
Abstract
Background
Prostate cancer is the leading cause of cancer death in Ecuadorian men. However, there is a lack of information regarding the evolution of prostate cancer mortality rates in Ecuador and its regions in the last few decades.
Objective
The aim of this study was to report prostate cancer mortality rates in Ecuador and its geographical areas and observe the evolution of these rates between 2004 and 2019.
Methods
An observational ecological study was conducted, analysing data for prostate cancer deaths from 2004 to 2019 in Ecuador. Age standardized mortality rates (ASMR) were calculated per 100,000 men using the world standard population with the direct method proposed by SEGI. Joinpoint regression analysis was performed to examine mortality trends. We used a Cluster Map to explore relationships among regions between 2015 and 2019.
Results
Ecuador reported 13,419 deaths by prostate cancer between 2004 and 2019, with the Coastal region accounting for 49.8% of the total deaths. The mean age at death was 79 years (± 10 years), 91.7% were elderly (more than 65 years old) and had primary education (53%). Deaths by prostate cancer were more frequently reported among mestizos (81.4%). There were no significant variations in these percentages in Ecuador and its regions during the study period. Carchi province had the highest mortality rate in 2005 and 2019 (> 13 deaths per 100,000). Heterogeneity in the evolution of mortality rates was reported among the provinces of Ecuador. Azuay decreased in the first few years, and then increased from 2010 to 2019, whereas Guayas and Pichincha decreased throughout the whole period.
Conclusion
Although prostate cancer mortality rates in Ecuador have remained stable over the past few decades, there are significant disparities among the different regions. These findings suggest the need for the development of national and provincial registration measures, integrated healthcare actions, and targeted interventions to reduce the burden of prostate cancer in the Ecuadorian population.
Similar content being viewed by others


Background
In 2020, GLOBOCAN reported approximately 1.4 million new cases (7.3% of all cancer sites) and 375,000 deaths (3.8% of all cancer sites) attributed to prostate cancer, making it the most common malignant neoplasm in men globally [1, 2]. However, incidence and mortality rates for prostate cancer present significant heterogeneity across different regions of the world. While Australia/New Zealand and several European regions have the highest incidence rates (above 75 per 100,000 men), the Caribbean and Middle Africa exhibit the highest mortality rates (above 25 per 100,000 men) [1,2,3].
Despite GLOBOCAN projections, epidemiological information by country in Latin America remains scarce. During the last decades, the life expectancy of the population of Latin America has increased, together with the increase in aging, thereby shaping current epidemiological profiles [4, 5]. This change inevitably results in an increasing incidence of cancer, including prostate cancer [6, 7], which constitutes one of the major public health problems in Latin America as well as a major challenge for health systems to respond to the growing burden of cancer [5].
In 2020, countries in Latin America, such as Suriname, French Guiana, Venezuela, and Guyana, reported cancer mortality rates of greater than 20 per 100,000 men [2], while in countries such as Ecuador, Peru, and Brazil mortality rates were reported to range from 11.4 to 13.7 per 100,000 men [1, 2, 8].
Prostate cancer is the most frequent cancer affecting Ecuadorian men [2]. Some reports have described the evolution of prostate cancer mortality rates in Ecuador. For example, the incidence of cancer per 100,000 inhabitants in Quito (capital of Ecuador) ranged from 23.1 in 1985 to 62.9 in 2013, while mortality ranged from 9.3 in 1985 to 18.7 in 2013 [9]. However, there are no studies on the evolution of mortality by prostate cancer in Ecuador and its regions in the last decades. Therefore, the aim of this study was to report the prostate cancer mortality rates in Ecuador and its geographical areas and describe the evolution of these mortality rates between 2004 and 2019.
Methods
Data source and study design
We conducted an observational ecological study. We analysed data for prostate cancer deaths identified as C61 according to the International Code of Diseases 10th edition (ICD-10) from 2004 to 2019 in Ecuador.
