
Abstract
Background
To assess the interaction of sleep duration and depression on the risk of cardiovascular disease (CVD).
Methods
A total of 13,488 eligible participants were enrolled in this retrospective cohort study eventually. Baseline characteristics were extracted from the China Health and Retirement Longitudinal Study (CHARLS) database, including age, sex, diabetes, high-density lipoprotein (HDL), blood glucose (GLU), glycosylated hemoglobin (GHB) etc. Univariate and multivariate negative binomial regression models were carried out to assess the statistical correlation of sleep duration and depression on CVD separately. Additionally, multivariate negative binomial regression model was used to estimate the interaction of sleep duration and depression on CVD risk.
Results
After adjusting for age, sex, educational background, hypertension, diabetes, dyslipidemia, the use of hypnotics, disability, nap, drinking, deposit, sleep disturbance, HDL, triglyceride, total cholesterol, GLU and GHB, the risk of CVD in participants with the short sleep duration was increased in comparison with the normal sleep duration [relative risk (RR)=1.02, 95% confidence interval (CI):1.01-1.03]; compared to the participants with non-depression, participants suffered from depression had an increased risk of CVD (RR=1.05, 95%CI:1.04-1.06). Additionally, the result also suggested that the interaction between short sleep duration and depression on the risk of CVD was statistically significant in these patients with diabetes and was a multiplicative interaction.
Conclusion
An interaction between short sleep duration and depression in relation to an increased risk of CVD among Chinese middle-aged and elderly individuals was noticed, which may provide a reference that people with diabetes should focus on their sleep duration and the occurrence of depression, and coexisting short sleep duration and depression may expose them to a higher risk of CVD.
Similar content being viewed by others

Background
Cardiovascular disease (CVD), as a common chronic disease, is still the main cause of global mortality and disability [1, 2]. In recent years, the incidence of CVD has remained a steady rise globally, reaching 523 million in 2019 [2]. It is estimated that there was 17.9 million people died of CVD every year, accounting for 32% of global deaths [3], brought huge burden of disease for many families. As a consequence, it is very important for closely paying attention to risk factors to prevent the occurrence of CVD.
To date, several studies have reported that poor behavior and mental health are closely associated with the CVD risk, including short sleep duration, long sleep duration, and depression [4, 5]. A systematic review and meta-analysis showed that both short and long sleep duration were markers of cardiovascular outcomes, and were also associated with a higher risk of coronary heart disease (CHD) [6]. In addition, Yin, et al. also pointed out that there was a U‐shaped association between sleep duration and risk of CVD, and insufficient or excessive sleep duration were significantly related to an elevated risk of CVD [7]. Depression as a mental illness of low mood and loss of interest, has become increasingly common worldwide [8]. A growing body of scientific evidence have evaluated the role of depression in the development of CVD [8, 9]. In the study of Carney, et al., the result showed that depression was recognized as a highly prevalent risk factor for CHD occurrence [10]. The association mechanism of depression and CVD risk might be associated with the vascular endothelial dysfunction and increased platelet aggregation among patients with depression, thus accelerating the development of CVD [11]. Notably, there were some studies have showed a bidirectional relationship of sleep duration and depression [12, 13]; insufficient or excessive sleep duration could increase the risk of depression [12]. Simultaneously, people with depression could bring a short sleep duration [13]. Although short/long sleep duration and depression have been considered as risk factors for the development of CVD, people with combined short/long sleep duration and depression may represent a population with a higher risk of CVD due to a possible interaction of short/long sleep duration and depression. There were few studies, to our knowledge, have assessed the influence of the coexistence of short/long sleep duration and depression with regard to the CVD risk to date among middle-aged and elderly people.
Herein, in this study, we attempted to investigate the association between short/long sleep duration, depression and the risk of CVD based on the China Health and Retirement Longitudinal Study (CHARLS) database, and evaluate a joint effect of short/long sleep duration and depression on the CVD risk.
