
Abstract
Background
This study aimed to investigate alcohol consumption and associated factors in middle-aged and older adults.
Materials and methods
We included 15,942 participants (7,384 men, 8558 women) with age range of 45-101 years from the 2011 baseline survey of the China Health and Retirement Longitudinal Study. Variables related to alcohol status and other potential risk factors were selected for analysis. Logistic regression analysis was used to analyze the factors associated with drinking.
Results
There was a significantly higher proportion of current drinkers among men than women (36.42% ± 0.86% vs. 3.73% ± 0.27%). Among the current drinkers, proportions of binge drinking, heavy drinking and daily drinking were 38.2, 53.0, 57.5% for men and 10.9, 37.2, 36.2% for women, respectively. Factors significantly associated with current drinking were age, health situation, smoking, geographic region, work status and social activities among men, and age, smoking, geographic region and work status among women. The favorite type of alcohol was spirits for both men and women. The type of beverage intake was also related socio- cultural-demographic factors as mentioned above.
Conclusions
Alcohol consumption behaviors and type of beverage was significantly influenced by socio- cultural-demographic factors. The socio-cultural-demographic factors affecting alcohol patterns should be further focused on to promote the development of alcohol control strategies.
Similar content being viewed by others

Introduction
Alcohol use disorders have been reported to be the most prevalent of all substance use disorders [1]. It was estimated that 992 million disability-adjusted life years (DALYs) and 4.2% of all DALYs were attributable to alcohol use in 2016 [1]. The burden attributable to alcohol was primarily from cirrhosis, transport injuries and cancer. It has also been suggested that the alcohol-attributable burden is highest in countries with either a low or middle–high socio-demographic index [1].
Alcohol drinking traditionally plays an important role in social activities in China. Drinking is considered to improve the atmosphere at festivals and ceremonies, and social drinking is encouraged as a way to build good relations in business [2]. Steady increases have been observed in alcohol production, availability and per capita consumption in China over recent decades because of rapid economic development and urbanization. These have led to increased levels of alcohol-related harm [3]. China faces an urgent need to implement a more rigorous alcohol policy to control the prevalence of alcohol-related problems [4].
Appropriate public health policies require understanding of which population groups are most affected by harmful alcohol use. In the last decades, several cross-sectional studies have explored the patterns of alcohol consumption in China. For example, Li et al. used data from the China Chronic Disease and Risk Factor Surveillance in 2007 to describe drinking patterns among Chinese residents aged 15–69 years [5]. However, they had no data on older people and insufficient information about alcohol-related risk factors. Lee et al. described alcohol consumption behaviors and alcohol dependence among older adults (aged 60 years and over) in China using the Chinese Longitudinal Healthy Longevity Survey (CLHLS) waves from 2000 to 2014 [6]. However, this study failed to explore the alcohol type and amount of alcohol consumed, and only reported the drinking status of older people. Using the 2010–2012 China National Nutrition and Health Survey, Li et al. explored drinking status and associated factors in adults aged 18 years and over and reported the rates of drinking, excessive drinking and harmful drinking [7]. However, it failed to explore drinking patterns. Considering the multi-dimensional characteristics of alcohol consumption measurement, researchers need to inspect covariation of quantity, frequency alcohol type and drinking pattern that contributes to causal inference between alcohol consumption and medical outcomes, and developing drinking guidelines.
To fill those gaps, we analyzed the data from the 2011 China Health and Retirement Longitudinal Study (CHARLS) baseline survey that included subjects aged ≥ 45 years and further simultaneously considered variables related to alcohol type, drinking frequency and volume, and drinking pattern to explore alcohol consumption status and examine the associations of potential risk factors with these behaviors.
