
Abstract
Objective
To investigate the impact of the COVID-19 pandemic on life expectancy at birth (e0) for 51 Asian countries and territories from January 1, 2020 to December 31, 2021.
Method
Based on age-sex-specific mortality used for estimating the changes in e0 for years 2019, 2020, and 2021 from the 2022 revision of the World Population Prospects, we employed Arriaga’s discrete method to decompose changes in e0 into both absolute and relative contributions of changes in age-specific death rate, and further obtained the age-sex-specific contribution to changes in e0 by country/territory and period (i.e., 2019–2020 and 2020–2021) for Asia.
Findings
The COVID-19 pandemic reduced 1.66 years in e0 of the Asian population from 2019 to 2021, slightly lower than the world average of 1.74 years. South Asia had a high loss of 3.01 years, whereas Eastern Asia had almost no changes. Oman, Lebanon, India, Armenia, Azerbaijan, Indonesia, and the Philippines experienced a high loss of above 2.5 years in e0. Despite significant national and territorial variations, the decline of e0 in Asia was mostly from the age group of 60–79 years, followed by age groups of 80 + and 45–59 years; and age groups of children contributed little (i.e., 0–4 and 5–14 years old). Males suffered more losses than females in this pandemic. Asian nations saw less loss in e0 in the second year of the pandemic, i.e., 2020–2021, than in the first year, i.e., 2019–2020, but this recovery trend was not observed in Southern Asia and South-Eastern Asia. Countries from Central Asia and Western Asia, such as Kazakhstan, Armenia, Azerbaijan, Lebanon, and Oman, had extraordinarily more losses in e0 in the first year at ages around 70.
Conclusion
The COVID-19 pandemic had significantly affected e0 of Asian populations, and most contribution to the reduction of e0 came from the three older age groups, 60–79 years, 80 + years, and 45–59 years, with great variations across countries/territories. Our findings could have important implications for development of more resilient public health systems in Asian societies with better policy interventions for vulnerable demographic groups.
Similar content being viewed by others


Introduction
The COVID-19 pandemic has lasted more than three years, with the official death toll of 6.84 million as of 16 February of 2023 [1]. This number, however, likely underestimates the true impact of COVID-19 on mortality, due to challenges in accurately identifying COVID-19-relateds deaths, incomplete registration systems in many countries and areas, and the undercounting of deaths indirectly caused by the pandemic. The inconsistent definitions of COVID-19 deaths across countries further prevent the use of official statistics for international comparisons [2, 3].
The use of excess deaths could address these limitations, which reveals the number of deaths exceeding the expected level projected in the absence of this pandemic [3]. According to the World Health Organization (WHO) and the United Nations Department of Economic and Social Affairs (UN DESA) joint Technical Advisory Group for COVID Mortality Assessment (thereafter WHO-UN COVID TAG) [3, 4], excess deaths not only encompass fatalities directly attributed to the COVID-19 virus but also account for indirect deaths resulting from factors such as limited access to medical care during outbreaks, as well as the reduced mortality due to fewer cases of seasonal influenza, traffic accidents, or occupational injuries during the pandemic [3]. The WHO-UN COVID TAG reported the number of global excess deaths due to the COVID pandemic was 14.9 million in 2020 and 2021, nearly three times the official death toll [3].
The COVID-19-related mortality varies by age and sex [3, 5,6,7,8,9], and such associations also change by the pandemic stage [10,11,12,13]. The sheer number of excess deaths is thus affected by the age and sex structures of a given population, making a direct comparison between nations and territories less meaningful. Calculating changes in sex-specific life expectancy during the pandemic may be more appropriate as it is independent of population age and sex structures. This method is suitable for international comparisons and provides insights into the impact of COVID-19 on mortality [10].
A large number of studies have estimated changes of life expectancy in this pandemic [14,15,16,17,18,19,20,21]. By incorporating the WHO-UN TAG’s age- and sex-specific estimates for excess deaths for each country, the 2022 revision of the World Population Prospects (thereafter WPP 2022) by the UN DESA, Population Division, reveals a global decrease of 1.74 years in life expectancy at birth (e0) for both sexes from 2019 to 2021, with 1.80 years for males and 1.61 years for females, respectively [9]. Such declines were primarily attributable to the increased mortality among individuals aged 60 or older with 65% for males and 72% for females [10].
