
Abstract
Background
Childhood overweight and obesity levels are rising and becoming a concern globally. In Costa Rica, the prevalence of these conditions has reached alarming values. Spatial analyses can identify risk factors and geographical patterns to develop tailored and effective public health actions in this context.
Methods
A Bayesian spatial mixed model was built to understand the geographic patterns of childhood overweight and obesity prevalence in Costa Rica and their association with some socioeconomic factors. Data was obtained from the 2016 Weight and Size Census (6 - 12 years old children) and 2011 National Census.
Results
Average years of schooling increase the levels of overweight and obesity until reaching an approximate value of 8 years, then they start to decrease. Moreover, for every 10-point increment in the percentage of homes with difficulties to cover their basic needs and in the percentage of population under 14 years old, there is a decrease of 7.7 and 14.0 points, respectively, in the odds of obesity. Spatial patterns show higher values of prevalence in the center area of the country, touristic destinations, head of province districts and in the borders with Panama.
Conclusions
Especially for childhood obesity, the average years of schooling is a non-linear factor, describing a U-inverted curve. Lower percentages of households in poverty and population under 14 years old are slightly associated with higher levels of obesity. Districts with high commercial and touristic activity present higher prevalence risk.
Similar content being viewed by others


Background
According to the World Health Organization (WHO) [1], the combined prevalence of overweight and obesity among children and adolescents aged 5-19 worldwide, has risen from 4% in 1975 to 18% in 2016, becoming one of the most significant global public health challenges of the 21st century [2]. Besides the immediate health effects like breathing difficulties, increased risk of fractures, hypertension, early markers of cardiovascular disease, and insulin resistance, this condition tends to persist into adulthood, deriving in a higher chance of premature death and disability [1]. In Costa Rica, the latest Weight and Size Census carried out in 2016 showed that overweight and obesity combined prevalence has reached a concerning 34.5% among children in school age (6-12) [3] for which the need to give an effective and timely response has been recognized [4].
The key determinant of weight gain in children is simply the surpassing of caloric consumption over expenditure, however, family and community related factors affect individual habits and behaviors that leads to this imbalance [5, 6]. Recent research has focused on the study of these kind of drivers in a broader ecological context [7, 8] in which population health and environment are interdependent in both micro (e.g., homes, schools) and macro (e.g., food distribution, urban/rural development) levels [9]. The intrinsic geographic nature of this approach and the resulting benefits of knowing where interventions are needed and if they were successful (critical in developing countries where resources are scarce) have encouraged the use of spatial statistics in obesity research and public health policy implementation [10].
In spatial statistical modeling, characterizing the autocorrelation of observations is clearly a subject of primary analytical interest, based on the fact that measures in a close spatial proximity tend to be more similar than others spatially separated and on the basic necessity to answer the “how much is where” question of georeferenced data [11]. Methodologically speaking, if spatial effects exist but are not accounted for in a model, the resulting estimates may be unreliable [12]. The Bayesian version of this kind of models is a flexible and robust approach to situations where both explanatory variables and spatial correlation must be considered [13].
Literature counting with a geographic component dedicated to the associations between weight and socioenvironmental factors has been growing recently [14]. Examples targeted specifically to children can be found in both developed and developing countries [15,16,17,18], with the limitation of being generally oriented to just one simultaneous categorical response (overweight, obesity or their combination). Even in restricted cases in which several nutritional states were contemplated [19, 20], overweight and obesity were not included as separated conditions, although, their relationships with certain determinants, their health implications over overall health and consequent interventions can differ. In Costa Rica, this distinction is present in the current approach to non-communicable diseases [21]. Gamboa et al. [22] already examined both conditions individually and their link with one socioeconomic status variable in this country, yet, spatial effects were not taken into account.
In this study, a Bayesian multinomial model was built using aggregated Census data to contribute to the understanding of overweight and obesity district prevalence as separate conditions for school-aged children in Costa Rica, by exploring their associations with certain socioeconomic characteristics and their respective geographic distributions and exceedance probabilities with respect to national health goals.
