
Abstract
Background
Access to essential medicines is a vital component of universal health coverage. The low availability of essential medicines for children (EMC) has led the World Health Organization (WHO) to issue a number of resolutions calling on member states on its improvement. But its global progress has been unclear. We aimed to systematically evaluate the progress of availability of EMC over the past decade across economic regions and countries.
Methods
We searched eight databases from inception to December 2021 and reference lists to identify included studies. Two reviewers independently conducted literature screening, data extraction and quality evaluation. This study was registered with PROSPERO, CRD42022314003.
Results
Overall, 22 cross-sectional studies covering 17 countries, 4 income groups were included. Globally, the average availability rates of EMC were 39.0% (95%CI: 35.5-42.5%) in 2009–2015 and 43.1% (95%CI: 40.1-46.2%) in 2016–2020. Based on the World Bank classification of economic regions, income was not proportional to availability. Nationally, the availability rate of EMC was reasonable and high (> 50%) in only 4 countries, and low or very low for the rest 13 countries. The availability rates of EMC in primary healthcare centers had increased, while that for other levels of hospitals slightly declined. The availability of original medicines decreased while that of generic medicines was stable. All drug categories had not achieved the high availability rate.
Conclusion
The availability rate of EMC was low globally, with slight increase in the last decade. Continuous monitoring and timely reporting of the availability of EMC are also needed to facilitate targets setting and inform relevant policy making.
Similar content being viewed by others

Background
Access to essential medicines is a vital component to the fulfilment of the right to the highest attainable standard of health [1]. As one of the Sustainable Development Goals of the United Nations, access to safe, effective, quality, and affordable essential medicines is important to health coverage for children by 2030 [2]. In the last ten years, to improve availability of essential medicines for children (EMC), the World Health Organization (WHO) has issued some resolutions calling on member states to focus on it and also has regularly updated the model list of EMC. [3,4,5] The first Essential Medicines List for Children was published in 2007. The current versions, updated in September 2021, are the 8th Essential Medicines List for Children (EMLc). [6].
To promote and standardize investigation on the availability, price, and affordability of essential medicines, WHO and Health Action International (HAI) have developed “Measuring medicine prices, availability, affordability and price components” in 2003. [5] Previous studies found that the availability and affordability of EMC was generally low in low- and middle-income countries (LMCs). [7,8] However, it is unclear whether there is a progress on the availability of EMC over the last decade globally, to what extent, and its variations among countries. Therefore, this systematic review and meta-analysis was conducted to examine the global trend on the availability of EMC, its variation among economic regions and countries, to provide benchmarking and inform evidence-based health policy-making.
Methods
Search strategy and selection criteria
We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. [9] The protocol of this systematic review was registered on PROSPERO, CRD42022314003.
We systematically searched PubMed, Embase, the Cochrane Library, Web of Science, CNKI, China Biology Medicine (CBM) from inception to December 2021. We also searched websites of WHO and Health Action International, reference lists of included studies, and published reviews for more eligible studies. The search strategy included a combination of medical subject headings and free text terms for (“child*” or “pediatri*”) and (“essential medic*” or “essential drug*”) and was adapted for each database.
The studies were included if they investigated medical institutions or pharmacies for availability of EMC, including vaccines, and they were designed as cross-sectional study. The studies published in all languages were included. Studies were excluded if they were: editorials, conference abstracts, and any unobtainable full-texts. Two reviewers (SYQ and CZ) selected studies according to the inclusion and exclusion criteria independently. Discrepancies were resolved by discussion or consultation with a third reviewer.
Data extraction and analysis
Two reviewers (SYQ and CZ) independently extracted data using predefined excel data extraction form. The extracted data included the first author, published year, survey area, survey time, methods, the availability of EMC. Joanna Briggs Institute (JBI) was used to evaluate the risk of bias of included studies. [10] This tool has nine items and categorized each item with “yes”, “unclear” and “no”, and gave them “1” and “0” points. The total score > 6 points was considered as high quality, between 4 and 6 points was considered as medium quality; < 4 was considered as low quality. [11].
