
Abstract
Background
Previous studies have suggested that lifestyle factors are associated with mortality in different population. However, little is known about the impact of lifestyle factors on all-cause mortality in non-communicable disease (NCD) population.
Methods
This study included 10,111 NCD patients from the National Health Interview Survey. The potential high-risk lifestyle factors were defined as smoking, excessive drinking, abnormal body mass index, abnormal sleep duration, insufficient physical activity (PA), overlong sedentary behavior (SB), high dietary inflammatory index (DII) and low diet quality. Cox proportional hazard model was used to evaluate the impact of the lifestyle factors and the combination on all-cause mortality. The interaction effects and all combinations of lifestyle factors were also analyzed.
Results
During 49,972 person-years of follow-up, 1040 deaths (10.3%) were identified. Among eight potential high-risk lifestyle factors, smoking (HR = 1.25, 95% CI 1.09–1.43), insufficient PA (HR = 1.86, 95% CI 1.61–2.14), overlong SB (HR = 1.33, 95% CI 1.17–1.51) and high DII (HR = 1.24, 95% CI 1.07–1.44) were risk factors for all-cause mortality in the multivariable Cox proportional regression. The risk of all-cause mortality was increased linearly as the high-risk lifestyle score increased (P for trend < 0.01). The interaction analysis showed that lifestyle had stronger impact on all-cause mortality among patients with higher education and income level. The combinations of lifestyle factors involving insufficient PA and overlong SB had stronger associations with all-cause mortality than those with same number of factors.
Conclusion
Smoking, PA, SB, DII and their combination had significant impact on all-cause mortality of NCD patients. The synergistic effects of these factors were observed, suggesting some combinations of high-risk lifestyle factor may be more harmful than others.
Similar content being viewed by others

Background
Non-communicable diseases (NCDs), primarily including cardiovascular disease (CVD), diabetes, chronic respiratory disease (CRD) and cancers, are the leading causes of premature death worldwide, and responsible for more than one-half of global disease burden and 70% of global deaths [1, 2]. Unhealthy lifestyle behaviors, such as smoking, drinking, insufficient physical activity and poor dietary pattern, are important risk factors of NCDs [3, 4]. Previous studies have also proved the impact of lifestyle on mortality of different populations [5,6,7,8,9]. Hence, a comprehensive understanding of these modifiable lifestyle factors on all-cause mortality of NCD patients would be beneficial for the prevention of premature death due to these factors.
Smoking, drinking, body mass index (BMI), physical activity (PA), diet quality and their combinations were the key lifestyle factors in previous studies [6, 10,11,12]. Recent studies in Denmark, Spain and China reported that healthy lifestyle behaviors could lower the risk of mortality from all cause, CVD and cancer [6,7,8]. An earlier meta-analysis also showed that the combination of healthy lifestyle factors could lowered the all-cause mortality risk by 66% [13]. However, few studies have focused on the impact of lifestyle factors on all-cause mortality in NCD patients, which deserved further attention. Moreover, some emerging and modern lifestyle factors may also have some influence on mortality risk [9, 14, 15].
In the current study, using a nationally representative population of NCD patients in the United States, we aimed to assess the impact of eight lifestyle factors on all-cause mortality of NCD patients. To assess whether the impacts differed in specific patient groups, we investigated the interaction effects between lifestyle factors and other variables. The mutually combinations of selected high-risk lifestyle factors were also created to explore the prevalence of these combinations and risk of mortality.
Methods
Study population
This study included participants ≥ 18 years old from the National Health Interview Survey (NHIS) during 2007–2014, which was an ongoing national cross-sectional survey administered by the National Center for Health Statistics and the Centers for Disease Control and Prevention. The matched mortality information for these participants were derived from the National Death Index by 31 December 2015. Participants were also excluded because of pregnancy, without NCDs, or missing data on mortality information. Finally, a total of 10,111 NCD patients were included in this study (Fig. 1). The NCDs mainly included metabolic syndromes (MS), CVD, CRD and cancer in this study (Supplementary Methods).

Flow diagram of participants in the study
Assessment of lifestyle factors
Lifestyle factors included in the current study were BMI, smoking, drinking, sleep duration, PA, sedentary behavior (SB), inflammatory potential of diet measured by dietary inflammatory index (DII) and diet quality measured by healthy eating index (HEI) 2015 [16, 17]. Potential high-risk lifestyle factors were defined as smoking, excessive drinking (> 30 g/day for males and > 15 g/day for females), BMI < 18.5 or > 24.9 kg/m2, sleep duration < 7 or > 9 h/day, PA < 150 min/week, SB > 5 h/day, DII in the top 60%, and HEI-2015 in the bottom 60% [18,19,20]. For each factor, the patients received 1 point if he/she met these criterions, otherwise they received 0 point for the factor. After the multivariable Cox proportional regression for these factors, the independent high-risk lifestyle factors positively related to mortality were selected to create high-risk lifestyle scores. Details of PA, DII and HEI-2015 were provided in the Supplementary Method and Supplementary Table 1.