Methods
Study region
Costa Rica is a country in Central America, bordered by Nicaragua, Panama, the Caribbean Sea, and the Pacific Ocean. It has a land area of 51,180 \(\text {km}^2\) administratively divided into seven provinces, 82 cantons and 489 districts. A population of about 5.1 million people resides in this territory; an estimated of 72.8% in urban areas [23]. It is considered an upper middle-income country, characterized by solid human development indicators, among them, one of the lowest poverty rates in Latin America [24], but also by its unsuccessful efforts to reduce it during the last 25 years, not to mention an extremely high inequality, with a Gini index of 47.8 [25]. Costa Rica is also characterized by its almost universal health care coverage and its historic investment in health promotion and prevention strategies. The Ministry of Health is the entity responsible for the overall stewardship of the health system with a focus on health promotion. It is in charge of strategic planning, sanitary regulation, research, and technology development. The Costa Rican Social Security Fund (CCSS) is the entity that provides health insurance for the entire population of the country, through a first, second, and third levels of care [26].
Data sources
The primary source of information is the Weight and Size Census 2016 [27]. This initiative captured anthropometric data of 347,379 children between 6 and 12 years old attending to the Costa Rican private and public scholar system in that specific period, disaggregated by administrative geographical units; provinces, cantons and districts. The districts were chosen as unit of analysis in order to increase the granularity and the representation of the socioeconomic heterogeneity at this level of aggregation [28]. Metrics from the 2011 Census [29], were associated to each spatial unit. As a result of this process, 472 territories were considered. Their basic characteristics in terms of area and general and interest population were summarized in Table 1.
Study variables
Overweight and obesity prevalence are the variables of interest in this study. They are defined as the percentage of children which body mass index (BMI), place them between 1 and 2 standard deviations above median (overweight) or more than 2 standard deviations above median (obesity) according to the WHO grow reference data [30]. Figure 1 presents spatial patterns of each of these conditions. The Empirical Bayes Index (EBI) [31], a modification of Moran’s I, was used to assess their spatial autocorrelation. The resulting values are 0.354 and 0.482 for overweight and obesity respectively, in both cases statistically considerable (p-value < 0.001).

Geographical patterns of overweight and obesity prevalence in Costa Rica. a Overweight prevalence. b Obesity prevalence. Grey polygons represent districts without data
The socioeconomic covariates that according to the literature could affect the prevalence values and were completed and available at district level are:
-
Unemployment rate (Unemployment): in general, parental unemployment appears to be associated with the promotion of unhealthy dietary and activity behaviors, nevertheless, these associations depend on the studied country and whether unemployment comes from the mother or the father [32].
-
Percentage of urban population (Urban Population): children living in urban areas are more likely to be overweight or obese than those in rural areas [33]. Urbanization is one of the most important drivers of change in dietary patterns and physical activity; the shortening of daily routes and the lack of open spaces for outdoor recreation tend to induce a sedentary lifestyle in children. [34].
-
Percentage of homes with at least one critical deprivation (Deprivation): responds to the unsatisfied basic needs methodology proposed by the Economic Commission for Latin America (CEPAL). It establishes four critical aspects: access to dignified shelter, healthy life, knowledge and other goods and services [35]. The lack of one of the features is a poverty proxy. In developing countries, economic improvement is related to higher obesity levels in children [36, 37].
-
Percentage of population under 14 years old (Population<14): Although the explicit link between this metric and childhood obesity was not found in the literature, there is evidence that greater presence of peers increase the physical activity in children and adolescents [38], a key factor in obesity reduction [39].
-
Percentage of homes supported by a single mother (Single Mother Homes): single-parent households are positively related to higher levels of obesity and obesogenic behaviors in children [40]. In the case of single mothers, studies suggest that this can be attributed to non-sufficient income to provide high nutritional value food or access to organized physical activities, besides restricted parental time availability to monitor their diet and exercise habits [41]. It is important to note that most of the research in this area is limited to high income countries.
-
Average number of occupants per home (Occupants): applying the quantity-quality trade-off theory, a nutrition quality decline will be expected as a consequence of a family size increase [42], however, larger families can also improve their nutrition due to the tendency to prepare home meal to take advantage of economies of scale [43]. Empirical results are also ambiguous and the studies so far are again limited to developed countries.
-
Average years of schooling (Schooling): divergent behaviors describing the connection between obesity and educational attainment suggest the possibility of a non-linear relationship [44].
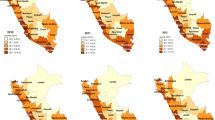
The spatial distribution of the values for each of the covariates is in Fig. 2 and their association with the incidence of obesity and overweight is shown in Fig. 3. Most of the associations are clearly linear but not necessarily considerable (e.g., Urban Population). It is important to note the concavity in the association between Schooling and obesity, supporting a possible existence of a non-linear relationship.