Statistical analysis
The availability rate was defined as the percentage of facilities with stock of the required on the day survey data were collected. We extracted the number of the facilities that had the medicine and total number of facilities on the day of data collection. Data were meta-analyzed using Stata 15.1 (Stata Corp, College Station, TX). The final availability rates were presented as weighted average and their 95% confidence intervals (CIs).
They were estimated by world, economic levels (The World Bank groups - high-income, upper-middle-income, lower-middle-income and low-income countries), country, types of medical institutions (ownership - public and private; institutional level - primary healthcare and other levels hospital), and medicine classification using the Anatomical Therapeutic Chemical (ATC) code. We also analyzed results across the six WHO geographical regions, but were excluded due to the small number of studies and lack of representativeness.
The United Nations Millennium Development Goals (MDGs) are goals that UN Member States have agreed to try to achieve by the year 2015. Therefore, we estimated the availability rate for 2009–2015 years and 2016–2020 years, respectively, to quantify its progress over time. [2].
The availability rate of essential medicines was classified as: not available (availability = 0); very low (0 < availability < 30%), low (30%≤availability < 50%), reasonable (50%≤availability < 80%) and high (≥ 80%) [12]. I2 test and Chi square test were used to examine heterogeneity. I2 > 50% or P ≤ 0.05 indicated significant heterogeneity among studies, where random effect model was used. Otherwise, fixed effect model was used.
Results
Study characteristics
We identified 15,171 unique titles for eligibility screening, and 22 studies were finally included after assessment of the full-text manuscript by two reviewers independently. (Fig. 1) The characteristics of the included studies were summarized in Table 1. All studies were cross-sectional studies conducted from 2009 to 2020. All included studies were from low-income (3/22), lower-middle-income (12/22), upper-middle-income groups (6/22), and one study (1/22) involved 8 LICs, 16 LMCs, 15 UMCs and 19 HICs. Methodologically, 15 (68.2%) studies used standardized WHO/HAI methodology, [14, 16,17,18, 20, 22,23,24,25,26, 30,31,32,33,34] 2 (9.1%) studies used adapted WHO/HAI method, [13, 29] and the remaining 5 (22.7%) studies used other methods. [15,19, 21, 27, 28] The mean number of essential medicines investigated was 31 (range: 5 to 121).

PRISMA flowchart of study selection
Risk of bias assessment
Seventeen studies (77.3%) selected surveyed essential medicines according to the WHO Model List of EMC (EMLc), [16, 18, 20,21,22,23,24,25,26,27,28,29,30,31,32,33,34] while other studies selected surveyed essential medicines from other sources (including “priority life-saving medicines for women and children” developed by the WHO, list of national rural health mission, childspecific essential medicines list of the state, international society of pediatric oncology, and regional supplemental directory). The source of the list in 2 studies was unknown. [13, 14]
Most studies (21, 95.5%) were rated as low risk of bias, [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27, 29,30,31,32,33,34] whereas one study (4.5%) was graded as medium risk. [28] 11 studies achieved 9 points and 9 studies scored 8 points. There was one article each for 6 and 7. The bias was mainly from the following items: five studies (22.8%) were considered as unwell-represented samples. [14, 15, 24, 27, 30] Four studies (18.2%) were considered as insufficient coverage of the identified sample. [15, 19, 23, 24] It is unclear that if the sample size was adequate in nineteen studies (86.4%),13–19, 21–[24, 26,27,28,29,30,31, 33]–[34] and coverage of the identified sample was sufficient in eleven studies (50.0%). [14, 16,17,18, 21, 22, 25,26,27, 29], 31The criteria and results of quality assessment for each study were shown in Supplementary Table 2.
