
Abstract
Background
To throw light on the under-researched association between socioeconomic position (SEP) and health in Cuba, this study examined SEP gradients in health and their underlying mechanisms among urban Cuban adults aged 18–65.
Methods
By applying linear regressions to data from the 2010 National Survey on Risk Factors and Chronic Diseases, the analysis explored the SEP-health gradient along three SEP dimensions − education, occupation, and skin colour − using ten health measures: self-reported health (SRH), general and abdominal obesity, hypertension, high glucose, high cholesterol, high triglycerides, low high-density lipoprotein cholesterol, metabolic syndrome, and cumulative risk factors. Regressions also included behaviours and health-related risk perceptions (tobacco and alcohol consumption, diet, physical activity, and risk-related behaviours). It thus investigated the SEP-health gradient and its underlying mechanisms via both behaviours and health-related risk perceptions.
Results
Once controlling for gender, age, marital status, region and provincial dummies, the analysis detected educational gradients in SRH (estimated coefficient [95% CI]: middle-level education = 3.535 [1.329, 5.741], p < 0.01; high-level education = 5.249 [3.050, 7.448], p < 0.01) that are partially explainable by both health-affecting behaviours (tobacco and alcohol consumption, diet, physical and sedentary activity) and risk perceptions. Using objective measures of health, however, it found no SEP-health gradients other than hypertension among people identified as having Black skin color (adjusted for demographic variables, 0.060 [0.018, 0.101], p < 0.01) and high cholesterol among those identified as having Mulatto or Mestizo skin color (adjusted for demographic variables, − 0.066 [− 0.098, − 0.033], p < 0.01).
Conclusions
In terms of objective health measures, the study provides minimal evidence for an SEP-health gradient in Cuba, results primarily attributable to the country’s universal healthcare system − which offers full coverage and access and affordable medications − and its highly developed education system.
Similar content being viewed by others

Background
Although the social and medical sciences have largely established a positive relation (i.e., gradient) between socioeconomic position (SEP) and health in Europe [1,2,3], the US [4,5,6,7,8], and other high-income countries [9,10,11,12], the evidence in low and middle-income countries (LMICs) is less clear, with some studies identifying positive SEP-health gradients [13,14,15] whilst some showing none [16,17,18,19]. One possible reason for this inconsistency in the results in LMICs is that socioeconomic disparities within nations vary substantially among countries. At the same time, despite much effort expended on identifying the SEP-health gradient, its underlying mechanisms remain unclear. Yet in order to devise efficient policies to reduce health inequalities across different SEP dimensions, policy-makers need to fully understand the nature of this gradient and its underlying pathways.
Cuba offers a particularly interesting case for assessing the SEP-health gradient because despite stable economic growth and an egalitarian healthcare system, it has a rapidly ageing population and a substantial burden of noncommunicable chronic diseases (NCDs). One concern is that its near tripling of per capita gross domestic product (GDP) during 2001–2010 [20] was accompanied by an increase in income inequality that does not appear to be a function of educational inequality [21]. In addition, although its egalitarian healthcare system offers high capacity primary care, universal coverage and access, affordable medications, and robust clinical registries [22], the nation is experiencing an increase in NCDs [23], with an overall burden of blood pressure-related premature deaths of around 40% [22]. At the same time, the nation is ageing so rapidly that by 2020, 25% of its total population is likely to be 60 and older [24].
This study thus uses a combination of self-reported health (SRH), blood-based biomarkers, health-related behaviours, and risk perceptions to determine the presence of SEP-health gradients in Cuba and explore the mechanisms that may underlie the SEP impact on health. To ensure an objective assessment of disease risk, it employs both subjective and objective health measures (biomarkers), and adds the SEP dimensions of occupation and skin colour to the commonly used factors of income and education.
Methods
Study design and data
The data are taken from the 2010 National Survey on Risk Factors and Chronic Diseases (NSRFCD), administered collaboratively by Cuba’s National Institute of Hygiene, Epidemiology and Microbiology; National Statistics Bureau, and Nutrition and Food Hygiene Institute [25]. This nationally representative survey, which maintained all samples under strict quality control, applied a stratified multistage cluster sampling design covering 14 of Cuba’s provinces and the Isle of Youth special municipality. Although the survey was administered in all urban areas in 1995 (NSRFCD I) and 2001 (NSRFCD II) and in both urban and rural areas in 2010 (NSRFCD III), only the 2010 wave collected blood biomarker data and was thus used as the basis for present study. A total of 7915 individuals aged 15+ were surveyed in 2010.
