
Abstract
Background
Intimate partner violence (IPV) affects more than one in three women in sub-Saharan Africa (SSA). It is associated with both pregnancy and HIV, adversely affecting women in this region. This is the first systematic examination of the effects of IPV on HIV-positive (HIV+) pregnant women in SSA.
Methods
A systematic review of the literature on HIV+ pregnant women experiencing IPV in SSA was carried out. Searches were carried out in PubMed, Web of Science and African Journals Online databases. Articles published between January 2010 and June 2020, in English, were included. Data extraction included details on study locations, study design, study participants and the study outcome variables (depression, IPV, medication adherence, postpartum unsafe sex, and HIV disclosure).
Results
Fourteen studies (ten cross-sectional studies, four cohort studies) were included. Results indicate a high prevalence of IPV amongst pregnant women with HIV in SSA (18.0 to 63.1%). The results suggest an association between HIV-positive status and consequences of IPV during pregnancy, particularly mental health effects, such as depression symptoms and suicidal ideation. HIV-related stigma has a key role within the relationship between HIV and IPV during pregnancy. One study described that the presence of IPV reduces adherence to Prevention of Mother-To-Child Transmission (PMTCT) medication. Three studies reported no association between HIV positive status or HIV status disclosure and IPV during pregnancy.
Discussion/conclusions
The systematic review confirms interconnections between IPV and HIV seropositivity amongst pregnant women in SSA. Importantly, stigma, social isolation and poor mental health hinder help-seeking, disclosure, and treatment adherence among HIV+ pregnant women exposed to IPV in SSA. As a result, the potential of community interventions to tackle issues associated with IPV in HIV-positive pregnant women in this area should be explored in research, policy, and practice.
Similar content being viewed by others

Background
Introduction
Violence against women is one of the most pervasive manifestation of gender inequalities and violation of human rights [1, 2]. The most common form is intimate partner violence (IPV), with 1 in 3 women, globally, experiencing violence by a partner or ex-partner in their lifetime [2, 3]. IPV results in devastating consequences for women and their children and these effects have been well-documented [4,5,6,7], as have the associations between IPV exposure and positive HIV status [8,9,10].
In the WHO Africa region, the estimated prevalence of HIV of 36.6% (95% CI = 32.7-40.5%) is higher than the rate in high-income countries of 23.2% (95% CI = 20.2-26.2%) [6]. The high burden and detrimental effects of HIV in sub-Saharan Africa (SSA) are well-known [11,12,13,14,15,16,17,18], accounting for 71% of the global burden of disease of HIV [19]. However, a comprehensive understanding of the literature on IPV, HIV and pregnancy is missing. This paper aims to systematically review the literature on HIV+ pregnant women experiencing IPV in SSA. The review focuses on SSA due to the high prevalence of IPV, high prevalence of HIV seropositivity, shared risk factors for IPV and HIV and the substantial lack of literature on IPV in this region.
Effects of IPV on health
Physical health consequences of IPV, regardless of pregnancy, include physical injuries, such as, bruises, broken ribs and head injuries [3, 20]. In addition, IPV is associated with long-term chronic health problems, including chronic pain and gastrointestinal disorders [3, 20], due to continued exposure to violence and stress. These health conditions persist even after exposure to violence has ended [20]. Mental health effects of IPV are also extensive and include depression, anxiety disorders, post-traumatic stress disorder (PTSD), sleep disturbances and suicide attempts [2, 5].
IPV restricts health seeking behaviour as well as sexual and reproductive control for women. This puts them at increased risk for other health problems such as sexually transmitted infections (STIs), unwanted pregnancies, obstetric complications and long-term chronic diseases as a result of stress [5,6,7]. IPV during pregnancy can have direct repercussions on neonates, with high rates of low birth weight and preterm birth associated with IPV, potentially due to the physiological responses to the stress induced by violence exposure [6, 8, 9]. Furthermore, IPV has been reported to reduce women’s ability to care for their children [9], with particular impacts on health-seeking behaviours for their children [1, 21] and breastfeeding [5, 11]. Figure 1 depicts the complexity of IPV’s interaction with the physical, mental, sexual, and reproductive health of women.

Pathways and health effects of IPV (Figure with permission from WHO [22])
While it is essential not to perpetuate harmful gender stereotypes by concentrating on women in relation to their reproductive potential [23, 24], IPV during pregnancy requires particular attention for four reasons. Firstly, pregnancy is a vulnerable time for women, making them more susceptible to harm [25]. Additionally, it affects two or more lives, with detrimental effects on mothers and neonates. Third, there is a wide variation of prevalence estimates for IPV during pregnancy; Devries et al. [26] discuss estimates of 3 to 30% from previous global prevalence studies. Finally, pregnancy can result in increased contact with healthcare services which allows for increased opportunities to screen for, detect and support women exposed to or at risk of IPV [27].
HIV and IPV in sub-Saharan Africa
WHO and UNICEF data report that vertical transmission of HIV from mother to child accounts for approximately 35% of HIV infected infants worldwide [28]. An estimated 9 out of 10 of the over 2.8 million children and adolescents who are living with HIV in 2020 were living in SSA [29, 30]. Studies focusing on how this burden is related to IPV during pregnancy are limited [5]. The WHO recognises how violence against women and girls can contribute to their increased vulnerability to HIV, especially in this region [31]. They implicate the following links between HIV and IPV: direct transmission through sexual violence, increased HIV risk-taking behaviours by women because of previous or current exposure to violence, fear of discussing condom use and fear of violence if tested HIV+, preventing women from being tested or disclosing their status.
Importantly, both HIV and IPV are associated with an overwhelming level of stigma [32,33,34,35,36,37], defined as having ‘a socially devalued identity’ which can be seen as a ‘mark of failure or shame’ ( [34]: p 2). This stigma can be externally or internally imposed, that is, either from others or from oneself respectively [38, 39]. It creates barriers for reporting and healthcare seeking and adds to the physical and mental health burden of HIV and IPV individually [32, 34,35,36,37]. Figure 2 [40] demonstrates four ways that IPV and HIV seropositivity interact amongst pregnant women: partner disclosure, Prevention of Mother-To-Child Transmission (PMTCT) uptake, mental health and relationship control. These effects of IPV and HIV, and associated stigma, are likely compounded in SSA, where a large proportion of women live in poverty; 27 of the 28 poorest countries in the world are in this region [41].

