
Abstract
Background
Undernutrition is a significant public health challenge and one of the leading causes of child mortality in a wide range of developing countries, including Ethiopia. Poor access to water, sanitation, and hygiene (WASH) facilities commonly contributes to child growth failure. There is a paucity of information on the interrelationship between WASH and child undernutrition (stunting and wasting). This study aimed to assess the association between WASH and undernutrition among under-five-year-old children in Ethiopia.
Methods
A secondary data analysis was undertaken based on the Ethiopian Demographic and Health Surveys (EDHS) conducted from 2000 to 2016. A total of 33,763 recent live births extracted from the EDHS reports were included in the current analysis. Multilevel logistic regression models were used to investigate the association between WASH and child undernutrition. Relevant factors from EDHS data were identified after extensive literature review.
Results
The overall prevalences of stunting and wasting were 47.29% [95% CI: (46.75, 47.82%)] and 10.98% [95% CI: (10.65, 11.32%)], respectively. Children from households having unimproved toilet facilities [AOR: 1.20, 95% CI: (1.05,1.39)], practicing open defecation [AOR: 1.29, 95% CI: (1.11,1.51)], and living in households with dirt floors [AOR: 1.32, 95% CI: (1.12,1.57)] were associated with higher odds of being stunted. Children from households having unimproved drinking water sources were significantly less likely to be wasted [AOR: 0.85, 95% CI: (0.76,0.95)] and stunted [AOR: 0.91, 95% CI: (0.83, 0.99)]. We found no statistical differences between improved sanitation, safe disposal of a child’s stool, or improved household flooring and child wasting.
Conclusion
The present study confirms that the quality of access to sanitation and housing conditions affects child linear growth indicators. Besides, household sources of drinking water did not predict the occurrence of either wasting or stunting. Further longitudinal and interventional studies are needed to determine whether individual and joint access to WASH facilities was strongly associated with child stunting and wasting.
Similar content being viewed by others

Introduction
Undernutrition, which includes stunting (low height-for-age), wasting (low weight-for-height), and underweight (low weight-for-age), is one of the major public health problems and makes children under-five years of age (under-fives) in particular, more vulnerable to disease and death. Stunting results from chronic or recurrent undernutrition, whereas wasting usually indicates recent and severe weight loss because a person has not had sufficient food intake and/or has had an infectious disease, such as diarrhea, resulting in rapid weight loss [1].
Early childhood linear growth is a strong indicator of healthy growth and is linked to child development in several domains, including cognitive, language, and sensory-motor capacities [2]. Globally, in 2020, 149 million under-fives were estimated to be stunted (too short for their age), and 45 million were estimated to be wasted (too thin for height). Undernutrition was reported to be responsible for approximately 45% of deaths among under-fives in low- and middle-income countries (LMICs), with Sub-Saharan Africa (SSA) bearing the greatest burden [1, 3, 4].
Undernutrition remains pervasive, with stunting, wasting, and underweight highly prevalent in SSA [3, 4]. Previous studies have shown this region to have the highest prevalence of stunting at 32% [5], underweight at 16.3%, and wasting at 7.1% [4]. A closer examination showed that the prevalence of malnutrition was highest in Eastern African countries, including Ethiopia [4, 6].
According to the 2019 Ethiopian Mini Demography and Health Surveys (EDHS) report, 37% of under-fives were stunted, 21% were underweight, and 7% were wasted [7]. In Ethiopia, several primary studies have also revealed that the prevalence of stunting and wasting in children ranges from 49.2 to 58.1% [8,9,10,11,12] and 13–17% [10,11,12], respectively. A systematic review conducted in Ethiopia showed that the overall pooled prevalence estimates of stunting, underweight, and wasting were 34.42%, 33.0%, and 15.0%, respectively [6].
In Ethiopia, several studies have identified the predictors of childhood undernutrition, revealing factors associated with stunting as the age of the child [8, 9], households that did not treat drinking water at the point of use [8], access to combined improved WASH facilities [10], lack of improved sanitation facilities [11], maternal body mass index (BMI) [8, 11, 12], lack of maternal education [13, 14], poor wealth status [13,14,15], house main floor material [13], lack of exclusive breastfeeding among infant under 6 months of age [12], no intake of meat by a child [12], birth size [13, 14], birth order [9], short birth interval [11], and a child having repeated diarrheal episodes [12]. Similarly, different studies elicited the predictors of wasting in children ,including: being born smaller than average size [10], sex of the child [8, 16], cough [8], fever [17], maternal body mass index [10], maternal education [8, 18], maternal occupation [8], diarrheal morbidity [16, 18, 19], and initiating complementary food before 6 months of age [18]. The evidence further indicates that children with poor access to proper WASH are likely to experience impaired child growth [20]. However, in SSA, studies on the effects of WASH on child growth are limited [21,22,23,24]. In Ethiopia, scientific evidence explicitly focusing on the relationship between WASH and childhood malnutrition is scarce [10, 25, 26].
Previous studies using EDHS datasets were surveyed specifically and focused on socioeconomic inequality [27], stunting [13, 14, 17], trends in child growth failure [28], investigating spatial variations [11], and focusing on concurrent nutritional deficiencies [9]. Besides, there is no quantitative pooled data evidence on the association between WASH and childhood undernutrition [10, 11].
