
Abstract
Background
Children with the most severe parental mental health conditions have an elevated risk of numerous adversities including somatic morbidity. However, there is no knowledge concerning physical health in most children affected by parental mental health conditions. Therefore, the aim was to examine the association between different severities of parental mental health conditions and somatic morbidity in children of different age-groups and further explore the combinations of maternal and paternal mental health conditions on child somatic morbidity.
Methods
In this register-based cohort study, we included all children born in Denmark between 2000–2016 and linked parents. Parental mental health conditions were categorised into four severity groups (no, minor, moderate, and severe). Somatic morbidity in offspring was categorised into broad disease categories corresponding to the International Classification of Diseases. We estimated the risk ratio (RR) using Poisson regression, of the first registered diagnosis in different age-groups.
Results
Of the around 1 million children in the study > 14.5% were exposed to minor parental mental health conditions and < 2.3% were exposed to severe parental mental health conditions. Overall, the analyses revealed a higher risk of morbidity in exposed children across all disease categories. The strongest association was observed for digestive diseases in children aged < 1 year exposed to severe parental mental health conditions (RR: 1.87 (95% CI: 1.74–2.00). Generally, the risk of somatic morbidity increased the more severe the parental mental health conditions. Both paternal and especially maternal mental health conditions were associated with a higher risk of somatic morbidity. The associations were strongest if both parents had a mental health condition.
Conclusion
Children with different severities of parental mental health conditions experience a higher risk of somatic morbidity. Although children with severe parental mental health conditions had the highest risk, children with minor parental mental health conditions should not be neglected as more children are exposed. Children with both parents having a mental health condition were the most vulnerable to somatic morbidity and maternal mental health conditions were more strongly associated with somatic morbidity than paternal. More support and awareness of families with parental mental health conditions is highly needed.
Similar content being viewed by others

Introduction
Two in five children grow up with parents suffering from mental health conditions [1] which adversely affects the children due to multiple deprivations [2]. However, only recently improving these children’s lives and well-being has become a public health priority [3,4,5]. Children’s physical health is highly important as illness and school absence entail detrimental consequences on the child’s social and academic development as well as a strain on the entire family. Furthermore, health inequality in childhood often perseveres into adulthood [6, 7]. Still, most information obtainable regarding children exposed to parental mental health conditions concerns their higher risk of developing mental health conditions themselves [5, 8, 9]. Notably little is known about these children’s physical health, even though unfavourable experiences in foetal life and childhood, such as exposure to parental mental health conditions, can cause a stress response, which is suggested leading to immune dysregulation [10,11,12]. Furthermore, mental health conditions might also have an impact on parenting behaviour [13,14,15,16] which, like environmental adversities, could be a component in children’s physical health [17, 18].
Studies examining somatic morbidity in children exposed to parental mental health conditions have mainly focused on mothers with depression, in particularly postpartum depression, and are mostly limited to asthma, injuries, and obesity [5]. Few other studies also indicate higher risk of epilepsy [19] and eczema [20, 21] in children of mothers with depression or schizophrenia. Thus in general, the father seems vastly neglected in the literature despite an increasing emphasis on paternal mental health conditions adversely affecting development upon offspring [22, 23].
To our knowledge, merely two studies have examined the risk of somatic morbidity across several disease categories in the offspring of parents with mental health conditions. Both studies found a higher risk in most of the categories for the examined age-groups (0–6 years [24] and 0–30 years [25]). However, these studies only focused on severe parental mental health conditions such as schizophrenia and bipolar disorder [24, 25]. Since only very few (2.2%) of the children with parental mental health conditions in Denmark have parents with a severe mental health condition [1], there is no knowledge concerning physical health in the majority of children with parental mental health conditions.
Aim
In order to accommodate the lacking knowledge of physical health in children affected by parental mental health conditions, this explorative study aimed to describe the morbidity in different age-groups of children with parental mental health conditions. Further, we aimed to examine whether there were differences in the risk regarding the severity of parental mental health conditions and explore the combinations of paternal and maternal mental health conditions concerning children’s somatic morbidity.
