
Abstract
Background
Musculoskeletal disorders and injuries (MSDI) are conditions that affect the locomotor system characterized by pain and impairment of functionality. They are the leading cause of years lived with disability. The aim of this study was to analyze the factors that influence the return to work (RTW) among workers on sick leave due to MSDI.
Methods
A longitudinal study was conducted in the city of São Paulo, Brazil, between 2020–2022. The participants were 216 workers who required social security compensation due to MSDI. They filled out online questionnaires about their sociodemographic characteristics, health risk behaviors, work characteristics and health conditions. They were followed for 365 days after their first day of sick leave. A Cox regression was performed to identify the factors that influenced their first RTW.
Results
Most participants were male (53.0%), mean age was 39.5 years (SD 10.6), 70.4% returned to work within the one-year follow-up period. The mean duration of sick leave was 192.6 days. Factors associated with a lower RTW were age 40 years and older (HR 0.54; 95%CI 0.39–0.76) and the interaction between perceptions of the need for improvement in the physical and psychological domains of quality of life (HR 0.67; 95%CI 0.48–0.94).
Conclusions
Occupational healthcare professionals should pay greater attention to patients who are aging and those with perceived worse physical and psychological conditions, in order to facilitate the reintegration process and promote sustained RTW after sick leave due to musculoskeletal disorder or injury.
Similar content being viewed by others


Introduction
According to the World Health Organization (WHO), musculoskeletal disorders and injuries (MSDI) are pathological conditions that affect the structures of the locomotor system, including bones, muscles, joints, and connective tissue. These conditions are characterized by pain and reduced mobility, dexterity, and functionality, which can lead to impaired work performance. They can have either a sudden onset with limited duration or a chronic progression that lasts throughout an individual's life, potentially causing limitations and disabilities [1].
The Global Burden of Diseases study reports that approximately 1.71 billion people worldwide are affected by MSDI. These conditions are the leading cause of Years Lived with Disability (YLD), accounting for 17% of all causes. The most prevalent forms of MSDI include low back pain, bone fractures, and osteoarthritis [2].
Various factors contribute to the development of MSDI, which can be classified as individual, biomechanical, and psychosocial factors. Individual factors include a sedentary lifestyle, smoking, high body mass index (BMI) and presence of comorbidities [3]. Biomechanical risk factors involve physical exertion, repetitive movements, improper static or dynamic posture and heavy lifting [3]. Psychosocial factors, particularly those related to work, include low social support, job dissatisfaction, high occupational stress, and lack of control at work [3].
Depending on the degree of dysfunction caused by MSDI, individuals may experience partial or total reduction in work capacity, either temporarily or permanently. In Brazil, disability benefits are provided to workers who require sick leave for more than 15 days. Between 2017 and 2019, an average of 2.32 million benefits were granted, with approximately 662,000 attributed to MSDI, comprising 40% of diseases and 60% of injuries [4]. After the cessation of this benefit, workers are required to report back to their companies for a return-to-work process, with necessitates evaluation by an occupational medicine professional if the sick leave exceeds 30 days.
Recent longitudinal studies conducted in several northern-hemisphere developed countries identified factors influencing the rate of return to work (RTW) in individuals with MSDI. These factors include: sociodemographic characteristics (such as sex [5,6,7], age [5, 7, 8], marital status [7], and education level [5, 7, 9]), working conditions (such as physical exertion [5, 6, 10, 11], length of absence [12], social support [8, 11], and self-efficacy [8, 11, 13, 14]) and clinical characteristics (such as site of injury [5], pain intensity [5, 11], comorbidities [7, 8, 12], and treatment used [6, 11]).
Considering the epidemiological significance of MSDI, the impact of these conditions on workers’ functionality, and their individual and social costs, it is in essential to identify the factors that predict RTW among workers on sick leave due to such conditions in the Brazilian context. This information will not only help identify individuals who require more attention in the return process, but also aid in defining more effective strategies for rehabilitation and professional reintegration. The aim of this study was to analyze the sociodemographic, occupational, and clinical factors that influence the RTW after sick leave due to musculoskeletal disorders or injuries.
Methods
Design
This longitudinal analytical study was conducted between 2020 and 2022.
