
Abstract
Background
Childhood obesity has become a significant public health issue worldwide. Socioeconomic status is among its key determinants. This study examined the socioeconomic inequality in different phenotypes of childhood obesity at the national level in Iran.
Methods
This national, multistage school cross-sectional study was undertaken in 2015 on 14,400 students aged 7–18 years from urban and rural areas of 30 provinces of Iran. Using principal component analysis, socioeconomic status (SES) was categorized into tertiles. SES inequality in different phenotypes of obesity (i.e., generalized obesity", "abdominal obesity", and combined obesity) was estimated using the concentration index. The determinants of this inequality were assessed by the Blinder-Oaxaca decomposition method.
Results
Overall, 14,274 students completed the study (response rate: 99%). The mean age was 12.28 years, 50.6% were boys, and 71.42% lived in urban areas. The prevalence of generalized obesity and abdominal obesity was 20.8% and 11.3%, respectively. The concentration index for different phenotypes of obesity was positive, indicating that inequality is more common amongst the low SES groups. High SES, being male, living in a rural, and having a positive family history of obesity were associated with general obesity. Moderate physical activity and living in a rural area were associated with abdominal obesity. In addition, living in a rural area, having a high SES, being male, and having a positive family history of obesity were associated with combined obesity.
Conclusion
According to the present study findings, all childhood obesity phenotypes were more prevalent in Iranian children with high SES. Therefore, due to obesity and other diseases, it is essential to implement environmental changes in addition to designing macro-educational programs and prevention strategies.
Similar content being viewed by others


Background
The increasing prevalence of childhood obesity (generalized and abdominal) has become a health concern worldwide in recent years. The rapidly rising obesity prevalence in children can lead to adult morbidity and mortality. Nonetheless, its prevalence has doubled in many countries since the 1980s [1].
Childhood obesity prevalence varies by country; for example, in Iran, 18%, Jordan 4%-8%, America, 11%-19% of children and adolescents aged 5–19 years, and in Spain, 37%-39% of children aged 6–11 years are overweight or obese [2,3,4].
The increasing risk of various associated co-morbidities with obesity, such as adulthood obesity, diabetes, and non-communicable diseases, has been confirmed in previous studies, implementing the importance of its prevention and control [2,3,4,5].
Nevertheless, managing childhood obesity remains a challenge and may relate to targeting adipose tissue. Thus, body mass index (BMI) could help assess the amount of fat [5]. However, individuals with obesity have heterogeneous phenotypes, each associated with various health conditions. Metabolically unhealthy obesity (MUO) defines subjects at high risk of metabolic diseases, and metabolically healthy obesity (MHO) refers to individuals with obesitythat are at a low risk of developing cardiometabolic disorders. Compared with MUO individuals, MHOs have more abdominal fat but less visceral fat mass and fat collection in their liver and skeletal muscles [6]. Additionally other types of obesity such as normal weight obesity (NWO) have been described. In this type of obesity, regardless of having a normal BMI, due to a high fat percentage, the individual is considered as obese; and is at increased risk of obesity related morbidity and mortality; however, since their BMI falls within the normal range, they may go undetected until obesity related morbidities appear [7]. Hence a thorough understanding of childhood obesity, BMI and their determinants is needed to fight this pandemic.
Some determinants affecting obesity are known as “social determinants”, which are a diverse range of social, economic and environmental factors that impact children's health. Therefore, to prevent childhood obesity, assessing their social determinants of health is essential [2, 8]; and although the associations between socioeconomic status (SES) and some growth disorders have been documented among the adult population, studies on children are limited and inconsistent. Therefore, recognizing these factors that impact and cause inequality regarding this subject is very important [8].
Inequality is one of the realities understood in people's lives as it affects people's lifestyles. This concept is generally defined according to individuals' different needs and conditions. Therefore, it is related to the states and characteristics of the recipients, not the particular service providers [9].