Methods
Design
This study was designed as a Danish nationwide register-based cohort study, with three different embedded cohorts. These cohorts were identified as cohort 1, encompassing the infant year (i.e., children below the age of 1 year), cohort 2 covering the preschool years (i.e., children between the ages of 1 to 5 years), and cohort 3 representing the schoolyears (i.e., children between the ages of 6 to 16 years). See Fig. 1.

Illustration of the study design with three embedded cohorts. Legend: Children were followed in each cohort from baseline (start of the arrow) until end of the arrow or until their first registered diagnosis in each disease category, death, emigration, or end of follow-up on 31 December 2017, whichever came first
Setting
Danish health care is universal and tax funded. In primary care, the general practitioner serves as a gatekeeper to secondary (specialised) care including referrals to in- and outpatient hospital care [26].
Data sources
Information on children’s somatic morbidity was obtained from the Danish National Patient Registry [27]. Data on the parents’ mental health condition was obtained from the following Danish nationwide registers: From the Danish National Patient Registry [27] we collected information on psychiatric disorders diagnosed at any Danish psychiatric hospital. The Danish National Health Service Register [28] provided information on contacts to general practitioners, private psychiatrists, and psychologists. From The Danish National Prescription Registry [29] we obtained information on redeemed prescriptions at Danish Pharmacies.
Data regarding the birth of the child, death, emigration, and residence of both the parents and the child were obtained from Statistics Denmark’s register on the population.
Statistics Denmark conducted the anonymisation of data and linkage between databases on an individual level using the personal registration number, a unique identifier assigned all residents and used in all Danish public registers [30].
Study population
We identified all children born in Denmark in the period between 1 January 2000 to 31 December 2016 and their corresponding parents. Regarding the three embedded cohorts: cohort 1 included all liveborn children in Denmark in the period. Children were included in cohort 2 on their 1st birthday and included in cohort 3 on their 6th birthday (see Fig. 1). Thus, children could appear in more than one cohort.
Children were excluded if their parents could not be ascertained for, in the specific exposure period or if the children were not living in Denmark at baseline for each cohort. Furthermore, we planned to exclude children if both parents had missing personal registration number. However, all mothers could be linked.
Variables
Exposure
Mental health conditions of the parents were classified into four mutually exclusive severity groups (no, minor, moderate, and severe) as described in Table 1. The most severe mental health condition of either parent defined the exposure group of the child. For the analysis regarding combinations of paternal and maternal mental health conditions moderate and severe mental health conditions were combined, due to numerous combinations and few children exposed to severe mental health conditions resulting in a moderate/severe exposure group.
Since mental health conditions often are recurrent or enduring [31], and 75% of parents in a Danish survey reported that their mental health condition lasted more than five years [32], all three severity groups in cohorts 1 and 2 were considered for a five-year period prior to baseline. To include the child’s entire lifetime until baseline, exposure of the parents was, in cohort 3, measured in a six-year period (see Fig. 1 and Table 1).
Outcome
Morbidity in children was categorised into eighteen overall disease categories corresponding to the International Classification of Diseases, Tenth Revision (ICD-10) [33]. Each disease category was analysed as a separate outcome within the different cohorts. Furthermore, we included death as an outcome of interest.
For the analysis regarding the combinations of maternal and paternal mental health conditions, the two most common paediatric disease categories were chosen (infectious and respiratory diseases).
Titles of the overall disease category with corresponding ICD-10 codes and short descriptions applied in Figs. 3 and 4 are available in table s1 in Supplementary. (see Additional file 1).
Follow-up
Children were followed in each cohort from baseline until their first registered diagnosis in each disease category, death, emigration, or end of follow-up on 31 December 2017, whichever came first. Additionally, children were followed differently in the three cohorts: from birth until the day before their first birthday (cohort 1), the day on their first birthday until the day before their sixth birthday (cohort 2), and the day on their sixth birthday until the day before their seventeenth birthday (cohort 3) (see Fig. 1).
Statistics
Within each of the three cohorts, the proportion of children with a registered diagnosis was calculated in each disease category for all severities of parental mental health conditions – that is, a father and/or a mother with either no, minor, moderate, or severe mental health conditions. The total number and proportion of children diagnosed in each category can be seen in Supplementary table s2.
Poisson regression was used to estimate the risk ratio (RR) and 95% confidence interval (CI). Some children in cohorts 2 and 3 were by design lacking complete follow-up. These children were considered without somatic morbidity if no diagnosis was registered during their actual follow-up period. Children with no parental mental health conditions were considered the reference group for all analyses.