Location
A social security service unit in the city of São Paulo was selected based on convenience. São Paulo is the most populous city in Brazil, located in the southeastern region of the country.
Sampling
In Brazil, if a worker´s sick leave lasts up to 15 days, the employer is responsible for providing payment. However, if the sick leave exceeds 15 days, workers must claim sickness benefits from the public social security system, known as the National Social Security Institute (INSS). Applicants undergo medical evaluations to determine eligibility for sick leave benefits. For this study, participants were workers on long-term sick leave for more than fifteen days who had sought benefits due to disability for work.
The calculation of the sample size required to achieve a dependable estimate of the proportion within an unrestricted population was based on the estimated prevalence of individuals engaging in their 'first return to work after a prolonged absence due to musculoskeletal disorders,' as reported in the study conducted by Kausto et al. [10]. A confidence level of 95% (α = 0.05) was selected, corresponding to a critical value of 1.96, while maintaining a maximum acceptable estimation error of 5%. The resulting minimum sample size determined for this study is 114 participants.
Inclusion and exclusion criteria
The inclusion criteria for the study were as follows: participants needed to have a formal employment contract with a permanent work situation, and they needed to have submitted an application for sickness benefit due to an illness classified in chapter XIII (Diseases of the musculoskeletal system and connective tissue) or chapter XIX (Injuries, poisoning and some other consequences of external causes) of the 10th edition of the International Statistical Classification of Diseases and Health-Related Problems (ICD10). Requests resulting from Mononeuropathies of the Upper Limbs (ICD10 G56) were also included, as their risk factors and clinical courses are similar to musculoskeletal disorders, although they are not strictly classified as such.
Workers without formal employment or with multiple formal employment were excluded due to the potential variability in study outcome. Individuals with a history of returning to work before their participation in this current study were also excluded.
Data collection
After undergoing a medical examination, workers who met the inclusion criteria were taken to a separate room, where they were invited to participate in the study and received information about its objectives and potential risks. Out of the 248 workers who were invited, 216 met the criteria and voluntarily agreed to participate. All of them signed a free and informed consent statement. They were then invited to complete a questionnaire using a link to an online platform.
Instruments
The participants answered a questionnaire consisting of four blocks of questions:
-
I.
Sociodemographic characteristics: This block included questions about sex, date of birth, schooling and marital status;
-
II.
Health risk behaviors: Participants were assessed for smoking, using the Fagerström Tolerance Questionnaire [15]; harmful alcohol consumption was assessed using the Audit C questionnaire developed by the World Health Organization [16]; and physical activity in the weeks prior to going on sick leave was also assessed;
-
III.
Characteristics and conditions of work: This block included questions about the participant´s current job position, number of years working in the current company, entry time for work shift, and occupational psychosocial factors evaluated using the Brazilian Portuguese version of the Effort-Reward Imbalance Questionnaire [17];
-
IV.
Clinical condition: This block comprised questions regarding clinical morbidities under medical follow-up; as well as self-related weight and height for calculating body mass index (BMI); and the Brazilian Portuguese version for the WHOQOL-bref (World Health Organization Quality of Life) questionnaire with 26 questions and answers on a 5-points Likert Scale. From this questionnaire, the participant´s perception of quality of life and satisfaction with health were analyzed by a single question; and mean scores from questions about physical (7), psychological (6), social relationships (3), and environmental (8) domains indicated a category – “need to improve”, “regular”, “good”, or “very good” [18].
After each participant completed these questionnaires, one of the researchers accessed their expert medical report to obtain additional information, including the Brazilian Classification of Occupations (BCO) code, the ICD10 code for the reason for sick leave, the type of benefit granted (work-related/ no work-related / not reported) and the date of onset of the disability.
Outcome
The date of first RTW was obtained from the National Register of Social Information (CNIS), a national system that collects workers’ social security data. The outcome, referred to as “survival time”, was evaluated as the number of days between the date when the work disability condition started (according to the medical expert report) and the date of the first RTW in the same company where the participant was working at the time of going on sick leave. In cases where no RTW occurred during the follow-up period, the end of the follow-up was defined as 365 days after the first day of work disability, representing type I right censoring.
