
Abstract
Background and aim
Exposure to lead can harm a child’s health, including damage to the nervous system, delayed growth, hearing loss, and many other adverse health effects, as well as implications for social, economic, educational and social well-being. Lead exposure in children is still a concern and cases require public health management to find the exposure source and interrupt the exposure pathway. Housing characteristics can indicate the presence of lead-contaminated paint and leaded water supply pipes. We aimed to explore the relationship between housing characteristics and elevated blood lead concentration (BLC) in children in England.
Methods
We used a retrospective cohort design and included all cases of lead exposure in children reported to the UK Health Security Agency between 2014 and 2020 via surveillance. A case was a child aged under 16 years, resident in England, BLC of ≥ 0.48 μmol/L (10 µg/dL) and referred for public health management. We collected case demographic details and housing characteristics (age and type). We explored associations between elevated BLC and risk factors, using generalised linear mixed effects models and compared cases’ housing type to that expected nationally.
Results
Two hundred and sixty-six out of 290 cases met the case definition. There was no difference in BLCs between genders, age groups, deprivation, and housing type. After adjusting for reporting source, housing age and type, cases residing in housing built pre-1976 had a BLC of 0.32 (95%CI 0.02, 0.63) µmols/L (6.63 (95%CI 0.42, 13.0) µg/dL) higher than cases living in housing built after this time. Cases were 1.68 times more likely to be living in terraced housing (housing adjoined to one another) than other children and less likely to live in apartments and detached properties.
Conclusion
This study suggests an association between housing characteristics and BLC in children. Housing age and type may act as a proxy for lead exposure risk through exposure to leaded paint, lead water pipes, and lead contaminated dust from indoor and outdoor sources. Public health action should consider targeting families more at risk in older housing by raising awareness of the potential presence of lead pipes and paint. Interventions should include working with wider stakeholders including other housing and environmental professionals, the private sector, as well as parents and carers.
Similar content being viewed by others


Background
It is estimated that 800 million children globally (around 1 in 3) have elevated blood lead concentrations (BLC), at or above 0.24µmols/L (micromoles per litre) (5 µg/dL) (micrograms per decilitre) [1]. Although more prominent in low- and middle-income countries, children in more developed countries are still exposed to lead in the environment. There is no recent comprehensive survey data estimating how many children in England are exposed to lead [2]. However, recent estimations by the Institute of Health Metrics [1], using the Global Burden of Disease tools suggest that for the United Kingdom (UK) there were 213,702 (95% Confidence Interval (CI) 186,117—281,542) children aged 0–19 years with a BLC of ≥ 0.24 µmol/L (≥ 5 µg/dL), and 29,036 (95% CI 25,099—42,470) children with BLC ≥ 0.48 µmol/L (≥ 10 µg/dl) in 2019. International population survey data may also be used for estimates; using the National Health and Nutrition Examination Survey (NHANES) undertaken in the USA between 2011 and 2016, the US Center for Disease Control and Prevention (USCDC) estimate that 2.5% of children aged 1–5 years have a BLC ≥ 3.5 µg/dL [3].
No safe level of lead exposure has been identified for children [4]. Timely removal or abatement of the exposure source or interruption of the exposure pathway is the mainstay of case management. Successful primary prevention efforts – targeted at reducing the use of lead in paints and fuels, regulation of lead concentrations in drinking water, planning controls and remediation of lead in soil, and control of industrial emissions – have been successful in reducing lead in the environment. However, lead is a persistent contaminant, lasting for many years; therefore, children can still be exposed to lead already in the environment [5]. Subsequent to the removal of lead from petrol, ingestion rather than inhalation is the most common route of exposure in high income countries, particularly from flakes and dust of leaded paint [6]. Other important routes of exposure in children are ingestion of lead-contaminated water, contaminated soil or dust, herbal medicine preparations, contaminated food, consumer products not meeting regulatory standards (e.g., paint on toys, make-up, ceramics, lead crystal glassware), or secondary exposure from parental hobbies or occupations (e.g., resulting in children being exposed to lead dust on work-clothing) [7].
Younger children and children with developmental disorders have been found to have higher BLCs [8]; whilst increased mouthing behaviour in early years is normal childhood behaviour, children with developmental disorder may also display this behaviour and hence are at higher risk of exposure due to increased mouthing (or “pica”) behaviour [9] (Fig. 1) leading to increased ingestion from lead in paint flakes, dust and soil, amongst other sources. Furthermore, iron deficiency may further increase susceptibility to lead toxicity [10,11,12].

Window sill with leaded paint picked off and eaten by a case. Children with pica are known to pick at and/or chew surfaces in the home painted with lead paint and this can be a source of lead exposure (photo courtesy of Rebecca Ingham, Advanced Health Protection Practitioner, Yorkshire and Humber Health Protection Team (HPT), UK Health Security Agency (UKHSA), 2021)
In the UK, in 1963 the UK Paintmakers Association voluntarily agreed to label paints containing more than 1% of lead and by 1980 lead-based paints were only available for specific purposes. Complying with European Standards in 1992, the sale of lead-containing paints to the public stopped except for special use, for example in the renovations of historic buildings [13,14,15]. However, older domestic housing may still have lead paint layers beneath newer paint, which become exposed if the surface is sanded down or chipped over time. Leaded water pipes may also be present in older houses. Although banned in plumbing for more than 25 years and subject to a program of replacement [16], lead pipes are still often found in homes, particularly in those built before 1970. Studies in the United States (US) have found that higher BLCs were associated with (amongst other factors) older housing age [17] and housing type [18], due to the presence of leaded paint and water pipes. Household leaded paint was the source of lead concentration in dust, which was correlated with age of housing (p = 0.036) [19]. Food and house dust have also been found to be key sources of lead contamination in the home [20], along with outdoor soil [21], household dust from kitchen floors and ingress of dust indoors from outdoor sources [22]. Given the expectation that older houses and houses with gardens are more likely to contain lead in various forms, it would seem reasonable to evaluate whether there is also an association between BLC and housing age and type in the UK.