As there is limited evidence of inequalities amongst obesity phenotypes [10,11,12,13], this study aimed to determine the socioeconomic inequality in different phenotypes of childhood obesity and its determinants in Iran.
Methods
Study design
The present study analyzed the combined data from the fifth national "Childhood and Adolescence Surveillance and PreventIon of Adult Noncommunicable Diseases (CASPIAN-V) Study. It was conducted in 2015 in urban and rural areas of 30 provinces of Iran. The detailed methodology has already been published [14].
Participants
In this school-based national survey, 14,400 students, 7–18 years, were selected using multistage, stratified cluster sampling from urban and rural areas of 30 provinces of Iran in 2015. Students were sampled in each province according to their place of residence (urban or rural) and education level (elementary or high school) using probability proportional to size sampling with an equal male/female ratio. Clusters were determined at the school level. In each sampling unit, ten students alongside their parents were included. The sample size included 480 students in each province (48 clusters of 10 students).
Data collection
The following variables were assessed:
-
i)
Demographic information: age, sex, place of residence, family characteristics such as the family history of obesity, and parental level of education.
Some complementary data on possessing a family private car and type of home (private/rental), some complementary information on screen time, physical activity, and other lifestyle habits were also obtained.
-
ii)
Socio-economic status (SES):
Family SES was calculated according to the previously approved standard method in the Progress in the International Reading Literacy (PIRLS) study [15]. Principal component analysis (PCA) determined the variables and summarized them in one principal component SES. (parents' education, parents' job, possessing a private car, school type (public/private), type of home (private/rental), and having a personal computer at home); next, SES was categorized into tertiles, in which the first tertile was the lowest SES and the third tile the highest.
-
iii)
Screen time (ST):
ST was considered the sum of the average daily hours spent watching TV or movies, leisure time using a personal computer (PC), or playing electronic games (EG). ST was asked separately for weekdays and weekends. ST was categorized into two groups: less than two hours per day (low) and two hours or more per day (high) according to the international ST recommendations [16].
-
iv)
Physical activity (PA):
Two questions assessed PA: "1) during the past week, how many days were you physically active for over 30 min? (Response options: from zero to seven days); and 2) How much time do you spend in an exercise class at school per week? (Response options: from zero to three or more hours) ". A frequency of fewer than two times per week was considered as low; two to four times a week as moderate, and more than four times a week as high.
Measurements
Anthropometric measurement and definitions
Standardized methods were used to assess BMI [14]. Waist circumference was measured using a non-elastic tape at a point midway between the lower border of the rib cage and the iliac crest at the end of normal expiration to the nearest 0.1 cm. Generalized obesity (GO) was defined according to the WHO growth curve as BMI > 95th for age-sex specific percentile [17], and abdominal obesity (AO) was designated as waist to height ratio (WHtR) > 0.5 [18]. Students were classified into four different phenotypes of obesity in terms of AO and GO: normal (5th < BMI < 85th percentile and WHtR < 0.5), only AO (WHtR > 0.5 and BMI < 95th percentile), only GO (BMI > 95th and WHtR < 0.5), combined obesity (CO) (BMI > 95th and WHtR > 0.5).
Statistical analysis
Data were analyzed using STATA package version 14.0 (Stata Statistical Software: Release 14. Stata Corp LP. Package, College Station, TX, USA), and a P-value < 0.05 was considered statistically significant.
Continuous data were presented as means (SD). The Prevalence of combinations of obesity was reported with 95% confidence intervals (CI). Univariate and multivariate logistic regression analysis assessed the association of independent variables with excess weight. The logistic regression analysis results are presented as OR (95% CI).