To our knowledge, only two studies have thus far examined changes in life expectancy during the pandemic and analyzed the variations by age and sex for Asia and its countries and territories [10, 22]. However, one focused solely on the changes in life expectancy at age 60 [10], whereas the other only investigated the changes in e0 for India in 2020 [22]. An examination of the age-sex-specific contribution to changes of e0 for Asian countries and territories could help fill the gap and shed light on understanding how the pandemic affected human mortality differently in Asian populations and help identify vulnerable groups for policy interventions. Moreover, as Asian countries and territories differed significantly during the pandemic in vaccination and containment policies [3, 4, 23,24,25] with varying infection rates and vaccination rates at different stages of the pandemic [11, 26,27,28,29], further analyses by region and period are necessary. Based on the WPP 2022 estimates, this study decomposed the changes in e0 from 2019 to 2021 to show the age-sex-specific contribution by region, country and territory, and period (i.e., the years 2020 and 2021) for Asia.
Methods
The age-sex-specific mortality that were used for estimating the changes in e0 in 51 Asian countries and territories for years 2019, 2020, and 2021 were obtained from WPP 2022 [9]. WPP 2022 incorporated the WHO-UN COVID TAG estimates on excess deaths from the COVID-19 pandemic for all countries of the world in 2020 and 2021 [4, 9, 18]. The detailed methodologies used by the WHO-UN COVID TAG and the WPP 2022 estimates are available on the WHO website [4] and the UNDESA Population Division website [9, 30, 31]. With these annual age-sex-specific mortality schemes, we employed the widely used Arriaga’s discrete method [20, 32] to decompose the changes in e0 into both absolute and relative contributions of changes in age-specific death rates between two time points [33]. The formula is as follows:
where l0 denotes the life table radix, and lx refers to the number of survivors at the exact age x given the radix l0; Lx denotes the number of person-year lived at age x; Tx refers to the number of cumulative person-year lived at age x and beyond; e0 denotes the number of years of life expectancy at birth; and (\(\omega -1)\) presents the last age group (i.e., 100 + years in this study). The first component in the right side of the equation \(\frac{{l}_{x}^{t1}}{{l}_{0}^{t1}}\left(\frac{{L}_{x}^{t2}}{{l}_{x}^{t2}}-\frac{{L}_{x}^{t1}}{{l}_{x}^{t1}}\right)\) refers to the number of years of the direct contribution of mortality change at age x to the changes in e0, whereas the second part \(\frac{{T}_{x+1}^{t2}}{{l}_{0}^{t1}}(\frac{{l}_{x}^{t1}}{{l}_{x}^{t2}}- \frac{{l}_{x+1}^{t1}}{{l}_{x+1}^{t2}})\) represents the number of years of the indirect contribution of mortality change at age x to the changes in e0. For the last age group (\(\omega -1)\), there is no second component. After calculating the contribution of each age from Eq. (1), we further calculated the cumulative contribution to the changes in e0 for any age range and the relative contributions of each age (or any age range).
In the present study, we presented both the annual and the biennial sex-specific absolute and relative contributions by mortality changes for age groups of 0–4, 5–14, 15–44, 45–59, 60–79, and 80 + years to changes in e0 from January 1, 2020 to December 31, 2021.
Results
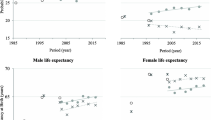
Figure 1 shows that e0 for both sexes combined had a decline in 2021 for the world and in most regions compared to 2019, with a reduction of 1.74 years for the world and a reduction of 1.66 years for Asia. Within Asia, Southern Asia and South-Eastern Asia declined by 3.01 and 2.03 years, respectively; by contrast, e0 in Eastern Asia increased slightly.

Life expectancy at birth for the world, regions, and the subregions of Asia, both sexes combined, 2019 and 2021
Table 1 displays age-sex-specific contributions to the changes in e0 from 2019 to 2021 by region. The global e0 experienced a decline by 1.6 and 1.8 years for females and males, respectively, most of which came from the age groups of 60–79 (0.8 years for females and 0.9 years for males) and 45–59 (0.4 years for females and 0.5 years for males). This pattern is generally applicable to Asia. With an exception for Eastern Asia, the age pattern of contribution to changes in e0 was similar across Asian subregions, although their magnitudes of contribution varied by different age groups.