Covariates
Covariates were included in the multivariable models to reduce confounding: sex (male and female), age group (< 60 years old and 60 ~ years old), race/ethnicity (Mexican American, other Hispanic, non-Hispanic white, non-Hispanic black and other race), marital status (married/living with partner, and widowed/divorced/separated/never married), education level (middle school or less, high school or equivalent, and college or more), income level (low, middle and high), MS, CVD, CRD and cancer.
Statistical analysis
Baseline characteristics were presented as numbers and percentages for categorical variables and means and standard deviations for continuous variables, and compared using chi-square test or analysis of variance as appropriate. Before the primary analyses, the variables with missing values were imputed using random forest imputation approach, which was available in “missForest” R package [21]. Random forest imputation was a nonparametric algorithm that involved a series of multiple imputations until convergence.
Cox proportional hazard model was used to calculate hazards radio (HR) and corresponding 95% confidence intervals (CI) to evaluate the impact of 8 lifestyle factors on all-cause mortality. The Kaplan-Meier survival curves with log-rank tests were used to compare the survival among different high-risk lifestyle scores, which was calculated from the independent high-risk lifestyle factors in the Cox model. The attributable risks for different number of high-risk lifestyles were calculated according to previous study [22].
To explore the possibility of interaction effects, the interactions between high-risk lifestyle scores and other covariates were included in the multivariable Cox models, respectively. We also made stratified analyses by the covariates whose interaction effects were statistically significant. To compare specific patterns of high-risk lifestyles, 15 possible mutually exclusive combinations of 4 lifestyle factors were created. The prevalence and HR (95% CI) for each combination were presented.
Potential confounding factors were adjusted in all multivariable Cox models, including sex, age, race/ethnicity, marital status, education level, income level, MS, CVD, CRD and cancer. The multi-categorical variables were transformed into dummy variables in the models. Variable assignments were listed in Supplementary Table 2. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, North Carolina), and a P value < 0.05 was considered statistically significant.
Results
Descriptive statistics
During 49,972 person-years of follow-up, 1040 deaths (10.3%) were identified among 10,111 NCD patients, which was increased with number of potential high-risk lifestyle factors (Supplementary Table 3). Patient characteristics were shown in Table 1. The average age of the study population was 55.0 years, 48.7% of the patients were male, 56.4% were married or living with partner, 45.2% had a high household income, 46.8% had an education level of college, and 29.7% had two or more NCDs. Among the lifestyle factors, 79.1% had abnormal BMI, 51.5% were smokers, 12.1% consumed excessive alcohol, 45.0% had abnormal sleep duration, 52.8% had insufficient PA, 51.0% had overlong SB, 60% had pro-inflammatory diet, and 60% had low diet quality. As the number of potential high-risk lifestyle factors increased, the distributions of sex, race/ethnicity, marital status, income level, education level and NCD prevalence have changed. More specifically, the proportions of male and married/living with partner, income level and education level were decreased, and NCD prevalence was increased.
Lifestyle factors and all-cause mortality
When eight individual lifestyle factors were entered in the model with other covariates, five were independently associated with all-cause mortality (Table 2). Of them, the increase of BMI had significantly decreased HR for all-cause mortality. Smoking (HR = 1.25, 95% CI 1.09–1.43), insufficient PA (HR = 1.86, 95% CI 1.61–2.14), overlong SB (HR = 1.33, 95% CI 1.17–1.51) and high DII (HR = 1.24, 95% CI 1.07–1.44) were risk factors for all-cause mortality. However, drinking, sleep duration and HEI-2015 showed no association with all-cause mortality.
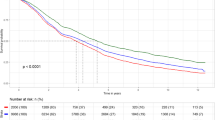
The risk of all-cause mortality was increased linearly as the high-risk lifestyle score increased, which was calculated from smoking, PA, SB and DII (P for trend < 0.01). Compared with patients without high-risk lifestyle, all-cause HRs for those with one, two, three, four high-risk lifestyle factors were 1.58, 2.14, 3.20 and 4.24, and the attributable risks were 2.43% 5.52% 11.59% and 17.69%, respectively (Table 3 and Supplementary Table 4). The cumulative mortality for patients with different high-risk lifestyle scores were statistically different (Fig. 2).