Ecuador is composed of 24 provinces, distributed in four geographical regions: Coastal, Highlands, Amazonian, and Insular. According to the National Institute of Census and Statistics (INEC), the population projection surpassed 17.7 million people and the male population exceed 8.7 million people (https://sni.gob.ec/proyecciones-y-estudios-demograficos). The Galapagos Island, which belongs to the Insular region, was excluded from the study due to a low number of deaths over more than 5 years of study.
Population denominators were obtained from the INEC data projections published in the Secretaría Nacional de Planificación web page (https://sni.gob.ec/proyecciones-y-estudios-demograficos). National, provincial and regional deaths related to prostate cancer were retrieved from the anonymized INEC databases (https://www.ecuadorencifras.gob.ec/defunciones-generales/), which are responsible for regulating, planning, directing, coordinating, and supervising the official statistics of the country. In addition, INEC registers all the causes of death according to death certificates issued by medical doctors following the standards established by the World Health Organization (WHO), considering the national regulations on the matter (legislation, deadlines, responsibilities, format of the Death Certificate).
The study variables analyzed were age, geographical distribution by province of residence, sex, ethnic self-identification, educational attainment, marital status, death area, death place and mortality. Due to data source incompleteness determined by the absence of data for the cases studied corresponding to variables such as ethnicity and location until 2010 and underreporting, the proportion of entries with missing data on ethnic self-identity, marital status, educational attainment, death area and place where death occurred, did not match the cumulative mortality for sex and age. The data was retrieved as it was documented within the reporting system.
Statistical analysis
All-cause mortality data and place of death 2004–2019 were obtained from the INEC. The 2004–2019 population were obtained from the INEC. The Statistical Package for Social Science Statistics (SPSS Statistics) 26th edition was used to obtain the annual frequencies for each province. The population numerator was the deaths of each province, according to the year. The population denominators were the annual population for each province. For the analysis by province, the deaths of the provinces corresponding to each region were added. The same calculation was performed for the denominators of each region. We analyzed numbers of death for each age group (1–4, 5–9, 10–14, …, 80 + years) and calendar year. Age standardized mortality rates (ASMR) were calculated per 100,000 men-years using the SEGI world standard population with the direct method [10].
We performed an analysis with the average prostate cancer mortality rates of the last 5 years (2015–2019) in Ecuador and its provinces. Joinpoint regression analysis was performed to examine the mortality trends using the Joinpoint regression Program version 4.7.0 [11]. We calculated the estimated annual percentage change (APC) and considered an APCs to be statistically significant with p-values < 0.05. The significance levels used are based on the Monte Carlo permutation method, using the logarithm of the ratio [11, 12].
Ethical approval
According to local and international regulation, this project did no required ethical approval. All the data was obtained from secondary unidentifiable public records. The mortality database is available through the INEC portal.
Results
Ecuador registered 13,419 deaths by prostate cancer between 2004 and 2019:49.8% in the Coastal region, 48.5% in the Highlands and 1.7% in the Amazonian region. The mean age at death was 79 years (± 10 years), 91.7% were elderly (more than 65 years old) and had a primary education (53%). Deaths were mainly located in urban areas (82.6%), and place where death was registered with more frequency was home (61.4%), followed by the hospital, clinic, or private practice (17.3%) and the institute of social security (7.8%) (Table 1).
Deaths caused by prostate cancer were more frequently reported among mestizos (81.4%), Afro-Ecuadorians (7.7%), indigenous (2.4%) and whites (2.2%). In the Coastal region mestizos and afro-Ecuadorians represented 90.4% of deaths and in the Highlands these groups represented 89.1% while in the Amazonian region 80.2% of deaths were registered in mestizos (Table 1).