Global trend of availability of essential medicines for children
Overall, the availability rate of EMC from 2009 to 2015 was 39.0% (95%CI: 35.5-42.5%), while that from 2016 to 2020 was 43.1% (95%CI: 40.1-46.2%). There was a high degree of heterogeneity between the studies in 2009–2015 and 2016–2020 (I2 = 98.44%, I2 = 94.23%), so the random effect model was used. (Figs. 2 and 3)

Availability rates (%) of essential medicines for children from 2009–2015
Note: A, Alimentary Tract And Metabolism; B, Blood And Blood Forming Organs; C, Cardiovascular System; D, Dermatologicals; G, Genito Urinary System And Sex Hormones; H, Systemic Hormonal Preparations, Excl. Sex Hormones And insulin; J, Antiinfectives For Systemic Use; L, Antineoplastic And Immunomodulating Agents; M, Musculo-Skeletal System; N, Nervous System; P, Antiparasitic Products, Insecticides And Repellents; R, Respiratory System; V, Various

Availability rates (%) of essential medicines for children from 2016–2020
Note: A, Alimentary Tract And Metabolism; B, Blood And Blood Forming Organs; C, Cardiovascular System; D, Dermatologicals; G, Genito Urinary System And Sex Hormones; H, Systemic Hormonal Preparations, Excl. Sex Hormones And insulin; J, Antiinfectives For Systemic Use; L, Antineoplastic And Immunomodulating Agents; M, Musculo-Skeletal System; N, Nervous System; P, Antiparasitic Products, Insecticides And Repellents; R, Respiratory System; V, Various
Economic regional availability of essential medicines by world bank country-income groups
By World Bank classification of income countries, the availability rate of EMC in LMC countries was the highest (48.1%, 95%CI: 41.9-54.4%) from 2009 to 2015. (Fig. 2) From 2016 to 2020, the availability rate of EMC was highest in HIC countries (95.8%, 95%CI: 93.5-97.7%). (Figs. 3 and 4)

Availability rates of essential medicines for children by income, ownership, level of medical institutions, original and generic medicines, 2009 to 2015 and 2016 to 2020
Note: HIC, high-income country; UMC, upper-middle income country; LMC, lower-middle-income country; LIC, low- income country; Private, private medical institutions; Public, public medical institutions; Primary, primary healthcare centers; Hospital, other levels of hospitals except for primary medical institutions; Original, original medicines; Generic, generic medicines
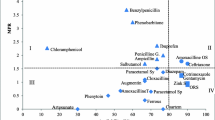
As was shown in the Fig. 5, there was no proportional between income and availability rates, and the regularity of changes between time and availability rates was not obvious.

Changes of availability rates (%) of essential medicines for children over time from 2009–2020
Note: LIC, low- income country; LMC, lower-middle-income country; UMC, upper-middle income country. 1 Total availability; 2 Public sectors; 3 Private sectors; 4 Original medicines; 5 Generic medicines. The size of the dots indicate the number of surveyed institutions
Availability of essential medicines for children by countries
Only 13 and 7 countries reported country-specific availability rate of EMC from 2009 to 2015 and from 2016 to 2020, respectively. From 2009 to 2015, the availability rate of EMC ranged from 16.8% (95% CI: 12.0%, 22.2%) in China to 70.1% (95% CI: 62.0-77.6%) in Sri Lanka. (Fig. 2) From 2016 to 2020, the availability rate of EMC was lowest in China (18.8%, 95%CI: 16.2-21.5%) and highest in Mongolia (69.2%, 95%CI: 58.6-79.0%). (Fig. 3) There were studies conducted in India, China and Ethiopia in both of the two periods, and the availability rates of India and China increased by 2.6% and 2.0%, respectively. While the availability rates of Ethiopia decreased by 1.0%. (Fig. 6)

Availability rates of essential medicine for children by country, from 2009–2015 (A) and from 2016–2020 (B) Note: The availability rate of medicines was calculated as percentage (%) of the surveyed outlets where the medicines were found on the day of data collection. The values in the bar chart were pooled average availability rates of all surveyed medicines in each country using Stata 15.1.