Cumulative probability of mortality for NCD patients with different number of high-risk lifestyle factors. The differences between any two survival curves were statistically significant (P < 0.05)
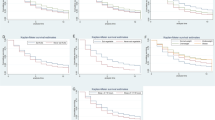
There were statistically significant heterogeneities regarding associations between high-risk lifestyle scores and all-cause mortality among some patient groups. The interactions between high-risk lifestyle scores, education level and income level were statistically significant (P < 0.01) (Supplementary Table 5). Stratified analysis suggested that high-risk lifestyle had stronger impact on all-cause mortality among patients with higher education level and higher income level (Supplementary Fig. 1). The association between high-risk lifestyle scores and all-cause mortality did not vary significantly by other patient groups.
Combinations of high-risk lifestyle factors
All 15 mutually exclusive combinations of four high-risk lifestyle factors were presented in Table 4. Of these, 93.5% patients had one or more high-risk lifestyle factors, while only 6.5% had no high-risk lifestyle factors. Out of four single high-risk lifestyle factors, insufficient PA (HR = 2.14, 95% CI 1.20–3.81) had the strongest association with all-cause mortality, followed by smoking (HR = 1.93, 95% CI 1.16–3.23). Among the patients with two and three high-risk lifestyle factors, Insufficient PA + overlong SB (HR = 2.99, 95% CI 1.79-5.00) and Insufficient PA + overlong SB + High DII (HR = 3.66, 95% CI 2.27–5.91) had the greatest impact on the increased all-cause mortality, respectively.
Discussion
In this study, we found that smoking, insufficient PA, overlong SB and high DII were independently associated with higher risk of all-cause mortality in NCD patients. The combined high-risk lifestyle scores, composite measures of these four factors, were significantly associated with increasing mortality as the number of high-risk factors increased. Stronger associations were observed among patients with higher education level and higher income level. The combinations involving insufficient PA and overlong SB had stronger associations with all-cause mortality than those with same number of factors.
Similar to some previous studies, this study found that smoking, insufficient PA and overlong SB were independently associated with higher all-cause mortality [6, 9]. Smoking was a well-established risk factor for some leading causes of death worldwide, such as CVD, lung cancer, lower respiratory infections and chronic obstructive pulmonary disease [23]. Insufficient PA was responsible for 9% of premature death of major NCDs [24]. The 2018 PA Guidelines for American recommended at least 75 min/week of vigorous-intensity PA or 150 min/week of moderate-intensity PA for substantial health benefit [25]. This study showed that even low-dose of PA can significantly reduce the all-cause mortality of NCD patients compared with physical inactivity. Besides displacing physical activity, SB and PA had independent effects on all-cause mortality, which meant that there were differences in the mechanisms of death caused by SB and PA.
Unhealthy diet was also a major risk factor for NCD globally, such as MS, CVD and certain types of cancer [26, 27]. The proportion of specific food elements (e.g., fruit, vegetable, milk) and some diet scores (e.g., HEI-2015, Mediterranean Diet) were applied in various studies to evaluate the diet pattern of lifestyle behaviors [8, 9, 19]. Compared with specific food elements, the comprehensive diet scores could better evaluate the effects of diet on health in its entirety. In previous studies on lifestyle, DII, which could characterize the inflammatory potential of diet, have not been included as a lifestyle factor. In the present study, DII (HR = 1.24, 95% CI 1.07–1.44) was a better index to evaluate the impact of diet on all-cause mortality than HEI-2015 (HR = 0.87, 95% CI 0.76-1.00).
Abnormal BMI and excessive drinking were not risk factors for all-cause mortality of NCD patients. The association of BMI with mortality was still controversial. A 2013 meta-analysis of 97 studies suggested that overweight might be protective factor for all-cause mortality [28]. U-shaped or J-shaped associations between BMI and all-cancer mortality have also been reported in previous studies [29, 30]. In this study, the increase of BMI was related with significantly lower all-cause mortality. The association between drinking and mortality risk also remained inconsistent. The cohort studies from Europe and the United States reported that excessive drinking was risk-factor for mortality, while moderate drinking is a protective factor [31, 32]. However, other studies showed that the risk of all-cause mortality rose with the level of drinking [33, 34]. Therefore, their effect on all-cause mortality still needed to be further verified by more sophisticated research.