In England, the UK Health Security Agency (UKHSA- previously Public Health England (PHE)) coordinates the Lead Exposure in Children Surveillance System (LEICSS) [2]. The surveillance was set up initially as a pilot after a research study demonstrated that direct laboratory reporting improved the timeliness of public health intervention in 80% of cases [23]. LEICSS has since captured details on some 300 children in England between 2014–2020 with elevated BLCs requiring public health intervention. The surveillance data provides an opportunity to explore the effect of housing on the level of blood lead in children.
The aim of the current study is to explore the relationship between elevated BLC in children reported to LEICSS and a range of routinely available housing-related risk factors (e.g., housing age and type).
Methods
Study design
We conducted a retrospective analysis in which we included all cases of lead exposure in children reported to UKHSA between 2014 and 2020.
Study population
The study population is comprised of children under the age of 16 years old resident in England.
Case definition
A case is defined as:
-
a child aged under 16 years at the time of first elevated BLC
-
resident in England
-
with an elevated BLC of ≥ 0.48 μmol/L (or ≥ 10 μg/dl) detected in a UK Accreditation Service (UKAS) biochemistry or toxicology laboratory, or reported to UKHSA for public health management at any BLC
-
reported to UKHSA by laboratories or clinicians during the period 01/01/2014 to 31/12/2020 inclusive.
For surveillance purposes during this time period participating labs reported cases with a BLC of ≥ 0.48 μmol/L (or ≥ 10 μg/dl) for public health case management in England. However, occasionally, cases with a BLC under this threshold were also reported, so we included all such cases requiring public health intervention irrespective of BLC. A separate sensitivity analysis (data not shown) found that excluding cases under the threshold did not affect the results.
Case data collection, extraction and handling
LEICSS is a passive surveillance system that integrates reports of incident (newly detected) cases of lead exposure in children from two sources; cases reported to UKHSA directly from a testing biochemistry/toxicology laboratory participating in surveillance, or by searching a case management system (HPZone, by Infact, Shipley) for cases first reported from a non-UKHSA source (e.g., the managing clinician or an environmental health officer) to a local UKHSA Health Protection Team (HPT). For further details of laboratories reporting to LEICSS see [2].
At each year’s end, data are extracted from HPZone and cases meeting the case definition on age and residence location are retained. Data on demographics, date of report (‘date entered’), date of onset/specimen date, source of reporting, current location, diagnostic notes, lab results, and status are extracted. Data were manipulated in Stata v14.2, MS Excel and mapped using ArcGIS ArcMap v10.5.1. Duplicate records were checked through NHS number, case name, date of birth, and address. Where duplicate records were found, we took the first BLC report and populated missing fields to make a more complete record.
Demographic data
Population demographics were derived from the Office of National Statistics (ONS) 2017 mid-year estimates for UKHSA Centre (UKHSAC) region areas [24], based on the midpoint of the time period of interest (2014–2020). Case postcodes were allocated geographical attributes by mapping location of cases in the Geographical Information System (GIS). The index of multiple deprivation (IMD) 2019 score [25] was obtained for each case through postcode matching to small area administrative Lower Super Output Area (LSOA). IMD is the official measure of relative deprivation for small areas or neighbourhoods (LSOAs, with 1,000–3,000 residents) in England and ranks every area from 1 (most deprived) to 32,844 (least deprived). It combines information from seven domain indices (income, employment, education, health, crime, access to housing and services, and living environment) to produce an overall relative measure of deprivation, with a quintile score from the first quintile representing the most deprived (group 1) to the fifth quintile representing the least deprived (group 5) areas.
Geographical variation
We considered that cases reported to the same region, HPT, or laboratory were more likely to be related, as the system by which they were detected and measured (clinical knowledge and referrals and laboratory testing regimes) would be similar. We used the variable HPT to represent such regional homogeneity. There are 17 HPTs in England, and this variable was thought to explain the regional similarities with sufficient geographical variation. A UKHSA Centre (UKHSAC) would be too large an area and local authority area too small. We also included reporting categorisation; Super Assay Service (SAS) laboratory (lab) (those belonging to a network of trace element biochemistry NHS labs), non-SAS lab, or cases reported directly to HPTs in case source of report influenced the level of BLC recorded.
Housing characteristics datasets
The age and type of housing for each case was used as an indicator for the potential presence of lead-containing paints and lead water pipes in the home and were obtained from two sources. Housing age was estimated from a dataset provided by the UK Valuation Office Agency (VOA) [26] for the LSOA of residence. This dataset provides the number of households built in each decade since the year 1900, which allows the percentage of housing built before 1973 to be calculated for each LSOA in England. Because lead-based paints were phased out voluntarily during the 1970’s [13], the year of 1973 was set as a break point for this dataset (being an available category cut off point): housing built before 1973 were considered likely to contain lead-based paint, while properties built from 1973 onwards were assumed to be without lead-based paint. The case was allocated the value of this percentage for their resident LSOA as a continuous variable. The percentage of homes built before 1973 was also calculated per Upper Tier Local Authority (UTLA) and plotted on a map.
A second source of data on housing characteristics was obtained from the UK Ordnance Survey (OS) [27]. This experimental dataset was compiled from different sources and gave each case’s address an estimated individual housing age and type based on a records match by Unique Property Reference Number (UPRN). Data were compiled from land use records in OS, from the OS Topography Layer, OS AddressBase Premium database, planning records, Ministry of Housing, Communities and Local Government Energy Performance Certificates [28] and Her Majesty’s Land Registry [29] Price Paid data. Housing age was given in categories of build era (10–30-year period), and then summarized as pre or post-1976, as an appropriate available cut off point in the categories of this dataset to represent older housing. Data on housing type included breakdown by self-contained flat, terraced, semi-detached and detached house, and house of multiple occupation (HMO) (OS Addressbase). To explore if BLC was associated with housing type, we compared the observed distribution of cases’ housing type to that expected for the population in England [30] and calculated observed/expected ratios.