We then calculated the age-specific contributions to the changes in e0 for each of all 51 Asian countries and territories from 2019 to 2021 (Fig. 2). For the six age groups analyzed (i.e., 0–4, 5–14, 15–44, 45–59, 60–79, and 80 + years), the most contribution to the reduction in e0 was primarily from ages 60–79 years, followed by the age groups 80 + and 45–59 years. The first two age groups (i.e., 0–4 and 5–14 years) made a very limited contribution to the reduction in e0, and in some cases, the mortality rate in age group 0–4 years witnessed even an improvement, which positively contributed to e0.

Contributed years to changes in life expectancy at birth (e0) by age group and sex for Asian country/territory classified by subregion, 2019–2021
A significant variation in the age pattern of contribution to changes in e0 was observed, however. Among Asia’s 51 countries and territories, Oman, Lebanon, India, Armenia, Azerbaijan, Indonesia, and the Philippines stood out with the largest decrease in e0 ,with above 2.5 years from 2019 to 2021, whereas almost all Eastern Asian countries and territories saw a relatively minor change in e0. For most countries in Asia, high mortality rates among older adults in the age group of 60–79 years usually contributed the most to the reduction in e0; however, Singapore, Thailand, and the Republic of Korea were exceptional, where the age group of 80 + years played a major role. It is also noteworthy that, among the countries with the largest decline in e0, the age group of 45–59 years made a sizeable contribution, especially in males.
Furthermore, within Asian subregions, the age-specific contribution to the changes in e0 also varied considerably. Taking South-Eastern Asia countries (or the Association of South-East Asian Nations, ASEAN) as an example, Indonesia and the Philippines had the largest reduction in e0 with 2.5–3.0 years losses for both sexes combined. The attributable reduction in e0 by 45–59 years in these two ASEAN countries was sizeable, around 20–30% for males, females, and two sexes combined. By contrast, the reduction in e0 in Singapore was primarily from increased mortality at ages 80 years and beyond; and the total reduction in e0 in Brunei Darussalam and the Lao People’s Democratic Republic was very minor. Another example is in Western Asia: the male mortality for ages 15–44 years in Syrian Arab Republic decreased due to the temporary ceasefire, contributed 1.2 years to e0 in 2021 compared to 2019, while mortality rate in the same age group in Oman and Lebanon witnessed a substantial increase, contributed 0.6 and 0.4 years to their respective e0 in 2019-2021.
Table 2 compares the changes in e0 in the two periods: 2019–2020 and 2020–2021 for 51 Asian countries and remaining 149 countries of the world. In the first year of the pandemic (i.e., 2019–2020), about 20% of the 51 Asian countries and territories experienced a reduction of more than 1.5 years in e0 for both males and females, compared to the previous year; in the second year of the pandemic (i.e., 2020–2021), this figure fell considerably to approximately 10%. Meanwhile, the proportion of countries with e0 increasing more than 0.3 years in the second year almost doubled, rising from approximately 10% (5 countries) to 20% (10 countries). A further check shows that such e0 increases in the second year among these 10 Asian countries were mainly driven by the reduced reduction in mortality in the age group of 60–79 years, which accounted for nearly half of the increase in e0. The patterns presented above suggest that the excess mortality observed in Asian countries and territories during the first year was reduced in the second year.
Table 2 also shows the rest part of the world, which did not see the exactly same pattern as Asia. Among the 149 non-Asian countries and territories of the world, about 10% underwent declines in e0 by more than 1.5 years in the first year, and this number almost doubled in the second year. But similar to Asia, as compared to the first year of the pandemic, the number of countries and territories with growing e0 increased in the second year.
Figure 3 further presents contributed years to the changes in e0 in 2019–2020, 2020–2021, and 2019–2021 for the world, regions, and Asian subregions by sex and age group, respectively. The graph clearly reveals that the changes in e0 varied greatly across different age groups, regions of the world, and subregions of Asia, and between the two periods ( 2019–2020 vs 2020–2021). Across the world, the first year of the pandemic usually witnessed more losses in e0 than the second year; however, an opposite pattern was observed for Southern Asia and South-Eastern Asia, both of which experienced more losses in the second year. In addition, Central Asia and Western Asia experienced significantly big losses in the first year at ages around 70 years for both females and males. Figure 3 further shows that the reduction in e0 in the second year was still mainly driven by the age groups from 60–64 to 75–79 years. These age groups accounted for nearly half of the reduction, although such shares reached 70–80% in the first year. With few exceptions, males and females shared similar age-specific reduction patterns within each region or subregion. A more or less similar pattern was also found in most Asian countries or territories (see Figure A1 in Appendix).