Although there are several methods to assess inequality in health outcomes, methods that assess inequality are not numerous. The Blinder-Oaxaca decomposition method is a well-known inequality assessment method for inequality determinants [9]. This method will divide the prevalence of the first and fifth quintile of obesity into two components. The explained or endowment component arises because of differences in the groups' characteristics, such as differences in a region or family size. An unexplained or coefficient component is attributed to different influences of these characteristics in each group [9]. In this study, using the Blinder-Oaxaca decomposition method, we assessed inequality and determinants of inequality in different phenotypes of obesity. In this method, SES inequality in different phenotypes of obesity was estimated by calculating the prevalence of different phenotypes of obesity across SES tertiles, the concentration index (C Index) [19].
C Index was estimated using the following equation, where “hi” is the value of obesity for the person “i”, “Ri” is the relative rank of person “i" in the SES variable distribution, and µ is the mean value of obesity
Negative and positive C Index values indicate that inequality is high and low in favor of the SES group, respectively [20].
The analysis of the obesity gap between the tertiles of SES was assessed using the Blinder-Oaxaca decomposition method [20]. in this method, two regression models fitted separately for the two population groups (in this study, upper and lower economic groups):
where “Y” is the outcome, “β” is the coefficient including interception, “X” is an explanatory variable, and “ε” is an error. The distance between the two groups is calculated as:s
and
This technique splits the gap between the mean values of a result into two components. The described component or endowment arises due to differences in the characteristics of the groups, such as differences in the area or family size. An unexplained part or coefficient is attributed to the different effects of these characteristics in each group [20].
A logistic regression model with independent variables was run for assessing decomposition in each economic group to determine the regression coefficients (β) as the main effect and their interaction with other independent variables.
This method assessed the gap decomposition in different phenotypes of obesity between SES's first and third tiles. In this study, we considered some demographic and lifestyle-related variables as determinants of different phenotypes of obesity.
Moreover, two logistic regression models (crude and adjusted) were used to assess the association of independent variables with different types of obesity. The adjusted model assessed all independent variables with the “Enter method”. To deal with the clustering effect, all analysis was performed using the”survey analysis method”.
Results
From the 14,400 invited subjects, 14,274 students participated and completed the study (response rate: 99%). The mean (SD) age was 12.28 (3.15) years; 50.6% were boys, and 71.42% lived in urban areas.
The distribution of general characteristics of students according to gender is presented in Table 1. The frequency of high PA among boys was significantly higher than in girls (p < 0.001). However, the association of ST, SES, family history of obesity, and residential area with gender was not statistically significant.
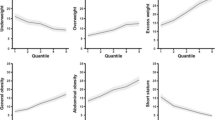
The prevalence of AO and GO was 20.8% and 11.3%, respectively. Figure 1 shows the prevalence of different phenotypes of obesity according to SES.

The prevalence of different phenotypes of obesity according to SES
Estimated values of “C Index” in this figure for different phenotypes of obesity were positive, indicating inequality was in favour of low SES groups.
Crude and adjusted association of independent variables with different phenotypes of obesity are presented in Table 2. In the adjusted model, by increasing age, the odds of "only GO" decreased significantly (OR: 0.91, 95% CI: 0.87–0.95). Moreover, having a positive family history of obesity was associated with "only GO" (OR: 1.26, 95% CI: 1.01–1.58).
In the multivariate model, living in rural areas decreased the odds of "only AO" (OR: 0.78, 95% CI: 0.64–0.95).
In the adjusted model, students with high SES (T2: OR: 1.22 95% CI:1.03–1.45, T3:OR: 1.26 95% CI: 1.07–1.49), being male (OR: 1.30 95% CI:1.09–1.56), living in rural areas (OR: 0.49 95% CI:0.40–0.60), and positive family history of obesity (OR: 1.38 95% CI:1.17–1.64) was associated with "GO". Moderate physical activity (OR: 1.12 95% CI: 1.03–1.22) increased, and living in a rural area (OR: 0.62 95% CI: 0.53–0.74) decreased the odds of "AO". In addition, living in rural areas (OR: 0.41, 95% CI: 0.33–0.51), high SES (OR: 1.28, 95% CI: 1.06–1.55), being male (OR: 1.30, 95% CI: 1.06–1.59) and positive family history of obesity (OR: 1.40, 95% CI: 1.14–1.71) was associated with combined obesity in the adjusted model.