Because malnutrition, especially undernutrition, remains endemic in Ethiopia, further evidence is needed to identify the links between WASH and both acute and chronic malnutrition in order to inform future directions for research in this area. This study aimed to assess the association between WASH and undernutrition (wasting and stunting) among under-fives in Ethiopia. Findings from this study will potentially inform and enable policymakers and public health researchers to target vulnerable children in the population for future interventions.
Methods
Study setting
Ethiopia is Africa’s second-most populated country, after Nigeria, with a population of over a hundred million people. Ethiopia, with a federal system of government has 10 regions (i.e., Afar, Amhara, Benishangul-Gumuz, Gambella, Harari, Oromia, Somali, Sidama, Southern Nations and Nationalities and People (SNNP), and Tigray) and two chartered cities (i.e., Addis Ababa and Dire Dawa). Ethiopia shares borders with Eritrea in the north, Kenya and Somalia in the south, South Sudan and North Sudan in the west, and Djibouti and Somalia in the East [29].
Data source
The datasets from the four rounds of the Ethiopian Demography and Health Surveys (EDHS) conducted from 2000 to 2016 were used in this study [29,30,31,32]. The EDHS is a nationally representative survey collected every five years, providing population and health indicators at the regional and national levels. The EDHS used a multistage cluster sampling technique, whereby data are hierarchical (i.e., children and mothers were nested within households, and households were nested within clusters). For this reason, we employed a multilevel logistic regression model, which has many advantages over the classical logistic regression model and is appropriate for analysing factors from different levels. A detailed description of analysis is presented in the data analysis section. The datasets of each survey were obtained from the following EDHS data repository https://dhsprogram.com.
Sampling and data collection
In brief, the 2000 and 2005 data were collected based on the 1994 population and housing census frame, while the 2011 and 2016 data were collected based on the 2007 population and housing census frame [29,30,31,32]. EDHS data were collected using a stratified two stage cluster sampling technique. In the first stage, a total of 539 enumeration areas (EAs) or clusters (138 in urban areas and 401 in rural areas), 540 EAs (145 urban and 395 rural), 624 clusters (187 in urban areas and 437 in rural areas), and 645 clusters (202 in urban areas and 443 in rural areas) were selected using systematic sampling with probability proportional to size, respectively the 2000, 2005, 2011 and 2016 EDHS surveys. At the second sampling stage, a systematic sample of households per EA was selected in all the regions to provide statistically reliable estimates of key demographic and health variables.
The EDHS used a questionnaire that was adapted from model survey tools developed for the DHS Program project. Mothers or caregivers provided all information related to children and mothers or caregivers through face-to-face interviews which were held at their homes. Water, Sanitation and Hygiene (WASH) indicators were also collected through face-to-face interviews and observation methods.
The EDHS collected data on children’s nutritional status by measuring the weight and height of under-fives in all sampled households. Weight was measured with an electronic mother-infant scale (SECA 878 flat) designed for mobile use. Height was measured with a measuring board (Shorr Board). Children younger than 24 months were measured lying down on the board (recumbent length), while standing height was measured for older children, in conformity with previous studies[29,30,31,32].
Study variables
Outcome variables
The prevalence of stunting and wasting, defined by the World Health Organization (WHO), were the primary outcome variables of interest [33]. Height-for-age is a measure of linear growth retardation and cumulative growth deficits. Children, whose height-for-age Z-scores were below minus two standard deviations (-2 SD) from the median of the reference population, were considered short for their age (stunted) or chronically undernourished [33, 34].The weight-for-height index measures body mass in relation to body height or length and describes current nutritional status. Children, whose Z-scores below minus two standard deviations (-2 SD) from the median of the reference population, were considered thin (wasted) or acutely undernourished [33].
Exposure variables
The key exposure variables examined were all variables related to WASH, and specifically, sanitation facility (improved/unimproved), sources of drinking water (improved/unimproved), time to obtain drinking water (round trip) were classified as ‘water on premise’, ‘≤ 30 minutes round-trip fetching times’, ‘31–60 minutes round-trip fetching times’, ‘and > 60 minutes round-trip fetching times’, child stool disposal (safe/unsafe), and housing floor (improved/unimproved). A household floor was considered as improved only if households were without dirt floors. The World Health Organization (WHO)/ United Nations Children’s Fund (UNICEF)- Joint Monitoring Programme (JMP) for water improved supply and sanitation definition was taken into consideration in this study [35]. Unsafe disposal of children’s stool was defined as the disposal of faeces in any site other than a latrine, whereas other methods such as “child used latrine or latrine” and “put/rinsed into latrine or latrine” were considered as “safe disposal” [36] (Table 1).
