
Abstract
Objectives
Sarcopenia is a clinically relevant syndrome with health, social, and economic implications. Alcohol consumption is one of the risk factors for sarcopenia, but it has not been fully investigated in Chinese populations. The purpose of the present study was to assess the relationship between alcohol consumption patterns (including the volume and frequency of alcohol consumption) and sarcopenia or its elements among Chinese women and men from Henan Province.
Method
A cross-sectional study was designed to collect information about nutrition and health in Henan Province, China, and a total of 680 individuals were studied. Sarcopenia was defined according to the Asian Working Group for Sarcopenia (AWGS) criteria updated in 2019. Alcohol consumption was calculated in grams per day and divided into three groups. Drinking frequency was divided into four groups. We assessed the likelihood that sarcopenia was associated with drinking patterns using multiple logistic regression analysis by odds ratios (ORs) with 95% confidence interval (CIs) after multiple adjustments.
Results
We found that men who consumed > 25 g of ethanol per day were approximately three times more likely to have low muscle mass (OR, 3.99; 95% CI, 1.10–17.05) or low grip strength (OR, 3.39; 95% CI, 1.33–9.92) than nondrinkers after multiple adjustments. In addition, males who consumed alcohol more than 4 times per week were approximately threefold to fivefold more likely to have low muscle mass (OR, 4.99; 95% CI, 1.24–25.55) or low grip strength (OR, 3.37; 95% CI, 1.40–8.74) than nondrinkers. Unfortunately, we did not find a relationship between alcohol consumption patterns and sarcopenia or gait speed among males, and there was no association between alcohol consumption patterns and sarcopenia or any elements.
Conclusion
Heavy alcohol consumption and frequent drinking are important risk factors for low muscle mass and muscle strength in Chinese men from Henan province.
Similar content being viewed by others


Introduction
The overall life expectancy of humans is dramatically increasing worldwide, leading to a surge in the elderly population. Aging is characterized by skeletal muscle mass decline by 1–2% annually after the age of 50, in concert with a decline in strength of 1.5% per year that accelerates to 3% annually after the age of 60 [1]. The characteristics of the decrease in muscle mass, muscle strength, and muscle efficiency with aging are often referred to as “sarcopenia” [2]. The prevalence of sarcopenia varies widely, ranging from 5.5 to 25.7% based on the Asian Working Group for Sarcopenia (AWGS) 2014 criteria for Asian populations [3]. Sarcopenia is considered to be an independent risk factor for various adverse outcomes, including osteoporosis, falls, reduced cardiopulmonary function, metabolic syndrome, and insulin resistance, and eventually leads to disability, longer lengths of stay at the hospital, readmission and death [4]. Thus, exploring the risk factors could be an effective solution for identifying early markers for sarcopenia prevention.
Alcohol consumption is responsible for 5.1% of the global burden of disease and injury [5]. Drinking alcohol is a widely accepted traditional Chinese cultural behavior. The drinking rate was 53.8% and 12.2% for men and women, respectively, based on the 2010–2012 national China Nutrition and Health Survey [6], which is increasing faster. [7]. Accordingly, drinking alcohol has become a serious problem that should be addressed.
Alcohol consumption is one of the modifiable behavioral factors that accelerates sarcopenia [8], which has attracted the attention of researchers. Some experimental studies among animals have demonstrated that alcohol consumption inhibits the synthesis of skeletal muscle proteins [9,10,11]. In humans, this relationship remains controversial, although a positive relationship has been reported between alcohol consumption and sarcopenia in the general population [12, 13]. In addition, the results of a recently reported meta-analysis did not support alcohol consumption as a risk factor for sarcopenia [14]. However, studies included in that meta-analysis were not designed considering the relationship between alcohol consumption and sarcopenia as the primary end point [15, 16].
In China, the relationship between alcohol consumption patterns and the risk of sarcopenia has not been fully investigated. Some studies focused on drinking frequency [17, 18], whereas others evaluated whether people should drink or not [19, 20], and most of them did not adjust for confounding factors in the analysis. In addition, no previous research has evaluated the effect of different alcohol consumption patterns as the primary end point on sarcopenia in Chinese populations. This is important because, except for drinking frequency, total alcohol intake may influence health outcomes. Accordingly, we assessed the association between patterns of alcohol consumption and the risk of sarcopenia using information from a cross-sectional study of general Chinese adults from Henan province.