Methods
Study sample and procedures
The CHARLS is an ongoing nationally representative longitudinal cohort study in China conducted by the National School of Development at Peking University. Residents aged 45 years and older and their spouses were interviewed at their homes, and data on socioeconomic and health status were collected using standardized questionnaires. A detailed description of the CHARLS has been published elsewhere [8]. Briefly, samples were selected using four stage stratified probability sampling. In the first stage, 150 counties within 28 provinces were randomly selected with a systematic sampling. In the second stage, probability-proportional-to-size sampling technique was used to choose 3 rural villages or urban communities (primary sampling units, PSUs) in each county. In the third stage, 80 households which contained residents aged ≥45 years were selected from each PSU using simple random sampling. In the final stage, one age-eligible person from the selected household were asked to participate in the survey. The baseline survey was conducted between June 2010 and March 2012. The respondents are followed every 2 years, and information collected through face-to-face computer-assisted personal interviews (CAPIs) with interviewers trained at Peking University by CHARLS staff members. Physical examinations were also carried out at the interviewees’ homes by trained interviewers. Information collected included demographic factors, socioeconomic status, and medical history.
In this study, we used the baseline survey, conducted between June 2011 and March 2012, which involved 17,708 respondents. We selected those aged 45 years and older. We removed anyone who had not provided full responses to the questions of interests, leaving data from 15,942 individuals (male: 7384; female: 8558) for analysis.
Measures
Alcohol consumption
In the baseline survey questionnaire, participants were asked how often they had drunk alcohol during the past year (never; less than once a month; ≥ once a month). Those who drank ≥ once a month in the last year were defined as ‘current drinkers’. Non-current drinkers were further asked if they had ever drunk alcoholic beverages in the past and how often (never; less than once a month; ≥ once a month). Those who never drank and had drank less than once a month in the past were considered as ‘abstainers’; those who previously drank ≥ once a month were defined as ‘former drinkers’; those who drank less than once a month in the last year and in the past were defined as ‘occasional drinkers’.
Current drinkers were further asked what type of alcoholic beverages (spirits, beer, or wine) and what amount they had most recently drunk (by 220 ml mugs or 550 ml bottles for beer, and number of 50 ml “liang” for wines and spirits) at the last drinking, and how often in the last 12 months (once a month, 2–3 times a month, once a week, 2–3 times a week, 4–6 times a week, once a day, twice a day, more than twice a day). They also indicated the age when start drinking and whether they drank first thing in the morning to steady their nerves or get rid of a hangover. We converted measures of frequency and number of alcoholic drinks consumed into units of pure alcohol consumed per week. The following alcohol content by volume (v/v) was used for this calculation: beer 3.9%, wine 12%, spirits 53% [9]. One drink (unit) was defined as 14 g of pure alcohol consumed [10]. Current drinkers were classified into 0–13.9 units per week, 14.0–27.9 units per week and ≥ 28 units per week for men and 0–6.9 units per week and ≥ 7.0 units per week for women. Heavy drinkers were those who drank more than 14.0 drinks per week for men and more than 7.0 drinks per week for women [10]. A “binge” was defined as consuming 5 or more drinks (male), or 4 or more drinks (female), in about 2 h [11].
Covariates
We included age in years, living in urban or rural areas, education, rural-urban status, smoking status, depression, working status, social activities and sleep time as potential control variables in logistic regression analyses. We categorized participants into seven age groups (45–49 years, 50–54 years, 55–59 years, 60–64 years, 65–69 years, 70–74 years, and ≥ 75 years) and categorized their area of residence into seven regions, East (one city [Shanghai] and six provinces [Shandong, Jiangsu, Zhejiang, Fujian, Anhui, and Jiangxi]), North (two cities [Beijing and Tianjin] and three provinces [Hebei, Shanxi, and Inner Mongolia]), North-East (three provinces [Liaoning, Jilin, and Heilongjiang]), North-West (four provinces [Shaanxi, Gansu, Qinghai, and Xinjiang]), Central (three provinces [Henan, Hubei, and Hunan]), South-Central (two provinces [Guangdong, and Guangxi]), and South-West (one city [Chongqing] and three provinces [Sichuan, Guizhou, and Yunnan]) [12]. Individuals living in Hainan, Ningxia, Taiwan, and Tibet were not included in this survey. All participants were classified as either urban or rural residents. Education level was divided into four categories: no formal education, elementary school, middle/high school, and college degree or higher. Self-assessed health was divided into five categories: excellent, very good, good, fair and poor. Being a smoker was defined as smoking more than 100 cigarettes over the course of a lifetime [13]. The measure of depressive symptoms was based on responses to the 10-item version of the Center for Epidemiologic Studies Short Depression Scale (CES - D). Each item had four response options coded from 0 to 3. The total score was the sum for all 10 items. A dichotomous variable was created using a score of 10 or more to indicate the presence of depressive symptoms [14]. Current working was defined as “engaging in agricultural work for more than 10 days in the past year” or “working for at least one hour last week”. Participating in social activities was defined as “Have done any of these activities in the last month”. Total sleep time per day was calculated by adding the sleep time at night to the duration of a nap after lunch. Sleep time was divided into three categories: <6.0 h, 6.0~7.9 h and ≥8.0 h. Details of the items was listed by BASELINE QUESTIONNAIRE for CHARLS [13].
