
Abstract
Background
It has been documented that income is a strong determinant of dental care use in Canada, mostly due to the lack of public coverage for dental care. We assess the contributions of food insecurity and home ownership to income-related equity in dental care use and access. We add to the literature by adding these two variables among other socio-economic determinants of equity in dental care use and access to dental care. Evidence on equity in access to and use of dental care in Canada can inform policymaking.
Methods
We estimate income-related horizontal inequity indexes for the probability of 1) receiving at least one dental visit in the last 12 months; and 2) lack of dental visits during the 3 years before the interview. We conduct the analyses using data from the 2013–2014 Canadian Community Health Survey (CCHS) at the national and regional level.
Results
There is pro-rich inequity in the probability of visiting a dentist or an orthodontist and in access to dental care in Ontario. Inequities vary across jurisdictions. Housing tenure and food insecurity contribute importantly to both use of and access to dental care, adding information not captured by standard socio-economic determinants.
Conclusions
Redistributing income may not be enough to reduce inequities. Careful monitoring of equity in dental care is needed together with interventions targeting fragile groups not only in terms of income but also in improving house and food security.
Similar content being viewed by others


Background
There is some evidence of socio-economic inequalities in oral health [1, 2]. Pro-rich socio-economic inequalities and income-related inequities in the utilization of some health care services in Canada, particularly dental care, have been documented [3,4,5,6,7,8,9,10]. Also, during and after the global financial crisis of 2008–9, food insecurity and housing problems have increased in Canada as well as in the US and Europe [11, 12]. There are good reasons to believe that food insecurity and home ownership may affect the extent of social inequalities and income-related inequity in dental care use in Canada. In this study, we propose to enrich the description of socio-economic status (SES) in assessing equity in access and utilization of dental care by adding these two measures of household economic and financial insecurity as non-need independent variables beside income. Annual income provides much information on what commodities a household can afford and, as a result, whether the household can afford dental care services without jeopardizing its other consumption. We posit that it does not, however, capture all relevant information, and we propose to enrich the description of SES by adding these two household characteristics. Food insecurity is a measure of how likely it is that a household cannot afford the required quantity and quality of food [11]. A general definition of household food insecurity is given by Anderson [13] and refers to having a limited or uncertain availability of nutritionally adequate and safe food, or to having to acquire foods in socially unacceptable ways. This is a measure of purchasing power, and we posit that purchasing power may vary across households with similar income levels, especially since the big recession of 2008. The second characteristic is home ownership: here, we hypothesize that two households with the same income may have different purchasing power and situations relative to uncertainty depending on whether they own their house, especially in Canadian urban centres where housing prices have increased dramatically [14, 15]. As a result, home ownership status may affect the affordability of dental care services, conditional on income, and we want to test this is the case. There is evidence for both Canada and the US that both food insecurity [16,17,18,19,20,21,22,23,24,25] and housing insecurity [26,27,28,29] have a negative impact on individual physical and mental health. Duncan and Bonner [30] for Canada find a detrimental effect of food insecurity on oral health. Access to healthy food is considered a factor that affects oral health [31, 32]. There is conflicting evidence on the link between food insecurity and health care use. Tarasuk et al. find an effect for Canada for ambulatory care [33] and for mental health care [25]. Kushel et al. [26] find an effect for the US and both ambulatory and emergency care. However, Bhargava and Lee [34] find no effect among the 50+ in Georgia, US. On dental care in particular, Allin et al. [5] find that, in Europe and the US, inequalities in dental care use are more pronounced across wealth than income quintiles. Muirhead et al. [35] show that food insecurity has a powerful impact on dental care use among Ontario working poor: 40% of those who are food insecure report seeing a dentist only when in pain, versus 18% of those who are food secure; 52% of those who are food insecure reported unmet dental care need, versus 24% of those who are food secure. Previous work on unmet needs for dental care in Canada found evidence that individuals with low income and without dental insurance coverage had the highest probability of reporting financial barriers to dental care and that reported unmet needs due to costs were associated with lower dental visit frequency and poorer oral health outcomes after controlling for the effects of income and insurance coverage [36]. However, the impact of both the lack of house ownership and food insecurity on income-related inequities in dental care use and unmet access to dental care has never been studied. We will add to the literature on income-related inequities by introducing these two variables among other socio-economic (non-need) determinants and by estimating their contribution on horizontal equity in dental care use. We will also add a rich set of controls describing chronic conditions, testing their role on dental care utilization. It has been shown for other countries like Italy that equity in the use of and unmet needs for health care services may vary not only by region [37] but also by type of chronic disease [38]. There is evidence for Canada that the use of health care services varies with the type of chronic conditions [4] and that being affected by diabetes tends to be associated with lower access to dental care [10].