For the analysis regarding the combinations of paternal and maternal mental health conditions on child physical health, eight different exposure groups were generated. The eight exposure groups then consisted of the different combinations of paternal and maternal mental health conditions – as for instance both the mother and the father having minor mental health conditions, or only one parent having minor mental health condition, or the mother with moderate/severe and father with minor mental health conditions and so forth.
With the aim of describing morbidity that might be overrepresented in children exposed to different severities of parental mental health conditions, no adjustments were conducted, except for the adjustment of the child’s birthyear, since the study sample extends numerous calendar years and the occurrence of parental mental health conditions increased during the study period. Each birthyear was modelled as its own baseline risk.
Results
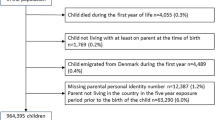
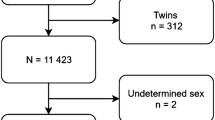
A total of 1,028,587 children in cohort 1, 965,253 children in cohort 2 and 680,799 children in cohort 3 fulfilled the inclusion criteria (see Fig. 2).

Flowchart of the inclusion, exclusion, and final study population in all three cohorts
Exposed children were especially exposed to minor parental mental health conditions with 14.5%, 15% and 22.6% in cohorts 1,2 and 3, respectively. About 10%-13% were exposed to moderate parental mental health conditions and less than 2.3% to severe parental mental health conditions.
Table 2 presents the proportion of children diagnosed in the eighteen overall disease categories along with death in the different exposure groups of parental mental health conditions. In cohort 1 (children < 1 year) the most common diagnosis originated in the perinatal period (ICD-10: P00-P99). Injuries (ICD-10: S00-T98) were numerous in cohort 2 (children aged 1–5 years) and cohort 3 (children aged 6–16 years). Furthermore, abnormal symptoms not elsewhere classified (ICD-10: R00-R99) were also highly present in children of all three cohorts.
Across all three cohorts and in most disease categories, the proportion of children registered with a diagnosis was higher the more severe the parental mental health condition.
Respiratory diseases (ICD-10: J00-J99) were the most commonly defined paediatric somatic morbidity across all three cohorts following infectious and parasitic diseases (ICD-10: A00-B99).
The overall number and total proportion of children diagnosed in each cohort and disease category is available in Supplementary table s2.
Figure 3 presents the risk ratios (RR) of children with different severities of parental mental health conditions in every disease category within each cohort, compared to children with no parental mental health condition. The exact RR estimates and confidence intervals are available in Supplementary table s3. Besides mental and behavioural disorders in all three cohorts, the strongest association in cohort 1 was observed for diseases of the digestive system (ICD-10: K00-K99) where children with severe parental mental health conditions had 87% (95% CI: 74–100%) higher risk compared to children with no parental mental health conditions. In cohort 2 the strongest association was found for diseases within the nervous system (ICD-10: G00-G99) where children with severe parental mental health conditions had 83% (95% CI: 63–104%) higher risk. Not considering death, the strongest association in cohort 3 was observed for endocrine, nutritional and metabolic diseases (ICD-10: E00-E90) where children exposed to moderate parental mental health conditions had 46% (95% CI: 41–51%) and children with severe parental mental health conditions also had 46% (95% CI: 35–58%) higher risk than children not exposed.

Risk ratio of registered diagnosis for children according to parental mental health conditions. Legend: Risk ratios for children exposed to different severities of parental mental health conditions with a registered diagnosis in each disease category were adjusted for birth year. International Classification of Diseases, Tenth Revision (ICD-10) codes – Infectious (ICD-10: A00-B99), Neoplasm (ICD-10: C00-D48), Blood (ICD-10: D50-D89), Endocrine (ICD-10: E00-E99), Mental (ICD-10: F00-F99), Nervous system (ICD-10: G00-G99), Eye (ICD-10: H00-H59), Ear (ICD-10: H60-H99), Circulatory (ICD-10: I00-I99), Respiratory (ICD-10: J00-J99), Digestive (ICD-10: K00-K93), Skin (ICD-10: L00-L99), Musculoskeletal (ICD-10: M00-M99), Genitourinary (ICD-10: N00-N99), Perinatal (ICD-10: P00-P96): Not relevant for cohort 2 and 3, Malformations (ICD-10: Q00-Q99), Other symptoms (ICD-10: R00-R99) and Injury (ICD-10: S00-T98)
Regarding death in all three cohorts, children exposed to parental mental health conditions had a higher risk. In cohort 1 children exposed to severe parental mental health conditions had a 46% (95% CI: 15–85%) higher risk of death than children not exposed. Similarly higher risk was found in children exposed in cohorts 2 and 3. However, in these two cohorts, only a few died during the study period resulting in very broad confidence intervals.