Confounders/control variables
As undernutrition results from a combination of factors, several control variables were considered in this study. We classified the control variables as child-related, parental-related, household-related, and community-related. As a result, the following factors were considered in the analysis. Child-related variables include: diarrhea, fever, symptoms of acute respiratory infection (ARI), sex, age (months), birth order, birth interval, size of child at birth (mother’s perceived baby size at birth), currently breastfeeding, early initiation of breastfeeding (children born in the past 2 years who started breastfeeding within one hour of birth), received all basic vaccination (i.e., child received a Bacillus Calmette–Guérin [BCG] vaccination against tuberculosis, 3 doses of Diphtheria, pertussis, and tetanus vaccine [DPT], ≥ 3 doses of polio vaccine [OPV], and 1 dose of measles vaccine). Parental-related factors included: mother’s age, mother’s educational level (no education, primary, secondary, and higher), mother’s occupation (not working, non-agriculture, or agriculture), antenatal care visits (ANC) (none, 1–3, or 4+), maternal body mass index (BMI), husband’s educational level, husband’s occupation (not working, non-agriculture, or agriculture), listening to the radio, and watching television. Household-level factors include: wealth index categorized (poor, middle, or rich) and household size (1–4 or ≥ 5). The wealth index is categorised into five wealth quintiles: ‘very poor’, ‘poor’, ‘middle’, ‘rich’ and ‘very rich. For this analysis, we re-coded the wealth index into three categories for adequate sampling in each category: ‘poor’ (poor and very poor), ‘middle’ and ‘rich’ (rich and very rich). Community-level factors include: ecological zone (tropical zone, subtropical zone, and cool zone), place of residence (urban and rural), and region (agrarian, pastoralist, and city-dweller).
Statistical analysis
All statistical analyses were conducted using Stata™ software version 15.1 (Stata Corp, College Station, TX, USA). Descriptive statistics were used to describe the socio-demographic and economic characteristics of children included in the study. Differences in the two outcome variables “stunting” and “wasting” were presented across socio-demographic characteristics of interest using frequencies and percentages. A multilevel logistics regression analysis was performed using a stage modelling approach for each outcome (i.e., stunting and wasting). This means that each of the five-level factors (i.e., WASH, child-related factors, parental-related factors, household-related factors, and community-level factors) were examined using a series of multilevel logistic regression models, adjusting for selected potential confounders. A multilevel logistic regression model was used because of the nested structure of the EDHS data (i.e., individuals nested within households and households nested within clusters). Sampling weight was used during data analysis to adjust for non-proportional allocation of sample and possible differences in response rates across regions included in the survey. A detailed explanation of the weighting procedure has described in the EDHS methodology report [29,30,31,32]. Hierarchical multilevel models were run following the recommendations of a previous study that suggest complex hierarchical relationships of different determinants at different levels [37]. This approach allowed distal factors to be adequately investigated without interference from proximal factors [38]. A similar approach was also used to identify previous related literature [39].
In brief, a multilevel bivariable logistic regression model (Model 0- maximum model) was fitted with each explanatory variable to select candidates with p-value a < 0.20 for the stage multivariable models. Accordingly, Model 1 incorporated WASH variables only. Model 2 incorporated WASH plus child-related variables (all child-related explanatory variables with p-values < 0.2 from Model 0 were entered into the Model1). Model 3 incorporated WASH + child-related variables + parental-related factors (all parental-related variable with p-values < 0.2 from Model 0 were entered into Model 3). Model 4 incorporated WASH + child-related factors + parental-related factors + household-related factors (all household-related variables with p-values < 0.2 from Model 0 were entered into the model 4). Model 5 incorporated WASH + child-related variables + parental factors + household factors + community-level factors. Model 6 was the final model that included only variables with a p-value < 0.2 from Model 5. Both crude odds ratio (COR) and adjusted odds ratio (AOR) ,along with 95% confidence intervals (CI), were used to estimate the strength of the association between explanatory and response variables.
Results
Summary of descriptive statistics
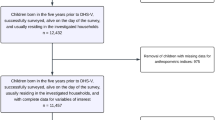
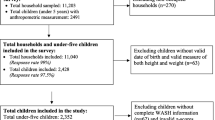
The background characteristics of children and prevalence of stunting and wasting across different background characteristics and covariates are presented in Table 2. In the current study, a total weighted sample of 33,744 and 33,763 under-five-year-old children was included to investigate child stunting and wasting, respectively. 51% of under-five children were males. 59% of children were older than twenty-four months. About one-third (33.9%) were from the rich categories. Nearly three-quarters (72.9%) of the mothers, and more than half of the husbands (54.2%) had no previous formal education. In this study, most children lived in rural (89.2%) and agrarian regions (54.4%). More than half (56.6%) of households practiced open defecation, 38.6% used unimproved sources of drinking water, and 78.9% practiced unsafe child stool disposal.
Prevalence of stunting and wasting
The overall prevalences of stunting and wasting were found to be 47.29% (95% CI: 46.75, 47.82%) and 10.98% (95% CI: 10.65, 11.32%), respectively. The prevalence of stunting among males was higher than females (52.9%; 47.1%), and similarly for wasting (55.6%; 44.4%). There was a higher burden of stunting in rural areas (92.1%) than in urban areas (7.9%). Children in households practising open defecation had a higher prevalence of stunting (62.9%) and wasting (65.8%) compared to their counterparts who did not practise open defecation (Table 2).
The prevalence of stunting and wasting by other WASH, child, and parental characteristics is shown in Table 3. In the multilevel bivariable binary logistic regression, we assessed the unadjusted or crude relationship between WASH and the prevalence of stunting and wasting among children (Additional File 1 and 2). The crude association revealed that the children from households with unimproved WASH facilities faced comparatively higher occurrences of stunting and wasting.
WASH factors associated with stunting
WASH factors associated with stunting included latrine facilities, sources of drinking water, and household flooring. Children from households having unimproved latrine facilities [AOR: 1.20, 95% CI: (1.05, 1.39)], practising open defecation [AOR: 1.29, 95% CI: (1.11, 1.51)], and living in households with dirt floors [AOR: 1.32, 95% CI: (1.12, 1.57)] were more likely to be stunted. Those having unimproved drinking water sources were significantly less likely to be stunted [AOR: 0.91, 95% CI: (0.83, 0.99)] (Table 4).