Table 3 shows that the gap between the low and high SES groups for the prevalence of combination obesity (GO –AO) and GO was 3.26%, and 3.27%, respectively, but generalized (β: -0.63, CI:-1.47, 0.21) and abdominal obesity (β: 0.57, CI:-2.17, 1.03) were not significant. In the explained component, place of residence significantly contributed to the gap between the two SES groups for the prevalence of combined obesity. For general obesity, place of residence and family history of obesity were the effective variables responsible for the gap.
Discussion
This study shows that the prevalence of obesity is higher in groups with high SES. This finding is consistent with previous studies [10, 3, 21].
Socioeconomic inequality in the health of children and adolescents is one of the most critical health concerns in any country [22]. Studies show that developed countries witness a weakening of the positive relationship between obesity and SES, and a gradual increase in their negative relationship [23]. However, developing countries like Iran report that the prevalence of childhood obesity is associated with high levels of socioeconomic inequality [21].
The epidemiological transition in low and middle-income countries (LMICs), where energy-dense foods are readily available at relatively low prices, is high [24, 25]. In Iran, increasing access to high-calorie foods and a sedentary lifestyle are the two major causes of obesity [21].
Georgina Gómez et al. found that SES matches the quality and variety of food [26]. A multilevel study on childhood determinants of obesity (2019) reported family income and the amount of child allowance was related to obesity and weight gain [27].
In many Asian cultures, obesity in children is a sign of their health in affluent families [28], and this belief can explain the prevalence of obesity in families with favourable socioeconomic status. SES has been raised as a fundamental determinant of adult health, although confirmation of this relationship in children requires further studies [29].
Our findings show that the prevalence of AO and GO were 20.8% and 11.3%, respectively, consistent with previous Iranian studies. For example, in a survey in northwestern Iran, the prevalence of GO and AO was 26.6% and 43.4%, respectively [30]. In Azerbaijan, the prevalence of GO and AO was 24% and 76.4%, respectively [31]. These results confirmed that AO in Iranian children and adolescents is more prevalent than GO.
According to the present findings, gender is a risk factor for combined obesity (AO, GO) and GO, such that the risk of this phenotype of obesity in boys is higher than in girls. Moreover, previous studies expressed the relationship between GO and AO with gender [21, 32]. Similarly, in a study of obesity trends in Chinese children between 2011 and 2015, obesity was higher among boys compared to girls [33]. However, in some studies, the results were different, and obesity was higher among girls compared to boys [34].
These differences can be attributed to cultural differences that attended to boys more than girls. For example, the prevalence of obesity and overweight in Iranian families is more common due to increased attention to boys [35]. Other causes of gender differences in obesity phenotypes include differences in lifestyle, socio-individual characteristics, and genetic and behavioural characteristics. However, in the present study, no significant relationship was observed between “only AO” and “only GO” with gender; no other studies have investigated their prevalence. This finding expresses the need to address obesity phenotypes as a cumulative indicator to expand the obesity pattern by adding and combining its phenotypes [36].
According to the results of the Oaxaca model, the highest proportion of differences between rich and poor groups regarded the living area, pertaining that urbanization was associated with a high prevalence of obesity phenotypes. Environmental factors such as place of residence and socioeconomic level, influenced children and adolescents' food consumption patterns and eating habits.
Differences in urban and rural food cultures are leading causes of these inequalities. Using traditional foods and living a more active life than ready-made and sedentary foods increases inequalities in obesity phenotypes [37].
The human–environment relationship is complex and requires a comprehensive method to create transformational change in health; because the environment directly or indirectly affects occupant behaviour; evidence suggests that with the proper lifestyle changes of improved nutritional intake and increased physical activity, obesity is a preventable disease [38]; thus indicating the importance of preventive measures.