Figure available on Open Access from Hatcher and colleagues: IPV and HIV-related health issues among pregnant women [40]
The aim of this review is to examine this double burden of IPV and HIV through studying the existing literature on IPV effects on HIV+ pregnant women in SSA. This is to shed light on the specific challenges this vulnerable group faces.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Additional files 1 and 3), informed by previous systematic reviews in this area [42,43,44,45,46].
Search methods
Systematic searches were performed in three electronic databases: PubMed, Web of Science and African Journals Online. Separate search strategies were developed for each database including key words and MeSH terms [46]. Search terms included intimate partner violence, domestic abuse, domestic violence, pregnancy, primigravida, HIV and human immunodeficiency virus (Additional file 2). Articles included were published from January 2010 to June 2020. This period was chosen with interest in up-to-date studies reflecting the time window where access to antiretroviral therapy (ART) in low- and middle-income countries was available. The number of people on ART increased from 2 million to 17.2 million people between 2005 and 2010 [47].
Selection process
All records captured by the search terms were exported to a Mendeley library. Duplicates were eliminated. Titles and abstracts were screened by the primary author. Those that did not meet the eligibility criteria were excluded. The remaining articles were examined through full-text review, with reasons for exclusion noted down, until a final set of studies to be included was established.
Eligibility criteria
Inclusion criteria
The eligibility criteria were studies published between January 2010 to June 2020. Articles based on original quantitative research results, undertaken in an SSA country using any of the following study designs: cross sectional, cohort, case control, and randomised controlled trial. Only articles published in English in peer-reviewed journals were included. Studies had to include pregnant women (or mothers attending postnatal care reporting IPV during pregnancy). Articles had to focus on IPV only (physical, sexual, and emotional) and/or risk factors. IPV was defined as violence occurring in relation to past and current spouses, boyfriends, fiancés, whether they were married, cohabitating or dating [43]. Articles were included when reporting HIV status of either women or both men and women.
Exclusion criteria
Exclusion criteria were: papers focusing on domestic violence/abuse that was familial or parental; papers focusing on IPV during pregnancy in non-SSA countries; reporting on effects or experiences of others than women (e.g. focusing on neonates, infants, children or men only); grey literature, non-academic papers (commentaries, editorials, etc.), books, book chapters; other systematic reviews (in order to focus on primary data and avoid double reporting); qualitative studies; studies focusing on treatment/management of IPV only; studies where strength of associations (p values) were not reported; studies where the methods used are not adequately described, for instance questionnaire contents not reported, or the questionnaires were not validated.
Data extraction
Following full-text analysis, data were extracted with the use of a data extraction form adapted from previous studies [43, 45]. Items included study locations, study design, study participants and outcomes. If two articles used the same data set but reported on different outcome variables, both articles were included if they met the eligibility criteria.
Quality assessment and risk of bias
Selected studies were assessed for quality and risk of bias by the primary author in discussion with the co-authors. Quality assessment was informed by the criteria used by Alhabib et al. [48], which were adapted for the purposes of this paper:
-
Target population explicitly stated
-
Use of probability sampling methods e.g., simple random sampling, stratified sampling, clustered sampling
-
Large enough sample size (≥ 300 participants)
-
Reported and adequate response rate (≥80%)
-
Reports the use of trained interviewers
-
Reports confidence intervals or standard errors
-
Reported attempt to reduce selection and/or measurement bias
-
Adjusted for confounding variables.
Articles were scored for quality, where each criterion was worth 1 point. Hence each included article was given a score out of 8. A score equal to or less than 4 was classified as “poor”, 5-6 as “good” and 7-8 as “very good”.
Results
Study characteristics
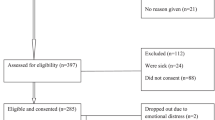
The search strategy captured 1112 records. Eighteen duplicates were removed, and 1094 abstracts were screened, eliminating 981 for not meeting the eligibility criteria, therefore resulting in 113 for full-text review. The review includes 14 studies (Fig. 3, Table 1). The most common reason for exclusion was study participants not being pregnant or solely focusing on the postpartum period.

PRISMA flow diagram of the data extraction process [42]
The earliest publication year was 2013, and the most common was 2016 (n = 4, 28.6%). Many of the studies were undertaken in South Africa (n = 10, 71.4%), followed by Zimbabwe (n = 2, 14.3%), Zambia (n = 1, 7.14%) and Tanzania (n = 1, 7.14%). Ten of the studies were cross-sectional (71.4%), while 4 were longitudinal cohort studies (28.6%). In relation to sample size, only one study had less than 300 participants. All studies collected data from clinical samples, except the research by Rodriguez et al. [58], which analysed population data from a province in South Africa. Questionnaires were used as the main data collection method in all studies; however, this was done in different ways: either face to face interviewing (n = 8 [49,50,51, 53, 54, 57, 59, 60]: or using Audio Computer-Assisted Self-Interview (ACASI; n = 6 [52, 55, 56, 58, 61, 62]. IPV was measured either through a WHO questionnaire (n = 6: studies [51, 53, 54, 56,57,58]) or the use of a Conflict Tactics Scale (n = 7: studies [52, 59,60,61,62,63,64]). A large proportion of the studies studied HIV+ women only (n = 11, 78.6%), despite the search strategy not differentiating between HIV+ and HIV-negative samples. Through quality assessment (Alhabib Score), one study was classified as “poor”, six as “good” and seven as “very good”.
Nine out of fourteen studies reported on mental health, three had IPV as one of the main outcomes, one reported on medication adherence, one on HIV status disclosure and one on postpartum unsafe sex. Eight of the papers included partner’s HIV status [50, 52, 55, 56, 58, 59, 61, 62], but none reported it as a main outcome. Table 1 presents a summary description of the included articles.
Overall, eight of the fourteen studies (57.1%) reported interactions between HIV+ status and IPV risk and/or effects during pregnancy. IPV prevalence reported in studies is summarised in Table 2.