In the final model, being female [AOR: 0.79, 95% CI: (0.72, 0.85)], birth order 2nd to 4th [AOR: 0.88, 95% CI: (0.78–0.98)], and birth order 5th or higher [AOR: 0.85, 95% CI: (0.75–0.96)] were less likely to be stunted. Children aged 12–23 months [AOR: 3.16; 95%: (2.59, 3.84)], aged ≥ 24 months [AOR: 6.47, 95% CI: (5.21–8.02)], average birth size [AOR:1.22, 95% CI: (1.11,1.34)], small size at birth [AOR:1.64, 95% CI: (1.48,1.82)], lack of maternal education [AOR: 1.54, 95% CI: (1.06,2.24)], lack of father education [AOR: 1.50, 95% CI: (1.17,1.92)], husband having primary education [AOR: 1.37,95% CI: (1.07,1.74)] were associated with increased odds of being stunted. Husbands being unemployed [AOR: 0.75, 95% CI: (0.61, 0.93)], and mothers with BMI ≥ 25 kg/m2 [AOR: 0.79, 95% CI: (0.65, 0.96)] were significantly associated with lower odds of being stunted. Children from poor households [AOR: 1.20, 95% CI: (1.07,1.35)] had higher odds of being stunted compared with children from the richest households. At the community level, children who lived in tropical [AOR: 0.67, 95% CI: (0.58,0.78)] and lived subtropical ecological zone [AOR: 0.75, 95% CI: (0.65,0.87)] were associated with lower odds of being stunted (Table 4).
WASH factors associated with wasting
We observed no evidence of an association between improved sanitation, safe disposal of a child’s stool, or improved household flooring and child wasting. Having unimproved drinking water sources was associated with lower odds of being wasted [AOR: 0.83, 95% CI: (0.73,0.93)]. Control variables associated with wasting included having diarrhea [AOR: 1.27, 95%CI: (1.11, 1.45)], having fever [AOR: 1.24, 95% CI: (1.09, 1.41)], birth order 5th or higher [AOR: 1.28, 95% CI: (1.09, 1.50)], and small size at birth [AOR: 1.58, 95% CI: (1.40, 1.82)] were associated with elevated odds of being wasted. Children from poor households [AOR: 1.40, 95% CI: (1.18, 1.66)] and those from middle households [AOR: 1.27, 95% CI: (1.05, 1.53)] reported higher odds of being wasted than those children from richest households. Being female [AOR: 0.73, 95% CI: (0.65,0.81)], age greater than 24 months [AOR: 0.62, 95% CI: (0.50,0.83)], having four and more ANC visits [AOR: 0.74, 95% CI: (0.64,0.87)], normal maternal BMI [AOR: 0.65, 95% CI: (0.58,0.73)], women classified as ‘overweight/obese’ [AOR: 0.39, 95% CI: (0.28,0.52)], and watching television [AOR: 0.71, 95% CI: (0.61,0.84)] were associated with lower odds of being wasted. At the community level, rural dwellers [AOR: 0.58, 95% CI: (0.46, 0.73)], and children who lived in tropical ecological zone [AOR: 1.61, 95% CI: (1.30, 1.99)] reported higher odds of being wasted (Table 5).
Discussion
A selection of socioeconomic and demographic variables as controlling factors were significantly associated with the prevalence of stunting and wasting among children in Ethiopia as demonstrated above. Early childhood linear growth is a strong indicator of healthy growth and is linked to child development in several domains. One of the factors affecting nutritional status in childhood is poor WASH. The lack of access to WASH may also affect children’s health and well-being in various ways (for example, through repeated exposure of diarrheal infections), which potentially increases the risk of wasting. This study identified the association between WASH factors and childhood undernutrition in Ethiopia. This study’s overall prevalence of stunting and wasting was 47.29% and 10.98%, respectively.
Stunting was associated with latrine facilities, sources of drinking water, and household flooring. All WASH factors (sanitation facility, sources of drinking water, disposal of the child’s stool, and time to the water source) were individually related to stunting among Ethiopian children under the age of five. However, only a few WASH variables remained statistically significant after correcting potential confounders.
Under-fives who lived with families where open defecation was practised, were more likely to be stunted. This finding agrees with recent findings from the Ethiopian research project entitled GROW (Growing Nutrition for Mothers and Children), which found that open defecation was strongly connected with stunting in Ethiopia [40]. Open defecation, which may be associated with poor sanitation and hygiene, is a significant predictor of a wide range of population diseases, including bacaterial and viral diarrhoeal illnesses such as typhoid, cholera, hepatitis, and are among childhood infectious conditions that are associated with undernutrition [41]. A study in India showed that children from households that defecate in the open have a 14% higher likelihood of being stunted than children from households that use improved latrines [42]. Another study by Rah et al. reported that compared with open defecation, household access to a latrine facility was associated with a 16–39% reduced odds of stunting among children aged 0–23 months, after adjusting for all potential confounders [43]. This finding indicated that children living in locations where open defecation was common were more vulnerable to stunting, and this is due to repeated episodes of diarrheal illnesses in these localities. Repeated episodes of diarrhea are known to be linked with poor WASH. Diarrheal illness contributes to undernutrition by reducing food intake, nutrient absorption, and increasing the catabolism of nutrient stores.