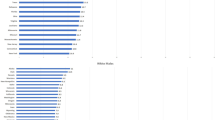
In relation to the prostate cancer mortality rates for the last 5 years (2015–2019) in Ecuador and its provinces, the highest mortality rates (> 13 deaths per 100,000 men) were reported in the Imbabura and Santo Domingo provinces, whereas the lowest mortality rates were in Sucumbios and Orellana provinces (< 5 deaths per 100,00 men) (Fig. 1).

Age-standardized (world population) prostate cancer mortality rates per 100,000 men in Ecuador, between 2015 and 2019
From 2004 to 2019, the ASMR in Ecuador increased from 10.32 in 2004 to 10.80 in 2019 per 100 000 men (4.7% overall increase), whereas these values increased from 9.65 in 2004 to 11.18 in 2019 (15.9% overall increase) in the Coastal region and from 4.83 in 2004 to 5.94 in 2019 in the Amazonian region (overall increase of 23%). On the other hand, in the Highlands region, the ASMR decreased from 11.48 in 2004 to 10.83 in 2019 (overall reduction of 5.7%) (Fig. 2 and Table 2). Heterogeneity in mortality rates was reported among the provinces of Ecuador. In 2004, the highest mortality rates by prostate cancer were Bolivar, Carchi, and Pichincha provinces (> 13 deaths per 100,000 men), whereas in 2019, the highest mortality rates were in the Carchi, Esmeraldas, Imbabura, and Pastaza (> 13 deaths per 100,000 men) (Table 2).

Prostate mortality rates for Ecuador and its geographical regions, for the period 2004–2019
Between 2004 and 2019, Ecuador and its regions (Coastal, Highlands and Amazonian) reported increases in prostate cancer mortality, although these were not significant. (Table 2 and Fig. 2). According to provinces, mortality in Guayas (− 1.1%) significantly decreased along the study period, whereas in Azuay mortality decreased by 4.9% annually from 2004 to 2010, and then increased by 2.9% annually until 2019 (Table 2).
Discussion
Our findings revealed that the mortality rate attributable to prostate cancer in Ecuador was approximately 11 deaths per 100,000 men, with comparable rates observed between the Coastal and Amazonian regions, ranging from 9 to 12 deaths per 100,000 men. However, there were substantial variations in mortality rates across Ecuadorian provinces, ranging from 1.52 to 14.72 deaths per 100,000 men in 2004 to 2.57 to 18.74 deaths per 100,000 men in 2019, indicating the persistent change of this disease in the country.
According to the GLOBOCAN 2020 estimates, prostate cancer in Ecuador is projected to be among the first cause of cancer mortality in men [2]. Mortality rates for prostate cancer in Ecuador are similar to those reported by other Latin American countries such as Argentina, Colombia, and Mexico [13, 14].
Throughout the entire period, there has been a substantial increase in mortality rates, albeit at a slower pace than the incidence [15]. However, these rates are significantly lower than those reported by Cuba and Venezuela, which recorded 20 deaths per 100,000 men in 2015 and 18 deaths per 100,000 men in 2019, respectively [13]. In comparison to European Union (EU) countries, Ecuador also reports lower mortality rates. Specifically, Croatia, Estonia, Latvia, Slovenia, Norway and Sweden all report rates higher than 14 deaths per 100,000 men [16].
Regarding age, the population projections for Ecuador between 2010 and 2020 indicated a decrease in birth rate and an increase in individuals aged 65 to 89 years [17]. However, individuals over 65 years of age have a higher prevalence of prostate cancer [18], suggesting that population aging may contribute to an increase in cases and deaths from this disease. This study found that the average age at death was 79 years (± 10 years), and official reports from Quito indicated that the average age at diagnosis was 77 years [15]. Most of the cases are diagnosed at advanced clinical stages (49%), and therefore treatment alternatives are limited, decreasing the probability of survival [19, 20].