Participants and methods
Study design and population
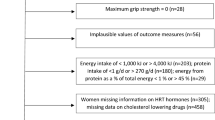
Our study population included residents aged 25–75 years from three communities in Henan, China. The diet, lifestyle, and anthropometry information of the participants was collected for investigation from January to November 2020, after excluding incomplete data and implausible energy intake. We excluded abstainers (n = 12) from the analysis because the number of people in this group was relatively small and because of the presumed presence of “sick quitters” (individuals who stopped drinking due to illness) among them [21]. We also excluded people with missing information (n = 75) or with conflicting answers regarding the amount and frequency of alcohol intake (n = 18). In all, 680 people (411 males and 269 females) were eligible for this study.
This study was approved by the Ethical Review Committee, and written informed consent was obtained from all participants (Protocol 2020–KY-066).
Sarcopenia assessment
Sarcopenia was measured by the recommended revised diagnostic algorithm of the AWGS [3]. Lean muscle mass in this study was measured by bioelectrical impedance analysis (Inbody 570, BioSpace, Seoul, Korea). All participants changed into paper gowns and were asked to remove all jewelry and other personal effects that could interfere with the examination. The appendicular skeletal muscle mass index (SMI) was calculated by the following formula: (lean mass from arm and leg)[kg]/height [m]2). Low muscle mass was defined by an SMI below 5.7 kg/m2 in females and below 7.0 kg/m2 in males. Muscle strength was assessed by grip strength, measured using a dynamometer (EH101; Camry, Zhongshan, China). The participants stood with their arms and wrists by the sides of the body and were asked to exert maximum grip with each hand. Tests were performed on two independent occasions, and the better of 2 results were chosen for analysis. The criteria were 28 kg and 18 kg for males and females, respectively. Usual gait speed (GS) on a 6 m course was used as an objective measure of physical performance, which was defined as < 1.0 m/s. Sarcopenia was identified by low muscle mass plus muscle strength or physical performance, and severe sarcopenia was diagnosed when all three criteria of the definition were met [3]. Because of the small sample size of this study, the sarcopenia stage (including severe sarcopenia) and its elements (low muscle mass, muscle strength, and physical performance) were analyzed.
Alcohol consumption assessment
Usual consumption of alcoholic beverages in the previous year was estimated with a validated diet history, which collected information on the beverage type (beer, wine, and hard liquor), the amount and frequency of intake, and used sets of food containers to help quantify the amount. Alcohol consumption was calculated in grams per day by multiplying the average frequency (times per day) by the usual consumption amount of each beverage and its average pure ethanol content (5.0 g for 100 g of beer, 12.0 g for 100 g of wine [22], and 40.0 g for 100 g of hard liquor) [23]. According to the dietary guidelines for Chinese residents [24], the recommendation for alcohol consumption is 25 g of pure ethanol per day for men and 15 g of pure ethanol per day for women. Accordingly, the participants were divided into three groups depending on the amount of alcohol consumed per day (nondrinker, light-to-moderate drinker (1–25 g/day), and heavy drinker (> 25 g/day)) for males and three groups (nondrinker, light-to-moderate drinker (1–15 g/day), and heavy drinker (> 15 g/day)) for females. The frequency of drinking was divided into four groups: nondrinker, < once/week, 1–4 times a week, and > 4 times a week.
Assessment of other variables
Data were collected by a general questionnaire and through two nonconsecutive 24-h dietary recalls. To help the respondents answer accurately, the 24-h dietary recalls were conducted face to face with the aid of food models. The average daily food intake and protein intake were analyzed by a nutrition calculator (Nutrition and Diet Management System of Traditional Chinese Medicine Combining with WesternMedcine software, NCCW software), which was calculated based on the China food composition Table [21]. Weight and height were measured by experienced investigators. The general questionnaire assessed age, sex, educational attainment, occupational status, marital status, income level, smoking status, snap frequency, and so on. Physical activity was collected through the Chinese version of the international physical activity questionnaire (IPAQ) [25], which appeared to have acceptable reliability and validity. Moderate-vigorous physical activity (Met-h/day, MET, metabolic equivalent of task) was calculated for each individual according to guidelines for Chinese residents [24].