Overall, the analyses revealed a higher risk of morbidity in exposed children across all disease categories within each cohort except neoplasm in cohort 3. Furthermore, in most disease categories the overall results indicate a pattern of an increased risk of somatic morbidity in children the more severe the parental mental health condition (Fig. 3).
Generally, RR of both respiratory and infectious diseases (the two most commonly defined diagnoses) were higher for children with only maternal mental health conditions, than for children exposed to only paternal mental health conditions (Fig. 4). However, children with paternal mental health conditions also had a higher risk than children with no parental mental health conditions. The risk was higher if both parents had a mental health condition, and children exposed to both a mother and father with moderate/severe mental health conditions had the highest risk of respiratory and infectious diseases. The confidence intervals are available in Supplementary table s4-s9.

Risk ratio for infectious and respiratory diseases according to combined severity of paternal and maternal mental health conditions. Legend: Risk ratios were adjusted for birth year
Discussion
In this nationwide cohort study, we describe and quantify a higher risk of somatic morbidity in children of different age-groups exposed to parental mental health conditions. Overall, this analysis discloses a somewhat poor physical health among these children indicated by an elevated risk across nearly all broad disease categories. Furthermore, in most disease categories and all age-groups of children, our results revealed a pattern of a higher risk the more severe the parental mental health condition. However, the large group of children exposed to minor parental mental health conditions also had a higher risk of somatic morbidity compared to children not exposed.
Both paternal and maternal mental health conditions were associated with a higher risk of infectious and respiratory diseases. However, associations were stronger for maternal mental health conditions than paternal. Children doubly exposed to a mother and father with moderate/severe mental health conditions had the most elevated risk of being diagnosed with an infectious and/or respiratory disease.
The direction of a higher risk of somatic morbidity across a broad range of disease categories in children with severe parental mental health conditions found in this explorative study is consistent with two other Danish nationwide studies [24, 25]. Although these children generally had the highest risk of being diagnosed, they merely concern a small proportion of the total study population. Our study revealed that children with minor parental mental health conditions also had a higher risk of poor physical health than children with no parental mental health conditions. This supports previous studies examining children exposed to minor parental mental health conditions that found a higher risk of asthma [34] and functional gastrointestinal disorder [35]. Thus, children with minor mental health conditions comprise a markedly large group that should not be disregarded.
It seems highly tempting to conclude that the higher risk of being diagnosed with somatic morbidity among children exposed to parental mental health conditions may be explained by an inappropriate parental utilization of healthcare. As reported by other studies, children of parents with mental health conditions are less likely to attend preventive healthcare such as routine childcare visits and childhood vaccinations [36, 37], though, more likely to use both primary and acute healthcare [38, 39]. Some might suggest that this higher frequency of healthcare use could be related to parental health anxiety. However, this study found that children with parental mental health conditions have a higher risk of being diagnosed with any somatic morbidity by a clinical specialist in secondary care. This may insinuate that the higher frequency of parental utilization of healthcare instead is compelled by a genuinely elevated need for healthcare regarding children with parental mental health conditions.
Mechanisms underlying this inequality are unknown, however, some evidence links early life and foetal life stressors, such as parental mental health conditions, to higher rates of mortality and morbidity from several chronic diseases through immune dysregulation [12]. Furthermore, children born of mothers with mental health conditions have a higher risk of being born prematurely [40] which affects both morbidity and mortality [41]. Although neonatal mortality has reduced [41], the association between maternal mental health conditions and preterm birth may especially explain some of the higher risk of death found in children aged below 1 year in cohort 1.