However, evidence is needed on the role of food insecurity and home ownership in income-related inequities in access to dental care in Canada.
Data
The data used were from the 2013–2014 Canadian Community Health Survey (CCHS) annual component, conducted by Statistics Canada [39]. This is a large survey representative of the Canadian population and at the provincial level.
CCHS includes both a mandatory core set of questions that are completed by respondents in all provinces and a set of optional components completed at the discretion of individual provinces. We based our analysis on the full national sample with non-missing values on all the variables used and the adult population aged more than 17 years old. We firstly estimated models for the probability of using dental care by using CCHS data for all Canadian main regions. For our purposes, respondents living in Ontario (approximately one-third of the population) were asked questions on unmet need for dental care, which we used to study access to dental care for that province only and we estimated models for the probability of reporting unmet need for dental care with the richer set of independent variables on dental care that was only available for Ontario (dental care inclusion modules 1 and 2 of the CCHS). The details of the selection process of the datasets used are reported in additional online resources (Additional file 1).
Dependent variables
Our two dependent variables measured dental health care use and lack of access to dental care. The measure for dental care utilization was based on a standard question regarding whether individuals consulted a dentist, dental hygienist or orthodontist during the 12 months preceding the interview (consulting meaning either seen or talked to).Footnote 1 To study access, we used a question posed to respondents living in Ontario (and Northwest Territories) only, relative to not having visited a dentist over the past 3 years. Respondents who reported no visit in the past 3 years were classified as having unmet access to dental care, under the assumption that any individual should visit a dentist at least once every 3 years. We also used a more subjective variable in a sensitivity analysis: those who reported no visits in 3 years were asked the reason for this, and we created a variable of unmet access for financial reasons by giving a value of 1 to respondents stating the reason was due to costs. Last, we used a question posed to respondents in Ontario only to run a sensitivity analysis on our analysis of dental care use (first analysis): “It was reported earlier that you have ‘seen’ or ‘talked to’ a dentist in the past 12 months. Did you actually visit one?”, the variable on utilization in the past 12 months being restricted to those who had visited one.
Independent variables
Need variables
The need variables included age, gender, poor self-assessed health, poor self-assessed mental health, and low perceived life satisfaction. Following previous studies [38], we tested the inclusion of additional chronic health indicators, including a dummy set for the main chronic diseases reported by respondents (rheumatic diseases, cardiovascular, respiratory, diabetes, cancer, digestive diseases, back problems and scoliosis, anxiety, and other chronic diseases).Footnote 2 After this, we kept the only chronic condition variable that had a significant impact in all our models, having been diagnosed with diabetes. Unfortunately, information on oral health (a potential important determinant of the need for dental health care) was available only for respondents living in Ontario. We ran a sensitivity analysis on that sub-population, including information on oral health, and concluded that including it did not change the statistical significance or values of the other estimated effects. For analyses conducted on respondents from Ontario, we used the following variable for oral health: we constructed an index for oral health status by Cronbach’s alpha, pooling a set of 14 questions on oral health conditions.Footnote 3 We then used a variable which takes the value of 1 if the individual belongs to the lowest tertile of the distribution of this index, reporting a poor dental health status, and zero otherwise.
