
Abstract
Background
In Brazil, 70% of the population depends on the public healthcare system. Since early detection is considered crucial, this study aimed to evaluate temporal changes in breast cancer screening coverage provided under the Brazilian National Health Service (SUS) according to the different regions of the country between 2008 and 2017.
Methods
This ecological study analyzed data on breast cancer screening within the SUS for women aged 50–69 years. Coverage was calculated from the ratio between the number of screening tests conducted and the expected number for the target population. Joinpoint regression analysis was used to calculate annual percent changes (APC) in coverage.
Results
Around 19 million mammograms were performed in 50–69-year old women within the SUS between 2008 and 2016. The estimated APC indicates that breast cancer screening coverage increased by 14.5% annually in Brazil between 2008 and 2012 (p < 0.01), with figures stabilizing between 2012 and 2017 as shown by an APC of − 0.4% (p = 0.3). In the five geographic regions of the country, the APC initially increased, then stabilized in the north, northeast and southeast and decreased in the south and Midwest. Of the 26 states, coverage increased in seven and remained stable in six. In the other 13, there was an initial increase followed by stabilization in 11, and a reduction in coverage in two. In the Federal District, coverage remained stable throughout the study period.
Conclusion
Evaluation of the temporal changes in breast cancer screening coverage provided under the Brazilian National Health Service revealed an initial increase, confirming that public policies were effective, although insufficient to ensure organized screening. There appears to be a lack of uniformity between the different regions and states and this situation is highlighted in the final 5-year period, with the APC reflecting stabilization of breast cancer screening coverage.
Similar content being viewed by others


Background
Several randomized clinical trials conducted between the 1960s and the 1990s have reported a reduction in mortality from breast cancer of up to 40% in the female population of 50–69 years of age submitted to breast cancer screening [1,2,3]. In geographical regions with limited financial resources and difficulties in accessing standard oncological treatment [4,5,6], this strategy may represent an opportunity for more conservative treatments and better clinical outcomes [7,8,9].
Despite the lack of population-based screening policy in Brazil [10,11,12], the disparity between access to screening within the public healthcare system, on which 70% of the Brazilian population relies, and access to screening within the private healthcare system is evident. The incidence of tumors diagnosed at advanced stages reflects this situation, since 36.9% of such cases occur in women consulting within the public healthcare network, while in the private sector this rate falls to 16.2% [13,14,15]. Nevertheless, this scenario has changed over recent decades, with declining mortality rates in some states of the country, possibly due to advances in the treatment of the disease [16].
Another factor that could have contributed to this stabilization was the development of programs such as the National Mammography Quality Program (PNQM) and the Cancer Database (SISCAN) [17, 18]. These initiatives aimed to improve the monitoring of the quality and reporting of test results, and patient follow-up. This represented an important step forward for public policies in the country [19, 20].
Nevertheless, there remains a need to improve such public policies. Because early diagnosis represents an important step in this process, the present study was developed to evaluate temporal changes in breast cancer screening provided under the Brazilian National Health Service (SUS) in accordance with the different regions of the country and the different states including the federal district, between 2008 and 2017.
Methods
This was an ecological time-series study in which data referring to mammograms conducted within the SUS were analyzed, for the country as a whole, each geographic region, the states and the federal district, for the period between 2008 and 2016. Brazil consists of 26 states and a federal district, with these areas being grouped together into five geographic regions: the north, northeast, southeast, south and Midwest [21].
Target population
The target population consisted of women of 50 to 69 years of age, according to the regulations of the Ministry of Health of Brazil [11]. Data regarding the population of women between 2008 and 2012 were collected from the System of Demographic and Socioeconomic Information on Health, Department of Information Technology of the SUS (DATASUS) [22]. The projected population of Brazil established by the Brazilian Institute of Geography and Statistics (IBGE) was used for the 2013–2016 period [23].
Estimated coverage
Breast cancer screening coverage was estimated based on two-yearly screening aimed at reaching 100% of the target population. Coverage was expressed as a percentage and calculated from the ratio between the number of scans performed and the expected number for the target population [14].
The number of exams carried out annually between 2008 and 2017 was obtained from the DATASUS outpatient database [24] according to the codes for the procedure: 0204030030 (mammography) and 0204030188 (bilateral mammography for screening purposes). The expected number of exams for the target population was calculated from the total number of women of 50–69 years of age and in accordance with the recommendations of the National Cancer Institute (INCA) for two-yearly screening [25].