Previous literature has widely acknowledged the relationship between unimproved sanitation and stunting [42, 44, 45]. This finding was reaffirmed in the current study as children from households having unimproved latrines were more likely to be stunted. Analysis of a variety of cross-sectional studies based on data from the Demographic and Health Surveys (DHS) from other countries have also indicated that improved sanitation is important for the linear growth of children. For instance, data from 172 Demographic and Health Surveys (DHS) showed that the odds of being stunted were lower in households with access to improved sanitary facilities [46]. On the other hand, studies from India and Indonesia reported that open defecation was negatively associated with height-for-age measures [47, 48].
It was hypothesised that improved water sources could have been linked to moderate-to-severe stunting [49, 50]. In this study however, we observed a negative association between unimproved sources of drinking water and lower odds of being stunted. In the bivariable multilevel model children from households that use unimproved sources of drinking water had higher odds of being stunted (OR: 1.39, 95% CI: 1.32–1.46, p-value < 0.001). This association did not remain consistent after adjustingg for individual and community variables. In line with this finding, Torlesse et al. reported that stunting was not associated with the household’s source of drinking water [48]. Another study from Indonesia also reported that the source of drinking water was not predictive of stunting [51]. On the other hand, the unavailability of water was reported as a significant factor associated with moderate and severe stunting [44, 52]. A cross-sectional study from Kersa, Ethiopia reported that households using non-piped water and that did not treat drinking water were at higher odds of being stunted [AOR: 1.5, 95% CI (1.07–2.00)], and [AOR: 1.9, 95% CI (1.31–2.85)], respectively [8]. The difference in the definitions of the terms across studies the and quality of drinking water including microbiological features, might have contributed to this inconsistent association. Furthermore, large experimental studies, such as the WASH-Benefits Bangladesh [53], the WASH-Benefits Kenya [21] and the Sanitation Hygiene Infant Nutrition Efficacy (SHINE) trials in Zimbabwe [22] found no effects of any WASH intervention on child linear growth. The evidence for the association between the water source and stunting remains unclear [48]. A study by Cumming and Cairncross suggested that the causal pathways linking poor WASH to child developmental are complex, spanning multiple routes [44].
The causes of stunting are multifactorial and interlinked, as depicted by various conceptual frameworks [54]. Our findings support the idea that nutrition interventions alone are unlikely to improve childhood nutritional problems. Importantly, in this study, children from households with dirt floors had higher odds of being stunted than their counterparts. Cross-sectional data from 54 Demographic and Health Surveys showed that improved housing was associated with 12% lower odds of stunting [55]. Current evidence clearly shows that the housing environment has significantly impacts children’s growth and development [55, 56].
WASH factors such as the type of latrine facilities, the disposal of the child’s stool, and household flooring were significantly associated with wasting in the unadjusted bivariable multilevel model. Still, they were all diminished after adjusting for all potential confounders. In this study, the type of latrine facilities, the disposal of the child’s stool, and household flooring were not significantly associated with childhood wasting in the final model. One possible explanation for the lack of association in our analysis is that there may be a weak link between safe and adequate coverage of improved water different parts of the country. Similar findings were reported by studies conducted in multiple countries including Ethiopia [10], Guatemala [57], and Nepal [58]. For instance, a study conducted in Ethiopia showed that access to improved individual water, sanitation, handwashing and combined WASH facilities were not predictive of wasting in children when adjusted for confounders [10]. Conversely, a study conducted among Afghan children found increased odds of wasting among children with unimproved water sources to children withen who had access to protected water sources [59].
We also observed an inversely significant relationship between the use of unimproved sources of drinking water and a lower likelihood of wasting. The lack of relevant data on bacteriological quality, chemical, physical properties of drinking water, and the duration of households with improved water sources in the EDHS datasets may explain the inverse association we found between the use of unimproved sources of drinking water and a lower risk of wasting. In this case, our definition did not meet the criteria for a safely managed drinking water service, which means that households must use an improved source that is: accessible on premises, available when needed, and free of contamination, as stated by the new global indicators for drinking water definition of WHO/UNICEF Joint Monitoring Programme for Water Supply and Sanitation [60]. Furthermore in Ethiopia, most household residents in both urban (88%) and rural (92%) areas report that they do not treat their water prior to drinking [29].
The current study used representative population-based data with a high response rate and was analyzed by adjusting for weighting, clustering, and stratification. There are some limitations to this study. Firstly, cause-effect relationships could not be established in the current study due to the study design. Secondly, due to a lack of relevant data in EDHS, the effects of the microbiological, chemical, and physical properties of drinking water sources on child growth outcomes is unknown. Thirdly, because the only access to WASH facilities was considered, the true association between WASH practices and child growth outcomes may be underestimated. Fourthly, as is often the situation in observational cross-sectional studies, it is difficult to rule out biases, included the recall biases in the current study. Fifthly, our study may have been hampered by unmeasured confounders, such as dietary practices and food security problems.