Contributed years to changes in life expectancy at birth (e0) by age group, sex, region, and period (2019–2020, 2020–2021, and 2019–2021)
Table 3 shows the male-to-female sex ratio of the reductions in e0 from 2019 to 2021 and the sex ratio of these reductions to e0 in 2019. The sex ratios for the world and all continents were greater than 1, suggesting that males experienced greater losses in e0 than females in both absolute and relative terms. Among Asian subregions, except for Eastern Asia and Central Asia, all other subregions had a sex ratio greater than 1 as well.
Discussion
The COVID-19 pandemic has imposed disastrous impacts on life and health of human beings worldwide. The global reduction in life expectancy in this pandemic may cause the first interruption of the increasing trend of global life expectancy since the year of 1950 [18]. As the world is currently seeing a gradual transition to the post-pandemic era, now comes a good timing to evaluate the impact of this pandemic on population health. By using the latest revision of WPP 2022 released by the United Nations, and focusing on Asia, the most populous continent in the world, this paper analyzed how different sexes and age groups contributed to changes in e0 during the pandemic, at different periods, for its subregions, and for 51 Asian countries and territories.
As revealed by this study, although Asia as a whole had a relatively smaller loss in e0 from 2019 to 2021 compared to other continents, Southern Asia suffered one of the largest losses in e0 in the world. Meanwhile, there was a great variation within Asia; in contrast to Southern Asia, Eastern Asia appeared to be one of the least affected regions in the world for the first two years of the pandemic. To elucidate the impact of COVID-19 on Asian populations, this study conducted the age-sex-specific decomposition of the changes in e0. Similar to other parts of the world, we found that the greatest reduction in e0 among Asian populations was primarily attributable to the mortality increase in the age group of 60–79 years, followed by two age groups of 80 + and 44–59 years.
The disproportionate impact that the COVID-19 pandemic has had on various communities underscores the need for a well-functioning public health system. As COVID-19 virus proves to be more threatening toward people at older ages and males, who are biologically frailer in the immune system [34], many deaths in the young older age group (65-79 years) and the adulthood group (15-59 years) should be preventable given a more robust and effective public health system. As shown in our analysis, the e0 reduction in Singapore, renowned for its advanced healthcare system [35], concentrated on the oldest-old populations. As suggested in literature, to response to this pandemic depends on the promptness of public interventions like lockdown enforcement and mass vaccination [36,37,38,39]. The pandemic also brought to the fore the strain on healthcare resources when medical services were overwhelmingly directed toward COVID-19 patients [40], and older adults may suffer from chronic conditions such as diabetes, heart disease, and chronic respiratory illnesses in many countries [41,42,43]. An effective healthcare system should respond relatively well to these challenges or crises, as shown by the good performance of Eastern Asian countries in our analysis. In this sense, our results align with previous studies highlighting the importance of healthcare accessibility and resource availability within the public health system in mitigating reduction of life expectancy during a pandemic [44, 45].
The effort of this study to reveal how the COVID pandemic impact was distributed among different age and sex groups provides useful clues to identify vulnerable demographic groups for policy interventions. Yet, further investigations are also needed to expand to include more factors. Plenty of evidence from different populations and geographic regions suggested that COVID-19 infections and mortality risk were associated with both macro-level factors (such as development levels, poverty, capacity of public healthcare system, healthcare equity, environmental characteristics, population density and composition, policy responses, vaccination coverage, culture) and individual factors (such as age, sex, socioeconomic status, race/ethnicity, lifestyles, health literacy, disease conditions) [5, 34, 46,47,48,49,50,51,52,53]. Understanding more of these affecting factors would help to prevent a natural disaster from turning into a social disaster, a key lesson the world could learn from this COVID pandemic [54]. In addition, the future analyses of the COVID-19 mortality impact, if considering a country or territory’ specific stage of epidemiological transition or demographic transition, could obtain extra theoretical and practical significance. Lastly, plenty of literature on the COVID impact on life expectancy did not pay much attention to the period difference. By comparing the two periods, 2019–2020 and 2020–2021, this study presented interesting temporal patterns of age-sex-specific contributions to the changes in e0. We highly recommend future studies incorporate this important dimension in analysis.