Analysis
The descriptive analyses included calculation means and standard deviations (SD) for quantitative variables, and absolute and relative frequencies for qualitative variables. For survival analyses (Kaplan–Meier curves and Cox regression), variables with categories that had a small number of participants were dichotomized.
Kaplan–Meier survival curves were constructed to estimate the probabilities of survival overall and accordance to the evaluated covariates. The log-rank test was used to compare accumulated survival curves between categories of independent variables. The statiscal significance was considered when p < 0.05. Those variables presenting p < 0.20 in the univariate analysis were selected for multiple analysis to avoid excluding any variable with potential confounding or interaction effects.
Cox regression analysis with the stepwise forward method was used to evaluate the combined effect of independent variables on the outcome. The assumption of risk proportionality was assessed using residual graphs and the Schoenfeld test, and significance was considered when p < 0.05. Independent variables that did not meet this fundamental assumption were excluded. Although a convenience sample may introduce some challenges and limitations when applying statistical inference, hazard ratios (HR) are frequently utilized in survival analysis to compare hazard rates between different groups. The limitations of utilizing this statistical inference in the present study are explored towards the end of the discussion section.
HR values below 1.0 indicate a reduced likelihood of returning to work based on the length of the follow-up period. Possible interaction or confounding effects were tested whenever the inclusion of a new variable in the model resulted in changes in the parameter estimates (changes exceeding 10.0% in HR values and their confidence intervals, reversal of statistical significance, or parameter adjustments regardless of significance). In these situations, potential interaction/confounding effects were examined through stratified analysis. If the stratified analysis suggested interaction, the modification of the effect was also tested by creating an interaction variable (product-term considering the exposure variable and the potential interaction factor). Possible overfitting effects resulting from association/collinearity between variables were also tested.
Ethical issues
The study was approved by the Ethics Committee for Research on Human Beings of the School of Public Health of the University of São Paulo (opinion report no. 3,166,922/2019; CAEE 87446718.9.0000.5421).
Results
Data from 216 individuals were collected. In terms of sociodemographic characteristics, it was observed that 53.2% were men. The age range was between 18.6 and 64.2 years, with a mean of 39.4 years (SD 10.6). The most common level of education was high school, with education ranging from more than 8 years to 11 years of study, accounting for 50.9% of the participants (Table 1).
Regarding reported health risk behaviors: 13.0% of the participants were smokers, 47.7% consumed alcoholic beverages, and 54.2% were sedentary in the weeks prior to going on sick leave (Table 1).
Table 2 presents information regarding the participants’ work. In terms of their occupation at the time of going on sick leave, a total of 108 BCO codes were mentioned. The most common groups were manual activities (61.6%), cleaning work (5%) and work as urban bus drivers (4.6%). The majority of participants had been working in their current role for less than five years (59.7%), with 17.6% having worked for less than a year. For 72.7% of participants, the start time of their work was always in the morning hours. The mean score for work effort was 14.0 points (SD 5.6) and the mean score for reward was 20.6 points (SD 9.4). A situation of imbalance was reported by 76.4% of the participants.
The mean BMI value was 27.9 kg/m2 (SD 4.9), ranging from 18.3 to 46.3 kg/m2. In terms of comorbidities, 26.4% of participants reported undergoing medical follow-up for another disease in addition to the condition that led to sick leave (Table 3).
When it comes to the participant´s perception of their quality of life, the majority (54.2%) rated it as regular or in need to improve. However, 66.7% of study participants expressed a good or very good level of satisfaction with their own health. In terms of the different domains, the social relationships domain had the highest mean score (3.5; SD 0.9), while the physical domain had the lowest mean score (2.6; SD 0.9).
Regarding the causes of the participants’ sick leave, 56.5% were classified under Group M (disorders) and 43.5% under Group S-T (injuries). The most frequent causes included back pain (11.5%), intervertebral disc disorders (10.1%), wrist and hand fractures (8.7%), shoulder injuries (7.8%) and leg fractures (5.9%). Regarding the type of benefit granted, 24.5% of the requests were considered work-related conditions.