Descriptive epidemiology
We characterised demographics (age, sex, and geographical location by UTLA, regional UKHSA Centre area and HPT, location (hospitalised), status (deceased, investigation open, closed, or pending), deprivation score, housing age – from both datasets (and if built before 1973 (VOA data) or 1976 (OS data)), housing type, source of report (lab or HPT, lab type (SAS lab or other), lab name), and BLC. Epidemiology of cases captured through surveillance are reported in detail elsewhere through annual surveillance reports [2], so are only described briefly in this paper.
Statistical analysis
We conducted an analysis of the characteristics potentially associated with elevated BLC for cases. A single variable analysis (SVA) was conducted to calculate the BLC coefficients (and 95% Confidence Intervals (CI)) for each of the explanatory variables, either per category for categorical values, or per unit increase if linear for continuous variables. We performed SVA using a linear mixed effects model with HPT as a random effect and tested significance at the 5% level with a Wald test.
Sometimes, observations were related to each other, so we explored clustering at the HPT/regional level. We were interested in seeing the fixed effect of risk factors on BLC with HPT as a random effect. A mixed effects model was used to model data characterised by a multilevel structure.
For the multivariable analysis (MVA), we explored the distribution of BLC using Tukey’s Ladder of Powers [31]. As BLC was not normally distributed, we explored potential transformations and the normality of the modelled residuals. No feasible transformation of the data was possible, so we took two approaches: 1) as observational environmental samples and human biomonitoring samples are often log-normal [32], we took the log (base e) of BLC, and 2) we used a generalised linear model (GLM) with a gamma distribution.
We considered all a-priori confounders in a multi-level mixed effects linear regression; age, gender, deprivation (IMD), region (UKHSAC), source of report, and designated housing type (OS) and housing age (VOA or OS data) as our explanatory variables. We used a backwards stepwise approach to identify a final model, keeping the explanatory variables of interest (housing age and type), eliminating variables with the most missing values first and identifying possible confounders. If a variable did not improve the model (p < 0.05 with a likelihood ratio test) it was removed, provided it was not a substantial confounder (> 20% change in effect estimates), therefore coefficients are not available for these predictors.
Finally, we chose the best model to present using Information Criteria (IC) by comparing and exploring the fit of the model against residuals. We plotted the residuals of each model against exploratory variables, e.g., housing age and type, (as those variables remained in the model and fitted value) for trend, bias and variance homogeneity. We used the quantile–quantile plot to look at the normality of the residuals (data not shown). We compared the fit of the model and chose the model with the lowest IC (AIC/BIC) fit criteria, to balance good fit with parsimony. AIC and BIC are both penalized-likelihood criteria and used for comparing non-nested models and choosing best predictor subsets in regression, suggesting best fit. As the models used different co-variates, we present the fit criteria as a supplementary table (Table S1). We compared the two models with and without fitting random effects. From the eight resulting models, we reported on the best fit model and the Coefficients and 95% CI for each explanatory variable adjusted for housing age and type.
Results
Descriptive epidemiology
We identified 290 records of lead exposure reported to UKHSA between 1/1/2014 to 31/12/2020. Of these, 268 (92%) records were under 16 years at specimen date and removing two duplicates left 266 cases meeting the case definition. Cases reported per year ranged from 31 to 50, with an average of 34 per year (Table 1). Most cases were male (177, 68%). Cases ranged from 0 to 14 years old, median age 3 years old, Inter Quartile Range (IQR) 0- 13 years. 57% of cases were aged between 1 and 5 years old, and 18% between 5–10 years old. Ethnicity data was poorly recorded (2.7% complete) so not analysed further. More detail on the epidemiology of cases is reported in surveillance annual reports [2].
There were 241 cases with BLC recorded (91%) and 25 (9%) cases without. The latter were more likely to be cases reported direct to HPTs from clinicians or other stakeholders. The BLC ranged from 0.24–17.59 µmols/L (4.97–364.2 µg/dL), median 0.71 µmols/L (14.7 µg/dL), IQR 0.29–3.66 µmols/L (6.0- 75.8 µg/dL). The data were not normally distributed (p < 0.001) and highly skewed to zero. Cases in hospital at the time of first elevated BLC had a BLC 1.78 (95%CI 1.17, 2.39) µmols/L (36.9 (95%CI 24.2, 49.5) µg/dL) (p < 0.001) higher than non-hospitalised cases.
BLC varied between years, being higher or lower compared to the base year (2014) (Table 1). Dataflows in the surveillance system took time to stabilise, from its set up and pilot phase, so the yearly variation is not thought to be of interest and was therefore not further analysed.
Cases were mapped by counts per Upper Tier Local Authority (UTLA) (Fig. 2). The majority of cases lived in the Yorkshire and Humber UKHSAC (31%) followed by London (21%). Case numbers were higher in areas of the country characterised by older housing (Fig. 2) although this may reflect population density and notification patterns. LEICSS participating labs reported 205 cases (77%), with SAS labs contributing the majority (72%) and 56 cases (21%) were reported to HPTs directly (Table 1).

Cases per Upper Tier Local Authority area and percentage of housing built before 1973 in England. Location of cases, counts per Upper Tier Local Authority (UTLA), UK Health Security Agency (UKHSA) Centre region areas, and percentage of housing built before 1973 per UTLA area (VOA data, 2014)
Cases were more likely to live in more deprived neighbourhoods, with half (49%) of cases living in the most deprived quintile (1); this is far higher than the 20% of households expected in this quintile. Cases were less likely to live in the top 2 least deprived quintiles (4 and 5); with 15% in these areas (expected 40%) (Table 1).