Health outcome measures
To combine the advantages of subjective and objective health indicators, we included SRH, individual biomarkers and composite measures of cardiometabolic disease/metabolic function. As the main measure of subjective health we used SRH, which encompasses not only mental and physical health but subjective experience of acute and chronic diseases and overall feelings of well-being [26]. SRH is generally considered a good predictor of mortality [27]. Our SRH measure is based on the following item: “To help people describe how good or bad their state of health is, we have drawn a scale similar to a thermometer, which is marked with a 100 for the best state of health that can be imagined and with a 0 for the worst state of health that you can imagine. We would like you to indicate on this scale with an arrow, in your opinion, how good or bad your health status is today”. Regarding objective health, we introduced physical measurements and blood-based biomarkers that directly relate to major chronic conditions such as general obesity, central obesity, high blood pressure, diabetes and coronary heart diseases. Specifically, the individual biomarker variables included body mass index (BMI), waist circumference (WC), blood pressure, total cholesterol, high-density lipoprotein (HDL) cholesterol and triglycerides. The two composite indicators included metabolic syndrome and cumulative risk factors.
Our binary health measures are better suited than continuous measures to a capture health state when both high and low values of a biomarkers as associated with a health risk [28]. Furthermore, all the markers in our analysis have well-established cutoff points denoting clinical risks. Finally, binary measures are robust to outliers which is particularly relevant when sample size are relatively small [28]. In our analysis, biomarker values were categorized into binary ones using cut-off points recommended by the International Diabetes Federation (IDF) or in other published studies [13, 18, 29, 30], with separate cut-off points for men and women where appropriate (see Table 1). In particular, metabolic syndrome was defined as having high abdominal girth and at least two of the following risk factors: diabetes, high triglycerides, low HDL cholesterol, and hypertension [18]. It was coded in a binary variable having a value equal to 1 if metabolic syndrome was present; 0 otherwise. Cumulative risk factors was coded in a binary variable equal to 1 if at least one cardiovascular disease risk factor was present (high waist circumference, diabetes, hypertension, high triglycerides, and high cholesterol ratio); 0 otherwise. Table 1 provides the cut-off points for each individual biomarker and definitions of cardiometabolic risk.
SEP measures
Since a variety of socioeconomic variables, including education, income, and occupation, along with self-assessed skin color, among others, show similar associations with health, a broader underlying dimension of social stratification or social ordering is needed when assessing the relation between SEP and health. Furthermore, different SEP measures may have differing effects on certain health outcomes [31]. Thus, existing studies on this topic put great emphasis on the multidimensional nature of SEP [31,32,33]. In accordance with this literature, our paper captures three important SEP dimensions, namely education, occupation and skin colour. Specifically, education is measured on a 3-point scale (low: illiterate/primary school; medium: secondary school/qualified worker/technical school; high: high school/university), with two dummy variables for “high” versus “medium,” with “low” as the reference. In addition, occupation is measured on a 4-point scale (1: unemployed; 2: housewife/husband; 3: self-employed; 4: state worker) and recoded as a set of dummy variables with “unemployed” as the reference. Contrary to other SEP dimensions, there is less of an ordering in the occupational categories – especially in the Cuban context. For example, self-employment is a common form of private entrepreneurial activity in Cuba [34] and it provides a viable alternative to many former State sector employees who suffered job losses or have been temporarily place on paid leave due to state-owned enterprises’ restructuring [35]. Since 2009 the share of workers in the state sector has declined sharply whilst the non-state sectors’ share has increased dramatically. The rate of self-employed workers to total employed workers has increased from 2.83% in 2009 to 8.25% in 2012 [36]. In addition, Cuba’s official unemployment rate has been remarkably low in comparison to other economies, including all those in Latin America. However, as Hernández-Catá [37] have emphasized: “Given the peculiar characteristics of the Cuban economy, the conventionally defined unemployment rate is a very bad indicator of labor market conditions” (p. 2). This is attributable to the failure of taking disguised unemployment and discouraged workers into account [37]. Skin colour is measured on a 3-point scale (1: people identified as having White skin color; 2: people identified as having Mulatto or Mestizo skin colour; 3: people identified as having Black skin colour) and then converted into a set of dummy variables with “those identified as having White skin colour” as the reference. It is important to note that skin colour refers to an individual’s perception of his or her skin colour. Although skin colour identity can evolve within one individual, it is a characteristic less amenable to change than the other SEP measures.