Statistical analysis
Continuous variables were shown as mean and standard deviation (SD), and categorical variables as percentage and corresponding standard error. All statistical analyses used SAS version 9.2, with adjustments for sample weights and survey design. Proc Surveyfreq procedure was used to calculate sex-specific prevalence of current drinking for each risk factor. Proc Surveylogistic procedure was used to examine the association between each risk factor and the prevalence of current and binge drinking. Both procedures considered the complex survey design and the nonresponse rate for the CHARLS survey when estimating the prevalence, prevalence odds ratio (OR), and corresponding standard errors and 95% confidence intervals (CIs), respectively. The sex-specific associations between the potential risk factors and alcohol consumption were tested by the statistical models adjusting for demographic characteristics (age groups, rural-urban status, marital status and region), and living status, smoking status, self- comment of health, depression, education, working status, participating in social activities and sleep time). All statistical tests were 2-sided and a P value less than 0.05 was considered statistically significant.
Results
Participants and current alcohol consumption
A total of 15,942 people (7,384 men and 8,558 women) with age range of 45-101 years were included in the analysis. Their mean age was 59.77 ± 9.68 years for men and 59.17 ± 10.06 years for women.
Table 1 shows the estimated prevalence rates of current drinking. The proportion of current drinkers was significantly higher among men than women (36.42% ± 0.86% vs. 3.73% ± 0.27%). In men, the prevalence of current drinking was higher at younger ages, in married subjects, in north-east areas, and in those with higher levels of education. In women, the prevalence was higher in rural areas and those living in the south-west region.
Among the current drinkers, proportions of binge drinking, heavy drinking and daily drinking were 38.2, 53.0, 57.5% for men and 10.9, 37.2, 36.2% for women, respectively. Men started drinking at significantly younger ages than women (23.24 ± 8.22 years vs. 28.25 ± 13.77 years). In total, 4.88% of current drinkers drank first thing in the morning to steady their nerves or get rid of a hangover. Both men and women living in rural areas had a higher proportion of “morning drinking” than those in urban areas (men: 6.11% vs. 1.83%; women: 2.89% vs. 0.00%).
Drinking behavior
The drinking status by factors is shown in Tables 2 and 3. Among men, there were significant differences in drinking status by age, marital status, education, smoking status, depression, working status and sleep time. There were more occasional drinkers among older people, and those with depression or poor health. Married drinkers seemed to be more likely to quit drinking. There were more former drinkers among participants with high levels of education. There was a higher proportion of heavy drinkers among those living in the north-east. Those who were working were more likely to be drinkers and heavy drinkers.
There were also more occasional drinkers among older women. Women who were married, or had high levels of education or good health status also tended to be former drinkers. The biggest proportion of heavy drinkers was in those living in the south-west. Those without a work trended to be lifetime abstainers.
Factors associated with alcohol consumption
The results of logistic regression detecting the relationship between included factors and alcohol consumption were listed in Tables 4 and 5. Among men, age and health situation were significantly and inversely associated with all alcohol consumption behaviors including current drinking, binge drinking, heavy drink and daily alcohol consumption. Smoking and living in north-east had a positive association with all of the alcohol consumption behaviors. Current working increased the risk of alcohol consumption behaviors including current drinking, heavy drink and daily alcohol consumption and social activities associated with current drinking (Table 4). Among women, smoking and current working were associated with increased levels of alcohol consumption. Compared with those in the central region, those living in the east area had an increased risk of drinking (Table 5).