Property age and type
All cases were mapped to a VOA property age band (Fig. 3a). 79% of cases were living in a LSOA where the housing stock is predominantly (> 60%) built pre-1973 with almost half (48%) living in areas where 80–100% of dwellings are pre-1973 (Table 1). At UTLA level, the percentage of homes built before 1973 varied regionally, with urban areas showing older housing stock (London, the south-east, north-east, north-west and midlands, Fig. 2).

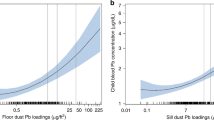
a, b, c Cases housing characteristics; a Distribution of housing age; percentage of houses built before 1973 for the cases local area. Values represent for each case, the % of housing built before 1973, for the small area (Lower Super Output Area (LSOA)) where the case resides. Data from the Valuation Office Agency (VOA) (2014). b Distribution of housing age for LEICSS cases (2014–2020) in England; using Ordnance Survey data. c Type of housing for cases of lead exposure in England (2014–2020) using Ordnance Survey data. HMO = House of Multiple Occupation
Using the OS dataset, 14% of cases were missing a housing age and 8% were missing housing type. Similarly to the VOA data, the majority of cases lived in older housing (pre 1966) with 78% living in houses built before 1976 (Fig. 3b, Table 1).
Compared to the national breakdown of housing types, a far higher proportion of cases live in terraced housing than the English housing stock proportion (47% v 28%) (Observed/Expected (O/E) ratio = 1.68) (Table 2). Terraced housing is typically units of double storey 2 or 3 bedroom houses joined directly to similar houses either side, often built in the Victorian era. Cases were less likely to live in flats (apartments), detached or semi-detached houses (attached to one other housing unit) (O/E < 1) (Fig. 3c, Table 1). Fewer cases lived in pre-1900 housing (15%) compared to the English national housing stock (21%), (O/E = 0.71).
Single variable analysis
In OS derived data, higher BLCs were associated with living in housing built pre-1976 compared to post-1976, and in children living in houses built between 1900–1929 compared to pre-1900 housing. There was no association found between housing age and BLC using VOA data. Lower BLC was associated with cases reported directly to HPTs, compared to those reported by labs. There was some evidence of regional differences in the levels of BLC in children. There was no difference in BLCs between the genders, between age groups, IMD quintiles, reporting labs, and housing type (Table 1).
Multivariable analysis
From the eight resulting models (Table S1), the model with best fit was the GLM fixed effects log distribution model. Table 3 shows the results of this model using log of BLC as the outcome variable and OS data as the housing age variable. The final model was adjusted for reporting source, housing age and type. Cases residing in housing built pre-1976 had a BLC 0.32 (95%CI 0.02, 0.63) µmols/L (6.63 (95%CI 0.42, 13.0) µg/dL) higher than cases living in housing built post-1976 (Table 3). Cases reported directly to HPTs had lower BLC than those reported by SAS labs (p = 0.003). There was no evidence for differences in BLC in children by housing type.
Discussion
The demographics of the cases are in line with previous descriptions of UK cases [2, 11, 12, 23, 33, 34]: more likely to be male (67%), aged between 1–5 years old (57%), and living in the most deprived quintile (49%) although BLC did not significantly vary between genders, age groups, and deprivation.
Our study supports previous research [35] showing relatively more older houses in northern and south-eastern areas of England, which suggests that regional BLC differences might be due to differences in lead exposure. However, it is difficult to draw firm conclusions given the known under-ascertainment of children with lead exposure [36] and known variation in case ascertainment [2]. For example, considerable awareness-raising activities in Yorkshire and Humber resulted from a serious case review following a death of a child from lead poisoning in 2015 [37] and led to a marked and sustained increase in reporting.
Cases were more likely to live in the most deprived areas; however, BLC did not show a dose–response relationship, potentially explained by the small sample size and the effect of other lead sources, e.g., diet. We would expect more deprived areas to have older sub-standard housing or more exposure to contamination sources as studies in the US (e.g. [17]) have found higher BLC associated with lower family income-to-poverty-ratio and lower socio-economic status.
Property age and type
The findings in this study broadly agree with research in other countries such as the US [17, 38,39,40], Canada [19], and France [41, 42] suggesting that housing age is a risk factor for exposure to lead in the domestic environment, likely due to exposure to old lead-painted surfaces or water supply pipes containing lead. Comparing housing age pre and post 1976 using the single variable analysis and OS data showed a significant association between BLC and housing age. However, OS 30-year age bands showed a less clear picture with only the 1900–1929 age band associated with higher BLC than pre-1900. This is unexpected since lead paint would have been in use during both these time periods. VOA housing age data is based on local area data (LSOA) but brownfield development and post-war infill leads to a mix of housing age, especially in urban areas, which may lead to misclassification and explain the lack of an association with BLC. In contrast, OS data assigns characteristics to individual properties using data derived from multiple sources and is likely to be more accurate, although incomplete data (14% for housing age) could have potentially introduced bias and misleading inference. Some significant associations at SVA disappeared in the multivariable model, potentially explained by residual confounding from other relevant exposures such as diet, soil, etc.
Whilst the modelled effect estimates for housing age were small, the coefficients associated with older housing (0.32 µmol/L; 6.6 µg/dL; 6.63 (95%CI 0.42, 13.0) µg/dL) are above the concentration (0.24 µmols/L; 5 µg/dL) at which public health intervention is now required in England [43] and in the US (0.16905 µmols/L;3.5 µg/dL) [44]. Whilst there is no threshold for adverse health effects, the World Health Organisation (WHO) advocate clinical intervention for any individual with a BLC above 5 µg/dL [36].
Although BLC was not found to be associated with a particular housing type in the model, the distribution of cases’ housing type compared to that expected showed that cases were nearly twice as likely to live in terrace housing (47%) compared to the national proportion (28%). The majority of terraced housing in the UK was built before the 1970s, so are likely to contain leaded water supply pipes and lead paint (even when renovated, as new paint is commonly painted over the original paint). The dangers of lead exposure through domestic redecoration have been highlighted in public information leaflets [45]. This type of housing is often populated with families with younger children, with relatively lower incomes.