Availability of essential medicines for children by types of medical institutions
By ownership of medical institutions, the availability rate of EMC was 31.9% (95% CI: 26.0-38.0%) in public medical institutions, lower than that of 37.6% (95% CI: 31.0-44.4%) in private medical institutions from 2009 to 2015. (Fig. 2) From 2016 to 2020, the availability rate of EMC in public medical institutions was 29.4% (95% CI: 25.3-33.6%), still lower than that of 32.0% (95% CI: 27.0-37.1%) in private medical institutions. (Figs. 3 and 4)
By level of medical institutions, the availability rate of EMC was 21.7% (95% CI: 1.0-58.4%) in primary healthcare centers, lower than that of 32.2% (95% CI: 24.7-40.0%) in higher level hospitals from 2009 to 2015. (Fig. 2) From 2016 to 2020, the availability rate of EMC in primary healthcare centers increased by 26.0%, while that of other level hospitals decreased by 2.3%. (Figs. 3 and 4)
Availability of original and generic essential medicines for children
The availability rate of generic medicines was much higher than original medicines. From 2009 to 2015, the availability rate of generic medicines was 34.9% (95% CI :27.0-43.1%), while that of original medicines was 20.2% (95% CI:11.9-30.0%). (Fig. 2) From 2016 to 2019, the availability rate of generic medicines was 32.2% (95% CI: 28.1-36.5%) and that of original medicines was 9.2% (95% CI: 6.4-12.2%), showing an enlarged gap between generic medicines and original medicines. (Figs. 3 and 4)
Availability of medicine categories according to ATC
The results showed that there were significant differences in the availability rate of different categories of medicines. From 2009 to 2020, 5 categories were scored as very low (C, N, M, H, P), low for 5 categories (B, J, D, R, A), reasonable for 1 category (L) and high for 1 category (V). Cardiovascular System had lowest availability (24.1%, 95%CI: 13.6-36.2%) and Antineoplastic and Immunomodulating Agents had highest availability (69.2%, 95%CI: 64.0-74.3%). (Fig. 7)

Availability of essential medicines for children by ATC, 2009 to 2020
Note: A, Alimentary Tract And Metabolism; B, Blood And Blood Forming Organs; C, Cardiovascular System; D, Dermatologicals; J, Antiinfectives For Systemic Use; L, Antineoplastic And Immunomodulating Agents; M, Musculo-Skeletal System; N, Nervous System; P, Antiparasitic Products, Insecticides And Repellents; R, Respiratory System; V, Various
Box limits indicate the range of the central 50% of the data, with a central line marking the median value. Lines extend from each box to capture the range of the remaining data. The black dots represent each specific availability value of ATC.
Discussion
In this study, we comprehensively assessed the global availability of EMC from 2009 to 2020. The global availability rate of EMC in 2016–2020 (43.1%) increased, but not significantly compared with that in 2009–2015 (39.0%). By World Bank country income groups, income was not proportional to availability. By country, the availability rate varied substantially across countries in both 2009–2015 and 2016–2020. By ownership of medical institutions, the availability rate of EMC in public medical institutions was slightly lower than that of in private medical institutions in both 2009–2015 and 2016–2020. By level of medical institutions, the availability rates in primary healthcare centers had increased, while that for higher level hospitals had slightly declined. In terms of generic and original medicines, the availability of generic medicines was stable but that of original medicines decreased. The availability rate of EMC also varied largely for drug categories, from low to reasonable availability. Furthermore, our findings showed that access to essential medicines for major noncommunicable diseases hadn’t reached the target of 80% [35].
As far as we know, this study is the first to quantify the availability rate of EMC and its trend with time globally, nationally and regionally for the last decade. The global availability rate of EMC had slightly increased in the last decade. There was substantial variability between countries and economic regions. However, there was a relatively limited number of economic regions and countries involved in surveys, indicating substantial research gaps globally, regionally and nationally. Caution is also needed in generalizing the availability rate of a country as representative of the whole economic region. We recommend that countries continue to conduct surveys on the availability of EMC to fill the current lack of data.