Geographical patterns of socioeconomic covariates

Association between covariates and prevalence of obesity and overweight
Spatial model
For the ith district, let us consider the counts of children with overweight (\(y_{i1}\)), obesity (\(y_{i2}\)) and without any of these conditions (\(y_{i3}\)), as realizations of a vector of random variables \(\mathbf {Y_{i}} = \{Y_{i1},Y_{i2},Y_{i3}\}\) with assigned probabilities \(\mathbf {p_{i}}=\{p_{i1},p_{i2},p_{i3}\}\), under the restriction \(\sum _{k=1}^{3} p_{ik} = 1\). If \(M_{i}=\sum _{k=1}^{3} Y_{ik}\) then
The above model can be treated as a set of independent binomial logistic models where one of the categories acts as reference or baseline [45]. In this particular case, the baseline corresponds to the category of children without the conditions, resulting in:
where \(\alpha _{k}\) is the intercept, \(\varvec{\beta _k}\) is a vector of fixed-effects and \(\textbf{x}\) is the vector of the covariate values. Notice that due to the restriction \(\sum _{k=1}^{3} p_{ik} = 1\), the probability for each condition and district can be expressed as a softmax function [46]:
A random effect \(b_{i}\) can be incorporated in the model, adding a new element to each linear predictor to take into account additional variation or spatial correlation due to not contemplated factors:
Using a BYM2 model [47, 48], the random effects corresponding to the m districts \(\textbf{b} = \{b_{1},\dots ,b_{m}\}\) is defined as:
Here, \(\textbf{v} \sim \mathcal {N}(0,I)\) is an unstructured random effect, where I is the identity matrix of size m, and \(\mathbf {u_{*}} \sim \mathcal {N}(0,Q_{*}^{-})\) is a scaled spatially structured component where \(Q_{*}^{-}\) is the general inverse of the standardized version of the precision \(m \times m\) matrix Q. Entries \(Q_{ij}\) of the matrix Q are equal to the number of neighbors of district i if \(i = j\), to \(-1\) if i and j districts are neighbors, and 0 otherwise.
Finally, the term \(\phi \in [0,1]\) is the proportion of the marginal variance explained by the latter effect and \(\tau\) is the overall precision. These hyperparameters have Penalized Complexity (PC) priors [47], where \(P(1/\sqrt{\tau } > U) = \alpha\) and \(P(\phi < U) = \alpha\). In the case of \(\tau\) the values for U and \(\alpha\) were set to 0.5/0.31 and 0.01 respectively, while \(U = 0.5\) and \(\alpha = 2/3\) were used in the case of \(\phi\), according to Simpson et al’s recommendation [47]. The fixed effects follows a normal distribution with mean 0 and precision 0.001.
All the available covariates were included as linear terms except for Schooling, that includes an additional quadratic term due to the behavior shown in Fig. 3. The estimation process was completed using Integrated Nested Laplace Approximation (INLA) through the R programming language [49] and the INLA package [50].
Results
We considered several model alternatives (Table 2) based on an exploratory analysis where we examined variable descriptive statistics (Table 3), including their correlations (and potential multicollinearity issues), and their statistical and theoretical relevance. WAIC [51] and CPO [52] criteria were used for model selection, and since they provided similar values across models, the most parsimonious one was chosen. The final model includes
Deprivation, Population<14, Schooling and Schooling2 as predictors.
Table 4 contains estimates of these fixed effects. These estimates can be interpreted in terms of the change in the odds of overweight (or odds of obesity) relative to non-overweight and non-obese children. The third and fourth columns for each category present the 95% credible interval of the corresponding odds ratio.
For both conditions, the credible intervals for Schooling and \(Schooling^2\) confirm the hypothesized non-linear nature of the variable. Prevalences are positively related to the average of completed years of education until a certain point (approximately 8 years), then the relationship shifts.
In the case of Deprivation and Population<14, these variables are statistically relevant just for obesity, and suggest that districts with less affluent and younger population are associated with lower odds of reaching this state. Particularly, there is a decrease of 7.7% (\([0.992^{10}- 1] \times 100\)) in the relative odds of obesity when there is a 10% increase in Deprivation. Moreover, there is a decrease of 14% (\([0.985^{10} - 1] \times 100\)) in the relative odds of obesity when there is a 10% increase in Population<14.