One other study (in the US) has identified specific housing types as being more likely to present a risk of lead exposure. As well as age of housing, this study identified privately rented multiple unit houses in poor repair as being more likely to present a risk of lead exposure [18]. Similar to our study, the occupants of such housing were more likely to be low income.
Limitations
The low ascertainment of cases identified through LEICSS has been discussed elsewhere [2]. The LEICSS reporting rate is approximately 5 children per million [2]; this is 0.1% of the 257,200 children in England in 2021 aged under 15 years with a predicted blood lead > 2 µg/dL (and 20,000 predicted > 5 µg/dL) estimated using ONS population projections and prevalence data from international surveys and human bio-monitoring surveys (e.g. [1, 46, 47]. It has been suggested that passive reporting to surveillance systems is non-random and reported cases are more likely to be severe [48]. The absence of blood lead data below the case definition of elevated blood lead could bias the results. Low ascertainment may lead to bias in the case sample, although our case demographics and epidemiology are in line with other studies [49, 50].
Further exposures which may be associated with elevated BLC were not included in our analyses and may therefore give rise to residual confounding; for example, housing tenancy (owned or rented) [18, 51] parental occupation [52, 53], ethnicity [17], other sources of exposure, diet, contaminated land, soil quality or contaminated consumer products [6, 19, 20, 38, 41, 54]. Additionally, some case characteristics used ecological proxy measures based on area (e.g., deprivation, housing age and type) which may be inaccurate, leading to misclassification. For this study we did not take environmental measurements for individual cases, which could have confirmed local exposures, although this data may have been available in other databases via case investigations.
A limitation of using housing datasets is that housing characteristics were estimated from other datasets, again leading to potential misclassification. Reliability and completeness of variables also limited the findings. The association found with housing age may still suggest appropriate public health action to target families living in older housing but should be interpreted with caution.
We acknowledge that cases spend time in places other than the home, especially for school-aged children. A study in Sao Paulo, Brazil, found no associations with lead intake by diet (p = 0.4) or mean lead found in household environmental screenings (p = 0.15) but did find an association with day care centres environmental screenings (p < 0.001) [54], suggesting that settings other than the home are important for lead exposure and need to be considered for case investigation. Time spent in education and day care settings should also be considered for exposure to lead sources and is considered in UK public health risk assessments. A recent UK study found elevated lead levels in school water [55]. UKHSA’s case exposure questionnaire used in case investigations now captures information on time spent at other locations.
Finally, for this type of study, examining associations with BLC may be less important than data on whether a child is identified as exposed to lead (being a case or not). A comparison of the location of cases and non-cases could better identify common exposures. It is possible that a different study design (such as case control) may be more able to identify these associations, but that was not possible using the data available at this time.
Implications for public health management and interventions
The dominance of older housing (built before 1970) in England [30] suggests that the risk of lead exposure in children is likely to persist for some time. In the UK, the Housing Health and Safety rating system (HHSRA) [56] tool used by local authorities could potentially screen for the potential risk of lead exposure using a similar appropriate age of housing threshold (perhaps through Early Years intervention schemes, as has been instituted in other countries [57]) or take appropriate environmental samples to test for the presence of lead. A recent study in the US estimated 29.4% of homes contained lead based paint and that households receiving Government housing assistance had a lower prevalence of lead paint hazards [58] which suggests social housing is subject to lead checks. Awareness raising activities could consider information provision advising on the dangers of leaded paint, renovation practices [45] and replacing leaded water supply pipes, in particular among younger families living in older housing.
Implications for further study
More accurate data are required regarding housing age and type for cases, across a larger and therefore more representative sample. Standardised case investigation questionnaires could incorporate information on residence characteristics as well as other exposures outside the home, e.g. extended families, child-care, schools, and nurseries. Alternative housing characteristics might also be explored as potentially better proxies for lead risk. Examples of these characteristics include a combination of housing age and value (which takes into account renovation and repairs that reduce lead exposure risk).
The likely under ascertainment of cases of raised BLC in England using LEICSS [2] and potential for bias in the sample is based on prevalence data from other countries. A prevalence study in England would not only provide more accurate data on BLC in children in England but could also collect further exposure data and inform future screening recommendations [59]. The power of both health and housing population-wide surveys, which in the US consists of the National Health and Nutrition Examination Survey [3] and the American Healthy Housing Survey, is that these surveys report data below blood lead reference values and paint, dust and soil lead levels below government standards. The recent lowering of the case definition for lead surveillance in England will result in an increase in cases reported to LEICSS [43] resulting in a larger sample size and a broader range of BLC. It is recommended to repeat the analysis to include the new cases.
Conclusions
This study suggests housing characteristics can indicate an increased risk for elevated BLC in children. Higher BLC was associated with cases living in housing built before 1976. BLC did not differ with type of housing in our model, but cases were more likely to be living in terraced housing and less likely to live in flats (apartments) and detached properties than the national proportion. They were also more likely to reside in more deprived areas. There were significant yearly and regional differences in the levels of BLC in children. The small sample size may have limited stronger effects being found.
We recommend undertaking a more detailed investigation of cases to better characterise potential sources including those in the home environment. The findings of this study may indicate avenues for public health interventions, by targeting housing risk factors associated with elevated BLC and primary prevention measures.
Availability of data and materials
Data are incorporated into the article and material contained within. Individual level data cannot be shared due to ethical/privacy reasons.
Code availability: Custom code using Stata15.