Strengths and limitations
The present study is the first to compare different phenotypes of childhood obesity based on socioeconomic levels by the Blinder-Oaxaca decomposition model. This model shows the proportion of each determinant in creating inequality [29].
Furthermore, our large sample size, using standard protocols and a validated questionnaire, is another strength of the present study; However, since it is cross-sectional, it can not express the causal relationship between the variables, which is one of the limitations of the recent research. In addition, in this study, we didn't assess Fat mass, which is another limitation. Therefore, prospective studies in this field are recommended.
Conclusion
According to the present study findings, all childhood obesity phenotypes were more prevalent in Iranian children with high SES. Therefore, due to obesity and other diseases, it is essential to implement environmental changes in addition to designing macro-educational programs and prevention strategies.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Klingelhöfer D, Braun M, Quarcoo D, Brüggmann D, Groneberg DA. Epidemiological Influences and Requirements of Global Childhood Obesity Research. Obes Facts. 2021;14(4):382–96.
Jenabi E, Khazaei S. Trends in obesity among iranian children and adolescents: 2000–2016. J Tehran Univ Heart Cent. 2020;15(1):41.
de Bont J, Díaz Y, Casas M, García-Gil M, Vrijheid M, Duarte-Salles T. Time trends and sociodemographic factors associated with overweight and obesity in children and adolescents in Spain. JAMA network open. 2020;3(3):e201171-e.
Al-Rahamneh H. The Prevalence of Obesity, Overweight, and Thinness among Jordanian Children and Adolescents. J Exerc Physiol Online. 2020;23(2):95–108.
Lebiedowska A, Hartman-Petrycka M, Błońska-Fajfrowska B. How reliable is BMI? Bioimpedance analysis of body composition in underweight, normal weight, overweight, and obese women. Ir J Med Sci (1971-). 2021;190(3):993–8.
Qorbani M, Khashayar P, Rastad H, Ejtahed H-S, Shahrestanaki E, Seif E, et al. Association of dietary behaviors, biochemical, and lifestyle factors with metabolic phenotypes of obesity in children and adolescents. Diabetol Metab Syndr. 2020;12(1):1–7.
Khonsari NM, Khashayar P, Shahrestanaki E, Kelishadi R, Nami SM, Heidari-Beni M, Abdar ZE, Tabatabaei-Malazy O, Qorbani M. Normal Weight Obesity and Cardiometabolic Risk Factors: A Systematic Review and Meta-Analysis. Front Endocrinol. 2022;13.
Viner R, Hargreaves D, Varnes L, Heys M. The social determinants of young people's health. Health. 2018.
Rahimi E, Hashemi Nazari SS. A detailed explanation and graphical representation of the Blinder-Oaxaca decomposition method with its application in health inequalities. Emerg Themes Epidemiol. 2021;18(1):1–15.
Djalalinia S, Kelishadi R, Qorbani M, Sheidaei A, Emamian MH, Motlagh ME, et al. Decomposition of socioeconomic inequality in growth disorders to its determinants in pediatric population: the CASPIAN IV study. J Diabetes Metab 2021:1–10.
Hoebel J, Kuntz B, Kroll LE, Schienkiewitz A, Finger JD, Lange C, et al. Socioeconomic inequalities in the rise of adult obesity: a time-trend analysis of national examination data from Germany, 1990–2011. Obes Facts. 2019;12(3):344–56.
Heshmat R, Hemati Z, Payab M, Hamzeh SS, Motlagh ME, Shafiee G, et al. Prevalence of different metabolic phenotypes of obesity in Iranian children and adolescents: the CASPIAN V study. J Diabetes Metab Disord. 2018;17(2):211–21.
Payab M, Qorbani M, Shahbal N, Motlagh ME, Hasani-Ranjbar S, Zahedi H, et al. Association of Anthropometric Indices With Metabolic Phenotypes of Obesity in Children and Adolescents: The CASPIAN-V Study. Front Endocrinol. 2019;10:786.