Additional SEP measure
Income is measured as monthly income in Cuban pesos (CUP). This indicator was included because, despite legitimate concerns about NSRFCD income data reliability (around 43% of missing values), it is widely used in evaluating SEP-health gradients. Besides the questionable reliability of the NSRFCD income data, such surveyed income measures have somewhat less relevance in the Cuban setting than in other countries, especially as relatively low nominal salaries are offset by subsidized healthcare, education, transportation and social services, and are supplemented by remittances from abroad [36]. Nevertheless, inflation, monetary dualism, gradual price liberalization (especially with regards to food and agricultural products), and the partial elimination of state subsidies have all contributed to the decline of the real purchasing power for most Cuban households [36].
Behavioural and risk perception measures
One component of research on the SEP-health gradient is the mechanisms underlying this gradient, that is the behavioural characteristics –health-enhancing behaviours such as healthy diets and physical exercise or health-compromising activities such as smoking or drinking alcohol [13] – which may drive the association between SEP and health. For example, income shocks are detrimental to individual lifestyles that include smoking and social drinking [38,39,40,41]. A higher level of education can positively affect individual health status mainly because one of the likely benefits of higher education is general knowledge (and in particular medical knowledge) that helps individuals become more health-conscious and take preventive actions [42, 43]. In order to identify the underlying mechanisms through which the different dimensions of SEP operate on health, the analysis explored three types of health-affecting behaviours:
-
(1)
Tobacco and alcohol consumption: measured by responses to two survey questions: “Do you currently smoke any tobacco products, such as cigarettes, cigars or pipes?” (1: yes; 0: no); “Have you consumed any drinks that contain alcohol, such as beer, wine, moonshine, cider or others during the previous month?” (1: yes; 0: no).
-
(2)
Diet: measured by five indicators: (i) frequency of eating fruits and vegetables: “On a typical week, how many days do you eat fruits/vegetables?” (1: 0–2 days; 2: 3–4 days; 3: 5–7 days); (ii) meals away from home during a week: “On a typical week, how many meals do you have outside the home?” (times/week); (iii) type of cooking oil consumed: “What kind of oil do you usually use at home to prepare foods?” (1: vegetable oil; 0: other); (iv) eating breakfast: “Are you used to having breakfast?” (1: yes, every day; 2: not always; 3: no); (v) salt consumption: “Do you add salt to your meals after they are cooked?” (1: yes; 2: sometimes; 3: no).
-
(3)
Physical activity (PA) versus sedentary activity (SA): PA was measured by responses to three questions: “Does your job demand any kind of intensity physical activity that leads to an important acceleration of breathing or heart rate?” (1: yes; 0: no); “Do you walk or ride a bicycle for at least 10 consecutive minutes when going about” (1: yes; 0: no); “In your free time, do you practice any kind of moderate intensity activity that involves a light acceleration of breathing or heart rate?” (1: yes; 0: no). SA was measured by responses to one question: “How long do you spend sitting or lying back on a typical day?” (hours/day).
The study also assessed risk perceptions for eight such activities:
-
Risk-related behaviours: (i) smoking, (ii) drinking alcohol occasionally, (iii) remaining where smokers are present even though you do not smoke, (iv) doing little physical exercise, (v) eating few fruits, (vi) adding salt to cooked food, (vii) eating few vegetables, (viii) being overweight, and (ix) eating pork fat.
-
Measurement: respondent rankings along a 4-point scale: 1: no health risk; 2: little health risk; 3: moderate health risk; 4: substantial health risk:
Covariates
As highlighted by Fuchs [44], health deteriorates with age, which is a fundamental fact of biology. Furthermore, gender difference in life expectancy has been discernable in almost every country [44]. In our health outcomes estimations we therefore introduced age and gender. In addition, given that marital status might affect household production of health caregiving and demand for health [44], we controlled for marital status in our analyses. To capture possible geographical heterogeneities in different health outcomes, we also introduced urban and provincial controls. Following these existing studies [31, 44, 45], our models included the following general demographics as analytic covariates: (i) gender (1: male; 0: female); (ii) age; (iii) marital status (three binary variables capturing singles, married/cohabiting individuals, divorced/separated/widowed individuals; with singles as the reference category); (iv) an urban dummy (1: urban; 0: rural); and (v) a provincial dummy, with Pinar del Río as the reference (see Table 1 for the descriptive statistics).