Statistical analysis
Data analysis was performed by using SAS statistical software, version 9.3 (SAS Institute, Cary, NC, USA), for all data analyses. A p value < 0.05 was considered statistically significant.
The normality of continuous variables was first tested by the Shapiro‒Wilk test and Kolmogorov‒Smirnov test. According to the data distribution, continuous variables were described by parametric tests or nonparametric tests. Categorical variables are provided as percentages (%), and chi-squared tests were used to determine whether any significant differences existed between groups.
We assessed the likelihood that sarcopenia was associated with drinking patterns (alcohol consumption, drinking frequency) using multiple logistic regression analysis by odds ratios (ORs) with 95% confidence interval (CIs). In the analysis, Model 1 was the crude model, and Model 2 adjusted for potential confounders (age, BMI, marital status, food intake, smoking, nap frequency, and moderate-vigorous physical activity).
Results
Data from 680 participants were used for analysis using the AWGS algorithm, which was updated in 2019. Table 1 shows the characteristics of the study participants according to their daily alcohol consumption by sex. Among males, 411 individuals with a mean age of 60 years were included in our study. Of these, 218 (53.0%) and 94 (22.9%) participants were defined as light-to-moderate drinkers and heavy drinkers, respectively. The proportions of Chinese males who were current smokers and married were higher at higher levels of alcohol intake. The prevalence of low grip strength among heavy drinkers was approximately threefold higher than that among nondrinkers. Among females, 269 participants with a mean age of 58 years were included in the analysis. Of these, 117 (53.2%) and 9 (3.3%) participants were defined as light-to-moderate drinkers and heavy drinkers, respectively. The variables of age, educational level, and grip strength were quite different according to alcohol consumption levels (Table 1).
Table 2 presents the association between alcohol consumption patterns (three levels of volume of drinking and frequency) and the risk of sarcopenia and its elements among Chinese males and females. Among males, we found a positive association between alcohol consumption patterns and the risk of low muscle mass and low muscle strength. Those who consumed > 25 g of ethanol per day were approximately three times more likely to have low muscle mass (OR, 3.99; 95% CI, 1.10–17.05) or low grip strength (OR, 3.39; 95% CI, 1.33–9.92) than nondrinkers after adjustment for age, marital status, smoking, BMI, food intake, physical activity and nap frequency. Those who consumed alcohol more than 4 times per week were approximately threefold to fivefold more likely to have low muscle mass (OR, 4.99; 95% CI, 1.24–25.55) or low grip strength (OR, 3.37; 95% CI, 1.40–8.74) than nondrinkers after multiple adjustments. Unfortunately, we did not find a relationship between alcohol consumption patterns and sarcopenia or gait speed among males. Among females, because of the small number of drinkers, we combined the light-to-moderate drinker group and heavy drinker group. That is, there were two groups (never drinker and current drinker) for the analysis of alcohol consumption and drinking frequency. However, there was no separate relationship of alcohol consumption and sarcopenia or its elements with alcohol consumption and drinking frequency.
Discussions
In this cross-sectional study, we examined the association between alcohol consumption patterns and the prevalence of the risk of sarcopenia among Chinese males and females from Henan Province. We concluded that higher alcohol intake (including volume and frequency) was linked to a tendency toward a higher risk of low muscle mass and low muscle strength after multiple adjustments, but no relation was found between alcohol consumption patterns and sarcopenia or gait speed among males. In addition, the relationship between alcohol consumption patterns and sarcopenia or its elements was not observed among females.