Motlagh ME, Ziaodini H, Qorbani M, Taheri M, Aminaei T, Goodarzi A, et al. Methodology and early findings of the fifth survey of childhood and adolescence surveillance and prevention of adult non-communicable disease: the CASPIAN-V study. Int J Prev Med. 2017;8.
Martin MO, Mullis IV, Kennedy AM. Progress in International Reading Literacy Study (PIRLS): PIRLS 2006 Technical Report. International Association for the Evaluation of Educational Achievement. 2007.
Hovsepian S, Qorbani M, Asadi M, Hatami M, Motlagh ME, Mahdavi-Gorabi A, et al. Socioeconomic Inequalities in Quality of Life in Iranian Children and Adolescents: The Weight Disorder Survey of the CASPIAN-IV Study. J Res Health Sci. 2019;19(3):e00451.
Group WMGRS, de Onis M. WHO Child Growth Standards based on length/height, weight and age. Acta paediatrica. 2006;95:76–85.
Ejtahed HS, Kelishadi R, Qorbani M, Motlagh ME, Hasani-Ranjbar S, Angoorani P, et al. Utility of waist circumference-to-height ratio as a screening tool for generalized and central obesity among Iranian children and adolescents: The CASPIAN-V study. Pediatr Diabetes. 2019;20(5):530–7.
Shafiee G, Qorbani M, Heshmat R, Mohammadi F, Sheidaei A, Motlagh ME, et al. Socioeconomic inequality in cardio-metabolic risk factors in a nationally representative sample of Iranian adolescents using an Oaxaca-Blinder decomposition method: the CASPIAN-III study. J Diabetes Metab Disord. 2019;18(1):145–53.
Singleton CR, Affuso O, Sen B. Decomposing racial disparities in obesity prevalence: variations in retail food environment. Am J Prev Med. 2016;50(3):365–72.
Kelishadi R, Qorbani M, Heshmat R, Djalalinia S, Sheidaei A, Safiri S, et al. Socioeconomic inequality in childhood obesity and its determinants: a Blinder-Oaxaca decomposition. J Pediatr (Rio J). 2018;94(2):131–9.
Homs C, Berruezo P, Según G, Estrada L, de Bont J, Riera-Romaní J, et al. Family-based intervention to prevent childhood obesity among school-age children of low socioeconomic status: study protocol of the FIVALIN project. BMC Pediatr. 2021;21(1):1–14.
Wang Y, Pan L, Wan S, Yi H, Yang F, He H, et al. Association of socioeconomic status and overweight/obesity in rural-to-urban migrants: different effects by age at arrival. Front Public Health. 2020;8: 622941.
Venturelli F, Ferrari F, Broccoli S, Bonvicini L, Mancuso P, Bargellini A, et al. The effect of Public Health/Pediatric Obesity interventions on socioeconomic inequalities in childhood obesity: A scoping review. Obes Rev. 2019;20(12):1720–39.
Misra A, Jayawardena R, Anoop S. Obesity in South Asia: phenotype, morbidities, and mitigation. Curr Obes Rep. 2019;8(1):43–52.
Gómez G, Kovalskys I, Leme ACB, Quesada D, Rigotti A, Cortés Sanabria LY, et al. Socioeconomic Status Impact on Diet Quality and Body Mass Index in Eight Latin American Countries: ELANS Study Results. Nutrients. 2021;13(7):2404.
Wijayanti D, Salimo H, Dewi YLR. Multilevel Analysis on the Determinants of overweight and obesity among primary school students in Boyolali, Central Java. J Matern Child Health. 2019;4(5):294–301.
Wali N, Agho KE, Renzaho AM. Factors associated with stunting among children under 5 years in five South Asian countries (2014–2018): Analysis of demographic health surveys. Nutrients. 2020;12(12):3875.