Statistical analysis
Since we focused on different dimensions of cardiometabolic risks, we adopted dichotomous variables in our regression analysis, which have been used extensively in existing studies on identifying SEP-health gradients [13, 18, 29]. After first applying an ordinary least squares (OLS) model to assess the SEP-SRH gradient, the analysis used linear probability models (LPMs) to estimate the SEP-health gradients based on individual and composite biomarkers (all performed using STATA/SE version 14) [46]. LPMs were deemed the most suitable because, unlike nonlinear probit or logit models whose maximum likelihood estimations are inconsistent in the presence of heteroscedasticity [47], they provide consistent estimates despite heteroscedasticity of the error term, as well as easily interpretable coefficients. The models used to estimate the SEP-health gradients contained different covariate sets: Whereas model 1 included gender, age, marital status, region and provincial dummy variables, models 2 and 3 stepwise added in the three SEP dimensions and health-related behaviours, respectively. Model 4 then included all the model 1 variables plus risk perceptions, after which model 5 controlled for all the covariates (including gender, age, marital status, region, provincial dummy variables, tobacco and alcohol consumption, diet, PA, and risk-related behaviours) simultaneously. The samples were weighted to ensure nationally representative estimates.
Results
Study population characteristics
This analytic sample was restricted to adults aged 18–65 (SRH, n = 4124; general obesity, n = 3741; abdominal obesity, n = 3764; hypertension: 3757; high glucose, n = 1009; high total cholesterol, n = 1018, high triglycerides, n = 1008; low high-density lipoprotein cholesterol, n = 246; metabolic syndrome, n = 244 and cardiovascular disease (CVD) risk factor, n = 234) for which complete demographic, SEP, health-related behaviour, and biomarker information was available.
As shown in Table 2, the mean SRH was around 87. The average values of BMI and WC were 25.4 kg/m2 and 83.8 cm, respectively, and the rates of general obesity and abdominal obesity were 16.1 and 45.3%, respectively. For cardiometabolic risks, the prevalence rates of hypertension was 17.5%. Approximately 16% of Cubans have high total cholesterol. Interestingly, however, about 57% of Cubans have low levels of HDL cholesterol. Thus, although especially NCDs are on the rise in Cuba, the general picture one gets from these set of indicators is that the Cuban population is healthier (with the exception of low HDL cholesterol) than the American. As can be seen in Table 3, there is some variation in the SEP variables used in our analysis, especially with regards to education: 11% illiterate or primary school, 27% secondary school, 2% qualified worker, 19% technical school, 28% high school, and 14% university. Variation in occupation is substantially lower, with over 64% classified as state workers. Nevertheless, about 9% of the sample are self-employed. With regards to skin colour, being White was the majority (65.7%), compared with being Mulatto/Mestizo and Black, with proportions of 24.6 and 9.7%, respectively. Regarding health-related behaviours, approximately 25.5 and 53.2% of Cubans were smoke tobacco and consume alcohol, respectively (Table 4). 26.5 and 33.1% of Cubans ate fruits and vegetables 5–7 days per week, respectively. 90.0% of Cubans reported smoking and 55.6% reported drinking alcohol occasionally as a substantial health risk. However, merely 36.3 and 41.4% of Cubans considered eating few fruits and vegetables, respectively, as a substantial health risk.
SEP and health gradient: the three dimensions
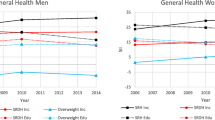
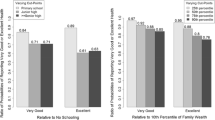
Table 5 shows the results of the SEP-health gradients with the adjustment of demographic characteristics. Table A1 provides a summary of associations between SEP and specific health outcomes. With general demographics and the three SEP dimensions controlled for (estimated coefficient [95% CI]: medium level education = 3.535 [1.329, 5.741], p < 0.01; high-level education = 5.249 [3.050, 7.448], p < 0.01), a better SRH was uniformly associated with a higher educational level. No such link emerged, however, between education and objective health outcomes. Both these latter and SRH also appeared unrelated to occupation, except in the case of general obesity, which was likely to be higher for a housewife or husband than for an unemployed worker. Whereas people that identified as having Black skin colour (relative to those identified as having White skin colour) was correlated with a higher probability of hypertension (0.060 [0.018, 0.101], p < 0.01), those identified as having Mulatto or Mestizo skin colour lowered the likelihood of high cholesterol (− 0.066, [− 0.098, − 0.033], p < 0.01). No associations were observable, however, between objective health outcomes and income (with general demographics controlled for, Table 5), although a better SRH did correlate with a higher monthly income (see Supplementary Materials Table A2 Panel A). We did not observe any income-health gradients when using both individual and composite objective health measures (see Supplementary Materials Tables A2-A4). Once general demographics were controlled for, all SEP dimensions remained uncorrelated with the two composite indicators of health outcomes, namely metabolic syndrome and cumulative risk factors.
