PA during adolescence. Furthermore, the number of persons in some of the PA patterns was small, which decreased the statistical power. Partly because of the sampling method (involving both sports clubs and schools), the young people in this study were more active than on average. However, this is also a strength, since it enabled a thorough analysis of PA and related factors for highly active young people in addition to those in the average population. Moreover, it can be claimed that the recruitment of the participants from six different regions of Finland (from 100 schools and 156 sports clubs) increased the quality of this study, even if the results are not directly generalisable to the entire Finnish age cohort in question.
Conclusions
This study contributed to the limited research base on PA development and its correlates during the transition to young adulthood. The results indicate that the relationship with one’s father may play a role in supporting maintained PA during the adolescent years. Furthermore, a healthier diet and non-smoking as a young adult are associated with more favourable PA development. The study gives indications that although dropout from a sports club is common during adolescence [5, 34], organised sports still have a contribution in supporting favourable PA development when adolescents reach young adulthood.
While the study was successful in revealing some characteristics of the PA patterns, much variation exists in PA behaviour and related factors. Thus, the findings also demonstrate the complex and multidimensional nature of PA behaviour. This implies that there can be no ‘one size fits all’ in PA promotion; nevertheless, by addressing multiple different aspects, there may be better possibilities for preventing a decrease in PA and supporting the maintenance of healthy PA.
Data Availability
The data underlying this article cannot be shared publicly since they contain confidential personal details and health information. The data will be shared on reasonable request to the principal investigator (sami.p.kokko@jyu.fi).
Abbreviations
- CI:
-
confidence interval
- MET:
-
metabolic equivalent
- MVPA:
-
moderate-to-vigorous physical activity
- OR:
-
odds ratio
- PA:
-
physical activity
References
Inchley J, Currie D, Budisavljevic S, Thorheim T, Jåstad A, Cosma A, et al., editors. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged children (HBSC) survey in Europe and Canada. International report. Volume 1. Key findings. Copenhagen: WHO Regional Office for Europe; 2020.
Corder K, Winpenny E, Love R, Brown HE, White M, van Sluijs E. Change in physical activity from adolescence to early adulthood: a systematic review and meta-analysis of longitudinal cohort studies. Br J Sports Med. 2019. https://doi.org/10.1136/bjsports-2016-097330.
Farooq A, Martin A, Janssen X, Wilson MG, Gibson A-M, Hugher A, et al. Longitudinal changes in moderate-to-vigorous-intensity physical activity in children and adolescents: a systematic review and meta-analysis. Obes Rev. 2020. https://doi.org/10.1111/obr.12953.
Bull FC, Al-Ansari SS, Biddle S, Korodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020. https://doi.org/10.1136/bjsports-2020-102955.
Aira T, Vasankari T, Heinonen OJ, Korpelainen R, Kotkajuuri J, Parkkari J, et al. Physical activity from adolescence to young adulthood: patterns of change, and their associations with activity domains and sedentary time. Int J Behav Nutr Phys Act. 2021. https://doi.org/10.1186/s12966-021-01130-x.
Lounassalo I, Salin K, Kankaanpää A, Hirvensalo M, Palomäki S, Tolvanen A, et al. Distinct trajectories of physical activity and related factors during the life course in the general population: a systematic review. BMC Public Health. 2019. https://doi.org/10.1186/s12889-019-6513-y.
Pate RR, Schenkelberg MA, Dowda M, McIver KL. Group-based physical activity trajectories in children transitioning from elementary to high school. BMC Public Health. 2019. https://doi.org/10.1186/s12889-019-6630-7.
Young DR, Cohen D, Koebnick C, Mohan Y, Saksvik BI, Sidell M, et al. Longitudinal associations of physical activity among females from adolescence to young adulthood. J Adolesc Health. 2018. https://doi.org/10.1016/j.jadohealth.2018.05.023.
Kwon S, Janz KF, Letuchy EM, Burns TL, Levy SM. Developmental trajectories of physical activity, sports, and television viewing during childhood to young adulthood: Iowa bone development study. JAMA Pediatr. 2015. https://doi.org/10.1001/jamapediatrics.2015.0327.
Reilly JJ. When does it all go wrong? Longitudinal studies of changes in moderate-to-vigorous-intensity physical activity across childhood and adolescence. J Exerc Sci Fit. 2016. https://doi.org/10.1016/j.jesf.2016.05.002.
Bauman A, Reis RS, Sallis JF, Wells JC, Loos RJF, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380:258–71.
Sallis J, Owen N. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health Behavior: theory, Research, and practice. San Francisco: Jossey-Bass; 2015. pp. 43–64.
Halfton N, Larson K, Lu M, Tullis E, Russ S. Lifecourse health development: past, present and future. Matern Child Health J. 2014;18:344–65.