Compared to most previous studies, we analyzed all the combinations of high-risk lifestyle factors, which showed that the same number of lifestyle factors contributed to mortality differently and that the combined effects may not be additive. The high-risk lifestyle factors tended to cluster, and 69.8% of patients had two or more high-risk lifestyle factors. Another interesting phenomenon was that the joint risk could be much higher than the sum of the individual risks. For example, although overlong SB on its own was not significantly associated with higher mortality risk, it augmented the risk noticeably when paired with insufficient PA and/or high DII (Table 4). This might indicate that overlong SB tended to be particularly harmful among those with insufficient PA and/or high DII. These findings suggested that there may be synergistic effects among lifestyle factors and that the epidemiological research and behavioral interventions should take into account the patterns of high-risk lifestyle and the interaction effects on all-cause mortality.
Our study has several limitations. First, most of the lifestyle factors were self-reported and thus some measurement errors were inevitable. However, the questionnaires for these factors have been validated and shown good reliability. Second, there were differences in the evaluation criteria of high-risk lifestyle factors, which might cause differences between studies. For example, the population of excessive drinking evaluated by drinking volume, frequency and pattern was likely to be different. Thresholds for sleep duration, SB, DII and HEI-2015 were also not defined. Third, the lifestyle information and covariates were collected at baseline. However, NCD patients were more likely to improve health status by changing high-risk lifestyle behaviors, which could not be considered in this study.
Conclusion
In conclusion, our findings suggested that smoking, PA, SB, DII and their combination had significant impact on all-cause mortality of NCD patients. The synergistic effects of these impacts were observed, especially for overlong SB. The education level and income level could impact the association between high-risk lifestyle score and all-cause mortality. Hence, these interaction effects should be considered in behavioral interventions for NCD patients.
Availability of data and materials
This data can be accessed using the following link: https://www.cdc.gov/nchs/nhanes/index.htm.
Abbreviations
- BMI:
-
body mass index
- CI:
-
confidence intervals
- CRD:
-
chronic respiratory disease
- CVD:
-
cardiovascular disease
- DII:
-
dietary inflammatory index
- HEI:
-
healthy eating index
- HR:
-
hazards radio
- MS:
-
metabolic syndromes
- NCDs:
-
non-communicable diseases
- NHIS:
-
National Health Interview Survey
- PA:
-
physical activity
- SB:
-
sedentary behavior
References
Organization WH. World health statistics 2016: monitoring health for the SDGs sustainable development goals. 2016.
Collaborators GCoD. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of Disease Study 2016. Lancet (London England). 2017;390(10100):1151–210.
Uddin R, Lee EY, Khan SR, Tremblay MS, Khan A. Clustering of lifestyle risk factors for non-communicable diseases in 304,779 adolescents from 89 countries: a global perspective. Prev Med. 2020;131:105955.
Benziger CP, Roth GA, Moran AE. The global burden of Disease Study and the preventable burden of NCD. Glob Heart. 2016;11(4):393–7.
Nechuta SJ, Shu XO, Li HL, Yang G, Xiang YB, Cai H, Chow WH, Ji B, Zhang X, Wen W et al. Combined impact of lifestyle-related factors on total and cause-specific mortality among Chinese women: prospective cohort study.PLoS Med2010, 7(9).
Ibsen DB, Sogaard K, Sorensen LH, Olsen A, Tjonneland A, Overvad K, Dahm CC. Modifiable lifestyle recommendations and mortality in Denmark: a Cohort Study. Am J Prev Med. 2021;60(6):792–801.
Wu MY, Wang JB, Zhu Y, Lu JM, Li D, Yu ZB, Shen P, Jiang DJ, Lin HB, Chen K. Impact of individual and combined lifestyle factors on mortality in China: a Cohort Study. Am J Prev Med. 2020;59(3):461–8.
Ruiz-Estigarribia L, Martinez-Gonzalez MA, Diaz-Gutierrez J, Gea A, Rico-Campa A, Bes-Rastrollo M. Lifestyle-related factors and total mortality in a Mediterranean prospective cohort. Am J Prev Med. 2020;59(2):e59–e67.
Ding D, Rogers K, van der Ploeg H, Stamatakis E, Bauman AE. Traditional and emerging lifestyle risk behaviors and all-cause mortality in Middle-Aged and older adults: evidence from a large Population-Based australian cohort. PLoS Med. 2015;12(12):e1001917.
Rizzuto D, Fratiglioni L. Lifestyle factors related to mortality and survival: a mini-review. Gerontology. 2014;60(4):327–35.
Bhaskaran K, dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3·6 million adults in the UK. The Lancet Diabetes & Endocrinology. 2018;6(12):944–53.