Other mechanisms could be related to parental health behaviour and health literacy, where parents’ mental health conditions may interfere with their capacity to understand and follow health advice from healthcare professionals on behalf of their child. Additionally, mental health conditions are associated with smoking and second-hand smoking in children has been causally linked to a higher risk of several diseases such as e.g. asthma and middle ear infections [42].
Mental health conditions may also negatively impact upon parenting behaviour [13,14,15,16], which could be a component in the poor physical health found in children with parental mental health conditions, as fundamental needs might be neglected. Our results indicate that a child with maternal mental health conditions and no paternal mental health conditions has a higher risk of infectious and/or respiratory diseases than a child with paternal mental health conditions and no maternal mental health conditions. This result might be explained by different gender household roles, where mothers most often take primary charge of child upbringing and overall care [43] and children more frequently cohabitate with their mother if parents do not cohabitate [44]. However, children with paternal mental health conditions still have a higher risk of somatic morbidity, thus, fathers and these children should not be neglected.
Strengths and limitations
This study comprises several strengths by using high-quality and valid data from the national Danish registers covering the entire population [30, 45]. This enabled the examination of somatic morbidity in children exposed to different severities of parental mental health conditions across a broad range of disease categories in three large cohorts.
By including data on medication and data from primary care, we were able to include minor parental mental health conditions, which are often undiagnosed and treated alone by general practitioners [46], therefore often not included in register-based studies using hospital data [47]. To our knowledge, this is the only study including different severities of parental mental health conditions on child physical health.
There are also some limitations to this study. Obtaining information from the registers solely allowed for the identification of children exposed to parental mental health conditions if their parents actually had sought medical care. Therefore, some children whose parents had mental health conditions may have been misclassified as not exposed. This misclassification may have underestimated the association.
For some chronic diseases, recurrent children may occur in the three different cohorts, which may explain some of the similar patterns found in the three cohorts. However, this pattern is also found in e.g., infectious diseases which are not chronic. In addition, recurrent children thus are repeatedly hospitalized and diagnosed by a clinical specialist during the altered follow-up period within the different cohorts.
We did not consider if the child in fact was living with the parent suffering from mental health conditions, although severe parental mental health conditions, especially parental schizophrenia, are a strong predictor of the child being placed in out-of-home care [48]. However, children might still be affected by their mentally ill parent suffering although they are not living with that particular parent.
Implication of findings
The overall higher risk of somatic morbidity predicted in children with minor, moderate or severe parental mental health conditions found in this study suggest a renewed emphasis upon these children’s physical health from both health professionals and politicians. Although, for some of the disease categories, the absolute differences were modest, we still find our results of great public health importance since parental mental health conditions concern a significantly large group of children [1]. Due to the excess cost used annually on e.g., hospital admissions among these children [9], targeted interventions may create public health benefits not only for the child and family, however also for government resources that are limited.
Our findings indicate that even within the first year of life children with parental mental health conditions require additional healthcare compared to children with no parental mental health conditions. This emphasises the need for early interventions perhaps even during pregnancy. From a public health perspective, it seems highly obvious that preventive interventions should be prioritised in these families. Such interventions may include supportive social networks and improvement of parenting behaviour and parental health literacy. However, solely based on this study no comprehensive improvement recommendations for such interventions can be made. Hence, future research is highly needed to examine other variables that yield the higher risk of somatic morbidity in children with different severities of parental mental health conditions observed in this study, in order to generate new hypotheses and hereafter concentrate on improving intervention strategies supporting these families.
Conclusion
Children with parental mental health conditions experience an overall poor physical health with an elevated risk across most broad disease categories. Generally, the risk of somatic morbidity increased the more severe the parental mental health condition. However, minor parental mental health conditions should not be neglected since this concerns a substantially large group of children.
Children with both parents having moderate/severe mental health conditions were the most vulnerable to somatic morbidity. Furthermore, paternal, and maternal mental health conditions were individually associated with a higher risk of somatic morbidity. However, associations were stronger for maternal mental health conditions than paternal.
More support and awareness of children exposed to different severities of parental mental health conditions physical health is highly needed.
Availability of data and materials
The data that supports the results of this study is accessible from Statistics.