SEP and the health gradient: underlying mechanisms
The exploration of mechanisms underlying SEP’s impact on health included individual behaviours (tobacco and alcohol consumption, diet, physical and sedentary activities) and risk perceptions (see Table 6). One notable outcome was that although the SRH gradient in high-level education became flatter once behavioural variables were controlled for, the addition of health-related risk perceptions had little effect on the gradient. In addition, although controlling for health-affecting behaviours, risk perceptions, or even both together diminished the hypertension differences regarding people identified as having Black skin colour, the addition of these behaviours partially accounted for the differences in high total cholesterol (especially for those identified as having Mulatto or Mestizo skin colour), which health-related risk perceptions did not.
Discussion
This study was a first attempt to combine both subjective and objective health measures to assess the SEP-health gradient in Cuba and identify its underlying mechanisms. Although the analysis confirmed the presence of education and income gradients in SRH − both partially explainable by health-affecting behaviours and risk perceptions − the use of objective health measures generally failed to identify any SEP-health gradients except for differences based on skin colour in hypertension and high cholesterol.
The analysis did, however, reveal significant discrepancies in the SEP-health gradient depending on whether the health measures used were subjective or objective. Hence, although SRH is acknowledged to be a good predictor of mortality following medical care [42], a certain amount of caution is warranted when using subjective measures to determine the SEP-health gradient. On the other hand, the education/income-SRH gradients identified resemble those observed in other high-income countries [2, 48, 49], and their mediation by health-affecting behaviours is mirrored in other Western studies [38, 39], indicating that the SEP-health gradient is partially attributable to smoking and social drinking. In one Costa Rican study, for example, using SRH as a measure indicated the presence of an SEP-health gradient but employing CVD risk factors like diabetes and total cholesterol did not [18]. Similarly, in a Mexican study, the SEP-health gradients identified using SRH vanished with the use of objective health indicators like obesity [29]. A study for China even documented that although higher SEPs were associated with better SRH [30], they were uncorrelated with objective health measures like obesity and hypertension [16].
Interestingly, the rates of general obesity and abdominal obesity (15.4 and 44.1%) were quite similar to the findings of Nie et al. [45] for Cuba aged 18+. For cardiometabolic risks, the rate of hypertension (16.7%) was much lower than that among U.S. adults (the age-adjusted prevalence of hypertension among the US adults aged 18 and over was 29.1% in 2011/2012 [50]). Approximately 15% of Cubans have high total cholesterol, which is substantially lower than that of Americans, with the prevalence of about 43% [51]. However, about 57% of Cubans have low levels of HDL cholesterol, a higher proportion than that in the US, with a prevalence of around 20% [51]. The findings of the present study contrast sharply with US evidence of Whites having generally more favorable health profiles than other racial/ethnic groups, especially Blacks, who have a higher risk of obesity, hypertension, and diabetes [52, 53]. Although the evidence reported here for Cuba does show people identified as having Black skin colour having a significantly higher probability of hypertension (relative to those identified as having White skin colour), this result contradicts a past study of the urban population of Cienfuegos in central Cuba, which observed no self-assessed skin colour differences in hypertension [54].
The nonexistence of an SEP-health gradient in Cuba could be attributable to the fact that Cubans have benefited from a universal health care system that focuses particularly on primary care and preventive medicine [55], especially given the substantial increase in coverage rate from 61.2% in 1979 to 75.9% in 1989 [56] to 98.2% in 2009 [57]. Its absence could also be influenced by a very well-developed educational system and a generally inclusive society in which racial discrimination is less of an issue than in many other countries.
Admittedly the current study was limited by uncertainties of the income variable (43% of values missing from the data), which led to a substantial difference between the NSRFCD-based average monthly salary of around 227 CUP and the official 2010 number of 448 CUP [58]. In fact, in one assessment of Nie et al. [45] the extent to which the NSRFCD income data follow a Benford distribution [59] indicated clear rejection of this assumption with a chi-square of 2775, whose very large magnitude itself raises serious concerns about data reliability. Nonetheless, the NSRFCD is not only the most recent nationally representative dataset for Cuba that contains detailed information on health outcomes, but one that employs vigorous quality assurance and control procedures.