No association was found between IPV and disclosure of HIV status to a partner [OR 0.73 (95% CI 0.50-1.06; p = 0.112)] or someone else [OR 0.87 (95% CI 0.57-1.31; p = 0.499)] in one study [62]. Furthermore, one study [49] reported that there was no difference in IPV prevalence between women who had been diagnosed with HIV previously compared to those newly diagnosed during the current pregnancy. Another study [53] reported no interaction between HIV and IPV exposure during pregnancy.
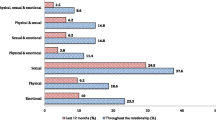
IPV prevalence during pregnancy ranged from 18.0% [53] to 63.1% [59]. In the studies examining different forms of IPV, emotional/psychological violence was found to be the most prevalent [49,50,51]. Studies looking at mental health symptoms, reported strong associations between IPV and depression symptoms [49, 51, 52, 54, 55, 60, 61, 63], postpartum emotional distress [53] and suicidal ideation [58] among HIV+ pregnant women.
Peltzer, Rodriguez and Jones [61] highlight a key component within the relationship between IPV, HIV, mental health and unplanned pregnancy. Among women who reported IPV, the odds of depression were higher for HIV+ women with an unplanned pregnancy compared to those with a planned pregnancy (p < 0.001). Contrastingly, when IPV was not reported, this difference in odds of depression between these groups ceases (p > 0.05). Additionally, Wong et al. [60], found that amongst HIV+ women experiencing IPV, younger women (18-24 years old) had a higher mean depression score compared to older women (≥25 years old) – 9.8 vs 6.8 (p = 0.01). Both younger and older HIV+ pregnant women experiencing IPV reported more depressive symptoms compared to those not experiencing IPV [60].
In the nine studies whose main outcome was mental health, six reported some relationship between HIV+ status and depressive symptoms in pregnant women [51,52,53, 55, 56, 58]. Manongi et al. [51] reported HIV as an effect modifier for the association between emotional violence and signs of depression with the adjusted odds of experiencing emotional violence being 2.61 (95% CI 1.62-4.20), compared to those without HIV 0.09 (95% CI 0.00-3.16). HIV-related stigma was one of the key factors associated with depressive symptoms [56, 61] and suicidal ideation [58]. Matseke et al. [52] further reported an association between HIV-related stigma and any form of IPV.
Two of the studies found a significant association between IPV and HIV risk behaviour [50, 57]. Hampanda [50] demonstrated that the presence of IPV reduces adherence to PMTCT medication, reporting a dose-response relationship where for each additional violent event a woman experienced, she had 20% reduced odds of adherence to the medication during pregnancy. Severe psychological and physical IPV, coupled with male controlling behaviour, increased the odds of unsafe sex postpartum among HIV+ women in Reyes et al. [57]. The authors reported an adjusted odds ratio (aOR) of 7.19 (95% CI 1.60-32.33) among IPV survivors after controlling for sociodemographic variables and length of relationship. The aOR increased to 7.74 (95% CI 1.59-37.71) among women who experienced IPV after addition of theoretical confounders to the model, including childhood abuse and age at first sex. This study did not find a statistically significant association between moderate IPV and postpartum unsafe sex.
Discussion
IPV exposure in HIV+ pregnant women poses a substantial health burden, especially in SSA. This is the first systematic review examining the effects of IPV on this group. There was a wide variety of reported IPV prevalence in the included studies of this review, with rates ranging from 19.6% [61, 62] to 56.3% [52]. This is likely due to the various challenges involved in determining IPV prevalence globally and more specifically in SSA [7, 20]. These are discussed in more detail in the limitations section.
The review’s findings demonstrate five key issues. Firstly, the relationship between IPV and the mental health outcomes of HIV+ pregnant women. Secondly, emotional/psychological violence was reported as the most prevalent form of IPV. Third, unplanned pregnancy was highlighted as a crucial factor in increased depressive symptoms in HIV+ pregnant women experiencing IPV. Fourth, stigma was shown to have a tremendous role to play within this relationship and finally, IPV increases HIV risk behaviours in this group, such as reducing condom use and reducing adherence to PMTCT medication. These findings align with the model from Hatcher et al. [40] that illustrates the interaction between IPV and HIV seropositivity.
Overall, the review describes a high prevalence, and thus a substantial burden, of IPV in HIV+ pregnant women in SSA, especially emotional/psychological abuse. It is crucial to note that it is usually more difficult to measure this form of IPV, since emotional/psychological abuse can be difficult to conceptualise [22, 27]. The nature of this type of abuse, however, could go some way in explaining its high prevalence of IPV in HIV+ pregnant women in SSA. Potentially, perpetrators and others may consider these behaviours more acceptable [27] and consequently, they may not view them as abuse. Further research in this area is necessary to explore emotional and psychological abuse in pregnant women in more depth.
Most studies focussed on the mental health of HIV+ pregnant women exposed to IPV, which is important as the search strategy did not target mental health explicitly. They report high levels of depressive symptoms, psychological distress, and suicidal ideation because of IPV exposure. Furthermore, HIV+ pregnant women exposed to IPV who are younger or who have unplanned pregnancies were at higher risk of increased depressive symptoms, compared to women who were not exposed to IPV. Ashaba et al. [64] corroborate this in their qualitative study. It demonstrated that increased verbal and emotional abuse was associated with unplanned pregnancy in women living with HIV, particularly when informing their partners about the unplanned pregnancy. This has implications for determining which groups to target within healthcare settings, and the role that sexual and reproductive health (SRH) services can play in IPV interventions. Additionally, Hatcher et al. [40] discuss how maternal mental health associated with IPV is often overlooked during maternal contact with health professionals, which could be an important point of entry for this group.
The double burden of adversity
HIV-related stigma was highlighted as a crucial contributor to the IPV experiences of pregnant women in our study. This review revealed that stigma was associated with all forms of IPV [52] and depressive symptoms [56] within this population. The findings imply that it is not just the physical experience of HIV, IPV or both that causes difficulties, but also, the associated feelings of shame, which can be both internalised and externally imposed.