Non-need variables
We divided income by the square root of household size and then took the logarithm of this equalized income. Food insecurity (FI) is measured by Statistics Canada with an indicator on Household Food Insecurity Status, based on a set of 18 questions, and describes the food security situation of the household in the previous 12 months. It captures three kinds of situations: 1–Food secure: no sign of difficulty with income-related food access; 2–Moderately food insecure: sign of compromised quality and/or quantity of food consumed; 3–Severely food insecure: sign of reduced food intake and disrupted eating patterns. This variable is adopted from the Health Canada model of food security status. FI is measured in the US and in Canada with a standard questionnaire. We used data from the Group Food Security Module of the CCHS survey. This is based on the definition of FI as “The uncertainty and insufficiency of food availability and access that are limited by resource constraints, and the worry or anxiety and hunger that may result from it” (Wunderlich and Norwood, p.49) [40]. Those households classified as food secure did not report issues. Households classified as moderately food insecure had problems in the quality and/or quantity of food consumed among adults and/or children, whereas severely food insecure showed more extensive compromises, including reduced food intake among adults and/or children because of a lack of money for food (see Statistics Canada [39]; Tarasuk [20]).Footnote 4 We therefore used two dummy variables if the individuals lived respectively in a severely or moderately food insecure family, and zero otherwise. Housing status in the survey was captured by a question relative to house tenure status, where individuals were asked if they were living in a rented home or had home ownership. We used the dummy for home rented as a proxy for house insecurity, as opposed to house security with home ownership. There was no possibility to distinguish between those owning their home with or without debt. In our estimates we controlled for a set of further non-need variables such as marital status, immigrant status, race/ethnicity (aboriginal, non-white), smoking status (daily smoking), obesity, regular alcohol consumption, and living in rural areas. The provinces in which individuals live were collapsed into six regions, and a dummy variable for each one was created: (1) Atlantic, which includes Nova Scotia, New Brunswick, Prince Edward Island and Newfoundland-Labrador; (2) Quebec; (3) Prairies, which includes Alberta, Saskatchewan and Manitoba; (4) Territories, which includes Yukon, Northwest Territories and Nunavut; (5) British Columbia; and (6) Ontario.
We added one variable related to dental hygiene lifestyle. In the special module available only for Ontario, individuals were also asked their frequency of brushing teeth (“How often do you brush your teeth?”). We used a dummy variable that takes the value of 1 if this was at least twice a day, and zero otherwise. Last, we used another dummy, taking the value of 1 if individuals were covered by dental insurance, and zero otherwise. Our reference individual for the models on dental visits utilization was a white local citizen, married (or common-law) middle income and middle-aged (46–55 years) woman, living in Ontario, not actively working as employee or self-employed i.e. being either unemployed, housework, student, receiving social support or in other non-active conditions, with secondary education level, with at least a fair health/mental health/life satisfaction status, not affected by diabetes, not obese, neither currently smoking nor practicing heavy drinking, not physically active, not food insecure, not having to pay rent for a home, living in an urban area. For the models on unmet access to dental visits, the reference individual had the same characteristics as above and, in addition, had at least a fair or good oral health, no dental insurance, and did not brush her/his teeth at least twice a day. Descriptive statistics for the main dependent and independent variables used are shown in Table 1.
Methods
According to the principle of horizontal equity in health care, access should depend only on need, while socio-economic factors unrelated to need should not influence utilization [41]. We tested for income-related equity in health care use, applying the indirect standardization by regression method [41,42,43,44,45]. The horizontal inequity index (HI) is defined as the difference between income-related inequality in the observed health care use (CM) and income-related inequality in “need-expected” use (CN). The need-expected use is obtained by setting at their sample mean all non-need variables. The concentration index CM is positive (negative) whenever better-off individuals (worse-off) use dental care more than worse-off individuals (better-off). If the need distribution is favouring those who are worse off (better off), then we observe that the value of CN is negative (positive). There is no inequity in access to care when CM equals CN or the difference is not statistically significant. A positive (negative) value of the inequity implies inequity favouring those who are better off (worse off). Conversely, when the dependent variable measures unmet access to dental care, a negative (positive) value of HI implies inequity favouring those who are better off (worse off). An intuitive interpretation of the HI results can be obtained by multiplying HI by 75; for example, a HI value of 0.2 implies that equity can be achieved by redistributing 15% (0.2 × 75) of care from the rich to the poor [41]. For more details on the methodology see the additional resource (Additional file 2). In order to estimate CN, we estimated two set of logit models for: 1–the probability of having consulted a dentist or an orthodontist in the last 12 months in Canada; 2–the probability of having visited a dentist or an orthodontist in the last 12 months and of reporting lack of access to dental visits in the last 3 years in Ontario. The model for the lack of access to dental visits in Ontario was also estimated for the subset of individuals that indicated the main reason for not having visited a dentist in the last 3 years to be dental care costs. In all models we distinguished independent variables between need and non-need variables (Table 1). Non-need variables were set to their sample mean for obtaining CN [41, 45]. We estimated the income-related HI index for 1) the probability of using dental care services (all Canada and provinces) and 2) for the probability of unmet access to dental visits in the last 3 years (Ontario). All estimates were derived from weighted models using the population weights provided by Statistics Canada with the survey data. The estimated standard errors were based on the bootstrap method using weights provided by Statistics Canada.