Conclusion
The present study showed that children from households that defecated in the open and had unimproved latrine facilities were more likely to be stunted. Similarly, when adjusted, a significant association of children’s linear growth failure (stunting) among under-five children was found among children living in households with dirt floors. On the other hand, there was no evidence of a relationship between wasting and the type of latrine facilities, the disposal of the child’s stool, or household flooring. Having unimproved drinking water sources was associated with lower odds of being wasted. Policies and interventions should target improved sanitation and housing conditions in order to prevent child stunting. Finally and to enlighten more on these issues in Ethiopia, further longitudinal and interventional studies are warranted, to examine the effects of access to WASH facilities and/or household WASH practices and their association with child nutritional status and development.
Abbreviations
- AOR:
-
Adjusted odds ratio
- ANC:
-
antenatal care visits
- BMI:
-
body mass index
- CI:
-
Confidence interval
- EDHS:
-
Ethiopian Demographic and Health Surveys
- SNNP:
-
Southern Nations and Nationalities and People
- WASH:
-
Water, sanitation, and hygiene
- WHO:
-
World Health Organization
References
Fact sheets -. Malnutrition [Internet]. [cited 2022 Jan 16]. Available from: https://www.who.int/news-room/fact-sheets/detail/malnutrition.
Stunting in a nutshell [Internet]. [cited 2022 Jan 12]. Available from: https://www.who.int/news/item/19-11-2015-stunting-in-a-nutshell.
Akombi BJ, Agho KE, Hall JJ, Wali N, Renzaho AMN, Merom D. Stunting. Wasting and Underweight in Sub-Saharan Africa: A Systematic Review. Int J Environ Res Public Health. 2017 Aug;14(8):863.
Akombi BJ, Agho KE, Merom D, Renzaho AM, Hall JJ. Child malnutrition in sub-Saharan Africa: A meta-analysis of demographic and health surveys (2006–2016). PLOS ONE. 2017 May 11;12(5):e0177338.
Ssentongo P, Ssentongo AE, Ba DM, Ericson JE, Na M, Gao X, et al. Global, regional and national epidemiology and prevalence of child stunting, wasting and underweight in low- and middle-income countries, 2006–2018. Sci Rep. 2021 Mar;4(1):5204. 11(.
Abdulahi A, Shab-Bidar S, Rezaei S, Djafarian K. Nutritional Status of Under Five Children in Ethiopia: A Systematic Review and Meta-Analysis. Ethiop J Health Sci. 2017 Mar;27(2):175–88.
EPHI ICF. Ethiopia MiniDemographic and Health Survey 2019: Key indicators. Maryland: EPHI and ICF.: Rockville; 2019.
Roba AA, Assefa N, Dessie Y, Tolera A, Teji K, Elena H, et al. Prevalence and determinants of concurrent wasting and stunting and other indicators of malnutrition among children 6–59 months old in Kersa, Ethiopia. Matern Child Nutr. 2021;17(3):e13172.
Geda NR, Feng CX, Henry CJ, Lepnurm R, Janzen B, Whiting SJ. Multiple anthropometric and nutritional deficiencies in young children in Ethiopia: a multi-level analysis based on a nationally representative data. BMC Pediatr. 2021 Jan 5;21(1):11.
Bekele T, Rahman B, Rawstorne P. The effect of access to water, sanitation and handwashing facilities on child growth indicators: Evidence from the Ethiopia Demographic and Health Survey 2016. PLoS ONE. 2020 Sep;22(9):e0239313. 15(.
Haile D, Azage M, Mola T, Rainey R. Exploring spatial variations and factors associated with childhood stunting in Ethiopia: spatial and multilevel analysis. BMC Pediatr. 2016 Apr;15(1):49. 16(.
Eshete Tadesse S, Chane Mekonnen T, Adane M. Priorities for intervention of childhood stunting in northeastern Ethiopia: A matched case-control study. PLoS ONE. 2020;15(9):e0239255.
Ayelign A, Zerfu T. Household, dietary and healthcare factors predicting childhood stunting in Ethiopia. Heliyon. 2021 Apr;7(4):e06733.
Fantay Gebru K, Mekonnen Haileselassie W, Haftom Temesgen A, Oumer Seid A, Afework Mulugeta B. Determinants of stunting among under-five children in Ethiopia: a multilevel mixed-effects analysis of 2016 Ethiopian demographic and health survey data. BMC Pediatr. 2019 Jun 1;19(1):176.
Stunting. and its determinant factors among children aged 6–59 months in Ethiopia | Italian Journal of Pediatrics | Full Text [Internet]. [cited 2022 Jan 28]. Available from: https://ijponline.biomedcentral.com/articles/https://doi.org/10.1186/s13052-017-0433-1.
Dires S, Mareg M. The Magnitude of Wasting and Associated Factors among Children Aged 2–5 Years in Southern Ethiopia: A Cross-Sectional Study. BioMed Res Int. 2021 May 7;2021:e6645996.
Muche A, Gezie LD, Baraki AG, egzabher, Amsalu ET. Predictors of stunting among children age 6–59 months in Ethiopia using Bayesian multi-level analysis. Sci Rep. 2021 Feb;12:11:3759.
Wasting in under. five children is significantly varied between rice producing and non-producing households of Libokemkem district, Amhara region, Ethiopia | BMC Pediatrics | Full Text [Internet]. [cited 2022 Jan 28]. Available from: https://bmcpediatr.biomedcentral.com/articles/https://doi.org/10.1186/s12887-019-1677-2.
Derso T, Tariku A, Biks GA, Wassie MM. Stunting, wasting and associated factors among children aged 6–24 months in Dabat health and demographic surveillance system site: A community based cross-sectional study in Ethiopia. BMC Pediatr. 2017 Apr;4(1):96. 17(.