Alcohol consumption is one of the leading causes of disease burden [26] In human studies, although the relationship between alcohol consumption and sarcopenia has been reported in the general population, related studies are still sparse, and their results are still controversial [12,13,14]. Among males, our findings showed that there was no relation between alcohol drinking patterns and sarcopenia or gait speed. However, we found that alcohol drinking patterns were positively associated with low muscle mass and low grip strength after multiple adjustments among males. Our findings were in line with previous studies that showed that high alcohol consumption was associated with a greater decline in the skeletal muscle index among older Brazilian people [27]. Moreover, a population-based prospective study showed a significant positive association between alcohol consumption and a decline in muscle strength, and this association did not change over the 2-year period among Japanese individuals [28]. The phenomenon of alcohol drinking patterns and a decline in muscle strength and the skeletal muscle index is known as “chronic alcoholic myopathy” [29], which manifests as a decrease in muscle mass and a reduced cross-sectional area for type II fiber-rich muscle [30, 31]. There have been many reports on the underlying molecular mechanism responsible for alcoholic myopathy. Studies have indicated that long-term alcohol consumption results in a protracted imbalance in protein homeostasis by impairing translation initiation in muscle by altering the activities of several eukaryotic initiation factors [32] or reducing protein/DNA ratios, a fact associated with lower myofibrillary Ca2-ATPase activity [33]. Moreover, alcohol intake induces defects in the insulin signal transduction pathway as a decreased ability of maximal stimulating doses of insulin growth factor (IGF)-1 to upregulate muscle protein synthesis [34]. Skeletal myopathy is worthy of attention because it may occur in as many as one-third of high alcohol consumers and may lead to a significant loss of muscle strength and function [35]. Poor muscle strength has also been associated with a high prevalence of chronic diseases [36] and a higher risk of mortality in older populations [37]. Although alcohol consumption is not known as a direct cause of sarcopenia, studies demonstrating the adverse effects of alcohol on muscle mass suggest that chronic alcohol consumption may promote the loss of muscle mass and strength. Therefore, reducing alcohol consumption may serve as a strategy for the prevention of the decline in muscle mass and muscle strength.
We found that the association between alcohol drinking patterns and sarcopenia or its elements was different for males and females. Several explanations may account for a possible interaction between sex and alcohol consumption patterns in this study. The number of cases was substantially lower among females than among males. In addition, the volume and frequency of alcohol consumption among Chinese women was quite low, with a mean of 1.1 g of ethanol daily for quantity and a mean of 0.44 times per week for frequency, whereas it was 17.3 g and 2.41 times per week among men, respectively. We cannot exclude the possibility that this result is related to low alcohol consumption. Finally, differences in alcohol pharmacokinetics [38] and beverage preferences between sexes may be another explanation. One article stated that a preference for a specific type of alcoholic beverage (wine or other) was considered when such a drink accounted for more than 80% of alcohol intake [39]. The preferred beverage was wine among females, which may be more beneficial than drinking beer or spirits [40], whereas liquor was favored by the males in this study. However, the results for women are less certain and warrant further study.
This study had several strengths and limitations. First, this was the first study to explore the association between alcohol consumption and sarcopenia in the general Chinese population. Additionally, sarcopenia was defined according to the updated standard criteria in 2019. An important strength was the definition of alcohol, which was divided into groups according to the dietary guidelines for Chinese residents, which provides a sound basis for drinking guidelines for the Chinese population.
Among the main limitations was that alcohol consumption was self-reported, so there may be recall error and social desirability bias. In addition, this study regarding alcohol intake and sarcopenia failed to investigate the dose‒response relationship. Moreover, considering the small sample size, we have not analysed by different age group. It is an urgent need to continue to collect samples and to further explore the relationship between alcohol consumption and sarcopenia at different age and gender level. Finally, our study was a cross-sectional study, and a causal relationship between alcohol consumption and sarcopenia or its elements should be investigated in a follow-up study.
Conclusion
These data showed heavy alcohol consumption and frequent drinking was associated with an increased risk of low muscle mass and muscle strength in Chinese men from Henan province. . Efforts to reduce alcohol consumption and drinking frequency among males in China should be pursued as part of comprehensive lifestyle modification approaches for the prevention and treatment of low muscle mass and muscle strength.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Waters DL, Baumgartner RN, Garry PJ, et al. Advantages of dietary, exercise-related, and therapeutic interventions to prevent and treat sarcopenia in adult patients: An update [J]. Clin Interv Aging. 2010;7(5):259–70.
Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: Revised european consensus on definition and diagnosis [J]. Age Ageing. 2019;48(1):16–31.
Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment [J]. J Am Med Dir Assoc. 2020;21(3):300–7 e302.
