
Abstract
Background
Studies suggest an association between weight change and subsequent poor physical health functioning, whereas the association with mental health functioning is inconsistent. We aimed to examine whether obesity and change of body mass index among normal weight, overweight and obese women and men associate with changes in physical and mental health functioning.
Methods
The Helsinki Health Study cohort includes Finnish municipal employees aged 40 to 60 in 2000–02 (phase 1, response rate 67%). Phase 2 mail survey (response rate 82%) took place in 2007 and phase 3 in 2012 (response rate 76%). This study included 5668 participants (82% women). Seven weight change categories were formed based on body mass index (BMI) (phase 1) and weight change (BMI change ≥5%) (phase 1–2). The Short Form 36 Health Survey (SF-36) measured physical and mental health functioning. The change in health functioning (phase 1–3) score was examined with repeated measures analyses. Covariates were age, sociodemographic factors, health behaviours, and somatic ill-health.
Results
Weight gain was common among women (34%) and men (25%). Weight-gaining normal weight (−1.3 points), overweight (−1.3 points) and obese (−3.6 points) women showed a greater decline in physical component summary scores than weight-maintaining normal weight women. Among weight-maintainers, only obese (−1.8 points) women showed a greater decline than weight-maintaining normal weight women. The associations were similar, but statistically non-significant for obese men. No statistically significant differences in the change in mental health functioning occurred.
Conclusion
Preventing weight gain likely helps maintaining good physical health functioning and work ability.
Similar content being viewed by others
Background
Obesity is a global threat to public health with the majority of adults in the OECD countries being overweight and one-fifth obese [1, 2]. In some countries the increase in obesity is slowing, but among middle-aged Europeans weight-gain remains common [3] and the worldwide prevalence [4] and the burden [5] attributable to obesity are still increasing. Obesity, but also weight gain itself, is associated with several public health issues, such as somatic diseases [6], work disability [7], premature mortality [8], poor quality of life and health functioning [9,10,11,12,13,14,15,16,17,18]. However, weight-loss has shown only small or no beneficial effects on health functioning [9,10,11,12,13,14]. Due to increased retirement age and life expectancy [19], the number of older employees is increasing. Health functioning is closely related to both work ability, quality of life, and ageing [20, 21], and therefore, factors associated with health functioning are important to study especially among ageing employees. In addition to prevention of obesity altogether, it is important for further studies to focus on factors that help maintaining good health, work ability and functioning in already-obese individuals.
Poor physical and mental health functioning, measured by the Short Form 36 Health Survey (SF-36), or similar other measures, are associated with obesity [15, 16, 22, 23]. A meta-analysis based on eight cross-sectional studies showed a dose—response association between body mass index (BMI) and poor physical health functioning [15]. The association with poor mental health functioning, however, occurred only for the obese with BMI ≥40 kg/m2. Also longitudinal studies suggest an association between obesity and poor subsequent physical, and possibly also mental health functioning [9,10,11,12,13,14, 17, 18].
Similarly to obesity, weight gain itself also associates with poor and declining physical health functioning, but inconsistently with mental health functioning [9,10,11,12,13,14, 17, 18]. A large study showed that weight gain among U.S. nurses aged 29 to 71 was associated with lower physical health functioning, but non-significantly with lower mental health functioning [9]. In contrast, greater weight-loss (>6,75 kg) among the overweight and obese participants was associated with better physical, but poorer mental health functioning. However, previous studies have shown inconsistent results and the effect of weight-loss is particularly poorly understood.
Comparing studies is challenging due to study-design heterogeneity; differences in follow-up time, measurements of weight change, and chose of statistical methods. In addition, some previous studies have been relatively small-scale [10,11,12, 17]. It seems that the associations with health functioning are stronger among women than men, but some large studies have only included women [9, 13].
Because obesity and weight-gain are associated with metabolic stress and inflammation [24, 25], consequently weight-gainers and those with the highest BMI could be at increased risk for obesity-related complications and poor health functioning. To judge whether weight-maintenance protects normal weight, overweight and obese employees from developing poor health functioning, longitudinal data are needed to examine the effect of weight change, in addition to body mass index, on physical and mental health functioning.
We aimed to deepen the understanding of the associations between BMI, weight change and health functioning by comparing the effect of weight change on physical and mental health functioning among different weight groups among midlife female and male employees. In addition, we adjusted for several covariates including age, marital status, socioeconomic position, employment status, smoking, drinking problem, physical activity, and somatic ill-health, as these factors are associated with health functioning and are often unequally distributed between the weight groups [26,27,28].
Methods
Data
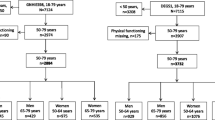
The Helsinki Health Study cohort includes 8960 municipal employees of the City of Helsinki, Finland, aged 40 to 60 in 2000–02 (phase 1, response rate 67%). Follow-up mail surveys were conducted in 2007 (phase 2, response rate 82%) and in 2012 (phase 3, response rate 76%). Altogether 6245 participants responded to all three phases. Women were in the majority (82%), which reflects the gender distribution in the Finnish municipal sector. Men, younger employees and manual workers were slightly underrepresented, but according to non-response analyses, the data represent the target population satisfactorily [29, 30]. Pregnant (n = 23), underweight at phase 1 (BMI <18.5 kg/m2) (n = 53), and participants retired due to disability (n = 397) were excluded. The final data in analyses consisted of 4645 women and 1023 men after exclusions of responders with missing information on height or weight (n = 100), physical and mental health functioning at all phases 1–3 (n = 4). In the final data 21% of the participants had retired at phase 2 and 41% at phase 3.