Methods
Data sources
All data in this retrospective cohort study were obtained from the CHARLS database [14], which is a nationally representative investigation of Chinese adults with 45 years or older. The investigation aimed at assessing the social, economic and health circumstances of residents. Respondents were followed every 2-3 years by conducting face-to-face computer-assisted personal interviews, physical measurements and blood tests. The baseline survey was carried out in 2011, with three follow-up surveys conducted in 2013, 2015, and 2018 [15, 16]. http://charls.pku.edu.cn/
Study eligibility criteria
Due to the high rate of lost follow-up for the included population of CHARLS database before 2015, in this retrospective cohort study, we chose the baseline data in the CHARLS database 2015, and follow-up data in 2018. Included criteria: participants had information about sleep duration and depression in the CHARLS database 2015 (n=14,962). Excluded criteria: participants already diagnosed with CVD before survey in 2015 (Fig. 1). All interviewees in CHARLS database needed to sign informed consent, and Biomedical Ethics Review Committee of Peking University approved the ethical review for the data collection in CHARLS database [14], thus according to the Ethics Review Committee of Guang’anmen Hospital, China Academy of Chinese Medical Sciences, secondary database analysis has been exempted from an ethical review.

Flow chart of participants. 4253 participants had missing data and were treated with multiple imputation
Data collection
Baseline variables and laboratory indicators were collected, including age (years), sex, educational background, marital status, deposit (CN¥), disability, exercise time (h/day), drinking, smoking, sleep time (h/day), depression, nap (min/day), chronic kidney disease (CKD), dyslipidemia, sleep disturbance, the use of hypnotics, diabetes, CVD, triglyceride (TG, mg/dl), high-density lipoprotein (HDL, mg/dl), low-density lipoprotein (LDL, mg/dl), systolic blood pressure (SBP, mmHg), diastolic blood pressure (DBP, mmHg), total cholesterol (TC, mg/dl), blood glucose (GLU, mg/dl), glycosylated hemoglobin (GHB, %).
Sleep duration was assessed by the respondents’ self-reported question which asked, “During the past month, how many hours of actual sleep did you get at night (average hours for one night)? This may be shorter than the number of hours you spend in bed.” The short, normal and long sleep duration were defined as <6 h, 6-8 h, >8 h, respectively [17]. Nap duration was measured by the following question “During the past month, how long did you take a nap after lunch on average?” (0 represent that respondent did not nap duration) [14]. Sleep disturbance was defined as how many days a week did participants have trouble falling asleep, frequently nighttime awakenings and earlier waking [18]: rarely or none of the time (<1 day), some or a little of the time (1-2 days), occasionally or a moderate amount of the time (3-4 days), and most or all of the time (5-7 days). The Epidemiological Studies Depression Scale (CES-D) was used to assess depression, which has been used to measure depression of the population [19]. The scale options consisted of 4 levels and were assigned: “rarely or none of the time=0”, “some or few times=1”, “occasionally or moderate number of times=2”, “most or all of the time=3”; The total score ranges from 0 to 30, with a scores ≥10 were defined as having depression [20]. Hypertension, CKD, dyslipidemia and diabetes was assessed by a self-report of physician's diagnosis: Have you been diagnosed with hypertension, CKD, dyslipidemia or diabetes by a doctor? Participants who answered “yes” to the question were defined as having hypertension, CKD, dyslipidemia or diabetes [21].
Outcomes
Outcome variable was defined as the occurrence of CVD in the present study. The CVD was assessed by the following questions: “Have you been told by a doctor that you have been diagnosed with a stroke” or “Have you been diagnosed with heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems?” Participants who answered “yes” to the question during the follow-up period were defined as having CVD [22].
Statistical analysis
The normality test of measurement data was conducted by Shapiro-Wilk, normal distribution data was exhibited as mean ± standard deviation (Mean ± SD), and comparison between groups adopted independent sample t-test and ANOVA was used for comparison between multiple groups. Non-normal data were described in terms of
median and interquartile range [M (Q1, Q3)], and the comparison between groups was performed by Mann-Whitney U test and Kruskal-Wallis H test was used for comparison between multiple groups. The enumeration data were expressed as number of cases and composition ratio n (%), Chi-square or Fisher's exact test was used for comparison between two groups.