Results
The proportion of Canadians visiting a dentist in 2013–2014 was approximately 67%; the proportion of those who reported they did not access a dental visit in the last 3 years—our measure for unmet access to dental care1—in Ontario and Northwest Territories was 16% (Table 1), and 14% in Ontario alone.Footnote 5 Of all individuals in Canada, 6% were living in food insecurity (4% moderate and 2% severe) (Table 1). Those living in a rented house were 27% of the total population, but this proportion more than doubles among the moderately food insecure (63%) and is almost three times higher among the severely food insecure (75%). Those who reported dental visits in the past 12 months were slightly less likely to be moderately (3.9%) or severely (1.6%) food insecure than the general population, and only 19% were tenants. These proportions were much higher among individuals reporting not having seen a dentist in the last 3 years in Ontario, of which approximately 17% were moderately (11%) or severely (6%) food insecure and 44% were tenants. Among those who reported unmet access, 30% were tenants and had food insecurity (either moderate or severe), i.e., five times the proportion of those who did not report problems in access (6%).
Overall, individuals who were better off were more likely to use dental care than the poor and less likely to report unmet access to dental visits during the 3 years preceding the interview. Tables 2 and 3 show the estimated odds ratios for all the logistic models. As expected, the probability of visiting a dentist or an orthodontist in Canada and of reporting problems in access to dental care is overall significantly associated with health care needs. With respect to the reference individual, being male, younger or elderly, being obese, and having diabetes are all factors associated with lower odds of use and higher odds of unmet access to dental care. Higher income is associated with higher odds of using dental care and conversely of unmet access to dental care, as high education and being employed. People with a high level of education and living in British Columbia were also more likely to access dental care. Ethnicity, marital status, and lifestyle all have associations with dental care access: being non-white or aboriginal, being a widow, being obese, smoking, and regular alcohol use are all associated with lower odds of using dental care. Engaging in regular physical exercise is associated with higher odds of visiting a dentist.
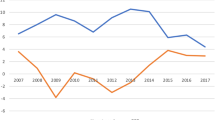
The results show that food insecurity is an important non-need factor of both equity in the use of and access to dental care. In particular, food insecurity is associated with lower odds of using dental care (Table 2) and higher odds of reporting lack of access to dental care (Table 3). Importantly, another component of financial insecurity related to housing, as measured by having to pay rent and not owning a house, is an important non-need factor in both horizontal equity in the use (Table 2) and unmet access to dental care (Table 3). Overall, the probability of visiting a dentist would be higher if people were not living in high food insecurity and/or owned their dwelling (Fig. 1). There is pro-rich inequity in the probability of visiting a dentist or an orthodontist (Table 2). Inequities vary across jurisdictions. Atlantic (HI = 0.14; P = 0.008; CI:0.000 0.129) and Quebec (HI = 0.13; P = 0.000; CI:0.113 0.148) show the highest inequity in the probability of dental care, Ontario (HI = 0.11; P = 0.000; CI:0.103 0.123) and the Territories (HI = 0.12; P = 0.000; CI = 0.071 0.152) are similar to the national average (HI = 0.11; P = 0.000; CI:0.105 0.117), whereas British Columbia (HI = 0.09; P = 0.000; CI: 0.077 0.11) and the Prairies (HI = 0.10; P = 0.000; CI: 0.076 0.108) show values below the national average (Fig. 2, Table 2). In comparison with previous articles based on data for the period 2000–2005, dental care is still distributed in favour of the richest [5, 7, 9]. We obtained almost identical results by using either the more general question, “Have you seen a dentist or orthodontist”, available at the national level for all regions, or the more specific question, “You reported that you have seen a dentist or orthodontist in the last 12 months: have you actually visited one?” (Table 3). This confirms the robustness of results obtained at the national and regional levels without the extended set of variables on dental care. There are high inequities in unmet access to dental visits in Ontario (HI = -0.39, P = 0.000, CI:-0.4276 0.3443); again, high food insecurity and housing insecurity appear autonomous non-need factors contributing to the probability of reporting problems in access to dental care (Table 3). Our results show that the HI for unmet access does not change substantially using the richer set of variables from the special modules variables on dental care inclusion in Ontario if the reason for unmet visits is due only to costs (HI-0.44, P = 0.000, CI: − 0.5209 0.3623) (Table 3). Estimates for Ontario show that high and moderate food insecurity are associated with higher odds of reporting unmet access to dental care and lower odds of using dental care. Differently from the countrywide estimates, the odds of high food insecurity are higher than the odds of moderate food insecurity for both use of and unmet access to dental care. Similar to the nationwide estimates, living in a rented house is associated with lower odds of using dental care and higher odds of having problems in access (Table 3).