While external stigma is important, and worth highlighting, the effects of internalised stigma need emphasis as these can be particularly insidious. The negative impact of both IPV and HIV on a person’s self-identity needs to be specifically focused on, as it relates to their individual coping strategies. This can result in harmful consequences, for instance limiting help-seeking behaviour or treatment adherence [35,36,37]. This can be aggravated when these exposures co-occur, as shown by two of the studies included in this review [52, 56].
Labels such as ‘victim’ or ‘HIV-infected’ can affect how a person sees themselves and how society perceives them [33, 38, 39]. Even if IPV or HIV are not disclosed, internalised stigma can still impact a person’s ability to seek help, therefore jeopardising opportunities for diagnosis and management [38, 39], or worsening their mental health [38, 65, 66]. The presence of both HIV and IPV stigma in this review have been described to leave expectant and current mothers feeling isolated [67, 68], creating a barrier to both HIV-related and pregnancy-related care [68]. A crucial step in IPV management, after these services have been made available, is recognising the need for them. Unfortunately, internalised stigma can hamper this tremendously. Moreover, it is a difficult aspect of this relationship to target as it requires changing both social norms and personal beliefs.
As discussed, HIV- and IPV-related stigma can influence medication adherence. Others have demonstrated a complex relationship between IPV, mental health and HIV medication adherence [40, 67]. Hatcher et al. [67] highlight that poor adherence can be used as a means of self-harm, as women experiencing both of these conditions during pregnancy may feel overwhelmed and therefore have a desire to end their lives. Additionally, ever present thoughts and experiences of violence can result in forgetfulness – either forgetting to take their medication or forgetting to pick them up. This effect can be aggravated by the memory impairment and concentration problems characteristic of PTSD and depression. Both these mental health conditions are strongly associated with IPV and trauma [1, 2, 69], despite PTSD not being one of the reported outcomes in the studies included in this review. For some women, however, motherhood can provide resilience, allowing them to focus on their child’s wellbeing [67]. This may allow women to continue taking their medication, however, it does not necessarily reduce their exposure to IPV nor its devastating effects.
IPV, HIV and fear
This review provided a better understanding of the relationship between HIV and IPV with fear acting as a potential mediating factor. The findings suggest that interactions between partner disclosure, PMTCT uptake, and relationship control are key in understanding the association between HIV and IPV during pregnancy [50, 57]. This is corroborated by previous qualitative research [40]. IPV and fear of IPV can result in women not feeling confident enough to request condom use [57], placing them at increased risk of HIV and other STIs [40, 68, 70]. Furthermore, Hampanda [50] demonstrates how IPV can reduce PMTCT medication adherence. A systematic review by Hatcher et al. [71], supports this as they report that the presence of IPV reduces adherence to antiretroviral therapy for HIV+ women.
There are various potential reasons for reduced medication adherence. Firstly, IPV can contribute to reduced adherence through direct partner control over access to HIV treatment [64, 67]. Second, fear of HIV disclosure can result in women avoiding taking their medication to prevent their partners finding out. Many studies have reported that this fear stems from a worry that their partners will consider them unfaithful, resulting in increased emotional or physical violence [40, 64, 70, 72,73,74]. While a study in this review [62] reported no association between IPV during pregnancy and HIV status disclosure, other studies have emphasised the importance of this relationship [40, 64, 72, 75, 76]. The potential impact of internalised stigma should also be highlighted here. This is because it can result in low self-esteem that means women do not feel capable of asserting safe sex practices or medication adherence. All in all, this review has demonstrated the variety of ways IPV complicates the experiences of HIV+ pregnant women.
Strengths and limitations
This review has key strengths. First, it was a systematic review, using PRISMA guidelines, to study effects of IPV on HIV+ pregnant women in SSA. Second, the search was conducted in multiple databases resulting in a more comprehensive review. Additionally, the inclusion of African Journals Online ensured that studies from SSA were not unintentionally excluded due to publication bias. Lastly, the exclusion of studies not reporting p values or data collection methods and the use of standardized quality assessment [48] of the included studies ensured avoidance of low-quality studies, which strengthen the reliance on the study findings. However, the explicit focus on studies published in English, the last 10 years and, within the medical literature may have excluded relevant literature.
Despite the valuable information garnered from the 14 included studies, the studies have several limitations. Firstly, all studies relied heavily on self-reporting for their key outcomes which is liable to social desirability bias, recall bias and under-reporting, especially considering the stigma associated with both conditions. The studies that used ACASI went some way in overcoming this as its use can contribute to reduced social desirability bias, and the audio function makes it more appropriate in low-literacy populations, but only if used correctly [77]. Secondly, depression symptoms were measured using the Edinburgh Postnatal Depression Scale, without diagnostic review. Therefore, it does not provide a definitive diagnosis of depression as defined by either the Diagnostic and Statistical Manual of Mental Disorders or the International Classification of Disease-10. This may have led to some discrepancies between studies.
As mentioned previously, prevalence of IPV varied greatly amongst the included studies. This is likely to be because what constitutes as abuse is not standardised between and within countries. In addition, it is heavily reliant on self-reporting [7] and women recognising what they experience as IPV. Secondly, the methodology of data collection in studies differ, including questionnaires or face to face interviews. These have their own inherent biases and can also result in different responses [19]. Furthermore, psychological/emotional forms of abuse and controlling behaviours may not be recognised as IPV, which may contribute to underreporting [7, 20]. Challenges in studying IPV and HIV are therefore likely to have impacted the studies included in this systematic review.
In addition to this, many of the studies used non-proportional sampling, meaning that some individuals had no chance of being selected. Subsequently, this inhibited the ability to estimate the effects of sample error resulting in a non-representative sample and potentially non-generalisable results. Importantly, most studies (n = 13) recruited clinical samples and only one study offered population estimates on IPV. As a result, prevalence estimates cannot be generalised. Moreover, only 3 studies included HIV-negative women in their sample, so it is difficult to draw conclusions based on this evidence. There is a need for further comparative studies to better understand this relationship.