In Table 5 we included posterior estimates statistics of the hyperparameters in equation (5), where we can observe that, for both conditions, the posterior behavior of \(\tau\) produces a non-trivial random effect and \(\phi\) supports the existence of a structured spatial component.
Figure 4 shows the posterior distributions mean values at each district per category. For overweight, higher values are concentrated in the center area of the country and in the border crossing areas to Panama. Obesity shows a more uniform pattern, but there is an evident contrast between the center of the country and the southeast districts that are not connected to commercial borders. A clearer picture can be seen in Fig. 5 which presents the exceedance probabilities, this means the probabilities of surpassing a given threshold, in this case, the current national values for overweight (20%) and obesity (14%), both established as baselines in the public health strategies directed to the study population [21]. The map in Fig. 5 (a) displays the probability that the overweight prevalence reaches 20% or higher in each district. Analogously, Fig. 5 (b) shows the probability of achieving a 14% or greater obesity prevalence. Besides the patterns already explained, districts with higher probabilities appear in the extreme of the upper peninsula (Península de Nicoya) in both maps, and in the Central Pacific coast in the case of obesity. These areas are connected by maritime transportation, creating a touristic and commercial route that changes the socioeconomic environment and consequently may affect the nutritional behavior of the residents. A similar explanation can be applied to the districts over the lower peninsula which have higher values relative to their surroundings. They receive the maritime traffic and are strategic stopover points before reaching the Panama border. Another detail to notice is that all administrative districts in the peripheral provinces present higher probability values. Again, this can be a consequence of the distinct characteristics of this localities, which concentrate governmental, health and recreational services.

Geographical patterns of the estimated posterior mean prevalence values in Costa Rica. a Overweight estimated prevalence. b Obesity estimated prevalence

Geographical patterns of exceedance probabilities in Costa Rica. a Probability that overweight prevalence exceeds 20%. b Probability that obesity prevalence exceeds 14%
Dashboard
As an additional contribution to the Costa Rican health authorities, we developed a Shiny [53] dashboard showing the data and results obtained in this study. The dashboard contains maps and tables with the completed district database and their posterior distributions, which allows the user to calculate customized credible intervals and exceedance probability scenarios for overweight, obesity and combined prevalence, which consider the children with either of the conditions. The dashboard can be accessed at https://manjagoc.shinyapps.io/chovobcrdsh/.
Discussion
With the progression in the prevalence of childhood overweight and obesity, public health authorities around the world are increasingly searching for innovated and locally adapted tools to better understand and address the diverse and complex factors leading to these conditions, including those social determinants that exceed the control of the children, their families, or their communities.
In this article, with the use of a Bayesian spatial mixed model, we analyzed geographic patterns of childhood overweight and obesity in Costa Rica and their links with some socioeconomic indicators. Given that multiple variables have been associated as risk factors of this increasing worldwide epidemic [54], our analysis allowed us to identify some of the ones that considerably affected the outcome of our model, as possible key drivers for childhood overweight and obesity in the country.
As it was suggested, the district average years of schooling proved to have a non-linear relationship with an increased weight status prevalence, especially with obesity. Results showed that a higher education, usually associated with an increased socioeconomic status, is initially related with augmented BMI in children, however, as educational levels become higher this relationship reverses and the prevalence starts to drop. These phenomenon have been identified in other studies, where education acts a “social vaccine” against obesogenic environments [55, 56] promoting a change in individual actions and healthier choices [57, 58]. At macro scale, with income as mediator, the same behavior has been detected in the relationship between economic development and obesity, defining what is known as the “Obesity Kuznest Curve” [59, 60].
In the case of the percentage of homes with at least one critical deprivation variable, the association was negative, implying that in districts with a wealthier population the odds of obesity in children increase, as observed in other studies from developing countries, where children born in a higher socioeconomic status have a higher risk of being overweight or obese, the opposite being observed in developed countries [61].
These results demonstrate the complex relationship between education, economic status and BMI in children, and highlights the importance of including public health interventions that target the promotion of healthy habits in parents at the forefront for the prevention of obesity, as their eating behavior, attitudes and perceptions are determinant in shaping the weight status of their children [62, 63].