Denmark. However, restrictions do apply to the availability, so data are not publicly available. Questions or requests regarding this data must be directed to the corresponding author Camilla Klinge Renneberg.
References
Christesen AMS, Knudsen CK, Fonager K, Johansen MN, Heuckendorff S. Prevalence of parental mental health conditions among children aged 0–16 years in Denmark: A nationwide register-based cross-sectional study. Scand J Public Health. 2021:1–9.
Maybery D, Ling L, Szakacs E, Reupert A. Children of a parent with a mental illness: perspectives on need. Aust e-J Adv Ment Heal. 2005;4:78–88.
Abel KM, Bee P, Gega L, Gellatly J, Kolade A, Hunter D, et al. An intervention to improve the quality of life in children of parents with serious mental illness: The young smiles feasibility rct. Health Technol Assess (Rockv). 2020;24:1–136.
Abel KM, Hope H, Swift E, Parisi R, Ashcroft DM, Kosidou K, et al. Prevalence of maternal mental illness among children and adolescents in the UK between 2005 and 2017: a national retrospective cohort analysis. Lancet Public Heal. 2019;4:e291-300.
Pierce M, Hope HF, Kolade A, Gellatly J, Osam CS, Perchard R, et al. Effects of parental mental illness on children’s physical health: Systematic review and meta-analysis. Br J Psychiatry. 2020;217:354–63.
Pearce A, Mason K, Fleming K, Taylor-Robinson D, Whitehead M, WHO Europe. Reducing inequities in health across the life-course: Early years, childhood and adolescence. 2020.
G. Irwin L, Siddiqi A, Hertzman C. Early child development: a powerful equalizer final report. 2007:1–41.
Rasic D, Hajek T, Alda M, Uher R. Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: A meta-analysis of family high-risk studies. Schizophr Bull. 2014;40:28–38.
Hope H, Osam CS, Kontopantelis E, Hughes S, Munford L, Ashcroft DM, et al. The healthcare resource impact of maternal mental illness on children and adolescents: UK retrospective cohort study. Br J Psychiatry. 2021;219:515–22.
Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Heal. 2017;2:e356–66.
Danese A, McEwen BS. Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiol Behav. 2012;106:29–39.
Fagundes CP, Glaser R, Kiecolt-Glaser JK. Stressful early life experiences and immune dysregulation across the lifespan. Brain Behav Immun. 2013;27:8–12.
Aarestrup AK, SkovgaardVæver M, Petersen J, Røhder K, Schiøtz M. An early intervention to promote maternal sensitivity in the perinatal period for women with psychosocial vulnerabilities: Study protocol of a randomized controlled trial. BMC Psychol. 2020;8:1–13.
Lovejoy MC, Graczyk PA, O’Hare E, Neuman G. Maternal depression and parenting behavior: A meta-analytic review. Clin Psychol Rev. 2000;20:561–92.
Fagundes CP, Bennett JM, Derry HM, Kiecolt-Glaser JK. Relationships and Inflammation across the Lifespan: Social Developmental Pathways to Disease. Soc Personal Psychol Compass. 2011;5:891–903.
Campbell SB, Brownell CA, Hungerford A, Spieker SJ, Mohan R, Blessing JS. The course of maternal depressive symptoms and maternal sensitivity as predictors of attachment security at 36 months. Dev Psychopathol. 2004;16:231–52.
Pearce A, Dundas R, Whitehead M, Taylor-Robinson D. Pathways to inequalities in child health. Arch Dis Child. 2019;104:998–1003.
Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults - The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14:245–58.
Gunnarsdóttir ED, Hällgren J, Hultman CM, McNeil TF, Crisby M, Sandin S. Risk of neurological, eye and ear disease in offspring to parents with schizophrenia or depression compared with offspring to healthy parents. Psychol Med. 2018;48:2710–6.
Hamann CR, Egeberg A, Silverberg JI, Gislason G, Skov L, Thyssen JP. Exploring the association between parental psychiatric disease and childhood atopic dermatitis: a matched case–control study. J Eur Acad Dermatology Venereol. 2019;33:725–34.
McKenzie C, Silverberg JI. Maternal Depression and Atopic Dermatitis in American Children and Adolescents. Dermatitis. 2020;31:75–80.
Sweeney S, MacBeth A. The effects of paternal depression on child and adolescent outcomes: A systematic review. J Affect Disord. 2016;205:44–59.