The review identified gaps in the existing literature. While physical violence and psychological/emotional violence were often reported in the included studies, there was limited information on sexual violence and male controlling behaviours. Furthermore, the studies that reported on mental health outcomes only discussed depressive symptoms and suicidal ideation. However, anxiety, PTSD and substance abuse are crucial mental health conditions that are likely to affect this group [1, 2, 69], but this was not captured in this review. Two studies reported on substance abuse [49] and alcohol use [60], but they did not explore how IPV affects these outcomes in HIV+ pregnant women. There is therefore a need to broaden the scope of the mental health outcomes while researching this group.
Finally, there are the limitations associated with the cross-sectional study design used in a large proportion of the studies. This hinders interpretation of causal links between IPV and HIV among pregnant women. The few longitudinal studies identified in the review opted for short follow-up periods determined by pregnancy status (pre- and post-partum), independent of changes to HIV status or IPV exposure. Finally, the geographical distribution of studies was limited, with all studies conducted in English speaking countries in SSA, and most of the studies being conducted in South Africa (n = 10). Nevertheless, this review provides a starting point for enhanced research into the effects of IPV exposure on HIV+ pregnant women in SSA.
Implications of findings
The results of this systematic review build on previous literature on IPV and HIV [43, 78,79,80]. This review offers new insights into the severe problem of IPV amongst HIV+ pregnant women in SSA, with devastating consequences on their mental and physical health. These findings have important implications for further research, policy, and practice.
The review has identified important research gaps. The presence of IPV during pregnancy complicates maternal mental health extensively amongst HIV+ women [49, 51, 52, 54]. Hence, further research is required into better diagnosis and management of mental health issues related to these two stigmatising conditions, especially looking at anxiety, PTSD, and substance abuse. Despite a search strategy aiming to identify sexual violence and controlling behaviours by intimate partners as well, little information was found, which could be both a cause and a consequence of stigma. It is also important to highlight that women who may not seek healthcare services will likely be underrepresented in this research, as most of the studies focused on healthcare settings. Subsequently, more efforts are needed to gather data on the needs of this specific group, and, how best to provide IPV services for them.
Only one included study reported on PMTCT adherence, however, this is noteworthy considering that one of the main ways that HIV spreads in SSA is vertical transmission from mother to child; Hampanda [81] approximates that it accounts for 15% of the total global incidence. Therefore, further qualitative and quantitative research on the effects of IPV during pregnancy on PMTCT adherence is vital to inform policymaking and advocacy. This also further corroborates the value of adding discussions on IPV into sexual reproductive health and rights discourse.
More research is also required comparing HIV-negative and HIV+ women’s experiences of IPV, perhaps with case-control studies, as many of the studies only examined HIV+ women. Furthermore, all longitudinal studies identified in the review included women enrolled during pregnancy with short term follow-up pre- and post-partum. Forthcoming studies should follow women through an extended period of their reproductive life and/or include comparison groups. This could contribute to understanding potential causal links between pregnancy, IPV and HIV status in the longer-term.
The findings provide guidance for policy and practice. The WHO guidelines on responding to IPV [82] suggest the use of antenatal care for increased IPV screening and intervention opportunities. This review highlights the importance of developing and implementing guidelines that recognize and target the concerns of HIV+ pregnant women exposed to IPV, particularly by Ministries of Health in SSA countries. This also includes increasing resources for training health workers to overcome the barriers of stigma related to these two conditions, as ensuring that healthcare workers do not retraumatise their patients is essential [83]. Due to the highly stigmatising nature of both HIV and IPV, including IPV management in already existing services and structures can help to capture women in this vulnerable group.
It could be argued that policies in the WHO AFRO region and at country level should consider IPV screening for pregnant women attending HIV clinics. The results suggest that exploration of outreach activities or targeted interventions, sensitised to stigma, should be considered. Our findings have illustrated how the isolation associated with HIV and IPV amongst pregnant women in SSA can affect their health-seeking behaviour. Hence, ensuring IPV screening and management is a part of antenatal, HIV and SRH services could be of tremendous value to these women.
Conclusions
The findings of this review have illustrated that in SSA, HIV+ pregnant women are experiencing high levels of IPV. IPV exposure in HIV+ pregnant women has detrimental effects on maternal mental health especially, as there is a high prevalence of depression and suicidal ideation in this population. Furthermore, HIV and IPV cause a double burden of adversity, interacting through stigma. The review revealed an intricate relationship between HIV medication adherence, mental health and IPV. These findings have substantial repercussions for both mothers and their children, as vertical transmission still contributes to a large proportion of new HIV infections in SSA.
HIV+ pregnant women experiencing IPV are a highly vulnerable and highly marginalised group. There is a need for more research on screening, diagnosis and management as well as increased attention in policy making for this group. IPV is a deeply traumatising and isolating experience, with a large presence in SSA. Addressing IPV, HIV and their related stigma is long overdue to guarantee that every woman, pregnant or not, can feel safe in her own home.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Abbreviations
- IPV:
-
Intimate Partner Violence
- HIV:
-
Human Immunodeficiency Virus
- WHO:
-
World Health Organization
- SSA:
-
Sub-Saharan Africa
- PTSD:
-
Post Traumatic Stress Disorder
- STIs:
-
Sexually Transmitted Infections
- HIV + :
-
HIV positive
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- ART:
-
Antiretroviral Therapy
- ACASI:
-
Audio Computer-Assisted Self-Interview
- PMTCT:
-
Prevention of Mother-To-Child Transmission
- aOR:
-
Adjusted Odds Ratio
- SRH:
-
Sexual and Reproductive Health
References
Halim N, Beard J, Mesic A, Patel A, Henderson D, Hibberd P. Intimate partner violence during pregnancy and perinatal mental disorders in low and lower middle income countries: a systematic review of literature, 1990–2017. Clin Psychol Rev. 2018;66(November 2017):117–35.
WHO. Violence against women: Geneva, World Health Organisation; 2017. Available from: https://www.who.int/en/news-room/fact-sheets/detail/violence-against-women. [cited 2020 Jul 10].
WHO & PAHO. Understanding and addressing violence against women: intimate partner violence: Washington, DC, Pan American Health Organisation. Geneva: World Health Organization; 2012. https://apps.who.int/iris/handle/10665/77432. Accessed 11 Nov 2021.