Hirvensalo M, Lintunen T. Life-course perspective for physical activity and sports participation. Eur Rev Aging Phys Act. 2011. https://doi.org/10.1007/s11556-010-0076-3.
Tones K, Tilford S. Health Promotion. Effectiveness, efficiency and equity. 3rd ed. Nelson Thornes; 2001.
Elder GH Jr, Johnson MK, Crosnoe R. The emergence and development of life course theory. In: Mortimer JT, Shanahan MJ, editors. Handbook of the life course. New York: Kluwer Academic/Plenum; 2003. pp. 3–19.
Li K-K, Cardinal BJ, Settersten RA. Toward a life-course perspective on physical activity promotion. Quest. 2009. https://doi.org/10.1080/00336297.2009.10483620.
Mielke GI. Relevance of life course epidemiology for research activity and sedentary behavior. J Phys Act Health. 2022. https://doi.org/10.1123/jpah.2022-0128.
Rangul V, Holmen TL, Bauman A, Bratber GH, Kurtze N, Midthjell K. Factors predicting changes in physical activity through adolescence: the young-HUNT study, Norway. J Adolesc Health. 2011. https://doi.org/10.1016/j.jadohealth.2010.09.013.
Zook KR, Saksvig BI, Wu TT, Young DR. Physical activity trajectories and multilevel factors among adolescent girls. J Adolesc Health. 2014. https://doi.org/10.1016/j.jadohealth.2013.07.015.
Kwon S, Janz KF, Letuchy EM, Burns TL, Levy SM. Parental characteristic patterns associated with maintaining healthy physical activity behavior during childhood and adolescence. Int J Behav Nutr Phys Act. 2016. https://doi.org/10.1186/s12966-016-0383-9.
Kokko S, Selänne H, Alanko L, Heinonen O, Korpelainen R, Savonen K, et al. Health promotion activities of sports clubs and coaches, and health and health behaviours in youth participating in sports clubs: the health promoting sports club study. BMJ Open Sport Exer Med. 2015. https://doi.org/10.1136/bmjsem-2015-000034.
Vähä-Ypyä H, Vasankari T, Husu P, Mänttäri A, Vuorimaa T, Suni T, et al. Validation of cut-points for evaluating the intensity of physical activity with accelerometry-based mean amplitude deviation (MAD). PLoS ONE. 2015. https://doi.org/10.1371/journal.pone.0134813.
Vähä-Ypyä H, Husu P, Suni J, Vasankari T, Sievänen H. Reliable recognition of lying, sitting, and standing with a hip-worn accelerometer. Scan J Med Sci Sports. 2018. https://doi.org/10.1111/sms.13017.
Genolini C, Falissard B. KmL: k-means for longitudinal data. Comput Stat. 2010. https://doi.org/10.1007/s00180-009-0178-4.
Gong H, Xiaolei X, Zhou Y. Profile clustering in clinical trials with longitudinal and functional data methods. J Biopharm Stat. 2019. https://doi.org/10.1080/10543406.2019.1572614.
Den Teuling NGP, Pauws SC, van den Heuvel ER. A comparison of methods for clustering longitudinal data with slowly changing trends. Commun Stat Simul Comput. 2015;53(3):621–648. https://doi.org/10.1080/03610918.2020.1861464.
Currie C, Inchley J, Molcho M, Lenzi M, Veselska Z, Wild F, Editors. Health Behaviour in School-aged children (HBSC) study protocol: background, methodology and mandatory items for the 2013/14 survey. St Andrews: CAHRU; 2014.
Liu Y, Wang M, Tynjälä J, Villberg J, Zhang Z, Kannas L. Test-retest reliability of selected items of Health Behaviour in School-aged children (HBSC) survey questionnaire in Beijing, China. BMC Med Res Methodol. 2010. https://doi.org/10.1186/1471-2288-10-73.
LIKES Research Centre for Sport and Health Sciences. https://www.liikkuvakoulu.fi/english Assessed 9 June 2022.
National Institute of Health and Welfare., School Health Promotion study, Finland: https://thl.fi/en/web/thlfi-en/research-and-development/research-and-projects/school-health-promotion-study. Assessed 8 June 2022.
Vereecken CA, Rossi S, Giacchi MV, Maes L. Comparison of a short food-frequency questionnaire and derived indices with a seven-day diet record in Belgian and Italian children. Int J Public Health. 2008;53:297–422.
Heikkilä L, Korpelainen R, Aira T, Alanko L, Heinonen OJ, Kokko S, et al. The associations between adolescents’ sports club participation and dietary habits. Transl Sports Med. 2021. https://doi.org/10.1002/tsm2.249.
Rinta-Antila K, Koski P, Heinonen OJ, Korpelainen R, Parkkari J, Savonen K, et al. Educational and family-related determinants of organized sports participation patterns from adolescence to emerging adulthood: a four-year follow-up study. Int J Health Promotion Educ. 2022. https://doi.org/10.1080/14635240.2022.2116943.