Although the etiology of prostate cancer is not fully understood, known determinants include age, family history, and race/ethnicity [6, 18]. Given the ethnic and regional diversity in Ecuador, which includes mestizos, indigenous peoples, Afro-Ecuadorians, and Whites, genetic studies or studies on resistance to certain treatments may shed light on the high mortality trends observed among the predominantly mestizo and Afro-Ecuadorian populations in the coastal region [21,22,23].
This study, conducted in Ecuador from 2004 to 2019, observed a non-significant increase (0.2%) in the age-standardized mortality rate. Comparison with GLOBOCAN data on Ecuador showed that adjusted mortality rates remained stable, with only slight decreases or increases [2].
Nevertheless, a province-wise analysis revealed a significant decrease in the mortality rate of 27.1% in Pichincha and 14.7% in Guayas. A possible explanation for this trend is that Pichincha, where Quito is located, and Guayas, where the main port of Ecuador is located, have the highest healthcare budget allocations in the country [19]. This allows the population to have greater access to specialized hospitals for the diagnosis and treatment of cancer compared to other provinces.
The results of a previous study conducted in Quito, which examined age-standardized mortality rates during the period of 1985 to 2013 and found an APC of 3.7% [24]. Furthermore, another study conducted in Quito during the period of 2009 to 2017 demonstrated a significant increase in mortality rate, with an APC of 4.1% [24]. These results suggest that a detailed analysis of the mortality rate's behavior in each city or canton of Ecuador is necessary to identify the potential causes of these changes. These changes could be attributed to factors such as population density, education level, or access to healthcare services [25, 26].
The first decade of the twenty-first century saw a remarkable 1,000% increase in the health budget by the Ecuadorian State. This increase facilitated notable improvements in various health indicators, such as the density of doctors per 1,000 inhabitants, the scope of preventive and diagnostic care coverage, and the availability of medications. Consequently, there was a decrease in Ecuadorian mortality due to all causes (per 1,000 inhabitants) from 4.6 in 2000 to 4.1 in 2011. Notably, these indicators could be associated with a decrease in mortality from prostate cancer in regions that had established records on the disease, such as some provinces of the Highlands region.
On the other hand, a notable rise in prostate cancer mortality was detected in provinces located in the Coastal region, where health coverage is insufficient [27]. Nevertheless, the provinces within the Amazon region exhibited the lowest mortality rates. These findings align with studies conducted in other countries within the region, including Colombia, Venezuela, Peru, and Brazil [28,29,30,31]. The geographical and temporal differences observed across Ecuador's provinces could be explained by factors that could be related to genetic, environmental, socioeconomic or cultural aspects, in addition to the variations in timely access to diagnostic and registration practices, limited access to initial basic treatment, and the lack of prioritize specific strategies [5, 32].
However, around 21% of Latin American countries have cancer registries, even some regions such as Central America (around 3%) and South America (around 10%) have poor high quality cancer registries [33]. Most countries in the region only have isolated programs and campaigns, generated by specific groups without government support or policies [34, 35].
Between 2006 and 2010, the Ministry of Public Health of Ecuador reported that prostate cancer cases were detected at an advanced stage [19]. In response, Ecuador implemented the National Strategy for Comprehensive Cancer Care in Ecuador in 2017, which established intensive screening regulations for prioritized neoplasms [19, 36]. This regulation excludes generalized collective screening, limiting screening to only well-informed patients who request it. Screening includes the prostate specific antigen test and digital rectal examination, and biopsy if necessary. Due to the need to obtain results in terms of disease incidence, these interventions often have long waiting periods. However, some studies have concluded that prostate cancer screening does not improve mortality [37]. Therefore, some studies recommend optimizing screening criteria to target high-risk populations, as well as increasing awareness and education on the risks and benefits of prostate cancer screening to make informed decisions [38, 39].