In terms of relationship of availability and income, there are several possible reasons for lower levels of EMCs in UMCs or than LMCs. Firstly, LMCs may focus on essential medicines from the WHO EMLc (covered by the survey); that UMCs often use other branded/combination medicines not on the EML, so their score were low on WHO EMLc medicines. Besides, an article surveyed availability of essential cytotoxic medicines for treating children with cancers in 50 countries also concluded that income is not proportional to availability, and analyzed that was attributed to a narrower range of clinical protocols or manage lower stages of disease and therefore rely on a smaller number of agents in LICs. [27] Finally, national policies may facilitate access to medicines. Sri Lanka, though a lower-middle income country, had a high availability rate, which might be related to its national policies. It had established a national pharmaceutical company to distribute drugs to the public and private sectors, and the public sector provided free essential medicines to residents. [13] China, a upper-middle income country, had officially implemented the essential medicine system since 2009, but there was a low availability of EMC, due to the high cost of development and low pricing, leading to lose motivation for enterprises. Secondly, the implementation of the policy of China’s list of essential medicine for children has been slow. Thirdly, the varieties of essential medicines procured by medical institutions at all levels are not fully consistent with EMLc. Therefore, China also needs to further implement the policy, formulate incentive measures, and encourage enterprise to invest. [24] In addition, there are other countries that increased availability rate through reforms. Uganda had improved access to cancer medicines from 28.5 to 85.8% within a space of 2 fiscal years by two main factors: first, redefining cancer medicines as highly specialized drugs and legalizing an independent procurement in 2016; second, by streamlining the procurement and supply chain to eliminate or minimize the role of middlemen. [36] The Mexico government had implemented pooled procurement to improve availability. [37].
We also found that the availability rate of EMC in public medical institutions was slightly lower than that of in private medical institutions in both 2009–2015 and 2016–2020, which were similar to a systematic review of essential medicines for asthma. [38] While private sector is important to facilitate access to EMC, more measures are warranted to increase the availability of EMC in public health institutions, for they are the main providers of public health and primary healthcare services and pivotal in pursuing universal health coverage in many countries.
The gap between the availability of original and generic medicines is growing. On the one hand, countries encourage the research and development of generic medicines, promoting higher availability of generic medicines. On the other hand, they also need to encourage the research and development of original medicines, establish an early reliable patent warning system of medicines, and protect intellectual property rights. [39] Therefore, introducing incentives for production infrastructure and suppliers improvements is crucial, including financial incentives and policy support to address the economic causes of manufacturing issues. [40].
There is also a large variation of availability rates among medicine categories, ranging from 24.1 to 87.1% in 2009–2020. Among them, the anti-neoplastic and immunomodulating agents had the highest availability rate. Among the survey institutions with an availability rate of > 80%, the type of institution and the level of the medical institution were not clearly indicated in part of studies due to the small number of available studies. Therefore, it could not be explained from this perspective. Analyzing income levels > 80% of the countries, high-income and upper-middle-income countries accounted for more than half, similar to the findings of a global cross-sectional survey of 82 countries. [41] Although availability was also high in low-income countries, the data are all from one study with only eight institutions, making them unrepresentative. Policy support may be a possible reason for the increased availability, indicating the important and positive role of pharmaceutical policies in improving the availability of EMC. A survey of 37 European countries from 2016 to 2018 showed that children and adolescents with cancer still experienced lack of access to essential medicines. [42] To address this issue, the Expert Committee in developing the WHO EMLc included several additional supportive care agents for cancer and the Essential Medicines Working Group of the International Society of Pediatric Oncology (SIOP) proposed a list of anti-neoplastic drugs, [43]–[44]. In our study, carboplatin, methotrexate, ifosfamide, cyclophosphamide, etoposide, vincristine, doxorubicin, dactinomycin, cytarabine, cisplatin are the top ten anticancer drugs in the research frequency and belong to the SIOP core catalog.
There were several limitations of this study. Firstly, limited by the number of studies included, economic regional and national availability rates estimated may not be stable or accurate. Secondly, limited by the quality of some studies, such as the medicines selected for investigation inconsistent, there were some bias in the results. However, this study provides a comprehensive map of the global, regional and national availability of EMC and that by medical institutions, original and generic medicines and medicine categories from 2009 to 2015 using evidence-based methodology, and there is nothing better for the moment, which shed light on the needs in practice and in research in the future.