Harewood T, Vallotton CD, Brophy-Herb H. More than just the breadwinner: the effects of fathers’ parenting stress on children’s language and cognitive development. Infant Child Dev. 2017;26:1–19.
Davidsen KA, Munk-Laursen T, Foli-Andersen P, Ranning A, Harder S, Nordentoft M, et al. Mental and pediatric disorders among children 0–6 years of parents with severe mental illness. Acta Psychiatr Scand. 2022;145:244–54.
Ranning A, Benros ME, Thorup AAE, Davidsen KA, Hjorthøj C, Nordentoft M, et al. Morbidity and mortality in the children and young adult offspring of parents with schizophrenia or affective disorders-a nationwide register-based cohort study in 2 million individuals. Schizophr Bull. 2020;46:130–9.
Schmidt M, Schmidt SAJ, Adelborg K, Sundbøll J, Laugesen K, Ehrenstein V, et al. The Danish health care system and epidemiological research: From health care contacts to database records. Clin Epidemiol. 2019;11:563–91.
Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National patient registry: A review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–90.
Sahl Andersen J, De Fine ON, Krasnik A. The Danish national health service register. Scand J Public Health. 2011;39:34–7.
Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: The Danish national prescription registry. Int J Epidemiol. 2017;46:798.
Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29:541–9.
Hardeveld F, Spijker J, De GR, Nolen WA, Beekman ATF. Recurrence of major depressive disorder and its predictors in the general population : results from The Netherlands Mental Health Survey and Incidence Study (NEMESIS). Psychol Med. 2013;43:39–48.
Psykiatrifonden [Danish Mental Health Fund]. Undersøgelse af forekomst af psykisk sygdom blandt foraeldre til børn i alderen 0–18 år [Study of the prevalence of mental illness among parents of children aged 0–18 years]. 2019.
WHO. International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). https://icd.who.int/browse10/2019/en#/II.
Heuckendorff S, Johansen MN, Overgaard C, Johnsen SP, Kelly Y, Fonager K. Parental mental health, socioeconomic position and the risk of asthma in children - a nationwide Danish register study. Eur J Public Health. 2022;32:14–20.
Heuckendorff S, Johansen MN, Overgaard C, Johnsen SP, Thomsen JL, Fonager K. Six-year-old children had greater risks of functional gastrointestinal disorders if their parents had mental health conditions. Acta Paediatr Int J Paediatr. 2022;111:2029–37.
Lyngsøe BK, Vestergaard CH, Rytter D, Vestergaard M, Munk-Olsen T, Bech BH. Attendance of routine childcare visits in primary care for children of mothers with depression: A nationwide population-based cohort study. Br J Gen Pract. 2018;68:e97-104.
Davidsen KA, Christiansen E, Haubek D, Asmussen J, Ranning A, Thorup AAE, et al. Parental mental illness, attendance at preventive child healthcare and dental caries in the offspring: a nation-wide population-based cohort study. Soc Psychiatry Psychiatr Epidemiol. 2021;56:583–92.
Heuckendorff S, Johansen MN, Johnsen SP, Overgaard C, Fonager K. Parental mental health conditions and use of healthcare services in children the first year of life – a register-based, nationwide study. BMC Public Health. 2021;21:1–12.
Lyngsøe BK, Rytter D, Munk-Olsen T, Vestergaard CH, Christensen KS, Bech BH. Maternal depression and primary healthcare use for children: a population-based cohort study in Denmark. Br J Gen Pract. 2019:182–9.
Knudsen CK, Christesen AMS, Heuckendorff S, Fonager K, Johansen MN, Overgaard C. The risk of preterm birth in combinations of socioeconomic position and mental health conditions in different age groups: a Danish nationwide register-based cohort study. BMC Pregnancy Childbirth. 2021;21:1–11.
Vogel JP, Chawanpaiboon S, Moller AB, Watananirun K, Bonet M, Lumbiganon P. The global epidemiology of preterm birth. Best Pract Res Clin Obstet Gynaecol. 2018;52:3–12.
Orton S, Jones LL, Cooper S, Lewis S, Coleman T. Predictors of children’s secondhand smoke exposure at home: A systematic review and narrative synthesis of the evidence. PLoS One. 2014;9.