Statistical analysis
The annual percent change (APC) in breast cancer screening coverage was calculated for Brazil as a whole, its different geographic regions, each state and the federal district. The relevant 95% confidence intervals (95%CI) were calculated, with p-values < 0.05 being considered statistically significant. The Poisson regression model was used for these calculations and the software program used was JoinPoint Regression, version 4.2.0.2 of June 2015 (National Cancer Institute) [26].
For analysis purposes, mammography coverage was considered to have increased when the APC increased, and the minimum value of the confidence interval was above zero. Coverage was considered to have decreased when the APC decreased, and the maximum value of the confidence interval was below zero. Coverage was considered to have remained stable when, irrespective of the rate of coverage, the minimum value of the confidence interval was below zero and the maximum value was above zero.
Ethical aspects
The data used are publicly available [24, 25]. For this type of study, formal consent is not required. All recommendations of good clinical practice were followed according to Brazilian law and the Helsinki Convention.
Results
In 2008, the female population of 50 to 69 years of age in Brazil was estimated at 14,432,692 women. This number increased to 19,584,342 in 2017, representing an increment of 36.0% in this population. Over that timeframe, a total of 1,227,514 and 2,790,937 mammograms, respectively, were approved for payment. This represents an increase of 127.0% in the number of exams paid for by the SUS, at a total cost of 968,567,514.42 Brazilian reais.
The estimated extent of breast cancer screening coverage provided under the SUS in Brazil for the 2008–2017 period ranged from 14.4 to 24.2%. Table 1 shows the estimated coverage per year for the entire study period according to the different geographic regions, the states and the federal district.
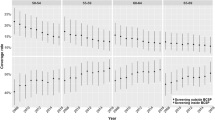
Regression analysis showed that, for Brazil as a whole, there was a significant increase in breast cancer screening coverage, with an APC of 14.5% (p < 0.01) for the 2008–2012 period, while for the 2012–2017 period coverage remained stable (p = 0.3) (Fig. 1). The same was true for the different regions of the country, with the analysis showing a significant increase in breast cancer screening in the north, northeast and southeast at the beginning of the study period, with APCs of 11.1, 14.4 and 14.1%, respectively (p < 0.01), followed by stabilization (Fig. 2a, b and c).

Trends in breast cancer screening coverage provided under the Brazilian National Health service for the female population of 50–69 years of age between 2008 and 2017

Trends in breast cancer screening coverage provided under the Brazilian National Health Service for the female population of 50–69 years of age between 2008 and 2017 according to the different geographic regions of the country. a) north; b) northeast; c) southeast d) south e) midwest
In the south and Midwest, however, the increase occurred between 2008 and 2011 and between 2008 and 2013, with APCs of 21.0 and 9.4%, respectively (p < 0.01). Nevertheless, after this period, there was a reduction in breast cancer screening coverage, with an APC of − 2.0% (p < 0.01) in the south and − 9.4% (p < 0.01) in the Midwest (Fig. 2d and e).
Of the 26 states, a significant increase in breast cancer screening coverage occurred in 7 (27%), while in 6 (23%) coverage remained stable throughout the study period. In 13 states (50%), there was significant increase in coverage at the beginning of the study period; however, after this period coverage remained stable in 11 states and decreased significantly in 2 (Table 2).
In the federal district, coverage remained stable between 2008 and 2014, with an APC of 17.7%. The APC for the 2014–2017 period was − 47.7% (Table 2).
Discussion
The present study showed that there was an increase in breast cancer screening coverage provided under the SUS in Brazil between 2008 and 2017. This coverage, however, failed to reach 25% of the expected number of exams for the Brazilian population of women of 50–69 years of age. This finding confirms that the number of scans performed fails to comply with the World Health Organization recommendation that at least 70% of the target population should have access to breast cancer screening in order to effectively reduce mortality rates [27, 28].
In the past decade, the SUS has invested around 969 million reais in breast cancer screening, representing an increase of 92% in the number of scans performed over the period. This led to an increase in the percent coverage of the target population, from 14.4 to 24.2%, suggesting a possible improvement in the investments and public policies aimed at the early detection of breast cancer in the country [10, 18, 29].
Nevertheless, analysis of the APC for breast cancer screening coverage in Brazil showed a significant annual increase of 14.5% followed by stabilization, with a tendency towards a decrease, albeit insignificant, of − 0.4% per year from 2012 onwards. This performance differed from one geographic region of the country to another, a finding that is understandable given Brazil’s continental dimensions. Indeed, each region has different geographic characteristics and there are cultural and socioeconomic differences as well as factors inherent to income distribution, which may hamper the population’s access to healthcare services [16, 30, 31].