Mosha MV, Msuya SE, Kasagama E, Ayieko P, Todd J, Filteau S. Prevalence and correlates of overweight and obesity among primary school children in Kilimanjaro, Tanzania. PLoS ONE. 2021;16(4): e0249595.
Tutunchi H, Jafarabadi MA, Hoojeghani S, Tabrizi S, Farrin N, Payahoo L, et al. General and abdominal obesity is related to socioeconomic status and food choices: a cross-sectional study. Food Sci Nutr. 2019.
Tabrizi JS, Sadeghi-Bazargani H, Farahbakhsh M, Nikniaz L, Nikniaz Z. Prevalence and associated factors of overweight or obesity and abdominal obesity in Iranian population: a population-based study of northwestern Iran. Iran J Public Health. 2018;47(10):1583.
Djalalinia S, Kelishadi R, Qorbani M, Peykari N, Kasaeian A, Nasli-Esfahani E, et al. A systematic review on the Prevalence of overweight and obesity, in iranian children and adolescents. Iran J Pediatr. 2016;26(3).
Zhang J, Wang H, Wang Z, Du W, Su C, Zhang J, et al. Prevalence and stabilizing trends in overweight and obesity among children and adolescents in China, 2011–2015. BMC Public Health. 2018;18(1):1–7.
Otitoola O, Oldewage-Theron W, Egal A. Prevalence of overweight and obesity among selected schoolchildren and adolescents in Cofimvaba, South Africa. South African Journal of Clinical Nutrition. 2021;34(3):97–102.
Moradi G, Mostafavi F, Azadi N, Esmaeilnasab N, Ghaderi E. Socioeconomic inequality in childhood obesity. J Res Med Sci. 2017;17(3):391.
Brandão I, Martins MJ, Monteiro R. Metabolically Healthy Obesity—Heterogeneity in Definitions and Unconventional Factors. Metabolites. 2020;10(2):48.
Moitra P, Madan J. Perceived barriers and facilitators of healthy eating and physical activity: focus groups with children, parents and teachers in Mumbai, India. Int J Community Med Public Heal. 2020;7(6):2363.
Funderburk L, Cardaci T, Fink A, Taylor K, Rohde J, Harris D. Healthy Behaviors through Behavioral Design-Obesity Prevention. Int J Environ Res Public Health. 2020;17(14):5049.
Acknowledgements
The authors would like to thank the executive team, research scientists and all relevant administrators of the CASPIAN project, Vice-Chancellor for Research, Alborz University of Medical Sciences, for their cooperation and foundation.
Funding
Vice-Chancellor for Research, Alborz university of Medical Sciences, funded this study. The funding source had no role in the writing, design, data collection or interpretation and submission of the manuscript. The authors were not precluded from accessing data in the study, and they accept responsibility for submitting and publication.
Author information
Authors and Affiliations
Contributions
ZM was involved in study design, project administration, drafting, writing and editing manuscript.PG was involved in study design, project administration, and writing and editing the manuscript.MQ was involved in study design, project administration, statistical analysis, and editing of the manuscript.A SH was involved in the statistical analysis and editing manuscript.RH was involved in project administration and editing the manuscript.M H and N MK were involved in project administration and editing the manuscript. R K and N MK were involved in project administration and editing the manuscript. All author(s) have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
informed consent was obtained from all participants, and if participants were under 18, informed consent was obtained from a parent and/or legal guardian as well.
Relevant guidelines and regulations were observed for all methods. The Ethics Committee of Alborz University of Medical Sciences approved all protocols (IR.ABZUMS.REC.1400.219).
All The methods of this study were carried out by relevant regulations and guidelines.
Consent to publication
Not applicable.
Competing of interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mahmoodi, Z., Gill, P., Qorbani, M. et al. Socioeconomic inequality in different phenotypes of childhood obesity and its determinants in Iran: a Blinder-Oaxaca decomposition method. BMC Public Health 22, 1580 (2022). https://doi.org/10.1186/s12889-022-13997-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-13997-x