Average marginal effect of high food insecurity and house rented on the probability of seeing a dentist or an orthodontist over samples of different income quantiles (quintile). Legend: Data source: CCHS 2013–2014

HI index estimation by Regions in Canada - Probability of having seen a dentist or an orthodontist in the last 12 months (estimates and their 95%confidence intervals). Legend: Data source: CCHS 2013–2014
Discussion
We can see from these results that not having food security and living in a rented house are associated with lower probability of using dental care, everything else being the same. These two variables also affect access to dental care in Ontario. Like in other countries such as Italy, we found that inequities in utilization are smaller than those in unmet access to dental care [37]. In the case of Ontario, inequities in access are three times higher than inequities in use of dental care. Estimates obtained by using the extended set of variables available for Ontario are similar to those obtained with the common set of variables available at the country level. This reinforces the results obtained with the core set of variables available nationwide. Our data are cross-sectional so we cannot infer causality. However, our evidence for Canada reinforces the view that reducing food insecurity in Europe and North America could counterbalance the negative effect of food insecurity on health care use [33, 46, 47]. Results are in line with previous evidence for Ontario showing that public spending on housing can offset the relationship between rising unemployment and food insecurity [47]. As a further test, we performed a decomposition analysis of the HI index for the probability of using dental care.Footnote 6 This confirmed the results that housing and food insecurity are relevant determinants, together accounting for the largest contribution after income on the HI index (see Additional file 3).Footnote 7
Conclusions
Estimates of the HI (horizontal inequity) index for the probability of using dental care show that, overall, inequities in dental care use in Canada are persisting. This work adds to the literature by also estimating inequities in unmet access to dental care in selected areas of Canada for which data were made available (Ontario and NW Territories). As expected, in these areas inequities in access are much higher than inequities in use. Therefore, it seems important for Canada to systematically report on indicators not only on the use of dental care but also on unmet access to dental care. The methodology applied aimed at describing the contribution of other non-need factors to horizontal inequity than the traditionally considered such as income, education etc. We newly showed that both food insecurity and home ownership are non-need factors contributing to income-related inequity in dental care access and use. This study is based on cross-sectional data, and therefore inference on causality is limited. We cannot interpret this as a causal relationship from food and housing insecurity to dental care use, as these two variables can be influenced by unobservable characteristics that can also affect dental care use. We could not fully explore the links among insurance coverage, food insecurity, and home ownership due to data limitations at the national level. Future work will be targeted at analysing in detail such links by allowing the confounders and mediators of the relationship between each of the covariates and dental services to vary. Moreover, further work is required to see if and how extended insurance coverage for dental care could at least partially offset the difficulty of living in food insecurity and without home ownership in terms of improving access to dental care. Despite its limitations, this study favours the argument that it is important to tackle the food and housing insecurity of households in order to reduce existing inequities in access to and use of dental care, thus improving the overall equity performance of Canada’s health care system. There is a need for interventions aiming at improving equity in access to dental care, such as increasing public dental care coverage for fragile groups. Our study suggests that redistributing income may not be enough to reduce inequities in dental care use and access to dental care. What matters is to also act on other dimensions of purchasing power, such as housing tenure status and food security.
Availability of data and materials
The data that support the findings of this study are available from Statistics Canada but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
All responsibility for using the data stems on the Authors.
Notes
We also considered the number of consultations to a dentist/orthodontist. However, as indicated by previous evidence for Canada, results from the estimation of count models showed that SES determinants were not as relevant, and they are not reported here.
For mapping chronic conditions, we used a set of dummy variables, taking the value of 1 if individuals replied positively when asked if they were affected by a set of chronic conditions (under the premise that they should have been diagnosed by a health professional) and that they expected the conditions to last or had already lasted 6 months or more, and zero otherwise.