The type of alcohol beverages
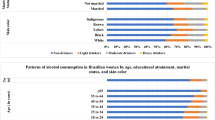
The favorite type of alcohol was spirits among both men and women. As age increased, the proportion of spirits consumed increased, and the proportion of beer consumed decreased. There were no significant differences in distribution of alcoholic type between urban or rural areas. As education level increased, participants were less likely to drink spirits. The proportion of spirits drunk was lowest in people living in the eastern area, where the consumption of both beer and wine was higher. Those with current working were more likely to drink beer and ≥ 2 types of alcohol beverage (Table 6).
Discussion
Approximately 36.42% of men and 3.73% of women reported consuming alcohol in the previous 12 months. The findings on drinking prevalence in our study are consistent with previous baseline survey from the China Kadoorie Biobank which is a nationwide prospective blood-based cohort study [15, 16]. The study involving 512,000 participants aged 30-79 years found a weekly drinking prevalence of 33% in men and 2% in women in 2004-08 [15, 16]. The estimated prevalence in our study was also comparable to the results from CLHLS among 16,255 adults aged ≥65 years. The study found that 34.14% of men reported drinking alcohol most weeks, compared with only 7.20% of women [17]. The prevalence among men was lower than that reported in the 2010–2012 Chinese Nutrition and Health Survey. The probable reason for this difference was that the age ranges of study participants varied. In Li’s study, the participants were aged 18 years or over, and the drinking rate was much higher among young adults than older people [5]. Generally, the alcohol consumption levels in China were lower than Whites or developed countries [17, 18]. The differences between the prevalence of alcohol consumption in China and developed countries may be partially due to the different levels of economic development. It was reported that greater economic wealth was broadly associated with higher levels of alcohol consumption and lower abstention rates [9]. Despite the relative low level of alcohol consumption, planning and implementation of a public health approach to alcohol control is urgently recommended for China’s governments because of a steady increase in alcohol production and consumption in recent decades [4] and the burden attributed to alcohol consumption [19,20,21,22].
Gender differences in drinking behavior have been observed in many studies [23, 24]. Drinking and smoking have been traditionally accepted and expected behaviors for Chinese men, but not for Chinese women. Research showed that 31.4% of female non-drinkers listed restriction by society as the main reason for their abstinence, whereas “Feeling sick after drinking” are the most common reason for male non-drinkers [25]. In China, especially in rural areas, men are more likely to take part in social activities, and it is accepted for men to drink with a meal, or to reduce pressure from work or to liven up the atmosphere. The highest prevalence of current drinking occurred during middle age in men. This is the age when men tend to be at the peak of their careers and might have more social interaction, which could increase the probability of drinking alcohol. It may also explain why the current drinking rate was higher in women with current work. Women with work tend to have more income and higher social status and therefore more social interactions.
Tobacco users were more likely to have other unhealthy dietary and health behaviors. Male drinkers who smoked also drank more alcohol than those who did not. Alcohol and tobacco are social tools in China. Traditionally, men believe that giving a cigarette and drinking together can bring people closer together quickly. Alcohol and tobacco use are highly co-morbid and have interactive effects on alcohol- and tobacco-motivated behaviors [26, 27]. Alcohol potentiates smoking behavior and vice versa.
Several variables such as depression, poor health status and sleeping problems, commonly co-occur with alcohol use disorder, and alcohol use disorder might increase the risk of those health-related disorders [28, 29]. However, we did not found the link between depression, sleep time and alcohol behaviors. The assessment of depression was concluded with the 10-item CES-D rather than diagnosed by psychologists, which may lead to inaccuracies. Furthermore, the purpose of social drinking in China is mainly to establish a joyful atmosphere and to easing tension [30]. Meanwhile, most drinking takes place accompanied by a meal which alleviated the damage done to the central nervous system by alcohol. Participants with poor health seemed to drink less. This may be because of the “sick-quitter” effect, where those with poor health stop drinking [31].