The other variable that was statistically relevant for obesity was the percentage of population under 14 years old. The results suggests that districts with a higher proportion of older residents are associated with an increased likelihood of childhood obesity. This finding is consistent with previous research indicating that spending more time with friends may play an important role in reducing the risk of childhood overweight/obesity, as they promote more active lifestyles [64]. This aspect becomes more important as over the past several decades, virtually all regions in the world have experienced fertility decline [65]. In Costa Rica, it is projected that by 2025 the main population concentration will be located in ages between 25 to 44 years, with an increase of those 65 years and more [66]. Therefore, primary prevention methods should also be aimed at educating the child and encouraging appropriate diet and exercise from a young age through adulthood as well as promoting the availability of safe places for children to encourage daily physical activity.
As for the geographical aspects, the study showed that there are high probabilities of exceeding current national values of overweight and obesity in districts in the central area of the country and border areas in the southeast region, besides other locations characterized by its intense commercial or touristic activity.
Childhood overweight and obesity are due to multiple causes: genetic factors, hormonal derangements, environmental influences, and lifestyle, converging in this public health problem that affects society as a whole. Therefore, developing effective strategies and interventions to address the issue at hand requires a collective effort and the cooperation of all stakeholders. Academia can play a crucial role in this effort by providing valuable insights to guide the use of available resources. This article is one such effort to contribute to this field, although further research is still needed.
Limitations and strengths
As a cross-sectional ecological study, our results are restricted to the understanding of the associations between certain socioeconomic characteristics of a population and its overweight or obesity prevalence. Therefore, they are not intended to serve as evidence for individual level or causal inferences [67, 68], nor to explain the complete etiology of this states. Besides, potential sex differences and relationships between the model predictors were not considered. Both constitute new research opportunities along with the inclusion of the temporal dimension when new data become available.
At the best of our knowledge, this is the first application of a spatial multinomial Bayesian model to explore the associations between socioeconomic factors and childhood nutritional states considering overweight and obesity as separate conditions. It is also the first study that analyzes the spatial aspect of these conditions in Costa Rica at national level. Another interesting feature is the use of the BYM2 model and the calculation of the prevalence exceedance probabilities with respect to Costa Rican health policy goals and the design of a Shiny app to support other researchers and authorities.
Conclusions
The study found a non-linear relationship (U-inverted) between the average years of schooling per district and the prevalence of overweight and obesity. In addition, a negative association was found between the prevalence of obesity and the percentage of households with at least one critical deprivation and with the percentage of population under 14 years of age. The spatial patterns indicate that districts in the central area and southeast borders of Costa Rica, as well as other districts with high levels of touristic and commercial activity or administrative importance, have higher prevalence values and a greater probability of exceeding national obesity and overweight targets.
Availability of data and materials
The data that support the findings of this study are available from the Health Ministry of Costa Rica but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the corresponding author upon reasonable request and with permission of the Health Ministry of Costa Rica.
References
World Health Organization. Obesity and overweight. 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 13 Sept 2021.
World Health Organization. Taking action on childhod obesity. 2018. https://apps.who.int/iris/bitstream/handle/10665/274792/WHO-NMH-PND-ECHO-18.1-eng.pdf. Accessed 13 Sept 2021.
Blanco D, Fernández X, Zúñiga M, Masis G, Barrantes A. Efectividad del modelo Póngale vida para la prevención de la obesidad infantil en escolares del cantón de La Unión, Costa Rica. Población Salud Mesoam. 2020;18(1). https://doi.org/10.15517/psm.v18i1.40816.
Ministerio de Salud. Plan para el abordaje integral del sobrepeso y obesidad en la niñez y adolescencia. / Secretaría de la Política Nacional de Alimentación y Nutrición. 2017. https://www.ministeriodesalud.go.cr/index.php/biblioteca-de-archivos-left/documentos-ministerio-de-salud/ministerio-de-salud/planes-y-politicas-institucionales/planes-institucionales/5071-plan-para-el-abordaje-integral-del-sobrepeso-y-la-obesidad-en-la-ninez-y-la-adolescencia/file. Accessed 10 May 2022.
Campbell MK. Biological, environmental, and social influences on childhood obesity. Pediatr Res. 2016;79(1):205–11.
Lobstein T, Baur L, Uauy R. Obesity in children and young people: a crisis in public health. Obes Rev. 2004;5(s1). https://doi.org/10.1111/j.1467-789X.2004.00133.x.
Lam TM, Vaartjes I, Grobbee DE, Karssenberg D, Lakerveld J. Associations between the built environment and obesity: an umbrella review. Int J Health Geogr. 2021;20(1):1–24.