This study has a few limitations. The data on the impacts of this pandemic on human life expectancy remains incomplete by far, owing to gaps and time lags in data collection and dissemination. Despite these challenges, WPP 2022 still accounted for the impact of the COVID-19 pandemic on population and demographic estimates with the latest available evidence for the years 2020 and 2021. There is an ongoing debate on the methodology and the outcome of excess deaths in this field [55], and the WPP estimates of excess deaths due to the COVID-19 pandemic still needs to be further improved with more data sources available in its 2024 Revision. As a result, the full impact of the pandemic on demographic and socioeconomic domains may not be known unless the data limitations and methodological debate are solved. Second, this study did not cover the most recent development of the COVID pandemic in Asia for the year 2022. The significant rise of COVID cases in Eastern Asian nations is not discussed, especially the recent relaxation of China’s COVID policy since the late 2022 [56, 57]. A complete report on the impact of the COVID-19 pandemic on life expectancy in Asia is expected to be done in the near future.
Availability of data and materials
The life tables used in this data are from the World Population Prospects 2022. United Nations, Department of Economic and Social Affairs, Population Division, New York. They can be downloaded at https://population.un.org/wpp/.
References
World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2003. Available from: https://covid19.who.int. [Cited 2023 Feb 17].
Karlinsky A, Kobak D. The World Mortality Dataset: Tracking excess mortality across countries during the COVID-19 pandemic. eLife. 2021;10:e69336. https://doi.org/10.7554/eLife.69336.
World Health Organization. Global excess deaths associated with COVID-19, January 2020 - December 2021. 2022. Available from: https://www.who.int/data/stories/global-excess-deaths-associated-with-covid-19-january-2020-december-2021. [Cited 2022 July 2].
World Health Organization. Methods for Estimating The Excess Mortality Associated with the COVID-19 Pandemic. 2022. Available from: https://www.who.int/publications/m/item/methods-for-estimating-the-excess-mortality-associatedwith-the-covid-19-pandemic. [Cited 2022 July 2].
Dowd JB, Andriano L, Brazel DM, Rotondi V, Block P, Ding X, et al. Demographic science aids in understanding the spread and fatality rates of COVID-19. Proc Natl Acad Sci. 2020;117(18):9696–8. https://doi.org/10.1073/pnas.2004911117.
Elo IT, Luck A, Stokes AC, Hempstead K, Xie W, Preston SH. Evaluation of age patterns of COVID-19 mortality by race and ethnicity from March 2020 to October 2021 in the US. JAMA Netw Open. 2022;5(5):e2212686. https://doi.org/10.1001/jamanetworkopen.2022.12686.
García-Guerrero VM, Beltrán-Sánchez H. Heterogeneity in excess mortality and its impact on loss of life expectancy due to covid-19: Evidence from Mexico. Can Stud Popul. 2021;48(2):165–200. https://doi.org/10.1007/s42650-021-00051-1.
PifarréiArolas H, Acosta E, López-Casasnovas G, Lo A, Nicodemo C, Riffe T, et al. Years of life lost to COVID-19 in 81 countries. Sci Rep. 2021;11(1):1–6. https://doi.org/10.1038/s41598-021-83040-3.
United Nations. World Population Prospects 2022: Summary of Results. United Nations, 2022. (Statistical Papers - United Nations (Ser. A), Population and Vital Statistics Report). Available from: https://population.un.org/wpp/Publications/Files/WPP2022_Methodology.pdf [Cited 2023 Feb 17].
Feng Q, Gu D. The COVID-19 pandemic and life expectancy among older adults in Asian countries. Asian Popul Stud. 2023;19(2):168–83. https://doi.org/10.1080/17441730.2023.2193483.
Ioannidis JPA, Axfors C, ContopoulosIoannidis DG. Second versus first wave of COVID-19 deaths: Shifts in age distribution and in nursing home fatalities. Environ Res. 2021;195:110856. https://doi.org/10.1016/j.envres.2021.110856.