Despite the mandatory application of this public policy at the national level, there are still limitations in accessing healthcare in various rural areas of Ecuadorian regions. This is compounded by the lack of information, delays in diagnosis, unequal access to diagnostic technologies and treatment options, high costs, and a lack of clinical practice guidelines and awareness among specialists [25, 40]. These issues are further compounded by inadequate consultation time for providing personalized counseling to patients. Consequently, those may be one of the reasons why most cases (49%) are diagnosed in advanced clinical stage IV [19, 20].
Moreover, although recent initiatives to increase early detection and raise awareness are anticipated to result in an upsurge in prostate cancer diagnoses, the effect on mortality rates remains to be ascertained.
Limitations and strengths
The study is limited by the quality of the national deaths reporting database, which is a common issue in studies that rely on secondary sources of information. The database lacks specific information on tumor characteristics such as histology and stage, and there are missing data and limited individual-level information. Additionally, there is variation in death registration completeness and quality. However, a major strength of our study is that it is the first report to comprehensively examine trends in prostate cancer mortality in Ecuador and its geographic regions, providing important insights for the development of national and provincial registration measures and integrated healthcare actions, as well as guiding future studies in provinces with fluctuating trends.
Conclusion
In conclusion, the mortality rates by prostate cancer in Ecuador have remained stable over the past few decades. However, it is imperative to centralize efforts in provinces where mortality rates remain high and in the provinces with significant decreases, identify the factors contributing to this behavior. The implementation of comprehensive and reliable national cancer registries is crucial for sharing information across the region and developing integrated national measures to decrease mortality from prostate cancer. These measures may include optimizing resources for the diagnosis, management, and treatment of patients, developing specific programmes to identify patients at risk, and continuing medical education programmes. Further studies are needed to determine the factors contributing to regional disparities. These studies will aid in the development of targeted interventions that may contribute to reducing the burden of this disease on the Ecuadorian population.
Availability of data and materials
The datasets used and/or analysed during the current study are available in the following link: https://www.ecuadorencifras.gob.ec/nacimientos-y-defunciones-informacion-historica/.
Abbreviations
- ICD-10:
-
International Code of Diseases 10th edition
- INEC:
-
National Institute of Census and Statistics
- SPSS:
-
Statistic Statistical Package for Social Science Statistics
- ASMR:
-
Age standardized mortality rates
- APC:
-
Annual percentage change
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin. 2021;71(3):209–49.
Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. 2020. [Cited 11 March, 2023]. Available from: https://gco.iarc.fr/today.
Ramaliba TM, Sithole N, Ncinitwa A, Somdyala NI. Prostate Cancer Patterns and Trends in the Eastern Cape Province of South Africa; 1998–2017. Front Public Health. 2022;10:1137.
Johns L, Houlston R. A systematic review and meta-analysis of familial prostate cancer risk. BJU Int. 2003;91(9):789–94.
Goss PE, Lee BL, Badovinac-Crnjevic T, Strasser-Weippl K, Chavarri-Guerra Y, St Louis J, Villarreal-Garza C, Unger-Saldaña K, Ferreyra M, Debiasi M. Planning cancer control in Latin America and the Caribbean. Lancet Oncol. 2013;14(5):391–436.
Bray F, Piñeros M. Cancer patterns, trends and projections in Latin America and the Caribbean: a global context. Salud Publica Mex. 2016;58(2):104–17.
Pilleron S, Soerjomataram I, Soto-Perez-de-Celis E, Ferlay J, Vega E, Bray F, Piñeros M. Aging and the cancer burden in Latin America and the Caribbean: Time to act. J Geriatr Oncol. 2019;10(5):799–804.
Piñeros M, Laversanne M, Barrios E, de Camargo CM, de Vries E, Pardo C, Bray F. An updated profile of the cancer burden, patterns and trends in Latin America and the Caribbean. Lancet Reg Health Am. 2022;13: 100294.
Corral Cordero F, Cueva Ayala P, Yépez Maldonado J, Tarupi Montenegro W. Trends in cancer incidence and mortality over three decades in Quito-Ecuador. Colomb Med. 2018;49(1):35–41.
Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age Standardization of Rates: A new Who Standard. 2001. [Cited 10 January, 2023]. Available from: https://cdn.who.int/media/docs/default-source/gho-documents/global-health-estimates/gpe_discussion_paper_series_paper31_2001_age_standardization_rates.pdf.
Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–51.
Kim HJ, Fay MP, Yu B, Barrett MJ, Feuer EJ. Comparability of segmented line regression models. Biometrics. 2004;60(4):1005–14.
Carioli G, Bertuccio P, Malvezzi M, Rodriguez T, Levi F, Boffetta P, La Vecchia C. Negri EJIJoC: Cancer mortality predictions for 2019 in Latin America. Int J Cancer. 2020;147(3):619–32.
Carioli G, La Vecchia C, Bertuccio P, Rodriguez T, Levi F, Boffetta P, Negri E, Malvezzi M. Cancer mortality predictions for 2017 in Latin America. Ann Oncol. 2017;28(9):2286–97.
SOLCA Núcleo de Quito/Registro Nacional de Tumores. Boletín Epidemiológico [Internet]. SOLCA, Núcleo de Quito. [cited April 3, 2023]. Available in: http://biblioteca.solcaquito.org.ec:9997/handle/123456789/136.
Bertuccio P, Santucci C, Carioli G, Malvezzi M, La Vecchia C, Negri E. Mortality Trends from Urologic Cancers in Europe over the Period 1980–2017 and a Projection to 2025. Eur Urol Oncol. 2021;4(5):677–96.
Instituto Nacional de Estadistica y Censos. Proyección por edades Provincias 2010–2020 y nacional. Available in: https://www.ecuadorencifras.gob.ec/proyecciones-poblacionales/.
Sierra MS, Soerjomataram I, Forman D. Prostate cancer burden in Central and South America. Cancer Epidemiol. 2016;44:S131–40.
Ministerio de Salud Publica. Estrategia Nacional para la Atención Integral del Cáncer en el Ecuador. Available in: https://aplicaciones.msp.gob.ec/salud/archivosdigitales/documentosDirecciones/dnn/archivos/ac_0059_2017.pdf.
Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, Davis M, de Smith AJ, Dutil J, Figueiredo JC. Cancer health disparities in racial/ethnic minorities in the United States. Br J Cancer. 2021;124(2):315–32.
Lewis DD, Cropp CD. The impact of African ancestry on prostate cancer disparities in the era of precision medicine. Genes. 2020;11(12):1471.
Yamoah K, Lee KM, Awasthi S, Alba PR, Perez C, Anglin-Foote TR, Robison B, Gao A, DuVall SL, Katsoulakis E. Racial and ethnic disparities in prostate cancer outcomes in the veterans affairs health care system. JAMA Netw Open. 2022;5(1):e2144027–e2144027.
Rebbeck TR. Prostate cancer genetics: variation by race, ethnicity, and geography. Semin Radiat Oncol. 2017;27(1):3–10.
Cueva P, Tarupi W, Caballero H. Cancer incidence and mortality in Quito: information to monitor cancer control policies. Colomb Med. 2022;53(1):e2024929
Reis RBd, Alías-Melgar A, Martínez-Cornelio A, Neciosup SP, Sade JP, Santos M, Villoldo GM. Prostate Cancer in Latin America: Challenges and Recommendations. Cancer Control. 2020;27(1):1073274820915720.
Dale W, Vijayakumar S, Lawlor EF, Merrell K. Prostate cancer, race, and socioeconomic status: inadequate adjustment for social factors in assessing racial differences. Prostate. 1996;29(5):271–81.
Ministerio de Salud Publica. Datos esenciales de salud: Una mirada a la década 2000 - 2010. Available in: https://www.salud.gob.ec/wp-content/uploads/downloads/2013/05/Datos-esenciales-de-salud-2000-2010.pdf.