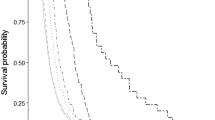
The incidence of RTW was 70.4% and the mean duration of sick leave was 192.6 days (SD 118.2). Among the workers who returned to work (70.4%), the probability of remaining on sick leave for up to 90 days was 76.2%, for up to 180 days was 48.3%, for up to 270 days was 32.9%, and for up to 365 day was 25.6% (Fig. 1).

Kaplan–Meier survival curve for return to work within one year of participants on sick leave due to musculoskeletal disorder or injury. São Paulo – Brazil, 2020–2022 (N = 216)
Table 4 presents the results from the univariate Cox regression analysis. It shows that several factors were significantly associated with a lower probability of returning to work, including being in the age group of 40 years or older, perceiving a regular or needing improvement in quality of life, perceiving regular or needing improvement in the physical and psychological domains of quality of life, having musculoskeletal diseases, and undergoing medical follow-up for diseases other than the condition that led to sick leave.
The multiple analysis revealed that the age group remained significant in the model, indicating that individuals aged 40 years or older had a lower likelihood of returning to work compared to younger (HR 0.54; 95% CI 0.39–0.76). Regarding quality of life, an interaction variable between the physical and psychological domains was constructed. It showed that among individuals who perceived their condition as regular or needing improvement, there was a lower probability of returning to work within one year after going on sick leave due to MSDI (HR 0.48; 95% CI 0.48–0.94).
Discussion
In this study, our objective was to analyze the sociodemographic, occupational, and clinical factors that influence the RTW after sick leave due to musculoskeletal disorder or injury. We identified two factors independently associated with a lower probability of returning to work: age equal or greater than 40 years and the interaction between the perceptions of needing improvement in the physical and psychological domains.
The incidence of RTW reported in previous studies with similar follow-up period has varied from 66.7% to 92% [5, 7, 8, 10]. The highest rates were observed in a survey conducted in Finland, among individuals who had been on sick leave due to back problems for at least ten days [10], and in a study conducted in Norway, among individuals who had been on sick leave for more than fifteen days due to musculoskeletal complaints [7]. The lowest rate was reported in a survey conducted in Sweden among women with an average age over 50 years [8].
The mean duration of sick leave in our study was longer than that reported in the study by Gjesdal et al. [7], where the durations were 101 days for back conditions, 110 days for upper-limb diseases, and 164 days for osteoarthritis. Another study conducted in Norway, by Rysstad et al., evaluated various trajectories between going on sick leave and reintegration into work. They found that one group returned after only 67.1 days, while another group with persistently higher sick leave duration returned to work after 221.1 days [19].
In a Norwegian cohort study with a one-year follow-up, the trajectory of individuals on sick leave due to MSDI was evaluated. It was observed that new episodes of sick leave occurred in the months following their RTW [19]. A study in Finland among workers on sick leave due to spinal problems identified recurrence factors such as advanced age, persistent health problems and comorbidities [10]. Therefore, reintegration into work is just one step in the process of returning to work, as sustained effectiveness in seeking reintegration is necessary.
Sociodemographic characteristics
In this Brazilian study, the survival rate for the return of workers over 40 years of age was found to be lower compared to younger individuals, which is consistent with the findings of Canceliere et al. [9] and other subsequent studies [5, 7, 8]. It is likely that resolving musculoskeletal conditions in older individuals is more complex due to the structural and functional degeneration of their tissue and bone elements, which reduces their ability to respond effectively to injuries [20].
Regarding the influence of sex on the RTW, studies have yielded divergent results. Some have reported longer time off work for both men [7] and women [5, 6]. Marital status at the time of the study is also a characteristic for which there is no consensus in the literature regarding its impact on the RTW. The study by Gjesdal et al. [7] found that not having a partner favored the return, whereas in the study by Rashid, Kristofferzon and Nilsson [8] reported the opposite. In the present study, sex and marital status did not have a significant influence on the RTW. Similarly, high levels of education were not found to be significant in the present study, although previous research has suggested that high education levels are associated with a higher likelihood of returning to work [5, 7,8,9].