Abbreviations
- BLC:
-
Blood Lead Concentration
- BRE:
-
Building Research Establishment
- CI:
-
95% Confidence Interval
- DEFRA:
-
Department for Environment, Food and Rural Affairs
- GIS:
-
Geographical Information System
- GLM:
-
Generalised linear model
- HMLR:
-
Her Majesty’s Land Registry
- HPT:
-
Health Protection Team
- HMO:
-
House of Multiple Occupation
- HHSRA:
-
Housing Health and Safety rating system
- IMD:
-
Index of Multiple Deprivation
- IC:
-
Information Criteria
- IQR:
-
Inter Quartile Range
- LEICSS:
-
Lead Exposure in Children Surveillance System
- LSOA:
-
Lower Super Output Area
- µmol/L:
-
Micromols per litre
- µg/dL:
-
Micrograms per decilitre
- MHCLG:
-
Ministry of Housing, Communities and Local Government
- MVA:
-
Multiple variable analysis
- NHANES:
-
National Health and Nutrition Examination Survey (US)
- ODPM:
-
Office of the Deputy Prime Minister
- O/E:
-
Observed/Expected ratio
- ONS:
-
Office for National Statistics
- OS:
-
Ordnance Survey
- PHE:
-
Public Health England
- SAS Lab:
-
Super Assay Service Laboratory
- SVA:
-
Single variable analysis
- UK:
-
United Kingdom
- UKAS:
-
United Kingdom Accreditation Service
- US:
-
United States
- USA:
-
United States of America
- US CDC:
-
United States Centre for Disease Control and Prevention
- USEPA:
-
United States Environmental Protection Agency
- UKHSA:
-
UK Health Security Agency
- UKHSAC:
-
UK Health Security Agency Centre
- UPRN:
-
Unique Property Reference Number
- UTLA:
-
Upper Tier Local Authority
- VOA:
-
Valuation Office Agency
- WHO:
-
World Health Organisation
References
UNICEF and Pure Earth. The Toxic Truth: Children’s Exposure to Lead Pollution Undermines a Generation of Future Potential. The-toxic-truth-children’s-exposure-to-lead-pollution-2020.pdf (unicef.org). 2020. https://www.unicef.org/media/73246/file/The-toxic-truth-children%E2%80%99s-exposure-to-lead-pollution-2020.pdf. Last accessed 18 May 2022.
UK Health Security Agency (UKHSA). Lead exposure in children surveillance system, annual report 2021, summary of 2020 data. 2021. Available at https://www.gov.uk/government/publications/lead-exposure-in-children-surveillance-reports-from-2021. Last accessed 18 May 2022.
Ruckart PZ, Jones RL, Courtney JG, et al. Update of the blood lead reference value — United States, 2021. MMWR Morb Mortal Wkly Rep. 2021;70:1509–12. https://doi.org/10.15585/mmwr.mm7043a4.
United States Centre for Disease Control and Prevention (USCDC). Prevent children’s exposure to lead. National Centre for Environmental Health. 2022a. https://www.cdc.gov/nceh/features/leadpoisoning/index.html. Last accessed 7/1/22.
USEPA (US Environmental Protection Agency). Basic information about lead air pollution. 2021. https://www.epa.gov/lead-air-pollution/basic-information-about-lead-air-pollution. Last accessed 5/11/21.
AAP- American Academy of Pediatrics. Lead exposure in children: prevention, detection, and management. Pediatrics. 2005;116(4):1036–46.
World Health Organization (WHO). Childhood lead poisoning. Geneva; 2010. https://www.who.int/publications/i/item/childhood-lead-poisoning. Last accessed 18 May 2022.
Lewendon G, Kinra S, Nelder R, Cronin T. Should children with developmental and behavioural problems be routinely screened for lead? Arch Dis Child. 2001;85(4):286.
US CDC Centers for Disease Control. Suggested priorities for screening (chapter 6). 1991. https://wonder.cdc.gov/wonder/prevguid/p0000029/p0000029.asp. Last accessed 18 May 2022.
Kwong WT, Friello P, Semba RD. Interactions between iron deficiency and lead poisoning: epidemiology and pathogenesis. Sci Total Environ. 2004;330(1):21–37.
Roberts DJ. Helen Crabbe, Tayo Owodunni, Harriet Gordon-Brown, Rebecca Close, Shanel Reshat, Barry Sampson, Ruth Ruggles, Gavin Dabrera, Araceli Busby, Giovanni Leonardi, Case epidemiology from the first three years of a pilot laboratory-based surveillance system for elevated blood-lead concentrations among children in England, 2014–17: implications for public health action. J Public Health. 2020;42(3):542–9. https://doi.org/10.1093/pubmed/fdz024.
Roberts DJ, Bradberry SM, Butcher F, Busby A. Lead exposure in children. BMJ. 2022;377:e063950. https://doi.org/10.1136/bmj-2020-063950.
Johnson L, Barlow PJ, Barratt RS. Lead in paint – Brushed aside? Perspect Public Health. 1984;104(2):64–7.
Millstone E. Lead and public health: the dangers for children. Earthscan; 1997. p. 222.
Zolfagharifard E. Has removing lead from paint and petrol reduced CRIME? Toxin is linked to surges in theft and violent assault. Article in Daily Mail; 2014. Available from https://www.dailymail.co.uk/sciencetech/article-2609623/Has-removing-lead-paint-petrol-reduced-CRIME-Toxin-linked-surges-theft-violent-assault.html. Last accessed 24/5/22.
UK Government. The Water Supply (Water Quality) Regulations 2016 (as amended) for England. UK Statutory Instruments, No 614, 2016. London: The Stationery Office; 2016. Accessed 11/01/2022 Available from: URL https://www.legislation.gov.uk/uksi/2016/614/contents/made. Last accessed 18 May 2022.
Egan KB, Cornwell CR, Courtney JG, Ettinger AS. Blood lead levels in U.S. children ages 1–11 years, 1976–2016. Environ Health Perspect. 2021;129(3). https://doi.org/10.1289/EHP7932. Published:17 March 2021CID: 037003.
Korfmacher KS, Kuholski K. Do the same houses poison many children? An investigation of lead poisoning in Rochester, New York, 1993–2004. Public Health Rep. 2007;122(4):482–7.