The proportion of heavy drinking in rural areas was higher than that in urban areas, although the difference was not statistically significant. Previous studies in China validated that participants who lived in rural areas drank more alcohol including all types (liqueur, beer and wine) than participants who lived in urban areas [32]. In Liu et al’s study, rural residents had higher risk of daily alcohol drinking and reporting alcohol dependence, regardless of province [3]. Meanwhile, homemade alcohol that was unrecorded alcohol was common in rural China. These findings claim the problems of alcohol consumption in rural areas and it deserves more attention from the Chinese government to take active measures for alcohol consumption control.
Alcohol consumption behaviors and lifestyles vary greatly across different regions in China. In this study, men in north-east region consumed more alcohol than residents of other areas. This may be because of the cold weather and the drinking culture in the north-east areas. However, women living in east region were more likely to drink. Probable reason is that east region is economically developed region of China, the social status and employment rate of women is comparable to that of men and they therefore have more access to social drinking.
The most common type of alcoholic beverage drunk was spirits. Individuals of different ages tended to consume different types of alcohol. Both men and women were more likely to consume spirits when they were older. The second most popular beverage was beer. Beer consumption trends with age showed the opposite of those for spirits. We also found a relatively high number of people who drank several types of beverage, particularly among younger adults. This may be because beer is relatively inexpensive and popular among young adults [3]. This phenomenon of mixed drinking is probably the result of exposure to a wider availability of alcoholic beverages brought by the rapid economic development and westernization of China [15].
Alcohol-related data have been reported in several studies of CHARLS [33,34,35]. However the focus of these researches were not with a view to alcohol consumption and the alcohol-related analyses were not exhaustive. The advantages of this study are the data adopted are based on national survey data, which is representative for the Chinese population and multi-dimensional data of alcohol consumption including alcohol type, drinking frequency and volume, and drinking pattern were analyzed. However, several limitations should be considered. Firstly, the data was from baseline survey that was cross-sectional designed, and therefore we only described the potential factors related to drinking behaviors and we cannot make any causal inferences about those factors for drinking behaviors. Secondly, we used a self-administered questionnaire to collect information on alcohol consumption and this may have resulted in self-report bias. Thirdly, the measure of alcohol use based on “the last time you consumed alcohol” may not accurately collect individual data on alcohol consumption [36, 37]. Lastly, the information was collected in CHARLS 2011–2012, and therefore the prevalence may now be different. Alcohol consumption has rapidly increased over time, and therefore further research is needed to monitor drinking patterns across the country.
Conclusion
There were strong gender disparities in drinking rate. Alcohol consumption behaviors and alcoholic type was significantly influenced by socio- cultural-demographic factors, such as age, smoking, working status and different regions. Our findings suggest that Chinese government should be provided with multidimensional interventions to meet different demands for different populations. In the future, the socio-cultural-demographic factors affecting alcohol patterns should be further focused on to promote the development of alcohol control strategies.
Availability of data and materials
The datasets generated and analyzed during the current study are available in the CHARLS website, available in http://charls.pku.edu.cn/en.
References
Alcohol GBD, Drug Use C: The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 2018, 5(12):987–1012.
Cochrane J, Chen H, Conigrave KM, Hao W: Alcohol use in China. Alcohol Alcohol 2003, 38(6):537–542.
Liu R, Chen L, Zhang F, Zhu R, Lin X, Meng X, Li H, Lei X, Zhao Y: Trends in Alcohol Intake and the Association between Socio-Demographic Factors and Volume of Alcohol Intake amongst Adult Male Drinkers in China. Int J Environ Res Public Health 2019, 16(4).
Tang YL, Xiang XJ, Wang XY, Cubells JF, Babor TF, Hao W: Alcohol and alcohol-related harm in China: policy changes needed. Bull World Health Organ 2013, 91(4):270–276.
Li Y, Jiang Y, Zhang M, Yin P, Wu F, Zhao W: Drinking behaviour among men and women in China: the 2007 China Chronic Disease and Risk Factor Surveillance. Addiction 2011, 106(11):1946–1956.