The current investigation was also at times hindered by relatively small sample sizes (e.g. those for HDL cholesterol and composite biomarkers), which limited the explanatory power of the models. It was, however, the first attempt to explore the SEP-health gradient and its underlying mechanisms in Cuba using both subjective and objective health measures. Two additional limitations were the age of the data and the cross-sectional setting, respectively, which prevented the capture of Cuba’s significant economic changes over the last decade and the drawing of conclusions on causality or temporality [60]. Further studies are thus needed to examine the SEP-health gradients over time using longitudinal data sets.
Conclusions
Overall, this study offers little evidence of an SEP-health gradient in Cuba, especially as it relates to objective measures of health. Its findings do, however, underscore the importance of incorporating biological indicators, especially for societies experiencing serious health problems that may not always translate into a correlation between self-assessments of personal health and objective health measures.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CVD:
-
Cardiovascular disease
- CUP:
-
Cuban pesos
- GDP:
-
Gross domestic product
- HDL:
-
High-density lipoprotein
- LMICs:
-
Low and middle-income countries
- LPMs:
-
Linear probability models
- NCDs:
-
Non-communicable chronic diseases
- NSRFCD:
-
National Survey on Risk Factors and Chronic Diseases
- OLS:
-
Ordinary least squares
- PA:
-
Physical activity
- SEP:
-
Socioeconomic position
- SRH:
-
Self-reported health
- SA:
-
Sedentary activity
- WC:
-
Waist circumference
References
DiPrete TA, Burik CAP, Koellinger PD. Genetic instrumental variable regression: explaining socioeconomic and health outcomes in nonexperimental data. Proc Natl Acad Sci. 2018;115(22):E4970.
Frijters P, Haisken-DeNew JP, Shields MA. The causal effect of income on health: evidence from German reunification. J Health Econ. 2005;24(5):997–1017.
Stringhini S, Carmeli C, Jokela M, Avendaño M, Muennig P, Guida F, Ricceri F, d'Errico A, Barros H, Bochud M, et al. Socioeconomic status and the 25×25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet. 2017;389(10075):1229–37.
Jia P, Xierali IM. Disparities in Patterns of Health Care Travel Among Inpatients Diagnosed With Congestive Heart Failure, Florida, 2011. Preventing Chronic Disease, 12, E150.
Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M, Posner S. Socioeconomic status in health research: one size does not fit all. JAMA. 2005;294(22):2879–88.
Smith JP. The impact of socioeconomic status on health over the life-course. J Hum Resour. 2007;42(4):739–64.
Williams DR, Mohammed SA, Leavell J, Collins C. Race, socioeconomic status, and health: complexities, ongoing challenges, and research opportunities. Ann N Y Acad Sci. 2010;1186(1):69–101.
Zhang Q, Wang Y. Using concentration index to study changes in socio-economic inequality of overweight among US adolescents between 1971 and 2002. Int J Epidemiol. 2007;36(4):916–25.
Präg P, Mills MC, Wittek R. Subjective socioeconomic status and health in cross-national comparison. Soc Sci Med. 2016;149:84–92.
Gunasekara F, Carter K, Liu I, Richardson K, Blakely T. The relationship between income and health using longitudinal data from New Zealand. J Epidemiol Commun H. 2011;66(6):e12.
Raphael D, Labonté R, Colman R, Hayward K, Torgerson R, Macdonald J. Income and health in Canada: research gaps and future opportunities. Can J Public Health. 2006;97(S3):S16–23.
Shibuya K, Hashimoto H, Yano E. Individual income, income distribution, and self rated health in Japan: cross sectional analysis of national representative sample. BMJ Clin Res. 2002;324(7328):16–9.
Brasher MS, George LK, Shi X, Yin Z, Zeng Y. Incorporating biomarkers into the study of socio-economic status and health among older adults in China. SSM Popul Health. 2017;3:577–85.
Fichera E, Savage D. Income and health in Tanzania. An Instrumental Variable Approach. World Dev. 2015;66:500–15.
Jia P, Anderson JD, Leitner M, Rheingans R. High-Resolution Spatial Distribution and Estimation of Access to Improved Sanitation in Kenya. PLoS ONE. 2016;11(7):e0158490.
Bakkeli NZ. Income inequality and health in China: a panel data analysis. Soc Sci Med. 2016;157:39–47.
Monteiro CA, Moura EC, Conde WL, Popkin BM. Socioeconomic status and obesity in adult populations of developing countries: a review. Bull World Health Organ. 2004;82(12):940–6.