The number of items for the index is 14, the average interim correlation is 0.1637, and the Cronbach’s alpha is 0.73.
The questions are ascending in the severity of circumstances in terms of FI. Individuals were firstly asked “Which of the following statements best describes the food eaten in your household in the past 12 months, that is, since [current month] of last year?”. They were then asked whether they or other individuals in the family exhibited these behaviours: worried that food would run out before household members had money to buy more; found that the food bought just didn’t last, and there was no money to get more; couldn’t afford to eat balanced meals; relied on only a few kinds of low-cost food to feed a child because they were running out of money to buy food; couldn’t feed a child a balanced meal because they couldn’t afford it; were not eating enough because they just couldn’t afford enough food; ever cut the size of meals, ate less than they felt necessary, skipped meals, were hungry but didn’t eat, personally lost weight, or did not eat for a whole day; and finally, reflecting the worst situation, whether they had had to cut the size of any child’s meals, any child had ever skipped meals, any child was ever hungry but they just couldn’t afford more food, or any child ever did not eat for a whole day because there wasn’t enough money for food. In order to determine household food security status, responses to each question were coded as either “affirmative” or “negative”. Depending on the question, they had to reply either yes or no, or that those circumstances were often true, sometimes true, or never true in the past 12 months. Responses were then grouped into the three categories of food secure, moderately food insecure, and highly food insecure.
Observations for the Northwest Territories were insufficient for a disaggregated analysis in our sample. Therefore, we reported results for Ontario. In Ontario, 71% reported that they visited a dentist during the last 12 months, 29% reported that the last time they visited a dentist was more than 1 year ago, 11% between 1 year and 2 years ago, 5.3% from 2 to 3 years ago, 3.5% from 3 to 4 years ago, 1.7% from 4 to 5 years ago, 7.2% 5 years or more ago, and 1.14% had never visited a dentist.
Estimates for Ontario and other provinces showed similar results; therefore, they are not reported.
We are aware that more advanced techniques for decomposition are available and could be applied. However, our primary concern here was to see whether these determinants affected the use of dental care. Future analyses will compare results from more advanced techniques of decomposition.
Abbreviations
- CCHS:
-
Canadian Community Health Survey
- FI:
-
Food Insecurity
- HI:
-
House dwelling status
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- SE:
-
Standard Errors
- SES:
-
Socio-economic status
References
Marmot M, Bell R. Social determinants and dental health. Adv Dent Res. 2011;23(2):201–6.
Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661–9 Epub 2005 Sep 30.
Van Doorslaer E, Masseria C. Income-related inequality in the use of medical care in 21 OECD countries: policy studies from the OECD Health Project. OECD. https://www.oecd.org/els/health-systems/31743034.pdf. Accessed 26 Nov 2020.
Asada Y, Kephart G. Equity in health services use and intensity of use in Canada. BMC Health Serv Res. 2007;7:1–12.
Allin S. Does equity in healthcare use vary across Canadian provinces? Healthc Policy. 2008;3(4):83–99.
Leake JL, Birch S. Public policy and the market for dental services. Community Dent Oral Epidemiol. 2008;34(4):287–95.
Grignon M, Hurley J, Wang L, Allin S. Inequity in a market-based health system: evidence from Canada’s dental sector. Health Policy. 2010;98(1):81–90.
Quinonez C, Grootendost P. Equity in dental care among Canadian households. Int J Equity Health. 2011. https://doi.org/10.1186/1475-9276-10-14.
Grignon M, Hurley J, Wang L. Income-related inequity in health and health care utilization in Canada, CHEPA (Centre for Health Economics and Policy Analysis) working paper series: McMaster University; 2015. p. 15–02. https://chepa.mcmaster.ca/docs/librariesprovider68/chepa-working-papers-2009-present/15-02-income-related-inequity-in-health-and-health-care-utilization-in-canada.pdf?sfvrsn=39490336_2. Accessed 22 Nov 2020
Zangiabadi S, Costanian C, Tamim H. Dental care use in Ontario: the Canadian community health survey (CCHS). BMC Oral Health. 2017;17:165.
Loopstra R, Reeves A, Mckee M. Food insecurity and social protection in Europe: quasi-natural experiment of Europe’s great recessions 2004–2012. Prev Med. 2016;89:44–50.