Kim Y, Cubbin C, Oh S. A systematic review of neighbourhood economic context on child obesity and obesity-related behaviours. Obes Rev. 2019;20(3):420–31.
Swinburn B, Egger G, Raza F. Dissecting obesogenic environments: the development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev Med. 1999;29(6):563–70.
Oshan TM, Smith JP, Fotheringham AS. Targeting the spatial context of obesity determinants via multiscale geographically weighted regression. Int J Health Geogr. 2020;19(1):1–17.
Schabenberger O, Gotway CA. Statistical Methods for Spatial Data Analysis. Florida: Chapman & Hall/CRC; 2005.
Chi G, Zhu J. Spatial regression models for demographic analysis. Popul Res Policy Rev. 2008;27(1):17–42.
Moraga P. Geospatial Health Data. Florida: CRC Press; 2020.
Jia P, Cheng X, Xue H, Wang Y. Applications of geographic information systems (GIS) data and methods in obesity-related research. Obes Rev. 2017;18(4):400–11.
Sun Y, Hu X, Huang Y, On Chan T. Spatial Patterns of Childhood Obesity Prevalence in Relation to Socioeconomic Factors across England. ISPRS Int J Geo-Inf. 2020;9(10):599.
Chalkias C, Papadopoulos AG, Kalogeropoulos K, Tambalis K, Psarra G, Sidossis L. Geographical heterogeneity of the relationship between childhood obesity and socio-environmental status: Empirical evidence from Athens. Greece Appl Geogr. 2013;37:34–43.
Grow HMG, Cook AJ, Arterburn DE, Saelens BE, Drewnowski A, Lozano P. Child obesity associated with social disadvantage of children’s neighborhoods. Soc Sci Med. 2010;71(3):584–91.
Sritart H, Taertulakarn S, Miyazaki H. Disparities in Childhood Obesity Prevalence and Spatial Clustering Related to Socioeconomic Factors in Isaan, Thailand. Int J Environ Res Public Health. 2022;20(1):626.
Di Cesare M, Bhatti Z, Soofi SB, Fortunato L, Ezzati M, Bhutta ZA. Geographical and socioeconomic inequalities in women and children’s nutritional status in Pakistan in 2011: an analysis of data from a nationally representative survey. Lancet Glob Health. 2015;3(4):e229–39.
Ngwira A. Climate and location as determinants of childhood stunting, wasting, and overweight: an application of semiparametric multivariate probit model. Nutrition. 2020;70:100010.
Ministerio de Salud. Estrategia Nacional de Abordaje Integral de las Enfermedades No Transmisibles y Obesidad 2022-2030. https://www.ministeriodesalud.go.cr/index.php/biblioteca-de-archivos-left/documentos-ministerio-de-salud/material-informativo/material-publicado/estrategias-en-salud/5699-estrategia-nacional-de-abordaje-integralde-las-enfermedades-no-transmisiblesy-obesidad-2022-2030/file. Accessed 29 Sept 2022.
Gamboa-Gamboa T, Fantin R, Cordoba J, Caravaca I, Gómez-Duarte I. Relationship between childhood obesity and socio-economic status among primary school children in Costa Rica. Publ Health Nutr. 2021;24(12):3825–33.
INEC. Clasificación de distritos según grado de urbanización. https://www.inec.cr/sites/default/files/documetos-biblioteca-virtual/imgmetodologia-indiceurbru.pdf. Accessed 25 May 2022.
World Bank. The World Bank in Costa Rica. https://www.worldbank.org/en/country/costarica/overview#1. Accessed 11 Mar 2022.
Organisation for Economic Co-operation and Development. OECD Economic Surveys: Costa Rica 2020. Paris: OECD Publishing; 2020.
Organisation for Economic Co-operation and Development. OECD Reviews of Health Systems: Costa Rica 2017 | READ online. https://read.oecd-ilibrary.org/social-issues-migration-health/oecd-reviews-of-health-systems-costa-rica-2017_9789264281653-en#page1. Accessed 25 May 2022.
Sistema de Integración Centroamericana. Costa Rica-Primer Censo Escolar Peso/Talla, 2016. 2019. https://bd.sica.int/index.php/catalog/105. Accessed 14 Sept 2021.
Mideplan. Índice de desarrollo social 2017. 2018. https://documentos.mideplan.go.cr/share/s/BXb_ILLDRwqVI_zHV3NadQ. Accessed 21 Jan 2023.