Rosero-Bixby L, Dow WH. Surprising SES gradients in mortality, health, and biomarkers in a Latin American population of adults. J Gerontol. 2009;64B(1):105–17.
Zimmer Z, Chayovan N, Lin H-S, Natividad J. How indicators of socioeconomic status relate to physical functioning of older adults in three Asian societies. Res Aging. 2004;26(2):224–58.
World Bank: World Bank national accounts data, and OECD National Accounts data files. In.; 2016.
de la Fuente A. Race and income inequality in contemporary Cuba. NACLA Rep Am. 2011;44(4):30–3.
Campbell NRC, Gonzalez YV, Ordunez P. The burden of hypertension in Cuba. Lancet Public Health. 2019;4(2):e79–80.
JdJ LR. Aging and dementia: Implications for Cuba's research community, public health and society. MEDICC Rev. 2013;15:54–9.
Ministry of Public Health. Statistical Yearbook, MINSAP, Cuba. Havana: Ministry of Public Health (CU); 2009.
Díaz Sánchez ME, Jiménez S, García RG, Bonet M, Wong I. Overweight, obesity, central adiposity and associated chronic diseases in Cuban adults. MEDICC Rev. 2009;20(2):23–8.
Xie S, Mo T. The impact of education on health in China. China Econ Rev. 2014;29:1–18.
Hoffmann R, Kröger H, Pakpahan E. Pathways between socioeconomic status and health: does health selection or social causation dominate in Europe? Adv Life Course Res. 2018;36:23–36.
Goldman N, Turra CM, Rosero-Bixby L, Weir D, Crimmins E. Do biological measures mediate the relationship between education and health: a comparative study. Soc Sci Med. 2011;72(2):307–15.
Smith KV, Goldman N. Socioeconomic differences in health among older adults in Mexico. Soc Sci Med. 2007;65(7):1372–85.
Yang W, Kanavos P. The less healthy urban population: income-related health inequality in China. BMC Public Health. 2012;12(1):804.
Cutler DM, Lleras-Muney A, Vogl T. Socioeconomic status and health: dimensions and mechanisms. In: Glied S, Smith P, editors. The Oxford Handbook of Health Economics. New York: Oxford University Press; 2011.
Deaton A, Paxson C. Mortality, income, and income inequality over time in Britain and the United States. In: Wise DA, editor. Perspectives on the Economics of Aging. Chicago: University of Chicago Press; 2004.
Torssander J, Erikson R. Stratification and mortality – a comparison of education, class, status, and income. Eur Sociol Rev. 2009;26(4):465–74.
Arzeni S. Entrepreneurship in Eastern Europe: a critical view. In: Brzezinski H, Fritsch M, editors. The Economic Impact of New Firms in Post-Socialist Countries: Bottom-up Transformation in Eastern Europe. Cheltenham and Vermont: Edward Elgar Publishing; 1996.
Smallbone D, Welter F. The distinctiveness of entrepreneurship in transition economies. Small Bus Econ. 2001;16(4):249–62.
GonzÁLez-Corzo MA, Justo O. Cuba’s emerging self-employed entrepreneurs: recent development and prospects for the future. J Dev Entrep. 2014;19(3):1450015.
Hernández-Catá E. Why is Cuba’s unemployment rate so low? Or is it really that low? In: The Conference of the American Economic Association. Atlanta: The American Economic Association; 2019.
Apouey B, Clark AE. Winning big but feeling no better? The effect of lottery prizes on physical and mental health. Health Econ. 2014;24(5):516–38.
van Kippersluis H, Galama TJ. Wealth and health behavior: testing the concept of a health cost. Eur Econ Rev. 2014;72:197–220.
Kaiser M, Bauer JM, Sousa-Poza A. Does unemployment lead to a less healthy lifestyle? Appl Econ Lett. 2017;24(12):815–9.
Kaiser M, Reutter M, Sousa-Poza A, Strohmaier K. Smoking and local unemployment: evidence from Germany. Econ Hum Biol. 2018;29:138–47.
Costa-Font J, Hernández-Quevedo C. Measuring inequalities in health: what do we know? What do we need to know? Health Policy. 2012;106(2):195–206.
Martin MA, Frisco ML, Nau C, Burnett K. Social stratification and adolescent overweight in the United States: how income and educational resources matter across families and schools. Soc Sci Med. 2012;74(4):597–606.
Fuchs VR. Reflections on the socio-economic correlates of health. J Health Econ. 2004;23(4):653–61.