Mahenge B, Stöckl H, Abubakari A, Mbwambo J, Jahn A. Physical, sexual, emotional and economic intimate partner violence and controlling behaviors during pregnancy and postpartum among women in Dar Es Salaam, Tanzania. PLoS One. 2016;11(10):1–10.
Sigalla GN, Rasch V, Gammeltoft T, Meyrowitsch DW, Rogathi J, Manongi R, et al. Social support and intimate partner violence during pregnancy among women attending antenatal care in Moshi municipality, Northern Tanzania. BMC Public Health. 2017;17(1):1–12.
Alhusen JL, Ray E, Sharps P, Bullock L. Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Women's Health. 2015;24(1):100–6.
Hill A, Pallitto C, McCleary-Sills J, Garcia-Moreno C. A systematic review and meta-analysis of intimate partner violence during pregnancy and selected birth outcomes. Int J Gynecol Obstet. 2016;133(3):269–76.
Ceccon RF, Meneghel SN. HIV and violence against women: study in a municipality with high prevalence of aids in the south of Brazil. Rev Panam Salud Publica. 2015 May;37(4–5):287–92.
Woollett N, Hatcher AM. Mental health, intimate partner violence and HIV. South African Med J. 2016;106(10):969–72.
Ruark A, Stern E, Dlamini-Simelane T, Kakuze MF. Love matters: exploring conceptions of love in Rwanda and Swaziland and relationship to HIV and intimate partner violence. African J AIDS Res. 2017;16(4):271–82.
Uthman OA. Prevalence and pattern of HIV-related malnutrition among women in sub-Saharan Africa: a meta-analysis of demographic health surveys. BMC Public Health. 2008;8:1–8.
Barth RE, Huijgen Q, Taljaard J, Hoepelman AIM. Hepatitis B/C and HIV in sub-Saharan Africa: an association between highly prevalent infectious diseases. A systematic review and meta-analysis. Int J Infect Dis. 2010;14(12):e1024–31.
Berhan A, Berhan Y, Yizengaw D. A meta-analysis of drug resistant tuberculosis in sub-Saharan Africa: how strongly associated with previous treatment and HIV co-infection? Ethiop J Health Sci. 2013;23(3):271–82.
Wasserman S, Engel ME, Griesel R, Mendelson M. Burden of pneumocystis pneumonia in HIV-infected adults in sub-Saharan Africa: a systematic review and meta-analysis. BMC Infect Dis. 2016;16(1):1–9.
Avert. Global HIV and AIDS statistics: Avert UK; 2018. Available from: https://www.avert.org/global-hiv-and-aids-statistics [cited 2020 May 25]
Dwyer-Lindgren L, Cork MA, Sligar A, Steuben KM, Wilson KF, Provost NR, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature. 2019;570(7760):189–93.
Cuadros DF, Li J, Branscum AJ, Akullian A, Jia P, Mziray EN, et al. Mapping the spatial variability of HIV infection in sub-Saharan Africa: effective information for localized HIV prevention and control. Sci Rep. 2017;7(1):1–11.
Bernard C, Dabis F, De Rekeneire N. Prevalence and factors associated with depression in people living with HIV in sub-Saharan Africa: a systematic review and meta-analysis. PLoS One. 2017;12(8):1–22.
Kharsany ABM, Karim QA. HIV infection and AIDS in sub-Saharan Africa: current status, Challenges and Opportunities. Open AIDS J. 2016;10(1):34–48.
Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359(9314):1331–6.
Goo L, Harlow SD. Intimate partner violence affects skilled attendance at most recent delivery among women in Kenya. Matern Child Health J. 2012;16(5):1131–7.
WHO. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. 2013.
Raymond SU, Greenberg HM, Leeder SR. Beyond reproduction: Women’s health in today’s developing world. Int J Epidemiol. 2005;34(5):1144–8.
WHO. Women’s Health. World Health Organisation. Available from: https://www.who.int/topics/womens_health/en/. [cited 2020 Jul 23]
Caleyachetty R, Uthman OA, Bekele HN, Martín-Cañavate R, Marais D, Coles J, et al. Maternal exposure to intimate partner violence and breastfeeding practices in 51 low-income and middle-income countries: a population-based cross-sectional study. PLoS Med. 2019;16(10):1–15.
Devries KM, Kishor S, Johnson H, Stöckl H, Bacchus LJ, Garcia-Moreno C, et al. Intimate partner violence during pregnancy: analysis of prevalence data from 19 countries. Reprod Health Matters. 2010;18(36):158–70.
Bailey BA. Partner violence during pregnancy: prevalence, effects, screening, and management. Int J Women's Health. 2010;2(1):183–97.
Yah CS, Tambo E. Why is mother to child transmission (MTCT) of HIV a continual threat to new-borns in sub-Saharan Africa (SSA). J Infect Public Health. 2019;12(2):213–23.
UNICEF. HIV and AIDS. New York: UNICEF; 2021. Available from: https://www.unicef.org/hiv. [cited 2021 Aug 20].
Avert. Children, HIV and AIDS. Brighton: Avert UK; 2018. Available from: https://www.avert.org/professionals/hiv-social-issues/key-affected-populations/children. [cited 2021 Aug 20].
VPA. The Ecological Framework. Violence Prevention Alliance. Available from: https://www.who.int/violenceprevention/approach/ecology/en/. [cited 2020 Jul 8]
Avert. HIV stigma and discrimination. Brighton: Avert; 2017. Available from: https://www.avert.org/professionals/hiv-social-issues/stigma-discrimination. [cited 2020 Sep 3].
Eckstein JJ. IPV stigma and its social management: the roles of relationship-type, abuse-type, and victims’ sex. J Fam Violence. 2016;31(2):215–25.
CDC. Facts about HIV Stigma: Centers for Disease Control and Prevention; 2019. Available from: https://www.cdc.gov/hiv/basics/hiv-stigma/index.html#. [cited 2020 Sep 3].
McCleary-Sills J, Namy S, Nyoni J, Rweyemamu D, Salvatory A, Steven E. Stigma, shame and women’s limited agency in help-seeking for intimate partner violence. Glob Public Health. 2016;11(1–2):224–35.