This poor coverage, together with the finding that the APC has stabilized, is concerning, particularly because the study population relies solely on the SUS. In fact, 70% of the Brazilian population depends exclusively on the National Health Service for access to healthcare [10, 15]. Another key point is the capacity to deliver mammography to the target population. Access depends on available appointments for screening, and geographic distance. A flattening of coverage may reflect insufficient capacity, long distances to screening facilities and lack of transportation, or no change in capacity and a large growth in population [7, 32, 33].
Recent studies have shown that mortality from breast cancer in Brazil is closely related to the human development index (HDI), with mortality rates being lower in the states with a higher HDI, while, conversely, in those with a lower HDI, the number of breast cancer-related deaths was higher [16]. A parallel can be drawn with the present study in which results show that the states in which breast cancer screening coverage provided under the SUS is highest were those with the highest HDI. These states were Minas Gerais, São Paulo, Paraná and Santa Catarina.
With respect to the geographic regions of the country, the northeast merits attention. Although breast cancer screening was below the internationally recommended level [27], an annual increase of 14.4% occurred in the first 6 years of breast cancer screening evaluated in this region. This finding may be explained by the increase in the number of mammography scanners available to the SUS and by the investment of government funding, particularly in areas such as health and education, improving human development indicators in recent years in this region [34].
On the other hand, data from the federal district, the seat of the national government, also merit attention. In the initial years analyzed in the present study, there was an increase, albeit insignificant, in breast cancer screening coverage, with an APC of 17.7% per year, which could be explained by local actions such as the inclusion of a mobile breast cancer screening program. However, problems related to the maintenance of the equipment, political instability and lack of investment in public health locally [6, 35] are factors believed to be responsible for a fall in breast cancer screening coverage, which decreased from 16% in 2014 to 0.6% in 2016, with a slight increase of 3.2% in 2017, representing an APC of − 47.7%. Although a considerable proportion of the population in the federal district has access to private healthcare, this situation may lead to an increase in diagnoses at advanced stages of the disease in the near future.
A possible under-notification of mammograms may constitute a limitation of the present study; however, this should be negligible, since the exams are only paid for after they have been included in the DATASUS platform. Nevertheless, this study illustrates the progress made in breast cancer screening coverage nationwide and may contribute towards guiding the federal government’s public policies in the control of breast cancer in Brazil, bearing in mind that the 1988 amendment to the constitution grants all citizens the right to health and establishes that the provision of healthcare is a duty of the state [36]. Therefore, all Brazilian women of 50–69 years of age have the right to a mammogram every 2 years.
Conclusion
Analysis of temporal changes in breast cancer screening coverage provided under the Brazilian National Health Service (SUS) showed an initial increase in coverage, confirming the effectiveness of public policies. However, these were insufficient to assure an organized screening program. There was a lack of uniformity among the different regions and states, and this situation is worsening, as highlighted by the annual percent change showing that breast cancer screening coverage remained stagnant in the final 5-year period of the study.
Availability of data and materials
The public access to the databases is open.
Links and references to databases used in the study:
-DATASUS/TABNET: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?ibge/cnv/popuf.def
-IBGE: https://ww2.ibge.gov.br/home/estatistica/populacao/projecao_da_populacao/2013/default.shtm
-SIA/DATASUS: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sia/cnv/qbuf.def
-INCA: http://bvsms.saude.gov.br/bvs/publicacoes/parametros_rastreamento_cancer_mama.pdf.
Abbreviations
- APC:
-
Annual percent changes
- DATASUS:
-
System of Demographic and Socioeconomic Information on Health, Department of Information Technology of the SUS
- HDI:
-
Human development index
- IBGE:
-
Brazilian Institute of Geography and Statistics
- INCA:
-
National Cancer Institute
- PNQM:
-
National Mammography Quality Program
- SISCAN:
-
Cancer Database
- SUS:
-
Sistema Único de Saúde, Brazilian National Health Service
References
Tabar L, Vitak B, Chen TH, et al. Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology. 2012;260:658–63.
Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev. 2013;6:CD001877.
Duffy SW, Yen AMF, Chen THH, et al. Long-term benefits of breast screening. Breast Cancer Manag. 2012;1:31–8.
Barrios CH, Reinert T, Werutsky G. Access to high-cost drugs for advanced breast cancer in Latin America, particularly trastuzumab. Ecancermedicalscience. 2019;13:898. https://doi.org/10.3332/ecancer.2019.898.