We adopted the univariate negative binomial regression model to explore the possible covariates that were associated with CVD. Then, multivariate negative binomial regression model was carried out to assess the statistical correlation of sleep duration and depression on CVD separately. Three models were used in this study. Model 1 was regarded as unadjusted; Model 2 adjusted several covariates that were performed for statistically significant in univariate analysis and had an impact on CVD in the literature, including age, sex, educational background, marital status, exercise time, chronic kidney disease, hypertension, diabetes, dyslipidemia, the use of hypnotics, disability, nap, drinking and deposit; Model 3 adjusted age, sex, educational background, marital status, exercise time, chronic kidney disease, hypertension, diabetes, dyslipidemia, the use of hypnotics, disability, nap, drinking, deposit, sleep disturbance, HDL, TC, TG, GLU and GHB. Additionally, we used the multivariate negative binomial regression models to evaluate the joint effect of sleep duration and depression on the CVD risk in different populations. Relative risk (RR) with 95% confidence interval (CI) was reported. With respect to missing data of the variables, we adopted multiple interpolation method. The data were interpolated for five times, and five datasets were generated. In the five datasets, the mean of the data with five times interpolations was taken for measurement data, and the mode of the data interpolated for five times was taken for enumeration data. A new interpolated dataset was obtained for subsequent analysis. Sensitivity analysis of missing data before and after interpolation was shown in Supplemental Table 1. Smoking data was missing too much and not participated in the analysis. We used the SAS (version 9.4, SAS institute., Cary, NC, USA) software for the statistical analysis and R (version 4. 0. 3, Mice package) for the multiple interpolation. Statistical tests were performed by using bilateral tests. P<0.05 was regarded as statistically significant.
Results
Baseline characteristics
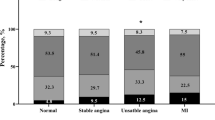
After excluded some participants who were diagnosed with CVD before survey (n=329), and we also excluded 1,145 participants did not record whether CVD occurred at the end of the follow-up. A total of 13,488 eligible participants were enrolled in this retrospective cohort study eventually, with an average follow-up time of 2.7 years. There are 1,563 (11.59%) incident cases of CVD identified at the follow-up period to 2018. All participants’ characteristics were shown in Table 1. The study subjects’ average age was 57.89 ± 9.87 years. Furthermore, 3,772 (27.97%) participants had short sleep duration and 1,231 (9.13%) had long sleep duration, 4,091 (30.33%) had depression. It is worth noting that the population proportion of CVD occurrence among short sleep duration was higher than normal and long sleep duration groups, and the CVD occurred more frequently in the depression group than the non-depression group. Detailed baseline information was given in Table 1.
Effect of sleep duration/ depression on CVD
Some possible variables that were associated with CVD were shown in Table 2 (P<0.05) by univariate negative binomial regression model. The effects on CVD of sleep duration were presented in the Table 3. Model 1 (RR=1.03, 95%CI:1.02-1.04) showed that the risk of CVD in the short sleep duration group was increased in comparison with the normal sleep duration group, with similar results in Model 2 (RR=1.02, 95%CI:1.01-1.03) and Model 3 (RR=1.02, 95%CI:1.01-1.03). While the results of Model 1, Model 2 and Model 3 demonstrated that there was no significant difference between long sleep duration group and CVD (P>0.05).
As presented in Table 3, the results of three models indicated the effects of depression on the risk of CVD. Compared with non-depression group, depression group had a 0.06-fold (Model 1: RR=1.06, 95%CI:1.05-1.07), 0.05-fold (Model 2: RR=1.05, 95%CI:1.04-1.06), and 0.05-fold (Model 3: RR=1.05, 95%CI:1.04-1.06) increased risk of CVD.
The interaction between short sleep duration and depression on CVD in different populations
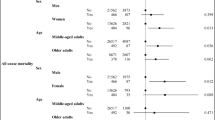
After incorporating short sleep duration, depression and the interaction term of short sleep duration and depression into multifactor negative binomial regression model, we found that the interaction between short sleep duration and depression on CVD was statistically significant in these patients with diabetes and was a multiplicative interaction (P<0.05, Table 4). However, with respect to the relationship between short sleep duration and depression on CVD for total population or hypertension population, no an interaction was observed (P>0.05, Table 4).
Discussion
In this analysis of 13,488 participants from CHARLS database, we revealed that short sleep duration and depression were independent risk factors for CVD occurrence; Importantly, we found that there might be an interaction between short sleep duration and depression in relation to an increased risk of CVD among middle-aged and elderly patients with diabetes.