Conclusions
In conclusion, the availability rate of EMC is still low globally, with only marginal increase in the last decade and only a few categories reached reasonable and high availability (> 50%). Income is not always proportional to EMC. No country had reached the target of high availability rate (> 80%) of EMC. It is suggested to carry out relevant studies to fill the data gaps in the children’s essential medicine survey and improve the accessibility of children’s medicines. Substantial efforts from all stakeholders are warranted to improve the availability of EMC globally and its equity among countries. Continuous monitoring and timely reporting of the availability of EMC are also needed to facilitate targets setting and inform relevant policy making.
Data availability
All datasets generated and analyzed, including the study protocol, search strategy, list of the included and excluded studies, data extracted, quality assessment, merged data and investigated medicines of each study are available in the article and upon request from the corresponding author.
Abbreviations
- ATC:
-
Anatomical Therapeutic Chemical
- CBM:
-
China Biology Medicine
- CI:
-
Confidence Intervals
- CNKI:
-
China National Knowledge Infrastructure
- EMLc:
-
Essential Medicines for Children
- HAI:
-
Health Action International
- HIC:
-
High-income countries
- JBI:
-
Joanna Briggs Institute
- LIC:
-
Low income countries
- LMC:
-
Lower Middle income countries
- MDGs:
-
The United Nations Millennium Development Goals
- NEML:
-
National Essential Medicine List
- NRHM:
-
National Rural Health Mission’s list
- PRISMA:
-
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- SARA:
-
Service availability and readiness assessment
- SIOP:
-
International Society of Pediatric Oncology
- UMC:
-
Upper-middle-income countries
- WHA:
-
World Health Assembly
- WHO:
-
World Health Organization
References
Hogerzeil HV. Essential medicines and human rights: what can they learn from each other? Bull World Health Organ. 2006;84(5):371–5.
World Health Organization. Millennium Development Goals (MDGs). 2018. https://www.who.int/news-room/factsheets/detail/millennium-development-goals-(mdgs). Accessed 4 Nov 2022.
World Health Organization. Better Medicines for Children. 2012. https://apps.who.int/iris/handle/10665/22030. Accessed 4 Nov 2022.
World Health Organization. Promoting Innovation and Access to Quality, Safe, Efficacious and Affordable Medicines for Children. 2016. https://www.who.int/publications/i/item/promoting-innovation-and-access-to-quality-safe-efficacious-and-affordable-medicines-for-children. Accessed 4 Nov 2022.
World Health Organization. Children: improving survival and well-being. 2020. https://www.who.int/en/news-room/fact-sheets/detail/children-reducing-mortality. Accessed 4 Nov 2022.
World Health Organization. WHO Model Lists of Essential Medicines. 2021. https://www.who.int/groups/expert-committee-on-selection-and-use-of-essential-medicines/essential-medicines-lists. Accessed 15 Mar 2023.
Stevens H, Huys I. Innovative approaches to increase Access to Medicines in developing countries. Front Med (Lausanne). 2017;4:218.
Chen Z, Li S, Zeng L, Liu Y, Zhang M, Choonara I, Zhang L. Accessibility of Medicines for Children: a systematic review. Front Pharmacol. 2021;12:691606.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. 2015;13(3):147–53.
Wilairatana P, Masangkay FR, Kotepui KU, Milanez GJ, Kotepui M. Prevalence and characteristics of malaria among COVID-19 individuals: a systematic review, meta-analysis, and analysis of case reports. PLoS Negl Trop Dis. 2021;15(10):e0009766.
World Health Organization. Price, availability and affordability: an international comparison of chronic disease medicines. 2014. http://apps.who.int/iris/handle/10665/116493. Accessed 4 Nov 2022.
Balasubramaniam R, Beneragama BV, Sri Ranganathan S. A national survey of availability of key essential medicines for children in Sri Lanka. Ceylon Med J. 2011;56(3):101–7.
Balasubramaniam R, Benaragama BV, Sri Ranganathan S. A national survey of price and affordability of key essential medicines for children in Sri Lanka. Indian J Pediatr. 2014;81(4):362–7.