Tarasuk V, Mitchell A, Dachner N. Household food insecurity in Canada, 2014. Toronto: Research to identify policy options to reduce food insecurity. Proof-Food Insecurity Policy Research–Toronto; 2016. https://proof.utoronto.ca. Accessed 20 Nov 2020
Anderson SA. Core indicators of nutritional status for difficult-to-sample populations. J Nutr. 1990;120:62.
Bunting T, Walks AR, Filion R. The uneven geography of housing affordability stress in Canadian metropolitan areas. Hous Stud. 2004;19(3):361–93. https://doi.org/10.1080/0267303042000204287.
Moore E, Skabursskis A. Canada’s increasing housing affordability burdens. Hous Stud. 2003;19:395–413. https://doi.org/10.1080/0267303042000204296.
Korenman S, Miller JE, Sjaastad JE. Long-term poverty and child development in the United States: results from the NLSY. Children and Youth Services Review. Pergamon. 1995;17(1–2):127–55.
Vozoris NT, Tarasuk VS. Household food insufficiency is associated with poorer health. J Nutr. 2003;133(1):120–6.
Whitaker RC, Phillips SM, Orzol SM. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics. 2006. https://doi.org/10.1542/peds.2006-0239.
Tarasuk VS. Health implications of food insecurity. In: Dennis R, editor. Social determinants of health: Canadian perspectives. Toronto: Canadian Scholars’ Press Inc.; 2008. p. 205–20.
Tarasuk V. Implications of a basic income guarantee for household food. Ontario: Northern Policy Institute; 2017. https://www.northernpolicy.ca/upload/documents/publications/reports-new/tarasuk_big-and-food-insecurity-en.pdf. Accessed 14 Nov 2020
Seligman HK, Laraia B, Kushel MB. Food insecurity is associated with chronic disease among low-income NHANES participants. J Nutr. 2010;140(2):304–10.
Kaur J, Lamb MM, Ogden CL. The association between food insecurity and obesity in children—the National Health and Nutrition Examination Survey. J Acad Nutr Diet. 2015;115(5):751–8.
Lombe M, Nebbitt VE, Sinha A, Reynolds A. Examining effects of food insecurity and food choices on health outcomes in households in poverty. Soc Work Health Care. 2016;55(6):440–60.
Schure MB, Katon JG, Wong E, Liu CF. Food and housing insecurity and health status among U.S. adults with and without prior military service. SSM Popul Health. 2016;2:244–8.
Tarasuk V, Cheng J, Gundersen C, de Oliveira C, Kurdyak P. The relation between food insecurity and mental health care service utilization in Ontario. Can J Psychiatr. 2018;63(8):557–69.
Kushel MB, Gupta R, Gee L, Haas JS. Instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med. 2006;21(1):71–7.
Gibson M, Gibson M, Petticrew M, Bambra C, Sowden AJ, Wright KE, et al. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. 2011;17(1):175–84.
Thomson H, Thomas S. Developing empirically supported theories of change for housing investment and health. Soc Sci Med. 2015;124:205–14.
St-Germain AAF, Tarasuk V. High vulnerability to household food insecurity in a sample of Canadian renter households in government-subsidized housing. Can J Public Health. 2017;108(2):129–34.
Duncan L, Bonner AJ. Effects of income and dental insurance coverage on need for dental care in Canada. J Can Dent Assoc. 2014;80:e6.
Petersen PE, Kwan S. Equity, social determinants and public health programs—the case of oral health. Community Dent Oral Epidemiol. 2011;39:481–7.
Sisson KL. Theoretical explanations for social inequalities in oral health. Community Dent Oral Epidemiol. 2007. https://doi.org/10.1111/j.1600-0528.2007.00354.x.
Tarasuk V, Cheng J, de Oliveira C, Dachner N, Gundersen C, Kurdyak P. Association between household food insecurity and annual health care costs. CMAJ. 2015. https://doi.org/10.1503/cmaj.150234.
Bhargava V, Lee JS. Food insecurity and health care utilization among older adults. J Appl Gerontol. 2017. https://doi.org/10.1177/0733464815625835.
Muirhead V, Quinonez C, Figueiredo R, Locker D. Oral health disparities and food insecurity in working poor Canadians. Community Dent Oral Epidemiol. 2009. https://doi.org/10.1111/j.1600-0528.2009.00479.x.