For the present study, after adjusted covariates, the risk of CVD in people with independent short sleep duration and depression was 0.02 times and 0.05 times than those with normal sleep duration and without depression, respectively. There was no doubt that our result showed that short sleep duration and depression were associated with the increased risk of CVD, which were mostly in line with prior researches [9, 23,24,25]. Short sleep duration was associated with an increased levels of markers of inflammation, [26]. When short sleep duration triggered mild inflammation, leading to an increased stress response in the hypothalamic-pituitary-adrenal axis, which may cause the rise of blood pressure and an increased risk of CVD [26]. Not only that, short sleep duration could induce biological effects including the changes in neural autonomic control and coagulation responses, an elevated level of oxidative stress, and accelerated atherosclerosis, triggering metabolic disorders to raise the risk of CVD [25]. Likewise, the associated mechanisms of depression and CVD might be related to endothelial dysfunction, autonomic nerve dysfunction, inflammation and life behavior [27, 28]. To our knowledge, some studies also reported a link between long sleep duration and increased risk of CVD among elderly people, which might be associated with arterial stiffness, blood pressure variability, gluco-regulatory function and systemic inflammation [29, 30]. However, our study showed that there was no statistically difference between long sleep duration group and CVD risk among Chinese middle-aged and elderly individuals [31], and the reason may be due to the difference of sample size. Simultaneously, we also found that there were 9.13% Chinese middle-aged and elderly individuals with long sleep duration, and more studies are still warranted on this relationship of long sleep duration and CVD risk in the future.
For the present study, the interaction between short sleep duration and depression on CVD risk for total population was not observed. However, we found that the interaction between short sleep duration and depression might be associated with an increased risk of CVD for middle-aged and elderly patients with diabetes. In other words, when patients with diabetes suffered from both of symptom of short sleep duration and depression, there was a higher risk of CVD. Nowadays, diabetes has been considered as one of the most common chronic conditions, and its prevalence are increasing worldwide [32]. Previous studies have suggested that people with diabetes appear to be at greater risk of depression [32,33,34]. In addition, some studies have shown that people with both diabetes and depression could suffer poorer outcomes, such as poorer quality of life, poorer self-management of diabetes and poorer medical outcomes [35, 36], which also suggested an importance of paying attention to the prognosis of patients with diabetes and depression. Additionally, insufficient sleep duration was also highly prevalent in patients with diabetes [37], which may contribute to a poor prognosis in those patients. In our study, coexisting short sleep duration and depression may increase the risk of CVD in middle-aged and elderly patients with diabetes. Accordingly, this finding may support the viewpoint that, patients with diabetes should pay attention to their sleep duration and the occurrence of depression. Appropriate increase of sleep duration and physical activities, a healthy diet and psychological treatment may beneficial to prevent the risk of CVD in middle-aged and elderly patients with diabetes [38, 39]. Although we found an interaction between depression and sleep duration on the risk of CVD in middle-aged and elderly patients with diabetes, more prospective studies are needed in the future to validate our results and explore the possible mechanism.
The strengths of our study included a large sample size, make the findings more convincing; and the results also may provide a reference that with respect to patients with diabetes, they should pay more attention to both the sleep time and the occurrence of depression, to decrease the risk of CVD. There are limitations that cannot be ignored. Firstly, the issue whether eligible patients diagnosed as short/long sleep duration or depression have been treated not considered in the present study, which may not be got from CHARLS database. Secondly, the coexistence duration of short sleep duration and depression may influence risk of CVD, there was no information collected from CHARLS database about the duration of both short sleep duration and depression, and more trials still are needed to confirm this association. Thirdly, CVD was defined as outcome variable, contained heart attack, coronary heart disease, angina pectoris, congestive heart failure or other heart problems and stroke, but we don’t know is that the synergistic interaction between short sleep duration and depression increase the higher risk for what kind of diseases. Fourthly, smoking has long been considered an important risk factor for CVD [40]. But, in this study, the variable (smoking) was missing so much that we excluded it. This is a limitation of our study. Lastly, short observational period for observation the incidence of CVD needs to be noted in this study, and more prospective studies with long follow-up periods need to be conducted in the future to verify our results.
Conclusion
In short, we found an interaction between depression and short sleep duration on the risk of CVD among middle-aged and elderly patients with diabetes. Patients with diabetes should pay more rigorous attention to their sleep duration and the occurrence of depression, and coexisting short sleep duration and depression may expose them to a higher risk of CVD. However, more researches are needed to confirm this association in the future.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available in the CHARLS repository, http://charls.pku.edu.cn/.
Abbreviations
- CVD:
-
Cardiovascular disease
- CHARLS:
-
China Health and Retirement Longitudinal Study
- TG:
-
Triglyceride
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- TC:
-
Total cholesterol
- GLU:
-
Glucose
- GHB:
-
Glycosylated hemoglobin
- CES-D:
-
Epidemiological Studies Depression Scale
- Mean ± SD:
-
Mean ± standard deviation
- M (Q1, Q3):
-
Median and interquartile range
References
Mensah GA, Roth GA, Fuster V. The global burden of cardiovascular diseases and risk factors: 2020 and beyond. J Am Coll Cardiol. 2019;74(20):2529–32.
Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021.
Flora GD, Nayak MK. A brief review of cardiovascular diseases, associated risk factors and current treatment regimes. Curr Pharm Des. 2019;25(38):4063–84.
Covassin N, Singh P. Sleep duration and cardiovascular disease risk: epidemiologic and experimental evidence. Sleep Med Clin. 2016;11(1):81–9.
Tobaldini E, Costantino G, Solbiati M, Cogliati C, Kara T, Nobili L, et al. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci Biobehav Rev. 2017;74(Pt B):321–9.
Cappuccio FP, Cooper D, D’Elia L, Strazzullo P, Miller MA. Sleep duration predicts cardiovascular outcomes: a systematic review and meta-analysis of prospective studies. Eur Heart J. 2011;32(12):1484–92.
Yin J, Jin X, Shan Z, Li S, Huang H, Li P, et al. Relationship of sleep duration with all-cause mortality and cardiovascular events: a systematic review and dose-response meta-analysis of prospective cohort studies. J Am Heart Assoc. 2017;6(9):e005947.
Almeida OP, Ford AH, Hankey GJ, Golledge J, Yeap BB, Flicker L. Depression, antidepressants and the risk of cardiovascular events and death in older men. Maturitas. 2019;128:4–9.
Macchi C, Favero C, Ceresa A, Vigna L, Conti DM, Pesatori AC, et al. Depression and cardiovascular risk-association among Beck Depression Inventory, PCSK9 levels and insulin resistance. Cardiovasc Diabetol. 2020;19(1):187.
Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. 2017;14(3):145–55.
Meng R, Yu C, Liu N, He M, Lv J, Guo Y, et al. Association of depression with all-cause and cardiovascular disease mortality among adults in China. JAMA Netw Open. 2020;3(2):e1921043.
Dong L, Xie Y, Zou X. Association between sleep duration and depression in US adults: a cross-sectional study. J Affect Disord. 2022;296:183–8.
Ouyang P, Sun W. Depression and sleep duration: findings from middle-aged and elderly people in China. Public Health. 2019;166:148–54.
Fu J, Zhang X, Moore JB, Wang B, Li R. Midday nap duration and hypertension among middle-aged and older Chinese adults: a nationwide retrospective cohort study. Int J Environ Res Public Health. 2021;18(7):3680.
Cai X, Qiu S, Liu S, Lu Y, Luo D, Li R, et al. Body-weight fluctuation and risk of diabetes in older adults: the China Health and Retirement Longitudinal Study (CHARLS). Diabetes Res Clin Pract. 2020;169:108419.
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43(1):61–8.
Lou P, Chen P, Zhang L, Zhang P, Chang G, Zhang N, et al. Interaction of sleep quality and sleep duration on impaired fasting glucose: a population-based cross-sectional survey in China. BMJ Open. 2014;4(3):e004436.
Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: A review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–32.
Smarr KL, Keefer AL. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire-9 (PHQ-9). Arthritis Care Res (Hoboken). 2011;63(Suppl 11):S454–66.
Luo H, Li J, Zhang Q, Cao P, Ren X, Fang A, et al. Obesity and the onset of depressive symptoms among middle-aged and older adults in China: evidence from the CHARLS. BMC Public Health. 2018;18(1):909.
Fan ZY, Yang Y, Zhang CH, Yin RY, Tang L, Zhang F. Prevalence and patterns of comorbidity among middle-aged and elderly people in China: a cross-sectional study based on CHARLS data. Int J Gen Med. 2021;14:1449–55.
Shi Z, Tuomilehto J, Kronfeld-Schor N, Alberti GK, Stern N, El-Osta A, et al. The circadian syndrome predicts cardiovascular disease better than metabolic syndrome in Chinese adults. J Intern Med. 2021;289(6):851–60.
Itani O, Jike M, Watanabe N, Kaneita Y. Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression. Sleep Med. 2017;32:246–56.
Irwin MR, Opp MR. Sleep health: reciprocal regulation of sleep and innate immunity. Neuropsychopharmacology. 2017;42(1):129–55.
Tobaldini E, Fiorelli EM, Solbiati M, Costantino G, Nobili L, Montano N. Short sleep duration and cardiometabolic risk: from pathophysiology to clinical evidence. Nat Rev Cardiol. 2019;16(4):213–24.