Safruk AM, McGregor E, Whitfield Aslund ML, Cheung PH, Pinsent C, Jackson BJ, Hair AT, Lee M, Sigal EA. The influence of lead content in drinking water, household dust, soil, and paint on blood lead levels of children in Flin Flon, Manitoba and Creighton. Saskatchewan Sci Total Environ. 2017;1(593–594):202–10. https://doi.org/10.1016/j.scitotenv.2017.03.141 Epub 2017 Mar 24 PMID: 28343040.
Ohtsu M, et al. Oral exposure to lead for Japanese children and pregnant women, estimated using duplicate food portions and house dust analyses. Environ Health Prev Med. 2019;24(1):72.
Hunt S, Johnson DL, Griffith DA. Mass transfer of soil indoors by track-in on footwear. Science of the Total Environment. V370. Iss. 2006;2–3:360–71.
Hunt A, Johnson DL, Griffith DA, Zitoon S. Citywide distribution of lead and other element in soils and indoor dusts in Syracuse, NY. Appl Geochem. 2012;27(5):985–94.
Public Health England. Surveillance of Elevated Blood Lead in Children (SLiC). A British Paediatric Surveillance Unit analysis. 2018. Available at https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/751982/SLiC_final_report_v3.pdf. Last accessed 18 May 2022.
Office of National Statistics [ONS, 2021] Estimates of the population for the UK, England and Wales, Scotland and Northern Ireland. https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland. Last accessed 26 Oct 2022.
National Statistics – English indices of deprivation 2019: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2019. Last accessed 12 Feb 2021.
VOA- Valuation Office Agency Housing Age dataset. 2014. https://data.london.gov.uk/dataset/property-build-period-lsoa. Last accessed 12 Feb 2021.
Ordnance Survey (OS). UK) AddressBase products Classification Scheme. Ordnance Survey GB. AddressBase Premium technical specifications v 2.5. 2021. Available from https://www.ordnancesurvey.co.uk/. Last accessed 18 May 2022.
Ministry of Housing, Communities and Local Government (MHCLG) 2021 Energy Performance Certificates, available at https://www.gov.uk/government/collections/energy-performance-of-buildings-certificates. Last accessed 18 May 2022.
Her Majesty’s Land Registry (HMLR) 2021 Price paid data; Available at https://landregistry.data.gov.uk/app/ppd/ (Last accessed 18th May 2022)
BRE (Building Research Establishment) Trust. The housing stock of the UK. 2020. Available from https://files.bregroup.com/bretrust/The-Housing-Stock-of-the-United-Kingdom_Report_BRE-Trust.pdf. Last accessed 18 May 2022.
Scott D. Tukey’s ladder of powers description. 2017. Available online: http://onlinestatbook.com/2/transformations/tukey.html. Accessed on 5 Nov 2021.
Samanta G, Sharma R, Roychowdhuryb T, Chakrabortic D. (2004) Arsenic and other elements in hair, nails, and skin-scales of arsenic victims in West Bengal. India Sci Total Environ. 2004;326:33–47.
Public Health Wales (PHW). ‘Lead- yesterdays public health problem?’ CIEH talk slide set. A Kibble, S Jones. 2021. Accessed at: https://www.cieh.org/media/1785/andrew-kibble-and-dr-sarah-jones.pdf. Last accessed 18 May 2022.
Public Health England (PHE). Lead exposure in children surveillance system. Surveillance reports: 2020. https://www.gov.uk/government/publications/lead-exposure-in-children-surveillance-reports. Last accessed 18 May 2022.
Wei W. An Investigation of Lead Poisoning in Children in England, with a Risk Map of Potential Lead Exposure and an Enhanced Questionnaire on Potential Sources. MSc thesis at Centre for Environmental Policy, Imperial College London. 2017. Unpublished.
World Health Organization (WHO). Guideline for clinical management of exposure to lead. 2021. https://www.who.int/publications/i/item/9789240037045. Last accessed 18 May 2022.
Talbot A, Lippiatt C, Tantry A. Lead in a case of encephalopathy. BMJ Case Rep. 2018;2018:bcr2017222388. https://doi.org/10.1136/bcr-2017-222388 PMID: 29523605; PMCID: PMC5847830.
Gaitens JM, et al. Exposure of U.S. children to residential dust lead, 1999–2004: I. Housing and demographic factors. Environ Health Perspect. 2009;117(3):461–7.
Reissman DB, et al. Use of geographic information system technology to aid health department decision making about childhood lead poisoning prevention activities. Environ Health Perspect. 2001;109(1):89–94.
Gasana J, et al. Blood lead levels in children and environmental lead contamination in Miami Inner City, Florida. Int J Environ Res Public Health. 2006;3(3):228–34.
Etchevers A, Bretin P, Lecoffre C, Bidondo ML, Le Strat Y, Glorennec P, et al. Blood lead levels and risk factors in young children in France, 2008–2009. Int J Hyg Environ Health. 2014;217(4–5):528–37.
Rollin L, et al. Follow-up of children suffering from lead poisoning or at risk of lead poisoning in Greater Paris, 1992–2002. Rev Epidemiol Sante Publique. 2008;56(6):391–7.
Public Health England (PHE). Evaluation of whether to lower the public health intervention concentration for lead exposure in children. PHE report. 2021. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/999149/Evaluation_of_whether_to_lower_the_public_health_intervention_concentration_for_lead_exposure_in_children.pdf. Last accessed 18 May 2022.
United States Centre for Disease Control and Prevention (US CDC, (2022b) CDC’s Blood Lead Reference Value. https://www.cdc.gov/nceh/lead/data/blood-lead-reference-value.htm (last accessed 4/2/22)
Department for Environment, Food and Rural Affairs (Defra). Advice on lead paint in older homes. 2013. Available at https://www.gov.uk/government/publications/advice-on-lead-paint-in-older-homes. Last accessed 10 May 2022.