Occupational factors
Previous studies have consistently shown that the prognosis for returning to work after a disability episode due to musculoskeletal disorders is worse for workers in manual activities [5, 6, 9,10,11]. This can be attributed to the higher physical and biomechanical demands faced by manual workers (blue-collar workers) compared to those in administrative occupations (white-collar workers), as well as lower levels of education and remuneration [21]. These factors may result in greater difficulties in accessing care and rehabilitation services, leading to impaired clinical resolution, and impacting work capacity recovery, especially for workers with fewer years of schooling and higher physical demands at work. However, in the present study, no significant impact was observed from the generic occupational characteristics when comparing manual workers with other occupations that likely had lower musculoskeletal workloads such as supervisors, administrative workers, and customer service workers.
Regarding organizational work characteristics (e.g., work shift) and occupational psychosocial factors (e.g., high effort, low reward, and their imbalance), the present study did not find any significant impact on the RTW outcome. This result is consistent with the findings of a review study that also did not find an association between these factors on the outcome of returning to work when studying a population with similar clinical conditions [9].
A study conducted by Devin et al. showed that individuals who received financial compensation for their time off work after spinal surgery took longer to RTW [5]. In Brazil, workers who receive a work-related type of disability benefit are entitled to job security for a minimum period of twelve months after their social security benefit ends. There was an expectation that this variable would have an impact on the rate of RTW. However, in the present study, no significant association was observed between receiving a work-related disability benefit ant the likelihood of returning to work.
Clinical issues
In the present study, participants’ perceptions of their quality of life during sick leave were found to influence their rate of RTW. Specifically, the perception of the need for improvement in both the physical and psychological domains indicated that better management of workers’ health conditions is necessary for successful reintegration into work. This suggests a direct relationship between the disabling condition and the worker´s ability to RTW. Interestingly, occurrences of medical follow-up for other diseases, which were significant in the univariate analysis, did not emerge as a risk factor in the final model.
Previous studies have shown that factors such as diffuse muscle pain [7, 11], pain intensity levels [8], and the presence or persistence of pain after surgical treatment [22] can influence the rate of RTW. Psychological aspects, including distress, somatization, and catastrophizing, have also been identified as negative factors for RTW in the Netherlands, with a group of workers with low back pain [11]. However, in this Brazilian study, the most unfavorable situation for RTW was when dissatisfaction was present in both the physical and psychological domains, as these factors alone did not independently influence the outcome. These findings align more closely with a study conducted in Sweden, where the coexistence of depression and musculoskeletal conditions had a negative impact on reintegration to work [8].
Self-efficacy has been identified as a predictive variable for RTW in several studies [8, 11, 13, 14, 19]. This could be explained by the fact that workers’ expectation of returning to work reflect not only their confidence recovering physical abilities, but also their emotional readiness to return to the work environment and activities. Therefore, even though workers expressed need for improvement in the physical and psychological domains, they might still lack the necessary self-confidence to attempt a RTW, as observed in the current study.
It is important to note that the definition of work ability is strongly influenced by workers’ perceptions of their own condition [23]. Therefore, physical rehabilitation alone may not be sufficient. The presence of depression, which often includes feelings of worthlessness and hopelessness [24], has also identified as a negative predictor for returning to work [8, 12]. Multidisciplinary rehabilitation programs that enhance workers’ motivation have shown positive results in terms of increasing the incidence of RTW [9, 12].
Study limitations
One of the strengths of this study was the longitudinal design for defining the outcome. However, the absence of multiple waves of data collection limited the exploration of various trajectories from the start of sick leave until the end of the follow-up period.
The study´s internal validity may have been affected by sampling bias, as participation depended on the interest of the invited individuals in the topic. However, the number of participants exceeded the minimum recommended. To address measurement bias, the study had a dual confirmation of participant´s diagnoses through medical certification from the physician who recommended the sick leave and who conducted the social security evaluation, also responsible to recruit potential cases. There may still have been some memory bias, particularly in responses to questions about exposures that had already ceased, such as work-related factors.
An additional limitation was the requirement imposed by Brazilian legislation, which only allows individuals to RTW after the end of their social security benefit. This may have led to a discrepancy between the recovery of work ability and the actual RTW date. To mitigate this bias, the outcome was determined based on registration information provided by the employing company to the Brazilian government.