Mahajan AP, Sayles JN, Patel VA, Remien RH, Sawires SR, Ortiz DJ, et al. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS. 2008;22(Suppl 2):S67–79.
Overstreet NM, Quinn DM. The intimate partner violence stigmatization model and barriers to help-seeking. Basic Appl Soc Psychol. 2013;35(1):109–22.
Fekete EM, Williams SL, Skinta MD. Internalised HIV-stigma, loneliness, depressive symptoms and sleep quality in people living with HIV. Psychol Health. 2018;33(3):398–415.
Rice WS, Burnham K, Mugavero MJ, James L, Atkins GC, Turan B. Association between internalized HIV-related stigma and HIV care visit adherence. J Acquir Immune Defic Syndr. 2017;76(5):482–7.
Hatcher AM, Woollett N, Pallitto CC, Mokoatle K, Stöckl H, MacPhail C, et al. Bidirectional links between HIV and intimate partner violence in pregnancy: implications for prevention of mother-to-child transmission. J Int AIDS Soc. 2014;17(1):19233.
Patel N. Figure of the week: understanding poverty in Africa. Washington DC: Brookings Institution; 2018.
Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Shamu S, Abrahams N, Temmerman M, Musekiwa A, Zarowsky C. A systematic review of African studies on intimate partner violence against pregnant women: prevalence and risk factors. PLoS One. 2011;6(3):1–9.
Onarheim KH, Iversen JH, Bloom DE. Economic benefits of investing in women’s health: a systematic review. PLoS One. 2016;11(3):1–23.
Apiribu F, Ncama BP, Joseph-Shehu E. Evidence of perpetration of intimate partner violence among HIV-positive couples: a systematic scoping review protocol. Syst Rev. 2019;8(1):159.
Baumann N. How to use the medical subject headings (MeSH). Int J Clin Pract. 2016;70(2):171–4.
Elflein J. Access to ART for HIV treatment global number 2000-2019: Statista; 2020. Available from: https://www.statista.com/statistics/265921/access-to-art-for-hiv-treatment-in-low-and-middle-income-countries/. [cited 2021 Jan 13].
Alhabib S, Nur U, Jones R. Domestic violence against women: systematic review of prevalence studies. J Fam Violence. 2010;25(4):369–82.
Bernstein M, Phillips T, Zerbe A, McIntyre JA, Brittain K, Petro G, et al. Intimate partner violence experienced by HIV-infected pregnant women in South Africa: a cross-sectional study. BMJ Open. 2016;6(8):e011999.
Hampanda KM. Intimate partner violence and HIV-positive women’s non-adherence to antiretroviral medication for the purpose of prevention of mother-to-child transmission in Lusaka, Zambia. Soc Sci Med. 2016;153:123–30.
Manongi R, Rogathi J, Sigalla G, Mushi D, Rasch V, Gammeltoft T, et al. The association between intimate partner violence and signs of depression during pregnancy in Kilimanjaro region, Northern Tanzania. J Interpers Violence. 2017;35(23-24):5797-811. https://doi.org/10.1177/0886260517724256.
Matseke G, Rodriguez VJ, Peltzer K, Jones D. Intimate partner violence among HIV positive pregnant women in South Africa. J Psychol Afr. 2016;26(3):259–66.
McNaughton Reyes HL, Maman S, Groves AK, Moodley D. Intimate partner violence and postpartum emotional distress among South African women: moderating effects of resilience and vulnerability factors. Glob Public Health. 2020;15(8):1157-67. https://doi.org/10.1080/17441692.2020.1751233.
Nyamukoho E, Mangezi W, Marimbe B, Verhey R, Chibanda D. Depression among HIV positive pregnant women in Zimbabwe: a primary health care based cross-sectional study. BMC Pregnancy Childbirth. 2019;19(1):53.
Peltzer K, Rodriguez VJ, Lee TK, Jones D. Prevalence of prenatal and postpartum depression and associated factors among HIV-infected women in public primary care in rural South Africa: a longitudinal study. AIDS Care. 2018;30(11):1372–9.
Peltzer K, Abbamonte JM, Mandell LN, Rodriguez VJ, Lee TK, Weiss SM, et al. The effect of male involvement and a prevention of mother-to-child transmission (PMTCT) intervention on depressive symptoms in perinatal HIV-infected rural south African women. Arch Womens Ment Health. 2020;23(1):101–11.
Reyes HLM, Maman S, Groves AK, Moodley D, Chen MS. A longitudinal study of the relationship between intimate partner violence and postpartum unsafe sex among newly diagnosed HIV-infected south African women. AIDS Care. 2019;31(6):707–13.
Rodriguez VJ, Cook RR, Peltzer K, Jones DL. Prevalence and psychosocial correlates of suicidal ideation among pregnant women living with HIV in Mpumalanga Province, South Africa. AIDS Care. 2017;29(5):593–7.
Shamu S, Abrahams N, Zarowsky C, Shefer T, Temmerman M. Intimate partner violence during pregnancy in Zimbabwe: a cross-sectional study of prevalence, predictors and associations with HIV. Tropical Med Int Health. 2013;18(6):696–711.
Wong M, Myer L, Zerbe A, Phillips T, Petro G, Mellins CA, et al. Depression, alcohol use, and stigma in younger versus older HIV-infected pregnant women initiating antiretroviral therapy in Cape Town, South Africa. Arch Womens Ment Health. 2017;20(1):149–59.
Peltzer K, Rodriguez VJ, Jones D. Prevalence of prenatal depression and associated factors among HIV-positive women in primary care in Mpumalanga province, South Africa. SAHARA J. 2016;13(1):60–7.
Ramlagan S, Matseke G, Rodriguez VJ, Jones DL, Peltzer K, Ruiter RAC, et al. Determinants of disclosure and non-disclosure of hiv-positive status, by pregnant women in rural South Africa. SAHARA J. 2018;15(1):155–63.
Rodriguez VJ, Shaffer A, Lee TK, Peltzer K, Weiss SM, Jones DL. Psychological and physical intimate partner violence and maternal depressive symptoms during the pre- and post-partum period among women living with HIV in rural South Africa. J Fam Violence. 2020;35(1):73–83.