Ornelas IJ, Perreira KM, Ayala GX. Parental influences on adolescent physical activity: a longitudinal study. Int J Behav Nutr Phys Act. 2007;4:3.
Levin KA, Dallago L, Currie C. The associations between adolescent life satisfaction, family structure, family affluence and gender differences in parent-child communication. Soc Indic Res. 2012;106:287–305.
Boniel-Nissim M, Tabak I, Mazur J, Borracciono A, Brooks F, Gommans R, et al. Supportive communication with parents moderates the negative effects of electronic media use on life satisfaction during adolescence. Int J Public Health. 2015. https://doi.org/10.1007/s00038-014-0636-9.
Jiménez-Iglesias A, García-Moya I, Moreno C. Parent-child relationships and adolescents’ life satisfaction across the first decade of the new millennium. Fam Relat. 2017. https://doi.org/10.1111/fare.12249.
Brooks F, Zaborskis A, Tabak I, Granado Alcón MdC, Zemaitiene N, de Roos S, Klemera E. Trends in adolescents’ perceived parental communication across 32 countries in Europe and North America from 2002 to 2010. Eur J Public Health. 2015;25(Suppl 2):46–50.
Inchley J, Currie D, Budisavljevic S, Thorheim T, Jåstad A, Cosma A, et al., editors. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged children (HBSC) survey in Europe and Canada. International report. Volume 2. Key data. Copenhagen: WHO Regional Office for Europe; 2020.
Pels F, Kleinert J. Loneliness and physical activity: a systematic review. Int Rev Sport Exer. 2016. https://doi.org/10.1080/1750984X.2016.1177849.
Heikkala E, Remes J, Paananen M, Taimela S, Auvinen J, Karppinen J. Accumulation of lifestyle and psychosocial problems and persistence of adverse lifestyle over two-year follow-up among Finnish adolescents. BMC Public Health. 2014;14:542.
Lounassalo I, Hirvensalo M, Kankaanpää A, Tolvanen A, Palomäki S, Salin K, et al. Associations of leisure-time physical activity trajectories with fruit and vegetable consumption from childhood to adulthood: the cardiovascular risk in Young finns Study. Int J Environ Res Public Health. 2019. https://doi.org/10.3390/ijerph16224437.
Raitakari O, Porkka K, Taimela S, Telama R, Räsänen L, Viikari J. Effects of persistent physical activity and inactivity on coronary risk factors in children and young adults. Am J Epidem. 1994;3(140):195–205.
West AB, Bittel KM, Russell MA, Evans MB, Mama SK, Conroy DE. A systematic review of physical activity, sedentary behavior, and substance use in adolescents and emerging adults. TBM. 2020. https://doi.org/10.1093/tbm/ibaa008.
Biddle S, Gorely T, Faulkner G, Mutrie N. Psychology of physical activity: a 30-year reflection on correlates, barriers, and theory. Int J Sport Exerc Psychol. 2023. https://doi.org/10.1080/1612197X.2022.2147261.
Acknowledgements
The authors thank all the sports clubs, schools, and young people who participated in the HPSC study, all those who assisted with the data collection, and Donald Adamson, who polished the English language of the manuscript.
Funding
This work was supported by the Ministry of Education and Culture (major, grant numbers: 6/091/2011, 28/626/2016), the Ministry of Social Affairs and Health (minor, grant number: 152/THL/TE/2012) encompassing all parts of the study. The funders had no role in the study design, data collection, statistical analysis, or preparation of this manuscript.
Open Access funding provided by University of Jyväskylä (JYU).
Author information
Authors and Affiliations
Contributions
SK is the principal investigator for the HPSC study, and was a major contributor in reviewing the manuscript together with TV. TA designed and conducted the analyses and drafted the manuscript, HV was responsible for processing the accelerometer data, and JK and JV advised on the statistical aspects of the study. TV, OH, RK, JK, JP, KS, KT, AU, MV, HV, and SK critically reviewed the final manuscript. All the authors contributed to the design of the work, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The HPSC study was conducted in accordance with the Declaration of Helsinki, and received ethical approval from the Ethics Committee of the Healthcare District of Central Finland (20.12.2012 (23 U/2012), 15.12.2016). Written informed consent was obtained from the participants, and also from a guardian when the participant was aged under 18. The permission notification included detailed information on the study, plus notification on the right of participants to refuse participation, and to withdraw their consent without giving a reason.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Aira, T., Vasankari, T., Heinonen, O.J. et al. Psychosocial and health behavioural characteristics of longitudinal physical activity patterns: a cohort study from adolescence to young adulthood. BMC Public Health 23, 2156 (2023). https://doi.org/10.1186/s12889-023-17122-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-17122-4