Gitanjali B, Manikandan S. Availability of five essential medicines for children in public health facilities in India: a snapshot survey. J Pharmacol Pharmacother. 2011;2(2):95–9.
Anson A, Ramay B, de Esparza AR, Bero L. Availability, prices and affordability of the World Health Organization’s essential medicines for children in Guatemala. Global Health. 2012;8:22.
Swain TR, Rath B, Dehury S, Tarai A, Das P, Samal R, Samal S, Nayak H. Pricing and availability of some essential child specific medicines in Odisha. Indian J Pharmacol. 2015;47(5):496–501.
Wang X, Fang Y, Yang S, Jiang M, Yan K, Wu L, Lv B, Shen Q. Access to paediatric essential medicines: a survey of prices, availability, affordability and price components in Shaanxi Province, China. PLoS ONE. 2014;9(3):e90365.
Droti B, O’Neill KP, Mathai M, Yao Tsidi Dovlo D, Robertson J. Poor availability of essential medicines for women and children threatens progress towards sustainable development goal 3 in Africa. BMJ Glob Health. 2019;4(Suppl 9):e001306.
Wang X, Yang S, Fang Y, Jiang M, Wu L. Study on the availability and price Pediatric essential Medicines in Retail Pharmacies in Shaanxi Province using WHO/HAI methodology. China Pharm. 2014;25:678–81.
Pujari N, Sachan A, Kumar YJIJoMS, Health P. Cross-sectional study on availability and affordability of some essential child-specific medicines in. Uttar Pradesh. 2016;5(10):1.
Sado E, Sufa A. Availability and affordability of essential medicines for children in the western part of Ethiopia: implication for access. BMC Pediatr. 2016;16:40.
Dorj G, Sunderland B, Sanjjav T, Dorj G, Gendenragchaa B. Availability, affordability and costs of pediatric medicines in Mongolia. BMC Pediatr. 2018;18(1):149.
Li S, Xu W, Du W, Fu Y. Study on the availability of pediatric essential medicines in China: based on the surveys in19 provinces. Chin J Health Policy. 2018;11:12–8.
Orubu ESF, Robert FO, Samuel M, Megbule D. Access to essential cardiovascular medicines for children: a pilot study of availability, price and affordability in Nigeria. Health Policy Plan. 2019;34(Supplement3):iii20–iii6.
Sun X, Wei J, Yao Y, Chen Q, You D, Xu X, Dai J, Yao Y, Sheng J, Li X. Availability, prices and affordability of essential medicines for children: a cross-sectional survey in Jiangsu Province, China. BMJ Open. 2018;8(10):e023646.
Martei YM, Iwamoto K, Barr RD, Wiernkowski JT, Robertson J. Shortages and price variability of essential cytotoxic medicines for treating children with cancers. BMJ Glob Health. 2020. https://doi.org/10.1136/bmjgh-2020-003282.
Dai Y, Li Z, Xu H, Zhu L, Zhu Y, Cheng H et al. A multicenter survey of the accessibility of EMC in China. Chin J Pediatr. 2020;301–7.
Faruqui N, Martiniuk A, Sharma A, Sharma C, Rathore B, Arora RS, Joshi R. Evaluating access to essential medicines for treating childhood cancers: a medicines availability, price and affordability study in New Delhi, India. BMJ Glob Health. 2019;4(2):e001379.
Wei G, Wang X, Li X, et al. A survey on the availability, price and affordability of essential medicine for children in Eastern China. Chin J Health Policy. 2019;12:72–8.
Wang X, Zhang A, Wang H, et al. Evaluation study on the availability and prices of paediatric essential medicines in Weifang. Chin Pharm Affairs. 2020;34:1085–92.
Tadesse T, Abuye H, Tilahun G. Availability and affordability of children essential medicines in health facilities of southern nations, nationalities, and people region, Ethiopia: key determinants for access. BMC Public Health. 2021;21(1):714.
Dinh DX, Nguyen HTT, Nguyen VM. Access to essential medicines for children: a cross-sectional survey measuring medicine prices, availability and affordability in Hanam province, Vietnam. BMJ Open. 2021;11(8):e051465.