Nie P, Alfonso Leon A, Díaz Sánchez ME, Sousa-Poza A. The rise in obesity in Cuba from 2001 to 2010: An analysis of National Survey on risk factors and chronic diseases data. Econ Hum Biol. 2018(28):1–13.
StataCorp. Stata Statistical Software: Release 14. College Station: StataCorp LP; 2015.
Hellevik O. Linear versus logistic regression when the dependent variable is a dichotomy. Qual Quant. 2009;43(1):59–74.
Ovd K, Lüschen G, Cockerham WC, Siegrist J. Socioeconomic status and health among the aged in the United States and Germany: a comparative cross-sectional study. Soc Sci Med. 2003;57(9):1643–52.
Lindahl M. Estimating the effect of income on health and mortality using lottery prizes as an exogenous source of variation in income. J Hum Resour. 2005;40(1):144–68.
Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. In: NCHS data brief, no 133. Hyattsville: National Center for Health Statistics. p. 2013.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–e322.
Nguyen AB, Moser R, Chou WY. Race and health profiles in the United States: an examination of the social gradient through the 2009 CHIS adult survey. Public Health. 2014;128(12):1076–86.
Wang Y, Beydoun MA, Liang L, Caballero B, Kumanyika SK. Will all Americans become overweight or obese? Estimating the progression and cost of the US obesity epidemic. Obesity. 2008;16(10):2323–30.
Ordúñez P, Kaufman JS, Benet M, Morejon A, Silva LC, Shoham DA, Cooper RS. Blacks and whites in Cuba have equal prevalence of hypertension: confirmation from a new population survey. BMC Public Health. 2013;13(1):169.
Armas Rojas N, Dobell E, Lacey B, Varona-Pérez P, Burrett JA, Lorenzo-Vázquez E, Calderón Martínez M, Sherliker P, Bess Constantén S, Morales Rigau JM, et al. Burden of hypertension and associated risks for cardiovascular mortality in Cuba: a prospective cohort study. Lancet Public Health. 2019;4(2):e107–15.
Barceló A, Díaz O, Norat T, Mateo de Acosta O. Diabetes mellitus en Cuba (1979-1989), I: variaciones relacionadas con edad y sexo. Rev Cuba Endocrinol. 1993(4):59–66.
Arnold Y, Castelo L, Licea MM. Comportamiento de indicadores epidemiológicos de morbilidad por diabetes mellitus en Cuba,1998–2009. Rev Cuba Endocrinol. 2012;16:6.
National Office of Statistics. Cuba average monthly salary 2008-2017. New York: Trading Economics. p. 2017.
Judge G, Schechter L. Detecting problems in survey data using Benford’s law. J Hum Resour. 2009;44(1):1–24.
McLaren L. Socioeconomic status and obesity. Epidemiol Rev. 2007;29(1):29–48.
Acknowledgments
We thank the staff at the various related institutions that provided us with the NSRFCD data, including the National Institute of Hygiene, Epidemiology and Microbiology; the National Statistics Bureau; and the Nutrition and Food Hygiene Institute. We would also like to thank the editor and two reviewers for valuable comments. The findings, interpretations, and conclusions expressed in this paper are entirely those of the authors.
Funding
This work was supported by the National Natural Science Foundation of China (grant number 71804142), the Start-Up Fund for Young Talent Support Plan (grant number 7121182501) and the research grant from the US-based Chinese Medical Board (grant number 16–262). The funding agencies had no further roles in the design of the study, the collection, analysis, and interpretation of data, or the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
PN conceptualized the study, PN, LLD, AAL and ASP drafted the manuscript, and PN and LLD took responsibility for data handling and statistical analysis. PN, LLD, AAL, ASP, HX, PJ, LW, MEDS and YFW contributed to the study conception and design, interpretation of data, critical revision of the manuscript, and study supervision. All authors read and approved the final manuscript. Dr. Peng Nie (PN) is an Associate Editor of BMC Public Health.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table A1.
Summary of SES and health gradients among Cuban aged 18–65. Table A2. OLS/linear probability estimates in SRH, obesity and hypertension among Cuban aged 18–65: NSRFCD 2010. Table A3. Linear probability estimates in biomarkers among Cuban aged 18–65: NSRFCD 2010. Table A4. Linear probability estimates in composite health indicators among Cuban aged 18–65: NSRFCD 2010
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nie, P., Ding, L., Sousa-Poza, A. et al. Socioeconomic position and the health gradient in Cuba: dimensions and mechanisms. BMC Public Health 20, 866 (2020). https://doi.org/10.1186/s12889-020-08980-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-020-08980-3