The results should be interpreted with caution, as the use of convenience sampling and the relatively small number of evaluated cases may introduce biases in the results. The characteristics of the social security services and the patients make it difficult to compose a probabilistic sample. However, these exploratory results can be considered indicative of the underlying processes of the first RTW. Further studies should evaluate the progress of workers following this endeavor, taking into account the potential for recurrent absences, which could signify a lack of success in professional reintegration.
To control biases, some precautions were taken, such as using validated instruments for use in Brazil, grouping categories in variables, modeling using the stepwise method, and testing for interactions through stratified analysis, and, if necessary, by creating an interaction variable.
In terms of external validity, the findings are limited to a sample of workers from a single urban area in Brazil, although the profile observed is aligned with studies conducted in other locations.
Conclusions
In the present study, it was identified that being 40 years and older at the time of sick leave, as well as the workers perceiving the need for improvement in both their physical and psychological domains of quality of life, had a negative impact on the RTW. Disabilities due to musculoskeletal disorder or injury led to significant financial and societal burden. Given the complexity of the return-to-work process, involving both workers and professionals who support them in a multidisciplinary approach may lead to greater success in facilitating reintegration.
More effective strategies and programs for tertiary prevention could benefit workers on sick leave in their return-to-work process, including its sustainability. Additional support should be given to individuals who are aging and those with more severe physical and psychological conditions.
Availability of data and materials
The datasets generated and analysed during the current study are available in the Figshare repository:
https://figshare.com/articles/dataset/Silva-Junior_et_al_2023_DataSet_xlsx/21824832/3.
References
World Health Organization. Musculoskeletal health. Geneva: WHO; 2022. Cited 06 Jan 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions.
Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10267):2006–17.
da Costa BR, Vieira ER. Risk factors for work-related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am J Ind Med. 2010;53(3):285–323.
Brasil. Ministério da Previdência Social. AEPS Infologo. Informações: Benefícios por Incapacidade Concedidos por CID. Brasília: MPS; 2022. Cited 06 Jan 2023. Available from: http://www3.dataprev.gov.br/infologo/GCON/CON10/CON10.php.
Devin CJ, Asher AL, Archer KR, Goyal A, Khan I, Kerezoudis P, et al. Impact of dominant symptom on 12-month patient-reported outcomes for patients undergoing lumbar spine surgery. Neurosurgery. 2020;87(5):1037–45.
Coric D, Zigler J, Derman P, Braxton E, Situ A, Patel L. Predictors of long-term clinical outcomes in adult patients after lumbar total disc replacement: development and validation of a prediction model. J Neurosurg Spine. 2021;1(aop):1–9.
Gjesdal S, Holmaas TH, Monstad K, Hetlevik Ø. New episodes of musculoskeletal conditions among employed people in Norway, sickness certification and return to work: a multiregister-based cohort study from primary care. BMJ Open. 2018;8(3): e017543.
Rashid M, Kristofferzon M-L, Nilsson A. Predictors of return to work among women with long-term neck/shoulder and/or back pain: A 1-year prospective study. PLoS ONE. 2021;16(11): e0260490.
Cancelliere C, Donovan J, Stochkendahl MJ, Biscardi M, Ammendolia C, Myburgh C, et al. Factors affecting return to work after injury or illness: best evidence synthesis of systematic reviews. Chiropr Man Therap. 2016;24(1):32.
Kausto J, Pentti J, Oksanen T, Virta LJ, Virtanen M, Kivimäki M, et al. Length of sickness absence and sustained return-to-work in mental disorders and musculoskeletal diseases: A cohort study of public sector employees. Scand J Work Environ Heal. 2017;43(4):358–66.
Bosman LC, Twisk JWR, Geraedts AS, Heymans MW. Development of prediction model for the prognosis of sick leave due to low back pain. J Occup Environ Med. 2019;61(12):1065–71.
Brendbekken R, Vaktskjold A, Harris A, Tangen T. Predictors of return-to-work in patients with chronic musculoskeletal pain: a randomized clinical trial. J Rehabil Med. 2018;50(2):193–9.