Alves Soares Ferreira N, Melo Figueiredo de Carvalho S, Engrácia Valenti V, et al. Treatment delays among women with breast cancer in a low socio-economic status region in Brazil. BMC Womens Health. 2017;17:13. https://doi.org/10.1186/s12905-016-0359-6.
Dos Santos Figueiredo FW, Adami F. Effects of the high-inequality of income on the breast cancer mortality in Brazil. Sci Rep. 2019;9:4173. https://doi.org/10.1038/s41598-019-41012-8.
Greenwald ZR, Fregnani JH, Longatto-Filho A, et al. The performance of mobile screening units in a breast cancer screening program in Brazil. Cancer Causes Control. 2018;29:233–41. https://doi.org/10.1007/s10552-017-0995-7.
Soares LR, Freitas-Junior R. The impact of mammography screening on the surgical treatment of breast cancer. Breast J. 2018;24:1138. https://doi.org/10.1111/tbj.13093.
Júnior FR, Nunes RD, Martins E, et al. Prognostic factors and overall survival of breast cancer in the city of Goiania, Brazil: a population-based study. Rev Col Bras Cir. 2017;44:435–43. https://doi.org/10.1590/0100-69912017005003.
Lee BL, Liedke PER, Barrios CH, et al. Breast cancer in Brazil: present status and future goals. Lancet Oncol. 2012;13:e95–e102. https://doi.org/10.1016/S1470-2045(11)70323-0.
Migowski A, Silva GAE, Dias MBK, Diz MDPE, Sant'Ana DR, Nadanovsky P. Guidelines for early detection of breast cancer in Brazil. II - new national recommendations, main evidence, and controversies. Cad Saude Publica. 2018;34:e00074817. https://doi.org/10.1590/0102-311X00074817.
Rodrigues DCN, Freitas-Junior R, Corrêa RS, et al. Performance of diagnostic centers in the classification of opportunistic screening mammograms from the Brazilian public health system (SUS). Radiol Bras. 2013;46:149–55.
Simon SD, Bines J, Werutsky G, et al. Characteristics and prognosis of stage I-III breast cancer subtypes in Brazil: the AMAZONA retrospective cohort study. Breast. 2019;44:113–9. https://doi.org/10.1016/j.breast.2019.01.008.
Corrêa RS, Freitas-Junior R, Peixoto JE, et al. Estimativas da cobertura mamográfica no Estado de Goiás, Brasil. Cad Saúde Pública. 2011;27:1757–67. https://doi.org/10.1590/S0102-311X2011000900009.
Brasil. Ministério da Saúde. Agência Nacional de Saúde Suplementar. Caderno de informação da saúde suplementar: beneficiários, operadoras e planos. Rio de Janeiro, RJ. Ano 11, n.2, p.1–64. Ministério da Saúde; 2017.
Gonzaga CMR, Freitas-Junior R, Curado MP, et al. Temporal trends in female breast cancer mortality in Brazil and correlations with social inequalities: ecological time-series study. BMC Public Health. 2015;15:96.
Brasil. Ministério da Saúde. Gabinete do Ministro. Portaria N° 531 de 26 de março de 2012. Institui o Programa Nacional de Qualidade em Mamografia – PNQM. Brasília, DF: Diário Oficial da União, N° 60, Página 91. Seção 1, de 27 de março de 2012.
Brasil. Ministério da Saúde. Gabinete do Ministro. Portaria N° 3.394 de 30 de dezembro de 2013. Institui o Sistema Nacional de Informação do Câncer – SISCAN, no âmbito do Sistema Único de Saúde. Brasília, DF: Diário Oficial da União, N° 253, Página 57. Seção 1, de 31 de dezembro de 2013.
Corrêa RS, Freitas-Junior R, Peixoto JE, et al. Effectiveness of a quality control program in mammography for the Brazilian National Health System. Rev Saude Publica. 2012;46:769–76.
Passman LJ, Farias AMRO, Tomazelli JG, et al. SISMAMA – implementation of an information system for breast cancer early detection programs in Brazil. Breast. 2011;20(Suppl 2):S35–9.
Instituto Brasileiro de Geografia e Estatística (IBGE). Sinopse do Censo Demográfico 2010 – Cidades, Goiás. Brasília, DF, 2010. http://www.ibge.gov.br/cidadesat/topwindow.htm?1. Accessed 20 June 2016.
Brasil. Ministério da Saúde. Departamento de Informática do SUS – DATASUS. Informações de Saúde (TABNET). Demográficas e Socioeconômicas. Brasília, DF, 201e6. http://tabnet.datasus.gov.br/cgi/deftohtm.exe?ibge/cnv/popuf.def. Accessed 20 June 2016.