Instituto Nacional de Estadístiva y Censos. Censo 2011. https://inec.cr/estadisticas-fuentes/censos/censo-2011. Accessed 24 Nov 2021.
World Health Organization. BMI-for-age (5-19 years). https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age. Accessed 17 Feb 2022.
Assuncao RM, Reis EA. A new proposal to adjust Moran’s I for population density. Stat Med. 1999;18(16):2147–62.
Iguacel I, Gasch-Gallén A, Ayala-Marín AM, De Miguel-Etayo P, Moreno LA. Social vulnerabilities as risk factor of childhood obesity development and their role in prevention programs. Int J Obes. 2021;45(1):1–11. https://doi.org/10.1038/s41366-020-00697-y.
The Lancet Diabetes & Endocrinology. Urbanisation, inequality, and non-communicable disease risk. Lancet Diabetes Endocrinol. 2017;5(5):313. https://doi.org/10.1016/S2213-8587(17)30116-X.
Pirgon Ö, Aslan N. The Role of Urbanization in Childhood Obesity. J Clin Res Pediatr Endocrinol. 2015;7(3):163–7. https://doi.org/10.4274/jcrpe.1984.
Méndez F, Trejos JD. Costa Rica: Un mapa de carencias críticas para el año 2000. In: Costa Rica a la luz del Censo del 2000. Costa Rica: Centro Centroamericano de Población de la Universidad de Costa Rica; 2004. p. 205–29.
Gupta N, Goel K, Shah P, Misra A. Childhood Obesity in Developing Countries: Epidemiology, Determinants, and Prevention. Endocr Rev. 2012;33(1):48–70. https://doi.org/10.1210/er.2010-0028.
Vazquez CE, Cubbin C. Socioeconomic Status and Childhood Obesity: a Review of Literature from the Past Decade to Inform Intervention Research. Curr Obes Rep. 2020;9(4):562–70. https://doi.org/10.1007/s13679-020-00400-2.
Salvy SJ, Bowker JC, Germeroth L, Barkley J. Influence of Peers and Friends on Overweight/Obese Youths’ Physical Activity. Exerc Sport Sci Rev. 2012;40(3):127-32. https://doi.org/10.1097/JES.0b013e31825af07b.
Hills AP, Andersen LB, Byrne NM. Physical activity and obesity in children. Br J Sports Med. 2011;45(11):866–70. https://doi.org/10.1136/bjsports-2011-090199.
Duriancik DM, Goff CR. Children of single-parent households are at a higher risk of obesity: A systematic review. J Child Health Care. 2019;23(3):358–69. https://doi.org/10.1177/1367493519852463. PMID: 31129999.
Noonan M, Turchi J. Childhood Obesity Differences in Single-Father and Single-Mother Families. Sociol Focus. 2019;52(3):216–30. https://doi.org/10.1080/00380237.2019.1624234.
Dasgupta K, Solomon KT. Family size effects on childhood obesity: Evidence on the quantity-quality trade-off using the NLSY. Econ Hum Biol. 2018;29:42–55. https://doi.org/10.1016/j.ehb.2018.01.004.
Datar A. The more the heavier? Family size and childhood obesity in the U.S. Soc Sci Med. 2017;180:143–51. https://doi.org/10.1016/j.socscimed.2017.03.035.
Cohen AK, Rai M, Rehkopf DH, Abrams B. Educational attainment and obesity: a systematic review. Obes Rev. 2013;14(12):989–1005.
Categorical Agresti A, Analysis Data. A Wiley-Interscience publication. New York: Wiley; 2002.
Goodfellow I, Bengio Y, Aaron C. Deep Learning. Cambridge: MIT Press; 2016.
Simpson D, Rue H, Riebler A, Martins TG, Sørbye SH. Penalising Model Component Complexity: A Principled, Practical Approach to Constructing Priors. Stat Sci. 2017;32(1):1–28. https://doi.org/10.1214/16-STS576.
Riebler A, Sørbye SH, Simpson D, Rue H. An intuitive Bayesian spatial model for disease mapping that accounts for scaling. Stat Methods Med Res. 2016;25(4):1145–65. https://doi.org/10.1177/0962280216660421. PMID: 27566770.
R Core Team. R: A Language and Environment for Statistical Computing. Vienna; 2019. https://www.R-project.org/.
Rue H, Martino S, Chopin N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J R Stat Soc Ser B (Stat Methodol). 2009;71(2). https://doi.org/10.1111/j.1467-9868.2008.00700.x.