James N, Menzies M, Radchenko P. COVID-19 second wave mortality in Europe and the United States. Chaos Interdiscip J Nonlinear Sci. 2021;31(3):031105. https://doi.org/10.1063/5.0041569.
Yao L, Graff JC, Aleya L, Ma J, Cao Y, Wei W, et al. Mortality in four waves of COVID-19 is differently associated with healthcare capacities affected by economic disparities. Trop Med Infect Dis. 2022;7(9):241. https://doi.org/10.3390/tropicalmed7090241.
Aburto JM, Kashyap R, Schöley J, Angus C, Ermisch J, Mills MC, et al. Estimating the burden of the COVID-19 pandemic on mortality, life expectancy and lifespan inequality in England and Wales: a population-level analysis. J Epidemiol Community Health. 2021;75(8):735–40. https://doi.org/10.1136/jech-2020-215505.
Aburto JM, Schöley J, Kashnitsky I, Zhang L, Rahal C, Missov TI, et al. Quantifying impacts of the COVID-19 pandemic through life-expectancy losses: a population-level study of 29 countries. Int J Epidemiol. 2022;51(1):63–74. https://doi.org/10.1093/ije/dyab207.
Castro MC, Gurzenda S, Turra CM, Kim S, Andrasfay T, Goldman N. Reduction in life expectancy in Brazil after COVID-19. Nat Med. 2021;27(9):1629–35. https://doi.org/10.1038/s41591-021-01437-z.
Chan EYS, Cheng D, Martin J. Impact of COVID-19 on excess mortality, life expectancy, and years of life lost in the United States. Bikbov B, editor. PLOS One. 2021;16(9):e0256835. https://doi.org/10.1371/journal.pone.0256835.
Heuveline P. Global and national declines in life expectancy: An end-of-2021 assessment. Popul Dev Rev. 2022;48(1):31–50. https://doi.org/10.1111/padr.12477.
Trias-Llimós S, Riffe T, Bilal U. Monitoring life expectancy levels during the COVID-19 pandemic: Example of the unequal impact of the first wave on Spanish regions. Navaneetham K, editor. PLOS One. 2020;15(11):e0241952. https://doi.org/10.1371/journal.pone.0241952.
Masters RK, Woolf SH, Aron LY. Age-specific mortality during the 2020 COVID-19 Pandemic and life expectancy changes in the United States and peer countries, 1980–2020. J Gerontol Ser B. 2022;77(Supplement_2):S127-37. https://doi.org/10.1093/geronb/gbac028.
Woolf SH, Masters RK, Aron LY. Effect of the covid-19 pandemic in 2020 on life expectancy across populations in the USA and other high income countries: simulations of provisional mortality data. BMJ. 2021;373:n1343. https://doi.org/10.1136/bmj.n1343.
Yadav S, Yadav PK, Yadav N. Impact of COVID-19 on life expectancy at birth in India: a decomposition analysis. BMC Public Health. 2021;21(1):1906. https://doi.org/10.1186/s12889-021-11690-z.
Chen SX, Lam BC, Liu JH, Choi HS, Kashima E, Bernardo AB. Effects of containment and closure policies on controlling the COVID-19 pandemic in East Asia. Asian J Soc Psychol. 2021;24(1):42–7. https://doi.org/10.1111/ajsp.12459.
Djalante R, Nurhidayah L, Van Minh H, Phuong NTN, Mahendradhata Y, Trias A, et al. COVID-19 and ASEAN responses: Comparative policy analysis. Prog Disaster Sci. 2020;8:100129. https://doi.org/10.1016/j.pdisas.2020.100129.
Furceri D, Kothari S, Zhang L. The effects of COVID-19 containment measures on the Asia-Pacific region. Pac Econ Rev. 2021;26(4):469–97. https://doi.org/10.1111/1468-0106.12369.
Moradhvaj KCS. Impact of the COVID-19 pandemic on the age-sex pattern of COVID-19 deaths in India. Asian Popul Stud. 2023;19(2):148–67. https://doi.org/10.1080/17441730.2023.2193077.
Arjun MC, Singh AK, Roy P, Ravichandran M, Mandal S, Pal D, et al. Long COVID following Omicron wave in Eastern India—A retrospective cohort study. J Med Virol. 2023;95(1):e28214. https://doi.org/10.1002/jmv.28214.