Zhao M, Veeranki SP, Magnussen CG, Xi B. Recommended physical activity and all cause and cause specific mortality in US adults: prospective cohort study. BMJ. 2020;370:m2031.
Loef M, Walach H. The combined effects of healthy lifestyle behaviors on all cause mortality: a systematic review and meta-analysis. Prev Med. 2012;55(3):163–70.
Li X, Chen B, Zhang J, Li M, Zhang Z, Zhu Y, Zeng XF, Li H, Wang Y, Wang SF et al. Association of dietary inflammatory potential with risk of overall and cause-specific mortality.Br J Nutr2021:1–10.
Patterson R, McNamara E, Tainio M, de Sá TH, Smith AD, Sharp SJ, Edwards P, Woodcock J, Brage S, Wijndaele K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. 2018;33(9):811–29.
Krebs-Smith SM, Pannucci TE, Subar AF, Kirkpatrick SI, Lerman JL, Tooze JA, Wilson MM, Reedy J. Update of the healthy eating index: HEI-2015. J Acad Nutr Diet. 2018;118(9):1591–602.
Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–96.
Zhu N, Yu C, Guo Y, Bian Z, Han Y, Yang L, Chen Y, Du H, Li H, Liu F, et al. Adherence to a healthy lifestyle and all-cause and cause-specific mortality in chinese adults: a 10-year prospective study of 0.5 million people. Int J Behav Nutr Phys Act. 2019;16(1):98.
Li Y, Pan A, Wang DD, Liu X, Dhana K, Franco OH, Kaptoge S, Di Angelantonio E, Stampfer M, Willett WC, et al. Impact of healthy lifestyle factors on life expectancies in the US Population. Circulation. 2018;138(4):345–55.
Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, Carty C, Chaput JP, Chastin S, Chou R, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–62.
Stekhoven DJ, Bühlmann P. MissForest–non-parametric missing value imputation for mixed-type data. Bioinf (Oxford England). 2012;28(1):112–8.
Cole P, MacMahon B. Attributable risk percent in case-control studies. Br J Prev social Med. 1971;25(4):242–4.
Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369(5):448–57.
Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–29.
Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, George SM, Olson RD. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–8.
Pan A, Lin X, Hemler E, Hu FB. Diet and Cardiovascular Disease: advances and Challenges in Population-Based Studies. Cell Metab. 2018;27(3):489–96.
Ley SH, Hamdy O, Mohan V, Hu FB. Prevention and management of type 2 diabetes: dietary components and nutritional strategies. Lancet. 2014;383(9933):1999–2007.
Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013;309(1):71–82.
Bhaskaran K, Dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018;6(12):944–53.
Global BMIMC, Di Angelantonio E, Bhupathiraju Sh N, Wormser D, Gao P, Kaptoge S, Berrington de Gonzalez A, Cairns BJ, Huxley R, Jackson Ch L, et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776–86.
Xi B, Veeranki SP, Zhao M, Ma C, Yan Y, Mi J. Relationship of Alcohol Consumption to All-Cause, Cardiovascular, and Cancer-Related mortality in U.S. adults. J Am Coll Cardiol. 2017;70(8):913–22.
Stockwell T, Zhao J, Panwar S, Roemer A, Naimi T, Chikritzhs T. Do “Moderate” drinkers have reduced mortality risk? A systematic review and Meta-analysis of Alcohol Consumption and all-cause mortality. J Stud Alcohol Drugs. 2016;77(2):185–98.
Britton A. Moderate alcohol consumption and total mortality risk: do not advocate drinking for ‘health benefits’. Nutr Metab Cardiovasc Dis. 2019;29(10):1009–10.
Alcohol use and burden. For 195 countries and territories, 1990–2016: a systematic analysis for the global burden of Disease Study 2016. Lancet. 2018;392(10152):1015–35.
Acknowledgements
Not applicable.
Funding
This study was supported by the National Natural Science Foundation of China (grant number: 72174049).
Author information
Authors and Affiliations
Contributions
Conception and study design by MJ and KY; data acquisition by YL and LW; data analysis and interpretation by YL, XF and KY; manuscript drafted by YL and MJ; critical revision of the manuscript by XF and MJ; all authors final approved the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All methods were performed in accordance with relevant guidelines and regulations (declaration of Helsinki). The protocol was approved by the Institutional Review Committee of National Center for Health Statistics. All the participants signed the informed consent forms.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Y., Fan, X., Wei, L. et al. The impact of high-risk lifestyle factors on all-cause mortality in the US non-communicable disease population. BMC Public Health 23, 422 (2023). https://doi.org/10.1186/s12889-023-15319-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15319-1