Bekele T, Rawstorne P, Rahman B. Effect of water, sanitation and hygiene interventions alone and combined with nutrition on child growth in low and middle income countries: a systematic review and meta-analysis. BMJ Open. 2020 Jul 1;10(7):e034812.
Null C, Stewart CP, Pickering AJ, Dentz HN, Arnold BF, Arnold CD, et al. Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Kenya: a cluster-randomised controlled trial. Lancet Glob Health. 2018 Mar 1;6(3):e316–29.
Humphrey JH, Mbuya MNN, Ntozini R, Moulton LH, Stoltzfus RJ, Tavengwa NV, et al. Independent and combined effects of improved water, sanitation, and hygiene, and improved complementary feeding, on child stunting and anaemia in rural Zimbabwe: a cluster-randomised trial. Lancet Glob Health. 2019 Jan 1;7(1):e132–47.
Pickering AJ, Djebbari H, Lopez C, Coulibaly M, Alzua ML. Effect of a community-led sanitation intervention on child diarrhoea and child growth in rural Mali: a cluster-randomised controlled trial. Lancet Glob Health. 2015 Nov 1;3(11):e701–11.
Briceño B, Coville A, Martinez S. Promoting handwashing and sanitation evidence from a large-scale randomized trial in rural Tanzania. Policy research working paper 7164. World Bank, 2015.
Kwami CS, Godfrey S, Gavilan H, Lakhanpaul M, Parikh P. Water, Sanitation, and Hygiene: Linkages with Stunting in Rural Ethiopia. Int J Environ Res Public Health. 2019 Jan;16(20):3793.
Girma M, Hussein A, Norris T, Genye T, Tessema M, Bossuyt A, et al. Progress in Water, Sanitation and Hygiene (WASH) coverage and potential contribution to the decline in diarrhea and stunting in Ethiopia. Matern Child Nutr. n/a(n/a):e13280.
Mohammed SH, Muhammad F, Pakzad R, Alizadeh S. Socioeconomic inequality in stunting among under-5 children in Ethiopia: a decomposition analysis. BMC Res Notes. 2019 Mar;29(1):184. 12(.
Bekele T, Rawstorne P, Rahman B. Trends in child growth failure among children under five years of age in Ethiopia: Evidence from the 2000 to 2016 Demographic and Health Surveys. PLoS ONE. 2021 Aug;5(8):e0254768. 16(.
Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Maryland: CSA and ICF: Addis Ababa, Ethiopia, and Rockville; 2016.
Central Statistical Authority [Ethiopia] and ORC Macro. Ethiopia Demographic and Health Survey 2000. Maryland: Central Statistical Authority and ORC Macro: Addis Ababa, Ethiopia and Calverton; 2001.
Central Statistical Agency [Ethiopia] and ORC Macro. Ethiopia Demographic and Health Survey 2005. Central Statistical Agency/Ethiopia and ORC Macro; 2006.
Central Statistical Agency [Ethiopia] and ICF International. Ethiopia Demographic and Health Survey 2011. Central Statistical Agency and ICF International; 2012.
WHO child growth standards: methods and development. Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age. Geneva: World Health Organization; 2006. [Internet]. Available from: http://www.who.int/nutrition/publications/childgrowthstandards_technical_report_1/en/.
WHO Child Growth Standards. Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age. WHO. 2006. [Internet]. Available from: https://www.who.int/publications/i/item/924154693X.
World Health Organization (WHO) and UNICEF. Core questions on drinking water and sanitation for household surveys. World Health Organization and UNICEF; 2006.
World Health Organization (WHO): Guidelines on sanitation and health. 2018, Licence: CC BY-NC-SA 3.0 IGO. Genvea. https://apps.who.int/iris/bitstream/handle/10665/274939/9789241514705-eng.pdf?ua=1.
Victora CG, Huttly SR, Fuchs SC, Olinto MT. The role of conceptual frameworks in epidemiological analysis: a hierarchical approach. Int J Epidemiol. 1997 Feb;26(1):224–7.
Ezeh OK, Abir T, Zainol NR, Al Mamun A, Milton AH, Haque MR, et al. Trends of Stunting Prevalence and Its Associated Factors among Nigerian Children Aged 0–59 Months Residing in the Northern Nigeria, 2008–2018. Nutrients. 2021 Nov;29(12):4312. 13(.
Kumie A. The effect of improved water and sanitation on diarrhea: Evidence from pooled Ethiopia Demographic and Health Surveys – A multilevel mixed-effects analysis. Ethiop J Health Dev.:9.
Ahmadi D, Amarnani E, Sen A, Ebadi N, Cortbaoui P, Melgar-Quiñonez H. Determinants of child anthropometric indicators in Ethiopia. BMC Public Health. 2018 May 15;18(1):626.
Spears D, Ghosh A, Cumming O. Open Defecation and Childhood Stunting in India: An Ecological Analysis of New Data from 112 Districts. PLoS ONE. 2013 Sep;16(9):e73784. 8(.
Rahman MHU, Malik MA, Chauhan S, Patel R, Singh A, Mittal A. Examining the linkage between open defecation and child malnutrition in India. Child Youth Serv Rev. 2020 Oct 1;117:105345.