Locker D, Maggirias J, Quinonez C. Income, dental insurance coverage, and financial barriers to dental care among Canadian adults. J Public Health Dent. 2011;71:4.
Giannoni M. Misurare la performance dei servizi sanitari in termini di equità di accesso e uso dei servizi sanitari nelle Regioni italiane (Measuring equity in access to health care in Italian Regions). In: Giannoni M, editor. Equità nell’accesso ai servizi sanitari, disuguaglianze di salute e immigrazione. La performance dei servizi sanitari. Milan: Franco Angeli; 2010. p. 106–35.
Masseria C, Giannoni M. Equity in access to health care in Italy: a disease-based approach. Eur J Pub Health. 2010. https://doi.org/10.1093/eurpub/ckq029.
Statistics Canada. CCHS 2013–2014 microdata and documentation. Ottawa: Statistics Canada; 2015.
Wunderlich GS, Norwood J, editors. Food insecurity and hunger in the United States: an assessment of the measure: The National Academies Press; 2006. https://doi.org/10.17226/11578.
O’Donnell O, van Doorslaer E, Wagstaff A, Lindelow M. Analyzing health equity using household survey data. Washington DC: The World Bank; 2008. https://doi.org/10.1596/978-0-8213-6933-3.
Kakwani N, Wagstaff A, van Doorslaer E. Socioeconomic inequalities in health: measurement, computation, and statistical inference. J Econ. 1997;77(1):87–103.
Wagstaff, A. and van Doorslaer, E. Equity in health care finance and delivery. In: Culyer AJ, Newhouse JP, editors. Handbook of health economics 1B: Elsevier Science; Amsterdam; 2000. p. 1803–61.
Wagstaff A, van Doorslaer E. Measuring and testing for inequity in the delivery of health care. J Hum Resour. 2000. https://doi.org/10.2307/146369.
van Doorslaer E, Jones AM. Income-related inequality in health and healthcare in the European Union. Health Econ. 2004;13:605–8.
Loopstra R, Reeves A, Stuckler D. Rising food insecurity in Europe. Lancet. 2015. https://doi.org/10.1016/s0140-6736(15)60983-7.
Loopstra R. Interventions to address household food insecurity in high-income countries. Proc Nutr Soc. 2018. https://doi.org/10.1017/s002966511800006x.
Acknowledgments
We are grateful to Statistics Canada for having granted access to the data.
Although the research and analysis are based on data from Statistics Canada, the opinions expressed in this paper do not represent the views of Statistics Canada.
The authors thank Professor Mike Veall (Director McMaster University-Statistics Canada Research Data Centre - RDC) and Dr. Peter Kitchen, Dr. Li Wang, Dr. Mustafa Ormek, Dr. Anna Kata for providing a supportive workplace and assistance on this project.
A special thanks from MGI goes to Professor Jean Eric Tarride (Director of CHEPA at McMaster University) and Prof. Holger Jens Schunemann (for hosting her as visiting Professor in 2018-2019 and Gioia Buckley (Research Associate at CHEPA) that supported her in all phases before and during visiting period at CHEPA.
MGI thanks the University of Perugia (Italy) that funded travel expenses to her period of visiting Professor at CHEPA.
Funding
This work has been partly funded by the University of Perugia (IT) that has covered travel expenses for MGI period of visiting Professor at McMaster University (CA) and by the PEHRG (Poverty and Equity in Health Research Group) Project at the University of Perugia sponsored by Umbria Region (Italy).
The usual disclaimer applies.
Author information
Authors and Affiliations
Contributions
MGI contributed to hypothesis conception and methodology definition, literature review, econometric and statistical analysis of the data and interpretation; manuscript drafting and write-up; MGR contributed to hypothesis conception and methodology definition, literature review, econometric and statistical analysis of the data, interpretation of the results, and critical review of the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Nothing to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Sample definition. Description of the sample used for the analysis.
Additional file 2.
Measuring horizontal inequity. Description of the methodology for measuring horizontal inequity.
Additional file 3.
Decomposition of the HI Index for the probability of having visited a dentist during the last 12 months – CANADA (*). File containing a figure showing results from the HI decomposition.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Giannoni, M., Grignon, M. Food insecurity, home ownership and income-related equity in dental care use and access: the case of Canada. BMC Public Health 22, 497 (2022). https://doi.org/10.1186/s12889-022-12760-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-12760-6