Brasil. Instituto Brasileiro de Geografia e Estatística. Diretoria de Pesquisas. Coordenação de População e Indicadores Sociais. Gerência de Estudos e Análises da Dinâmica Demográfica. Projeção da população do Brasil e Unidades da Federação por sexo e idade para o período 2000–2030. https://ww2.ibge.gov.br/home/estatistica/populacao/projecao_da_populacao/2013/default.shtm. Accessed 9 June 2018.
Brasil. Ministério da Saúde. Departamento de Informática do SUS – DATASUS. Sistema de Informações Ambulatoriais do SUS (SIA/SUS). Brasília, DF, 2016. http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sia/cnv/qbuf.def. Accessed 9 June 2018.
Brasil. Ministério da Saúde. Parâmetros técnicos para o rastreamento do câncer de mama: recomendações para gestores estaduais e municipais. Rio de Janeiro: INCA, 2009. http://bvsms.saude.gov.br/bvs/publicacoes/parametros_rastreamento_cancer_mama.pdf. Accessed 30 Apr 2019.
United States of America. National Cancer Institute. Joinpoint Regression Program. Version 4.0.4. Bethesda; 2015. http://surveillance.cancer.gov/joinpoint/. Accessed 31 August 2015.
World Health Organization. Cancer control: knowledge into action. WHO guide for effective programmes: early detection. Geneva: WHO; 2007.
Freitas-Junior R, Rodrigues DCN, Corrêa RS, et al. Contribution of the unified health care system to mammography screening in Brazil, 2013. Radiol Bras. 2016;49:305–10.
Brasil. Ministério da Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva. Controle do câncer de mama: documento de consenso. http://www.inca.gov. br/publicacoes/Consensointegra.pdf. Accessed 9 June 2018.
Silva TB, Mauad EC, Carvalho AL, et al. Difficulties in implementing an organized screening program for breast cancer in Brazil with emphasis on diagnostic methods. Rural Remote Health. 2013;13:2321.
Tomazelli JG, Silva GAE. Breast cancer screening in Brazil: an assessment of supply and use of Brazilian National Health System health care network for the period 2010-2012. Epidemiol Serv Saude. 2017;26:713–24. https://doi.org/10.5123/S1679-49742017000400004.
Vieira RADC, Formenton A, Bertolini SR. Breast cancer screening in Brazil. Barriers related to the health system. Rev Assoc Med Bras (1992). 2017;63:466–74. https://doi.org/10.1590/1806-9282.63.05.466.
Buranello MC, Meirelles MCCC, Walsh IAP, Pereira GA, Castro SS. Breast cancer screening practice and associated factors: Women's health survey in Uberaba MG Brazil, 2014. Cien Saude Colet. 2018;23:2661–70. https://doi.org/10.1590/1413-81232018238.14762016.
Duggan C, Cruz TA, Porto MRT, et al. Improving breast health Care in the State of Sergipe, Brazil: a commentary. J Glob Oncol. 2018;4:1–3. https://doi.org/10.1200/JGO.18.00114.
Barros ÂF, Araújo JM, Murta-Nascimento C, Dias A. Clinical pathways of breast cancer patients treated in the Federal District, Brazil. Rev Saude Publica. 2019;53:14. https://doi.org/10.11606/S1518-8787.2019053000406.
Brasil. Ministério da Saúde. Constituição da República Federativa do Brasil, de 5 de outubro de 1988. http://www.planalto.gov.br/ccivil_03/Constituicao/Constituicao.htm. Accessed 9 April 2017.
Acknowledgements
None.
Funding
This study is not supported by any funding source.
Author information
Authors and Affiliations
Contributions
DCNR, RMSR, RSC, JEP and RFJ designed the study. DCNR, RSC and PAG were responsible for collecting the data. DCNR, RFJ, RMSR, RSC, PAG, JEP, EM and LRS made substantial contributions to the data analysis and interpretation. DCNR, RFJ, RMSR, RSC, PAG, JEP, EM and LRS were responsible for drafting the article and revising it critically for important intellectual content. All the authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Rodrigues, D.C.N., Freitas-Junior, R., Rahal, R.M.S. et al. Temporal changes in breast cancer screening coverage provided under the Brazilian National Health Service between 2008 and 2017. BMC Public Health 19, 959 (2019). https://doi.org/10.1186/s12889-019-7278-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-019-7278-z