Mensah KB, Mensah ABB, Bangalee V, Padayachee N, Oosthuizen F. Evaluating essential medicines for treating childhood cancers: availability, price and affordability study in Ghana. BMC Cancer. 2021;21(1):683.
World Health Organization. Global Action Plan for the prevention and control of noncommunicable diseases 2013–2020. 2013. https://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf?sequence=1&isAllowed=y. Accessed 4 Nov 2022.
Osinde G, Niyonzima N, Mulema V, Kyambadde D, Mulumba Y, Obayo S, Anecho E, Watera S, Constance M, Kadhumbula S, et al. Increasing access to quality anticancer medicines in low- and middle-income countries: the experience of Uganda. Future Oncol. 2021;17(21):2735–45.
Moye-Holz D, van Dijk JP, Reijneveld SA, Hogerzeil HV. Policy approaches to improve availability and affordability of medicines in Mexico - an example of a middle income country. Global Health. 2017;13(1):53.
Stolbrink M, Thomson H, Hadfield RM, Ozoh OB, Nantanda R, Jayasooriya S, Allwood B, Halpin DMG, Salvi S, de Oca MM, et al. The availability, cost, and affordability of essential medicines for asthma and COPD in low-income and middle-income countries: a systematic review. Lancet Glob Health. 2022;10(10):e1423–e42.
National Health Commission of the People’s Republic of China: Opinions of the General Office of the State Council on reforming and improving the supply guarantee and use policies of generic medicines. 2018. http://www.nhc.gov.cn/wjw/gwywj/201804/ac9eb7a6c3594ec4b419fd7fcb76a9a6.shtml. Accessed 4 Nov 2022.
Vyas M, de Vries EGE, Casali PG, Tabernero J. Shortages of inexpensive essential medicines. Lancet Oncol. 2019;20:e224–e25.
Fundytus A, Sengar M, Lombe D, Hopman W, Jalink M, Gyawali B, Trapani D, Roitberg F, De Vries EGE, Moja L, et al. Access to cancer medicines deemed essential by oncologists in 82 countries: an international, cross-sectional survey. Lancet Oncol. 2021;22(10):1367–77.
Vassal G, Kozhaeva O, Griskjane S, Arnold F, Nysom K, Basset L, et al. Access to essential anticancer medicines for children and adolescents in Europe. Ann Oncol. 2021;32:560–8.
Robertson J, Magrini N, Barr R, Forte G, Ondari C. Medicines for cancers in children: the WHO model for selection of essential medicines. Pediatr Blood Cancer. 2015;62(10):1689–93.
Mehta PS, Wiernikowski JT, Petrilli JA, Barr RD. Essential medicines for pediatric oncology in developing countries. Pediatr Blood Cancer. 2013;60(5):889–91.
Acknowledgements
Not applicable.
Funding
Science and Technology Plan Project of Sichuan Province (2020YFS0035) and the Fundamental Research Funds for the Central University (SCU2022D006).
Author information
Authors and Affiliations
Contributions
LLZ, KZ, ZC conceptualized and designed the study and offered methodological guidance; YQS, ZC and DL screened the literature, YQS and ZC extracted the data, accessed the quality of studies and wrote the draft of the manuscript; all authors contributed to critical revision of the manuscript and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable
Competing interest
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article has been updated to amend the readability of figure 6.
Electronic supplementary material
Below is the link to the electronic supplementary material.
12889_2023_15820_MOESM1_ESM.docx
Supplementary Table 1. Search strategy. Supplementary Table 2. Quality assessment of included studiesusing the Joanna Briggs Institute?JBI?tool. Supplementary Table 3. The lists of essential medicines for children in included studies Supplementary Table 4. The global availability of essential medicines for children from 2009-2015. Supplementary Table 6. Characteristics of excluded studies
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shi, Y., Chen, Z., Zou, K. et al. Global, regional and national availability of essential medicines for children, 2009–2020: a systematic review and meta-analysis. BMC Public Health 23, 1185 (2023). https://doi.org/10.1186/s12889-023-15820-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15820-7