Lee YH, Chang YC, Liu CT, Shelley M: Correlates of alcohol consumption and alcohol dependence among older adults in contemporary China: Results from the Chinese Longitudinal Healthy Longevity Survey. J Ethn Subst Abuse 2020, 19(1):70–85.
Li YR, Wang J, Zhao LY, Wang ZH, Yu DM, He YN, Ding GG: [The drinking status and associated factors in adults in China]. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39(7):898–903.
Zhao Y, Hu Y, Smith JP, Strauss J, Yang G: Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol 2014, 43(1):61–68.
Organisation WH: World Health Organisation: Global status report on alcohol and health. 2014.
https://www.cdc.gov/alcohol/fact-sheets/alcohol-use.htm. Accessed 11 Jan 2022.
NIAAA Council approves binge drinking definition. National Institute on Alcohol Abuse and Alcoholism 2004, http://pubs.niaaa.nih.gov<background-color:#FF3300;bu>/publications/Newsletter/</background-color:#FF3300;bu>winter2004/Newsletter_Number3.pdf. Accessed 11 Jan 2022.
Zhou M, Astell-Burt T, Bi Y, Feng X, Jiang Y, Li Y, Page A, Wang L, Xu Y, Wang L et al: Geographical variation in diabetes prevalence and detection in china: multilevel spatial analysis of 98,058 adults. Diabetes Care 2015, 38(1):72–81.
http://charls.pku.edu.cn/Public/ashelf/public/uploads/document/application/CHARLS2011________.doc. Accessed 11 Jan 2022.
Boey KW: Cross-validation of a short form of the CES-D in Chinese elderly. Int J Geriatr Psychiatry 1999, 14(8):608–617.
Im PK, Millwood IY, Guo Y, Du H, Chen Y, Bian Z, Tan Y, Guo Z, Wu S, Hua Y et al: Patterns and trends of alcohol consumption in rural and urban areas of China: findings from the China Kadoorie Biobank. BMC Public Health 2019, 19(1):217.
Millwood IY, Walters RG, Mei XW, Guo Y, Yang L, Bian Z, Bennett DA, Chen Y, Dong C, Hu R et al: Conventional and genetic evidence on alcohol and vascular disease aetiology: a prospective study of 500 000 men and women in China. Lancet 2019, 393(10183):1831–1842.
Li J, Wu B, Selbaek G, Krokstad S, Helvik AS: Factors associated with consumption of alcohol in older adults - a comparison between two cultures, China and Norway: the CLHLS and the HUNT-study. BMC Geriatr 2017, 17(1):172.
Luczak SE, Wall TL: Gambling problems and comorbidity with alcohol use disorders in Chinese-, Korean-, and White-American college students. Am J Addict 2016, 25(3):195–202.
Lee S, Guo WJ, Tsang A, He YL, Huang YQ, Zhang MY, Liu ZR, Shen YC, Kessler RC: Associations of cohort and socio-demographic correlates with transitions from alcohol use to disorders and remission in metropolitan China. Addiction 2009, 104(8):1313–1323.
Yang L, Zhou M, Sherliker P, Cai Y, Peto R, Wang L, Millwood I, Smith M, Hu Y, Yang G et al: Alcohol drinking and overall and cause-specific mortality in China: nationally representative prospective study of 220,000 men with 15 years of follow-up. Int J Epidemiol 2012, 41(4):1101–1113.
Guo L, Deng J, He Y, Deng X, Huang J, Huang G, Gao X, Zhang WH, Lu C: Alcohol use and alcohol-related problems among adolescents in China: A large-scale cross-sectional study. Medicine (Baltimore) 2016, 95(38):e4533.
Xi B, Veeranki SP, Zhao M, Ma C, Yan Y, Mi J: Relationship of Alcohol Consumption to All-Cause, Cardiovascular, and Cancer-Related Mortality in U.S. Adults. J Am Coll Cardiol 2017, 70(8):913–922.
Wei H, Derson Y, Xiao S, Li L, Zhang Y: Alcohol consumption and alcohol-related problems: Chinese experience from six area samples, 1994. Addiction 1999, 94(10):1467–1476.