Ralph D. ‘Who should do the caring’? Involved fatherhood and ambivalent gendered moral rationalities among cohabiting/married Irish parents. Commun Work Fam. 2016;16:63–79.
Ranning A, MunkLaursen T, Thorup A, Hjorthøj C, Nordentoft M. Children of parents with serious mental illness: with whom do they grow up? A prospective, population-based study. J Am Acad Child Adolesc Psychiatry. 2016;55:953–61.
Thygesen LC, Daasnes C, Thaulow I, Brønnum-Hansen H. Introduction to Danish (nationwide) registers on health and social issues: Structure, access, legislation, and archiving. Scand J Public Health. 2011;39:12–6.
Goldberg DP, Goodyer IM. The origins and course of common mental disorders. 1st ed. New York: Routledge; 2005.
Hvidberg MF, Johnsen SP, Glümer C, Petersen KD, Olesen AV, Ehlers L. Catalog of 199 register-based definitions of chronic conditions. Scand J Public Health. 2016;44:462–79.
Ranning A, Laursen TM, Thorup A, Hjorthøj C, Nordentoft M. Serious mental illness and disrupted caregiving for children: A nationwide, register-based cohort study. J Clin Psychiatry. 2015;76:e1006–14.
Acknowledgements
Not applicable.
Funding
This study was funded by Helsefonden (grant number: 22-B-0173).
Helsefonden did not in any way influence the design nor conduct the study. Neither did they influence the analysis and interpretation of data or review/approve the manuscript before the submission.
Author information
Authors and Affiliations
Contributions
CKR, RBKB, SH, BHB and KF contributed to the planning, design, analysis, and interpretation of data. RBKB performed data management. CKR performed statistical analyses and drafted the manuscript. CKR, RBKB, SH, BHB and KF contributed to the review and revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The STROBE guidelines were applied for the reporting of this study and all methods were performed according to relevant regulations and guidelines, including the 1975 Declaration of Helsinki. This project fulfils The Act on Processing of Personal Data in Denmark (Act No. 429 of May 31, 2000), which obeys the European Union Directive 95/46/EC on the protection of human individuals. The data usage and project were approved by the Danish Data Protection Agency (Region North of Denmark – Approval number 2019–2078). Furthermore, the legal and ethical parts of the study were approved by Statistics Denmark (account number 707196). All data was acquired from already existing administrative national registries and Statistics Denmark conducted the anonymity of data before researchers gained access. The paper of this study solely includes aggregated results and no personal data. This study is register-based and according to Danish Law (available at: www.nvk.dk/english/act-on-research), register-based studies require neither approval by ethical or scientific committees nor written informed consent and therefore no requirement of informed consent (neither oral nor written) from parents/guardians of minors included in this study is needed.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplementary table s1. Titles of overall disease category with corresponding ICD-10 codes and short description applied in Figs. 3 and 4 in main manuscript. Supplementary table s2. The overall number and total proportion of children diagnosed in each cohort and disease category. Supplementary table s3. Risk ratio (RR) and 95% confidence interval (CI) for children exposed to different severities of parental mental health conditions with a registered diagnoses in each disease category within all three cohorts. Supplementary table s4. Risk ratio for infectious diseases according to combined severity of paternal and maternal mental health conditions cohort 1. Supplementary table s5. Risk ratio for respiratory diseases according to combined severity of paternal and maternal mental health conditions cohort 1. Supplementary table s6. Risk ratio for infectious diseases according to combined severity of paternal and maternal mental health conditions cohort 2. Supplementary table s7. Risk ratio for respiratory diseases according to combined severity of paternal and maternal mental health conditions cohort 2. Supplementary table s8. Risk ratio for infectious diseases according to combined severity of paternal and maternal mental health conditions cohort 3. Supplementary table s9. Risk ratio for respiratory diseases according to combined severity of paternal and maternal mental health conditions cohort 3.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Renneberg, C.K., Brund, R.B.K., Heuckendorff, S. et al. Children of parents with different severities of mental health conditions have higher risk of somatic morbidity: a Danish nationwide register-based cohort study. BMC Public Health 23, 810 (2023). https://doi.org/10.1186/s12889-023-15714-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15714-8