Watanabe S. A Widely Applicable Bayesian Information Criterion. J Mach Learn Res. 2013;14(1):867–97.
Pettit L. The conditional predictive ordinate for the normal distribution. J R Stat Soc Ser B (Methodol). 1990;52(1):175–84.
Chang W, Cheng J, Allaire J, Sievert C, Schloerke B, Xie Y, et al. shiny: Web Application Framework for R. 2021. R package version 1.7.1. https://CRAN.R-project.org/package=shiny.
Wang Y. Potential mechanisms in childhood obesity: causes and prevention. Energy Balance Obes. 2017;10:69–78.
Liu Y, Ma Y, Jiang N, Song S, Fan Q, Wen D. Interaction between Parental Education and Household Wealth on Children’s Obesity Risk. Int J Environ Res Public Health. 2018;15(8). https://doi.org/10.3390/ijerph15081754.
Jeon H, Salinas D, Baker DP. Non-linear education gradient across the nutrition transition: mothers’ overweight and the population education transition. Public Health Nutr. 2015;18(17):3172–82.
Vogel C, Lewis D, Ntani G, Cummins S, Cooper C, Moon G, et al. The relationship between dietary quality and the local food environment differs according to level of educational attainment: A cross-sectional study. PLoS ONE. 2017;12(8):e0183700.
Aitsi-Selmi A, Bell R, Shipley MJ, Marmot MG. Education modifies the association of wealth with obesity in women in middle-income but not low-income countries: an interaction study using seven national datasets, 2005–2010. PLoS ONE. 2014;9(3):e90403.
Grecu AM, Rotthoff KW. Economic growth and obesity: Findings of an Obesity Kuznets curve. Appl Econ Lett. 2015;22(7):539–43.
Windarti N, Hlaing SW, Kakinaka M. Obesity Kuznets curve: international evidence. Public Health. 2019;169:26–35. https://doi.org/10.1016/j.puhe.2019.01.004.
Dinsa GD, Goryakin Y, Fumagalli E, Suhrcke M. Obesity and socioeconomic status in developing countries: a systematic review. Obes Rev. 2012;13(11):1067–79.
Savage JS, Fisher JO, Birch LL. Parental influence on eating behavior: conception to adolescence. J Law Med Ethics. 2007;35(1):22–34.
Tang D, Bu T, Dong X. Are parental dietary patterns associated with children’s overweight and obesity in China? BMC Pediatr. 2020;20(1):1–11.
Vandewater EA, Park SE, Hébert ET, Cummings HM. Time with friends and physical activity as mechanisms linking obesity and television viewing among youth. Int J Behav Nutr Phys Act. 2015;12(1):1–11.
World Health Organization. World Population Prospects 2019 Highlights. https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf. Accessed 21 Sept 2022.
Mideplan. Costa Rica: Prospectiva en cambio demográfico al 2045. https://archivo.cepal.org/pdfs/GuiaProspectiva/CostaRicaProspectiva2045.pdf. Accessed 21 Sept 2022.
Piantadosi S, Byar DP, Green SB. The ecological fallacy. Am J Epidemiol. 1988;127(5):893–904.
Garrett TA. Aggregated versus disaggregated data in regression analysis: implications for inference. Econ Lett. 2003;81(1):61–5.
Acknowledgements
Authors want to thank the disposition of the Health Ministry of Costa Rica for facilitating us the 2016 Weight and Size Census data which made possible this study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Study concept and design: MG, LB, PM; acquisition of data: LB, PV; analysis and interpretation of data: MG, LB, PM, PV; drafting of the manuscript: MG, LB, PM, PV; critical revision of the manuscript: MG, PV; statistical analysis: MG, LB, PM; study supervision: LB, PM. All authors read and approved the final version of the manuscript.
Authors’ information
Not applicable.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Census data and administrative permission to use it were provided by the Ministry of Health of Costa Rica. This data was anonymized before its use. The procedures related to the participants were conducted in accordance with the guidelines and regulations laid down in the Declaration of Helsinki and approved by the National Board of Health Research (CONIS) of Costa Rica. Written informed consent was obtained from parents or guardians of the participants in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gómez, M.J., Barboza, L.A., Vásquez, P. et al. Bayesian spatial modeling of childhood overweight and obesity prevalence in Costa Rica. BMC Public Health 23, 651 (2023). https://doi.org/10.1186/s12889-023-15486-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15486-1