Jones GW. Impact of COVID-19 on mortality in Asia. Asian Popul Stud. 2023;19(2):131–47. https://doi.org/10.1080/17441730.2023.2193476.
Matsunaga N, Hayakawa K, Asai Y, Tsuzuki S, Terada M, Suzuki S, et al. Clinical characteristics of the first three waves of hospitalised patients with COVID-19 in Japan prior to the widespread use of vaccination: a nationwide observational study. Lancet Reg Health West Pac. 2022;22:100421. https://doi.org/10.1016/j.lanwpc.2022.10042.
United Nations. World Population Prospects - Population Division - United Nations. 2022. Available from: https://population.un.org/wpp/. [Cited 2022 Dec 3].
United Nations. World Population Prospects 2022: Methodology of the United Nations population estimates and projections. United Nations; 2022. (Statistical Papers - United Nations (Ser. A), Population and Vital Statistics Report). Available from: https://population.un.org/wpp/Publications/Files/WPP2022_Methodology.pdf [Cited 2023 Feb 17].
Arriaga EE. Measuring and explaining the change in life expectancies. Demography. 1984;21(1):83–96. https://doi.org/10.2307/2061029.
Preston SH, Heuveline P, Guillot M. Demography-Measuring and Modeling population Processes. Oxf Blackwell Publ, 2001.
Ciarambino T, Para O, Giordano M. Immune system and COVID-19 by sex differences and age. Womens Health. 2021;17:17455065211022262. https://doi.org/10.1177/17455065211022262.
Healthcare in Singapore. In: Wikipedia. 2023. Available from: https://en.wikipedia.org/w/index.php?title=Healthcare_in_Singapore&oldid=1138890306 [Cited 2023 Feb 23].
Haldane V, De Foo C, Abdalla SM, Jung AS, Tan M, Wu S, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27(6):964–80. https://doi.org/10.1038/s41591-021-01381-y.
Sagan A, Erin W, Dheepa R, Marina K, Scott LG. Health system resilience during the pandemic: It’s mostly about governance. Eurohealth. 2021;27(1):10–5.
Cheng ZJ, Zhan Z, Xue M, Zheng P, Lyu J, Ma J, et al. Public Health Measures and the Control of COVID-19 in China. Public Health Measures and the Control of COVID-19 in China. Clin Rev Allergy Immunol. 2023;64(1):1–16. https://doi.org/10.1007/s12016-021-08900-2.
Gianfredi V, Pennisi F, Lume A, Ricciardi GE, Minerva M, Riccò M, et al. Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature. Vaccines. 2021;9(6):574. https://doi.org/10.3390/vaccines9060574.
Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J Pers Med. 2022;12(8):1295. https://doi.org/10.3390/jpm12081295.
Chin MH. Uncomfortable Truths—What Covid-19 Has Revealed about Chronic-Disease Care in America. N Engl J Med. 2021;385(18):1633–6. https://doi.org/10.1056/NEJMp2112063.
Edge R, Meyers J, Tiernan G, Li Z, Schiavuzzi A, Chan P, et al. Cancer care disruption and reorganisation during the COVID-19 pandemic in Australia: A patient, carer and healthcare worker perspective. PLOS One. 2021;16(9):e0257420. https://doi.org/10.1371/journal.pone.0257420.
Kendzerska T, Zhu DT, Gershon AS, Edwards JD, Peixoto C, Robillard R, et al. The effects of the health system response to the COVID-19 pandemic on chronic disease management: a narrative review. Risk Management and Healthcare Policy. 2021;14:575–84. https://doi.org/10.2147/RMHP.S293471.
Ji Y, Ma Z, Peppelenbosch MP, Pan Q. Potential association between COVID-19 mortality and health-care resource availability. Lancet Glob Health. 2020;8(4):e480. https://doi.org/10.1016/S2214-109X(20)30068-1.
Tchicaya A, Lorentz N, Leduc K, de Lanchy G. COVID-19 mortality with regard to healthcare services availability, health risks, and socio-spatial factors at department level in France: a spatial cross-sectional analysis. PLOS One. 2021;16(9):e0256857. https://doi.org/10.1371/journal.pone.0256857.