Matiz JLP, Reyes NJA, Becerra MPS, Almendrales FPD. Evolución de la mortalidad por cáncer de próstata en Colombia: estudio ecológico. Urol Colomb. 2014;23(1):3–10.
Capote Negrin LG. Aspectos epidemiológicos del cáncer en Venezuela. Rev Venez Oncol. 2006;18(4):269–81.
Borges MFdSO, Koifman S, Koifman RJ, da Silva IF. Cancer incidence in indigenous populations of Western Amazon. Brazil Ethn Health. 2022;27(6):1465–81.
Torres-Roman JS, Ruiz EF, Martinez-Herrera JF, Mendes Braga SF, Taxa L, Saldaña-Gallo J, Pow-Sang MR, Pow-Sang JM, La Vecchia C. Prostate cancer mortality rates in Peru and its geographical regions. BJU Int. 2019;123(4):595–601.
Lucio R, Villacrés N, Henríquez R. Sistema de salud de Ecuador. Salud Publ Mex. 2011;53:s177–87.
Piñeros M, Abriata MG, de Vries E, Barrios E, Bravo LE, Cueva P, de Camargo CM, Fernández L, Gil E, Luciani S. Progress, challenges and ways forward supporting cancer surveillance in Latin America. Int J Cancer. 2021;149(1):12–20.
Arrossi S. Cancer registration and information systems in Latin America. Lancet Oncol. 2015;16(14):1400–1.
Piñeros M, Abriata MG, Mery L, Bray F. Cancer registration for cancer control in Latin America: a status and progress report. Rev Panam Salud Publica. 2018;41: e2.
Barrios CH, Werutsky G, Mohar A, Ferrigno AS, Müller BG, Bychkovsky BL, Uribe CJ, Villarreal-Garza C, Soto-Perez-de-Celis E, Gutiérrez-Delgado F. Cancer control in Latin America and the Caribbean: recent advances and opportunities to move forward. Lancet Oncol. 2021;22(11):e474–87.
Andriole GL, Crawford ED, Grubb RL III, Buys SS, Chia D, Church TR, Fouad MN, Isaacs C, Kvale PA, Reding DJ. Prostate cancer screening in the randomized Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial: mortality results after 13 years of follow-up. J Natl Cancer Inst. 2012;104(2):125–32.
Krilaviciute A, Albers P, Lakes J, Radtke JP, Herkommer K, Gschwend J, Peters I, Kuczyk M, Koerber SA, Debus J. Adherence to a risk-adapted screening strategy for prostate cancer: First results of the PROBASE trial. Int J Cancer. 2023;152(5):854–64.
Takahashi T. PSA screening in high-risk groups: what are the changes in benefits and harm? Br J Cancer. 2022;127(7):1173–4.
Anampa-Guzmán A, Acevedo F, Partridge AH, Alfano CM, Nekhlyudov L. Cancer survivorship in Latin America: Current status and opportunities. JCO Glob Oncol. 2021;7:1472–9.
Acknowledgements
We thank the Universidad Cientifica del Sur for proofreading our manuscript.
Funding
Self-funded.
Author information
Authors and Affiliations
Contributions
Conceived and designed the idea: KSR, JSRT. Had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis: KSR, JG, JSRT. Contributed to the writing of the manuscript: All authors. Contributed to the statistical analysis: KSR, JSTR. Critical revision of the manuscript: KSR, GDK, JYM, JFMH. Approval of the submitted and final version: All authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval and consent of the participants were not necessary since this study involved the use of a previously published secondary database.
Consent for publication
Not applicable.
Competing interests
The author(s) declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Simbaña-Rivera, K., Torres-Roman, J.S., Challapa-Mamani, M.R. et al. Regional disparities of prostate cancer mortality in Ecuador: an examination of trends and correlates from 2004 to 2019. BMC Public Health 23, 992 (2023). https://doi.org/10.1186/s12889-023-15941-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15941-z