Rah JH, Cronin AA, Badgaiyan B, Aguayo VM, Coates S, Ahmed S. Household sanitation and personal hygiene practices are associated with child stunting in rural India: a cross-sectional analysis of surveys. BMJ Open. 2015 Feb 12;5(2):e005180.
Cumming O, Cairncross S. Can water, sanitation and hygiene help eliminate stunting? Current evidence and policy implications. Matern Child Nutr. 2016;12(S1):91–105.
Ademas A, Adane M, Keleb A, Berihun G, Tesfaw G. Water, sanitation, and hygiene as a priority intervention for stunting in under-five children in northwest Ethiopia: a community-based cross-sectional study. Ital J Pediatr. 2021 Aug;24(1):174. 47(.
Fink G, Günther I, Hill K. The effect of water and sanitation on child health: evidence from the demographic and health surveys 1986–2007. Int J Epidemiol. 2011 Oct;40(5):1196–204.
Chakrabarti S, Singh P, Bruckner T. Association of Poor Sanitation With Growth Measurements Among Children in India. JAMA Netw Open. 2020 Apr 15;3(4):e202791.
Torlesse H, Cronin AA, Sebayang SK, Nandy R. Determinants of stunting in Indonesian children: evidence from a cross-sectional survey indicate a prominent role for the water, sanitation and hygiene sector in stunting reduction. BMC Public Health. 2016 Jul 29;16(1):669.
Mengesha A, Hailu S, Birhane M, Belay MM. The Prevalence of Stunting and Associated Factors among Children Under Five years of age in Southern Ethiopia: Community Based Cross-Sectional Study. Ann Glob Health. 2021 Nov 17;87(1):111.
Asfaw M, Wondaferash M, Taha M, Dube L. Prevalence of undernutrition and associated factors among children aged between six to fifty nine months in Bule Hora district, South Ethiopia. BMC Public Health. 2015 Jan 31;15(1):41.
Rah JH, Sukotjo S, Badgaiyan N, Cronin AA, Torlesse H. Improved sanitation is associated with reduced child stunting amongst Indonesian children under 3 years of age. Matern Child Nutr. 2020;16(S2):e12741.
Agho KE, Akombi BJ, Ferdous AJ, Mbugua I, Kamara JK. Childhood undernutrition in three disadvantaged East African Districts: a multinomial analysis. BMC Pediatr. 2019 Apr 23;19(1):118.
Luby SP, Rahman M, Arnold BF, Unicomb L, Ashraf S, Winch PJ, et al. Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Bangladesh: a cluster randomised controlled trial. Lancet Glob Health. 2018 Mar 1;6(3):e302–15.
UNICEF. Improving child nutrition. The achievable imperative for global progress. 2013. Retrieved from New York: https://www.unicef.org/gambia/Improving_Child_Nutrition_-_the_achievable_imperative_for_global_progress.pdf.
Tusting LS, Gething PW, Gibson HS, Greenwood B, Knudsen J, Lindsay SW, et al. Housing and child health in sub-Saharan Africa: A cross-sectional analysis. PLOS Med. 2020 Mar 23;17(3):e1003055.
Gao Y, Zhang L, Kc A, Wang Y, Zou S, Chen C, et al. Housing environment and early childhood development in sub-Saharan Africa: A cross-sectional analysis. PLoS Med. 2021 Apr;18(4):e1003578.
Arnold B, Arana B, Mäusezahl D, Hubbard A, Colford JM Jr. Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. Int J Epidemiol. 2009 Dec 1;38(6):1651–61.
Langford R, Lunn P, Panter-Brick C. Hand-washing, subclinical infections, and growth: a longitudinal evaluation of an intervention in Nepali slums. Am J Hum Biol Off J Hum Biol Counc. 2011 Oct;23(5):621–9.
Frozanfar MK, Yoshida Y, Yamamoto E, Reyer JA, Dalil S, Rahimzad AD, et al. Acute malnutrition among under-five children in Faryab, Afghanistan: prevalence and causes. Nagoya J Med Sci. 2016 Feb;78(1):41–53.
WASH in. the 2030 Agenda New global indicators for drinking water, sanitation and hygiene. [Internet]. Available from: https://washdata.org/report/jmp-2017-wash-2030-agenda.
Acknowledgements
We would like to thank the Measure DHS Program for providing the DHS datasets.
Funding
No organization funded this research.
Author information
Authors and Affiliations
Contributions
BS: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft. PP: Visualization, Validation, Writing – review & editing. AK: Supervision, Visualization, Methodology, Writing – review & editing. LM: Visualization, Validation, Writing – review & editing. GB: Writing – review & editing. DA, YT, DZ, and FD: Writing – review & editing. KEA: Supervision, Visualization, Validation, Writing – review & editing. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The data were obtained via online registration to measure the DHS program and downloaded after the purpose of the analysis was communicated and approved. An approval letter for the use of the EDHS data set was gained from MEASURE DHS. Only de-identified data were used and no information obtained from the data set was disclosed to any third party. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Data availability
The dataset was demanded and retrieved from the DHS website https://dhsprogram.com after formal online registration and submission of the project title and detailed description.
Competing interests
The authors declare that they have no any competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sahiledengle, B., Petrucka, P., Kumie, A. et al. Association between water, sanitation and hygiene (WASH) and child undernutrition in Ethiopia: a hierarchical approach. BMC Public Health 22, 1943 (2022). https://doi.org/10.1186/s12889-022-14309-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14309-z