National Health and Nutrition Examination Survey (US) (NHANES) 2021 Questionnaires, Datasets and Related Documentation. Available at https://wwwn.cdc.gov/nchs/nhanes/ . Last accessed 18 May 2022.
TSoi M-F, Cheung C-L, Cheung TT, Cheung BMY,. Continual decrease in blood lead level in Americans: United States National Health Nutrition and Examination Survey 1999–2014. Am J Med. 2016;129(11):1213–8.
Chen RT, Orenstein WA. Epidemiologic methods in immunization programs. Epidemiol Rev. 1996;18(2):99–117. https://doi.org/10.1093/oxfordjournals.epirev.a017931 PMID: 9021306.
Tebby C, Caudeville J, Fernandez Y, Brochot C. Mapping blood lead levels in French children due to environmental contamination using a modeling approach. Science of the total environment. 2022;808. https://doi.org/10.1016/j.scitotenv.2021.152149T.
World Health Organization (WHO) Europe. Levels of lead in children’s blood. Fact sheet 4.5. December 2009. 2009. CODE: RPG4_Chem_Ex1 European Environment and Health information Centre, Accessed 4/2/22. https://www.euro.who.int/__data/assets/pdf_file/0003/97050/4.5.-Levels-of-lead-in-childrens-blood-EDITING_layouted.pdf.
Naicker N, et al. Prenatal and adolescent blood lead levels in South Africa: child, maternal and household risk factors in the birth to twenty cohort. Environ Res. 2010;110(4):355–62.
Whelan EA, Piacitelli GM, Gerwel B, Schnorr TM, Mueller CA, Gittleman J, Matte TD. Elevated blood lead levels in children of construction workers. Am J Public Health. 1997;87(8):1352–5. https://doi.org/10.2105/ajph.87.8.1352.PMID:9279275;PMCID:PMC1381100.
Sallmén M, Suvisaari J, Lindbohm ML, Malaspina D, Opler MG. Paternal occupational lead exposure and offspring risks for schizophrenia. Schizophr Res. 2016;176(2–3):560–5. https://doi.org/10.1016/j.schres.2016.06.004 Epub 2016 Jun 16 PMID: 27318522.
Leroux IN, Ferreira APSd, Silva JPd, et al. Lead exposure from households and school settings: influence of diet on blood lead levels. Environ Sci Pollut Res. 2018;25:31535–42. https://doi.org/10.1007/s11356-018-3114-8.
Tapper J. Science project reveals high lead levels in schools’ water. The Observer newspaper. 2021. Available at: https://www.theguardian.com/environment/2021/sep/05/science-project-reveals-high-lead-levels-in-schools-water. Last accessed 18 May 2022.
ODPM (Office of the Deputy Prime Minister). Housing Health and Safety Rating System. Operating Guidance. 2006. Available at https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/15810/142631.pdf. Last accessed 18 May 2022.
Schwab LT, et al. Inaccuracy in parental reporting of the age of their home for lead-screening purposes. Arch Pediatr Adolesc Med. 2003;157(6):584–6.
US department of Housing and Urban Development. American Healthy Homes Survey II. 2022. Available at https://www.hud.gov/program_offices/healthy_homes/ahhs_ii. Last accessed 4 Aug 2022.
UK National Screening Committee. Child screening programme for Lead Poisoning Review. 2022. Available at: https://view-health-screening-recommendations.service.gov.uk/lead-poisoning/. Last accessed 11/2/2022.
Acknowledgements
The authors would like to thank the staff of UKHSA Geographic Information System (GIS) team for facilitation of the residential property classification of cases. The authors would like to acknowledge the provision of the experimental dataset on housing characteristics from the Ordnance Survey and the use of the dataset for this study. We thank Rebecca Ingham, Advanced Health Protection Practitioner, Yorkshire and Humber HPT, UKHSA, for the use of the photograph. The authors would also like to thank Health Protection Teams for providing advice to cases and capturing risk factor information for cases.
Funding
Routine work undertaken by UKHSA as part of public health response. The research was part-supported by the National Institute for Health Research (NIHR) Health Protection Research Unit in Environmental Exposures and Health, a partnership between UK Health Security Agency, the Health and Safety Executive and the University of Leicester.
Author information
Authors and Affiliations
Contributions
HC designed the study concept, methods, conducted analysis, mapping and lead the writing of the article. NV advised on statistical analysis. AB and GL are principal investigators of the surveillance and made significant contributions to conception of the study design. All authors contributed to the interpretation of results, critical review and contributed to the writing and editing of the article. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. All data were collected within statutory approvals granted to UKHSA for public health disease surveillance and control. Information was held securely and in accordance with the Data Protection Act 2018, GDPR and Caldicott guidelines. Ethics approval is deemed unnecessary according to national regulations for Public Health Surveillance under the UK Health Protection Regulations (2010, as amended).
All data were collected within statutory approvals granted to UKHSA for public health disease surveillance and control. Information was held securely and in accordance with the Data Protection Act 2018, GDPR and Caldicott guidelines. The Privacy Notice for the use of case data is described in [2].
Consent for publication
All data were collected within statutory approvals granted to UKHSA for public health disease surveillance and control. Information was held securely and in accordance with the Data Protection Act 2018, GDPR and Caldicott guidelines. Consent for publication was approved via UKHSA approval processes. Written informed consent for publication of Fig. 1 was obtained from the owner.
The views expressed in this article are those of the author(s) and are not necessarily those of UK Health Security Agency or the Department of Health and Social Care.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Goodness of fit of the four models and comparison of AIC/BIC and models with and without the random effect.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Crabbe, H., Verlander, N.Q., Iqbal, N. et al. ’As safe as houses; the risk of childhood lead exposure from housing in England and implications for public health’. BMC Public Health 22, 2052 (2022). https://doi.org/10.1186/s12889-022-14350-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14350-y