Banik A, Nag T, Chowdhury SR, Chatterjee R. Why Do COVID-19 Fatality rates differ across countries? An explorative cross-country study based on select indicators. Glob Bus Rev. 2020;21(3):607–25. https://doi.org/10.1177/0972150920929897.
Garenne MM. COVID-19 and socioeconomic development in Africa: The first 6 months (February 2020-August 2020). Int J Popul Stud. 2020;6(2):1–14. https://doi.org/10.18063/ijps.v6i2.12221.
Jinjarak Y, Ahmed R, Nair-Desai S, Xin W, Aizenman J. Accounting for global COVID-19 diffusion patterns, January–April 2020. Econ Disasters Clim Change. 2020;4(3):515–59. https://doi.org/10.1007/s41885-020-00071-2.
Kashnitsky I, Aburto JM. COVID-19 in unequally ageing European regions. World Dev. 2020;136:105170. https://doi.org/10.1016/j.worlddev.2020.105170.
Millett GA, Jones AT, Benkeser D, Baral S, Mercer L, Beyrer C, et al. Assessing differential impacts of COVID-19 on black communities. Ann Epidemiol. 2020;47:37–44. https://doi.org/10.1016/j.annepidem.2020.05.003.
Pal R, Yadav U, Grover S, Saboo B, Verma A, Bhadada SK. Knowledge, attitudes and practices towards COVID-19 among young adults with Type 1 Diabetes Mellitus amid the nationwide lockdown in India: A cross-sectional survey. Diabetes Res Clin Pract. 2020;166:108344. https://doi.org/10.1016/j.diabres.2020.108344.
Polyakova M, Udalova V, Kocks G, Genadek K, Finlay K, Finkelstein AN. Racial disparities in excess all-cause mortality during the early COVID-19 Pandemic varied substantially across states. Health Aff. 2021;40(2):307–16. https://doi.org/10.1377/hlthaff.2020.02142.
Tajvar A, Aghamolaei T, Mohseni S, Fakherpour A, Damiri Z, Jahangiri M, et al. Knowledge, performance, and attitude towards mask use to prevent and control COVID-19 outbreak among a group of Iranian people: A cross-sectional study. Shiraz E-Med J. 2021;22(11):e111491. https://doi.org/10.5812/semj.111491.
Fakhruddin B SHM, Blanchard K. Ragupathy D Are we there yet? The transition from response to recovery for the COVID-19 pandemic. Prog Disaster Sci. 2020;7:100102. https://doi.org/10.1016/j.pdisas.2020.100102.
Moeti M, Makubalo L, Gueye AS, Balde T, Karamagi H, Awandare G, et al. Conflicting COVID-19 excess mortality estimates. The Lancet. 2023;401(10375):431. https://doi.org/10.1016/S0140-6736(23)00112-5.
Leung K, Leung GM, Wu JT. Modelling the adjustment of COVID-19 response and exit from dynamic zero-COVID in China. medRxiv; 2022. https://doi.org/10.1101/2022.12.14.22283460. Available from: https://www.medrxiv.org/content/10.1101/2022.12.14.22283460v1 [Cited 2023 Feb 23].
Liu J, Ding F, Wu Y, Jing W, Yan W, Qin C, et al. Vital surveillances: Trends of SARS-CoV-2 infection in sentinel community-based surveillance after the optimization of prevention and control measures — China, December 2022–January 2023. China CDC Weekly. 2023;5(7):159–64. https://doi.org/10.46234/ccdcw2023.028.
Acknowledgements
None
Disclaimer
Views expressed in the paper are solely those of the authors and do not necessarily reflect those of the National University of Singapore or the United Nations.
Funding
None.
Author information
Authors and Affiliations
Contributions
YM, QF, and DG drafted the paper. QF and DG revised the paper. DG performed the analysis and grants the accuracy of the results.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable as the data used for this study are aggregations at country-level and are publicly available.
Consent to publish
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix Figure A1.
Contributed years to the changes in life expectancy at birth (e0) by age group and Asian country/territory, both sexes combined, 2019-2021
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mo, Y., Feng, Q. & Gu, D. Impacts of the COVID-19 pandemic on life expectancy at birth in Asia. BMC Public Health 23, 1508 (2023). https://doi.org/10.1186/s12889-023-16426-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-16426-9