Ashaba S, Kaida A, Coleman JN, Burns BF, Dunkley E, O’Neil K, et al. Psychosocial challenges facing women living with HIV during the perinatal period in rural Uganda. PLoS One. 2017;12(5):e0176256.
Turan B, Budhwani H, Fazeli PL, Browning WR, Raper JL, Mugavero MJ, et al. How does stigma affect people living with HIV? The mediating roles of internalized and anticipated HIV stigma in the effects of perceived community stigma on health and psychosocial outcomes. AIDS Behav. 2017;21(1):283–91.
Friedland BA, Sprague L, Nyblade L, Baral SD, Pulerwitz J, Gottert A, et al. Measuring intersecting stigma among key populations living with HIV: implementing the people living with HIV stigma index 2.0. J Int AIDS Soc. 2018;21:e25131.
Hatcher AM, Stöckl H, Christofides N, Woollett N, Pallitto CC, Garcia-Moreno C, et al. Mechanisms linking intimate partner violence and prevention of mother-to-child transmission of HIV: a qualitative study in South Africa. Soc Sci Med. 2016;168:130–9.
Marais A, Kuo CC, Julies R, Stein DJ, Joska JA, Zlotnick C. “If He’s Abusing You . . . the Baby Is Going to Be Affected”: HIV-Positive Pregnant Women’s Experiences of Intimate Partner Violence. Violence Against Women. 2019;25(7):839–61.
McCloskey LA, Boonzaier F, Steinbrenner SY, Hunter T. Determinants of intimate partner violence in sub-Saharan Africa: a review of prevention and intervention programs. Partn Abus. 2016;7(3):277–315.
Shamu S, Abrahams N, Temmerman M, Shefer T, Zarowsky C. “That pregnancy can bring noise into the family”: exploring intimate partner sexual violence during pregnancy in the context of HIV in Zimbabwe. PLoS One. 2012;7(8):e43148.
Hatcher AM, Smout EM, Turan JM, Christofides N, Stoeckl H. Intimate partner violence and engagement in HIV care and treatment among women: a systematic review and meta-analysis. AIDS. 2015;29(16):2183–94.
Rujumba J, Neema S, Byamugisha R, Tylleskär T, Tumwine JK, Heggenhougen HK. “Telling my husband I have HIV is too heavy to come out of my mouth”: pregnant women’s disclosure experiences and support needs following antenatal HIV testing in eastern Uganda. J Int AIDS Soc. 2012;15(2):17429.
Hatcher AM, Romito P, Odero M, Bukusi EA, Onono M, Turan JM. Social context and drivers of intimate partner violence in rural Kenya: implications for the health of pregnant women. Cult Health Sex. 2013;15(4):404–19.
Kiarie JN, Farquhar C, Richardson BA, Kabura MN, John FN, Nduati RW, et al. Domestic violence and prevention of mother-to-child transmission of HIV-1. AIDS. 2006 Aug;20(13):1763–9.
Colombini M, James C, Ndwiga C, Team I, Mayhew SH. The risks of partner violence following HIV status disclosure, and health service responses: narratives of women attending reproductive health services in Kenya. J Int AIDS Soc. 2016;19:20766.
Kennedy CE, Haberlen S, Amin A, Baggaley R, Narasimhan M. Safer disclosure of HIV serostatus for women living with HIV who experience or fear violence: a systematic review. J Int AIDS Soc. 2015;18(Suppl 5):20292.
Hewett PC, Mensch BS, Erulkar AS. Consistency in the reporting of sexual behaviour by adolescent girls in Kenya: a comparison of interviewing methods. Sex Transm Infect. 2004;80(SUPPL. 2):43–8.
Tam M, Amzel A, Phelps BR. Disclosure of HIV serostatus among pregnant and postpartum women in sub-Saharan Africa: a systematic review. AIDS Care. 2015;27(4):436–50.
Illangasekare SL, Burke JG, McDonnell KA, Gielen AC. The impact of intimate partner violence, substance use, and HIV on depressive symptoms among abused low-income urban women. J Interpers Violence. 2013;28(14):2831–48.
Kayibanda JF, Bitera R, Alary M. Violence toward women, men’s sexual risk factors, and HIV infection among women: findings from a national household survey in Rwanda. J Acquir Immune Defic Syndr. 2012;59(3):300–7.
Hampanda K. Vertical transmission of HIV in sub-Saharan Africa: applying theoretical frameworks to understand social barriers to PMTCT. ISRN Infect Dis. 2013;2013(September 2012):1–5.
WHO. No responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines; Geneva, World Health Organisation; 2013. Available from: https://apps.who.int/iris/bitstream/handle/10665/85240/9789241548595_eng.pdf;jsessionid=1450BFD224BF3E93077EF7517FB150B6?sequence=1. [cited 2020 Aug 24].
Joyner K. Relevance and feasibility of WHO recommendations for intimate partner violence care in south African primary health settings. Afr Saf Promot. 2013;11(2):21–7.
Acknowledgements
I would not have been able to accomplish this feat without the support of my family, friends, global health teachers and peers. Special thanks to my mother, Ambassador Jackline Yonga, for continuously listening to my successes and frustrations as I worked through this last summer. I would also like to take the time to thank my dear friend Nikita Hukerikar for always being a sounding board for doubts and worries.
Funding
The authors received no financial support for the research and authorship of this article. A personal grant from the University of Bergen (Dr Kristine Husøy Onarheim) covered the publication fee.
Author information
Authors and Affiliations
Contributions
Ashley Yonga (Author 1) undertook data extraction, wrote the main manuscript text, and prepared images and tables. All authors edited, reviewed, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable as manuscript does not report on any animal or human data or tissue.
Consent for publication
Not applicable as manuscript does not report on any animal or human data or tissue.
Competing interests
The authors have no competing interests as defined by BMC, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yonga, A.M., Kiss, L. & Onarheim, K.H. A systematic review of the effects of intimate partner violence on HIV-positive pregnant women in sub-Saharan Africa. BMC Public Health 22, 220 (2022). https://doi.org/10.1186/s12889-022-12619-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-022-12619-w