Cruz-Jentoft AJ, Landi F, Schneider SM, et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the international sarcopenia initiative (ewgsop and iwgs) [J]. Age Ageing. 2014;43(6):748–59.
WHO. Global status report on alcohol and health. Geneva:World health organization; 2014.
Li YR, Wang J, Zhao LY, et al. [the drinking status and associated factors in adults in china] [J]. Zhonghua Liu Xing Bing Xue Za Zhi. 2018;39(7):898–903.
Tang YL, Xiang XJ, Wang XY, et al. Alcohol and alcohol-related harm in china: Policy changes needed [J]. Bull World Health Organ. 2013;91(4):270–6.
Rom O, Kaisari S, Aizenbud D, et al. Lifestyle and sarcopenia-etiology, prevention, and treatment [J]. Rambam Maimonides Med J. 2012;3(4):e0024.
Steiner JL, Kimball SR, Lang CH. Acute alcohol-induced decrease in muscle protein synthesis in female mice is redd-1 and mtor-independent [J]. Alcohol Alcohol. 2016;51(3):242–50.
Lang CH, Frost RA, Svanberg E, et al. Igf-i/igfbp-3 ameliorates alterations in protein synthesis, eif4e availability, and myostatin in alcohol-fed rats [J]. Am J Physiol Endocrinol Metab. 2004;286(6):E916–26.
Lang CH, Pruznak AM, Nystrom GJ, et al. Alcohol-induced decrease in muscle protein synthesis associated with increased binding of mtor and raptor: Comparable effects in young and mature rats [J]. Nutr Metab (Lond). 2009;6(4):1–17.
Kwon YJ, Lim HJ, Lee YJ, et al. Associations between high-risk alcohol consumption and sarcopenia among postmenopausal women [J]. Menopause. 2017;24(9):1022–7.
Yoo JI, Ha YC, Lee YK, et al. High prevalence of sarcopenia among binge drinking elderly women: A nationwide population-based study [J]. BMC Geriatr. 2017;17(1):114.
Steffl M, Bohannon RW, Petr M, et al. Alcohol consumption as a risk factor for sarcopenia - a meta-analysis [J]. BMC Geriatr. 2016;11(16):99.
Alexandre Tda S, Duarte YA, Santos JL, et al. Prevalence and associated factors of sarcopenia among elderly in brazil: Findings from the sabe study [J]. J Nutr Health Aging. 2014;18(3):284–90.
Park S, Ham JO, Lee BK. A positive association of vitamin d deficiency and sarcopenia in 50 year old women, but not men [J]. Clin Nutr. 2014;33(5):900–5.
Lau EM, Lynn HS, Woo JW, et al. Prevalence of and risk factors for sarcopenia in elderly chinese men and women [J]. J Gerontol A Biol Sci Med Sci. 2005;60(2):213–6.
Han P, Kang L, Guo Q, et al. Prevalence and factors associated with sarcopenia in suburb-dwelling older chinese using the asian working group for sarcopenia definition [J]. J Gerontol A Biol Sci Med Sci. 2016;71(4):529–35.
Liu X, Hao Q, Yue J, et al. Sarcopenia, obesity and sarcopenia obesity in comparison: Prevalence, metabolic profile, and key differences: Results from wchat study [J]. J Nutr Health Aging. 2020;24(4):429–37.
Liu X, Hou L, Xia X, et al. Prevalence of sarcopenia in multi ethnics adults and the association with cognitive impairment: Findings from west-china health and aging trend study [J]. BMC Geriatr. 2020;20(1):63.
Shaper AG. Alcohol and mortality: A review of prospective studies [J]. Br J Addict. 1990;85(7):837–47. discussion 849–861.
Y YX, XC MH. P. China food composition [M]. 2nd. Beijing: Peking University Medical Press; 2009.
Huang S, Li J, Shearer GC, et al. Longitudinal study of alcohol consumption and hdl concentrations: A community-based study [J]. Am J Clin Nutr. 2017;105(4):905–12.
Society CN. Dietary guidelines for chinese residents(2016) [M]. Beijing: People’s Medical Publishing House; 2016.
Qu NN, Li KJ. [study on the reliability and validity of international physical activity questionnaire (chinese vision, ipaq)] [J]. Zhonghua Liu Xing Bing Xue Za Zhi. 2004;25(3):265–8.
Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010 [J]. Lancet. 2012;380(9859):2224–60.
Coelho MPP, Diniz KGD, Bering T, et al. Skeletal muscle mass index and phase angle are decreased in individuals with dependence on alcohol and other substances [J]. Nutrition, 2020,71(110614.
Cui Y, Huang C, Momma H, et al. The longitudinal association between alcohol consumption and muscle strength: A population-based prospective study [J]. J Musculoskelet Neuronal Interact. 2019;19(3):294–9.
Preedy VR, Adachi J, Ueno Y, et al. Alcoholic skeletal muscle myopathy: Definitions, features, contribution of neuropathy, impact and diagnosis [J]. Eur J Neurol. 2001;8(6):677–87.
Freilich R, Kirsner R, Whelan G, et al. Quantitative measure of muscle strength and size in chronic alcoholism: An early indication of tissue damage [J]. Drug Alcohol Rev. 1996;15(3):277–87.
Hanid A, Slavin G, Mair W, et al. Fibre type changes in striated muscle of alcoholics [J]. J Clin Pathol. 1981;34(9):991–5.
Lang CH, Wu D, Frost RA, et al. Inhibition of muscle protein synthesis by alcohol is associated with modulation of eif2b and eif4e [J]. Am J Physiol. 1999;277(2):E268–76.
Martin FC, Slavin G, Levi AJ, et al. Investigation of the organelle pathology of skeletal muscle in chronic alcoholism [J]. J Clin Pathol. 1984;37(4):448–54.
Hong-Brown LQ, Frost RA, Lang CH. Alcohol impairs protein synthesis and degradation in cultured skeletal muscle cells [J]. Alcohol Clin Exp Res. 2001;25(9):1373–82.
Vernet M, Cadefau JA, Balagué A, et al. Effect of chronic alcoholism on human muscle glycogen and glucose metabolism [J]. Alcohol Clin Exp Res. 1995;19(5):1295–9.
Häkkinen A, Hannonen P, Häkkinen K. Muscle strength in healthy people and in patients suffering from recent-onset inflammatory arthritis [J]. Br J Rheumatol. 1995;34(4):355–60.
Ruiz JR, Sui X, Lobelo F, et al. Association between muscular strength and mortality in men: Prospective cohort study [J]. BMJ. 2008;337(7661):a439.
Mumenthaler MS, Taylor JL, O’Hara R, et al. Gender differences in moderate drinking effects [J]. Alcohol Res Health. 1999;23(1):55–64.
Valencia-Martín JL, Galán I, Rodríguez-Artalejo F. The association between alcohol consumption patterns and adherence to food consumption guidelines [J]. Alcohol Clin Exp Res. 2011;35(11):2075–81.
Grønbaek M, Becker U, Johansen D, et al. Type of alcohol consumed and mortality from all causes, coronary heart disease, and cancer [J]. Ann Intern Med. 2000;133(6):411–9.
Acknowledgements
We thank the participants for their willingness to participate in this study. Our special thanks go to Yafei Sun and Xiumei Xu for their assistance with the collection and input of the data.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All authors had full access to all of the data and take responsibility for the integrity of the data and the accuracy of the data analysis. Baihui Ma, Lijun Guo, and Yongxia Kong acquired the data. Junya Zhai, Baihui Ma, and Rui Liang analyzed and interpreted the data. Junya Zhai, Baihui Ma, and Pipasha Khatun drafted the manuscript, which was critically revised for important intellectual content by all authors. Quanjun Lyu, Jin Qin and Minghua Cong were responsible for the statistical analysis and revised the manuscript. Junya Zhai supervised the study and is a guarantor.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines laid out in the Declaration of Helsinki, and all procedures involving research study participants were approved by the First Affiliated Hospital of Zhengzhou University (Protocol 2020–KY-066). Written informed consent was obtained from all participants. Verbal consent was witnessed and formally recorded.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhai, J., Ma, B., Qin, J. et al. Alcohol consumption patterns and the risk of sarcopenia: a population-based cross-sectional study among chinese women and men from Henan province. BMC Public Health 22, 1894 (2022). https://doi.org/10.1186/s12889-022-14275-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14275-6