Ruparelia N, Chai JT, Fisher EA, Choudhury RP. Inflammatory processes in cardiovascular disease: a route to targeted therapies. Nat Rev Cardiol. 2017;14(3):133–44.
Li H, Zheng D, Li Z, Wu Z, Feng W, Cao X, et al. Association of Depressive Symptoms With Incident Cardiovascular Diseases in Middle-Aged and Older Chinese Adults. JAMA Netw Open. 2019;2(12):e1916591.
Vaccarino V, Badimon L, Bremner JD, Cenko E, Cubedo J, Dorobantu M, et al. Depression and coronary heart disease: 2018 position paper of the ESC working group on coronary pathophysiology and microcirculation. Eur Heart J. 2020;41(17):1687–96.
Matsubayashi H, Nagai M, Dote K, Turana Y, Siddique S, Chia YC, et al. Long sleep duration and cardiovascular disease: associations with arterial stiffness and blood pressure variability. J Clin Hypertens (Greenwich). 2021;23(3):496–503.
Full KM, Malhotra A, Gallo LC, et al. Accelerometer-Measured Sleep Duration and Clinical Cardiovascular Risk Factor Scores in Older Women. J Gerontol A Biol Sci Med Sci. 2020;75(9):1771–8.
Wang YX, Zhang L, Li CJ, Qi X, Fan YQ, He JS, et al. Predicted 10-year cardiovascular disease risk and its association with sleep duration among adults in Beijing-Tianjin-Hebei Region. China Biomed Environ Sci. 2021;34(10):803–13.
Tabbalat A, Dargham S, Al Suwaidi J, Aboulsoud S, Al Jerdi S, Abi KC. Mortality and socio-economic outcomes among patients hospitalized for stroke and diabetes in the US: a recent analysis from the National Inpatient Sample. Sci Rep. 2021;11(1):8204.
Sartorius N. Depression and diabetes. Dialogues Clin Neurosci. 2018;20(1):47–52.
Jiang CH, Zhu F, Qin TT. Relationships between chronic diseases and depression among middle-aged and elderly people in china: a prospective study from CHARLS. Curr Med Sci. 2020;40(5):858–70.
Gonzalez JS, Peyrot M, McCarl LA, Collins EM, Serpa L, Mimiaga MJ, Safren SA. Depression and diabetes treatment nonadherence: a meta-analysis. Diabetes Care. 2008;31(12):2398–403.
Zurita-Cruz JN, Manuel-Apolinar L, Arellano-Flores ML, Gutierrez-Gonzalez A, Najera-Ahumada AG, Cisneros-González N. Health and quality of life outcomes impairment of quality of life in type 2 diabetes mellitus: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1):94.
Lin L, Lu C, Chen W, Guo VY. Daytime napping and nighttime sleep duration with incident diabetes mellitus: a cohort study in Chinese older adults. Int J Environ Res Public Health. 2021;18(9):5012.
Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. 2019;107:525–39.
Cuijpers P, Quero S, Dowrick C, Arroll B. Psychological treatment of depression in primary care: recent developments. Curr Psychiatry Rep. 2019;21(12):129.
Kondo T, Nakano Y, Adachi S, Murohara T. Effects of tobacco smoking on cardiovascular disease. Circ J. 2019;83(10):1980–5.
Acknowledgements
Not applicable.
Funding
This study was supported by the Scientific and Technological Innovation Foundation of China Academy of Chinese Medicine Sciences (No. CI2021A04306) and Beijing Natural Science Foundation (No. 7222315).
Author information
Authors and Affiliations
Contributions
BJ, HZ and HY designed the study. BJ and HZ wrote the manuscript. FS and GW collected, analyzed and interpreted the data. HY critically reviewed, edited and approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research analyzed de-identified information downloaded from CHARLS database, which is exempt from Institutional Review Board approval of Guang’anmen Hospital, China Academy of Chinese Medical Sciences. All methods were carried out in accordance with relevant guidelines and regulations. Written Informed Consent was obtained from all subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplemental Table 1. Sensitivity analysis of missing data before and after interpolation.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jin, B., Zhang, H., Song, F. et al. Interaction of sleep duration and depression on cardiovascular disease: a retrospective cohort study. BMC Public Health 22, 1752 (2022). https://doi.org/10.1186/s12889-022-14143-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-14143-3