Hao W, Su Z, Liu B, Zhang K, Yang H, Chen S, Biao M, Cui C: Drinking and drinking patterns and health status in the general population of five areas of China. Alcohol Alcohol 2004, 39(1):43–52.
Wei H, Young D, Lingjiang L, Shuiyuan X, Jian T, Hanshu S, Zhunghong Y, Xiouying T, Xudong W: Psychoactive substance use in three sites in China: gender differences and related factors. Addiction 1995, 90(11):1503–1515.
Ma J, Betts NM, Hampl JS: Clustering of lifestyle behaviors: the relationship between cigarette smoking, alcohol consumption, and dietary intake. Am J Health Promot 2000, 15(2):107–117.
Verplaetse TL, McKee SA: An overview of alcohol and tobacco/nicotine interactions in the human laboratory. Am J Drug Alcohol Abuse 2017, 43(2):186–196.
Zheng D, Yuan X, Ma C, Liu Y, VanEvery H, Sun Y, Wu S, Gao X: Alcohol consumption and sleep quality: a community-based study. Public Health Nutr 2021, 24(15):4851–4858.
McHugh RK, Weiss RD: Alcohol Use Disorder and Depressive Disorders. Alcohol Res 2019, 40(1).
Wei H: Alcohol policy and the public good: a Chinese view. Addiction 1995, 90(11):1448–1450.
Emberson JR, Bennett DA: Effect of alcohol on risk of coronary heart disease and stroke: causality, bias, or a bit of both? Vasc Health Risk Manag 2006, 2(3):239–249.
Millwood IY, Li L, Smith M, Guo Y, Yang L, Bian Z, Lewington S, Whitlock G, Sherliker P, Collins R et al: Alcohol consumption in 0.5 million people from 10 diverse regions of China: prevalence, patterns and socio-demographic and health-related correlates. Int J Epidemiol 2013, 42(3):816–827.
Ding L, Liang Y, Tan ECK, Hu Y, Zhang C, Liu Y, Xue F, Wang R: Smoking, heavy drinking, physical inactivity, and obesity among middle-aged and older adults in China: cross-sectional findings from the baseline survey of CHARLS 2011-2012. BMC Public Health 2020, 20(1):1062.
Li Z, Fu C, Yang F, Mao Z: Prevalence and risk factors of hypertension for the middle-aged population in China - results from the China Health and Retirement Longitudinal Study (CHARLS). Clin Exp Hypertens 2019, 41(1):80–86.
Yao Y, Lu T, Liu Y, Qin Q, Jiang J, Xiang H: Association of depressive symptoms with ambient PM2.5 in middle-aged and elderly Chinese adults: A cross-sectional study from the China health and Retirement Longitudinal Study wave 4. Environ Res 2022, 203:111889.
Rehm J, Greenfield TK, Walsh G, Xie X, Robson L, Single E: Assessment methods for alcohol consumption, prevalence of high risk drinking and harm: a sensitivity analysis. Int J Epidemiol 1999, 28(2):219–224.
Kesmodel U, Olsen SF: Self reported alcohol intake in pregnancy: comparison between four methods. J Epidemiol Community Health 2001, 55(10):738–745.
Acknowledgements
We thank the CHARLS research and field team and every respondent in the study for their contributions.
Funding
This work was supported by the Pilot Project of Public Welfare Development and Reform for Commonweal Scientific Institutes in Beijing (Jingyiyan 2019-9).
Author information
Authors and Affiliations
Contributions
Wang Qianqian designed the concept and performed the data analysis, interpreted the data and prepared the manuscript. Zhang Yanzhuo and Wu Chengai contributed to the manuscript reviewing and data interpretation. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures and methods performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethics approval for the data collection in the CHARLS was obtained from the Biomedical Ethics Review Committee of Peking University (IRB00001052-11015). Each participant included in this study signed a written informed consent form before taking the survey.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, Q., Zhang, Y. & Wu, C. Alcohol consumption and associated factors among middle-aged and older adults: results from China Health and Retirement Longitudinal Study. BMC Public Health 22, 322 (2022). https://doi.org/10.1186/s12889-022-12718-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-12718-8