Hara KW, Bjørngaard JH, Jacobsen HB, Borchgrevink PC, Johnsen R, Stiles TC, et al. Biopsychosocial predictors and trajectories of work participation after transdiagnostic occupational rehabilitation of participants with mental and somatic disorders: a cohort study. BMC Public Health. 2018;18(1):1014.
Gragnano A, Villotti P, Larivière C, Negrini A, Corbière M. A Systematic search and review of questionnaires measuring individual psychosocial factors predicting return to work after musculoskeletal and common mental disorders. J Occup Rehabil. 2021;31(3):491–511.
Halty LS, Hüttner MD, de Oliveira NettoSantosMartins ICVAG. Análise da utilização do Questionário de Tolerância de Fagerström (QTF) como instrumento de medida da dependência nicotínica. J Pneumol. 2002;28(4):180–6.
Figlie NB, Pillon SC, Laranjeira RR, Dunn J. Audit indentifica a necessidade de interconsulta específica para dependentes de álcool no hospital geral? J Bras Psiquiatr. 1997;46(11):589–93.
Chor D, Werneck GL, Faerstein E, de Alves MG M, Rotenberg L. The Brazilian version of the effort-reward imbalance questionnaire to assess job stress. Cad Saude Publica. 2008;24(1):219–24.
Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Application of the Portuguese version of the abbreviated instrument of quality life WHOQOL-bref. Rev Saude Publica. 2000;34(2):178–83.
Rysstad T, Grotle M, Aasdahl L, Dunn KM, Tveter AT. Identification and characterisation of trajectories of sickness absence due to musculoskeletal pain: a 1-year population-based study. J Occup Rehabil. 2023;33(2):277–87.
Frontera WR. Physiologic changes of the musculoskeletal system with aging: a brief review. Phys Med Rehabil Clin N Am. 2017;28(4):705–11.
Azevedo LM, Chiavegato LD, Carvalho CRF, Braz JR, Nunes Cabral CM, Padula RS. Are blue-collar workers more physically active than white-collar at work? Arch Environ Occup Health. 2021;76(6):338–47.
Dubert T, Girault C, Rozenblat M, Dorey J, Dubert-Khalifa H, Katz G. Impact of patient-surgeon relationship on patient’s return to work. J Bone Joint Surg Am. 2019;101(15):1366–74.
Ilmarinen JE. Aging workers. Occup Environ Med. 2001;58(8):546–52.
American Psychiatric Association. Manual Diagnóstico e Estatístico de Transtornos Mentais. 5th ed. Porto Alegre: Artmed; 2014.
Acknowledgements
The authors would like to thank the National Social Security Institute (Instituto Nacional do Seguro Social—INSS) of Brazilian Social Security Ministry for granting permission to conduct the study in the institute´s physical premises; and the Brazilian National Council for Scientific and Technological Development (Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq) for financial support.
Funding
CBM received funding by the Brazilian National Council for Scientific and Technological Development (Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq) – protocol 304375/2017–9; FMF received two fundings by CNPq (protocol 2018–9; and 306963/2021–3).
Author information
Authors and Affiliations
Contributions
JSSJ made a substantial contribution to the concept and design of the work, acquisition, analysis and interpretation of data; and drafted the article. MCM, CBM and FMF made a substantial contribution to the concept and design of the work; and revised it critically for important intellectual content. FSS made a substantial contribution to the interpretation of data; and drafted the article. All authors approved the version to be published and take public responsibility for appropriate portions of the content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the Declaration of Helsinki and all methods were carried out in accordance with relevant guidelines and regulations. The research project was approved by the Ethics Committee for Research on Human Beings of the School of Public Health of the University of São Paulo (opinion report no. 3,166,922/2019; CAEE 87446718.9.0000.5421). Workers who voluntarily agreed to participate signed a free and informed consent statement before the invitation to answer the online questionnaires.
Consent for publication
Informed consent was obtained from all the participants to publish their information collected during research in an online open-access publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Silva-Junior, J.S., Martinez, M.C., Sekiya, F.S. et al. Return to work after sick leave due to musculoskeletal disorder or injury: a longitudinal study conducted in Brazil. BMC Public Health 23, 1881 (2023). https://doi.org/10.1186/s12889-023-16789-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16789-z