The ethics committees of the Department of Public Health, University of Helsinki and the health authorities of the City of Helsinki approved the Helsinki Health Study protocol.
Measures
Body mass index
The self-reported weight (kg) divided by the square of the height (m) defined the BMI (kg/m2), and a BMI change ≥5% between phase 1 and phase 2 defined the weight change. As long as the height is stable, a percentage change of BMI is equal with a percentage change in kilograms. Based on the weight change and BMI at phase 1, the participants formed seven groups: 1) normal weight weight-maintainers (BMI 18.5–24.9 kg/m2, weight change ≤5%), 2) normal weight weight-gainers (BMI 18.5–24.9 kg/m2, weight gain ≥5%), 3) overweight weight-maintainers (BMI 25–29.9 kg/m2, weight change ≤5%), 4) overweight weight-gainers (BMI 25–29.9 kg/m2, weight gain ≥5%), 5) obese weight-maintainers (BMI ≥30 kg/m2, weight change ≤5%), 6) obese weight-gainers (BMI ≥30 kg/m2, weight gain ≥5%) and 7) all weight-losers (weight loss ≥5%).
Physical and mental health functioning
The SF-36 focuses on self-assessed well-being and functioning and is a widely used measure of general health and quality of life [20]. The measure includes eight subscales scored from 0 to 100: physical functioning, role limitations due to physical health problems, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems and mental health. The SF-36 physical component summary (PCS) and mental component summary (MCS) scores can be calculated from the subscales by means of factor analyses to measure general physical and mental health functioning. The component summary scores range from 0 to 100, with a mean of 50 and a standard deviation of 10 observed in the general US population. Higher scores indicate better functioning. A change greater than 3.0 points can be regarded as clinically significant [31].
Covariates
Phase 1 age included five categories: 40, 45, 50, 55 and 60. Socioeconomic position (SEP), measured at phase 1, consisted of managers and professionals, semi-professionals, routine non-manual employees, and manual workers [32]. Employment status categories at phase 2 and 3 were non-employed and employed, including part-time workers. Other covariates included measurements from all three phases and were used as time-variant. Marital status included married and cohabitants, and unmarried. Based on self-reported estimates of average weekly hours of leisure-time physical activity per each four intensity grades i.e. walking, brisk walking, jogging, running, or their equivalent activities, we calculated total leisure-time metabolic equivalent (MET) hours per week by multiplying the weekly hours by the MET value [33] of each physical activity intensity grade and adding the four values together [34]. Less than 14 MET-hours per week indicated physical inactivity (e.g. 2.5 h of brisk walking equals 15 MET-hours) [35]. Drinking problems as measured on the CAGE-questionnaire [36] included problem drinking and no problem drinking (the cut-off scores were two and three points for women and men, respectively). Smoking status included smokers, ex-smokers and non-smokers. Somatic ill-health was considered to be present among those who reported that a doctor had ever diagnosed them with at least one of the following diseases: gout, osteoarthrosis, rheumatoid arthritis, angina pectoris, myocardial infarction, claudication, epilepsy, or disturbance of the cerebral circulation. Participants non-reporting marital status, employment status, physical activity, problem drinking, smoking and somatic ill-health were considered as singles, employed, active, no problem drinkers, non-smokers, and healthy.
Statistical analyses
Firstly, we used cross-tabulation to describe the phase 1 characteristics (Table 1). Secondly, we calculated the mean scores and standard deviations for the physical and mental health functioning by weight change groups at all three phases (Table 2). Thirdly, we calculated adjusted cross-sectional differences in PCS and MCS scores at phases 1 and 3 by weight change groups using linear regression analysis (Figs. 1 and 2). Fourthly, we calculated adjusted differences in the changes of PCS and MCS scores from phase 1 to phase 3 (including phase 2) with repeated measures analysis using MIXED procedure in SPSS (Tables 3 and 4). The results are reported as regression coefficients (β) and their standard errors (SE). Normal weight weight-maintainers served as a reference group. Model 1 adjusted for age, and model 2, model 3, and model 4 adjusted additionally for socio-demographic factors, health behaviours and somatic ill-health, respectively. All covariates, except for socioeconomic position, functioned as time variants. Women and men were examined separately in all analyses due to a gender interaction (PCS p = 0.008; MCS p = 0.006). We conducted the analyses with IBM SPSS Statistics 23.

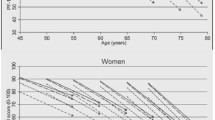
Age-adjusted mean differences of SF-36 physical component summary (PCS) score at phase 1 and phase 3 compared with normal weight weight-maintaining women (n = 4407) and men (n = 976); * p < 0.05

Age-adjusted mean differences of SF-36 mental component summary (MCS) score at phase 1 and phase 3 compared with normal weight weight-maintain maintaining women (n = 4407) and men (n = 976); * p < 0.05
Results
At phase 1 13% of both women and men were obese, whereas 45% of men and 31% of women were overweight (Table 1). Between phase 1 and phase 2 weight gain was common among women (33%) and men (24%), whereas weight-loss occurred less often (women 11%, men 14%). Phase 1 PCS scores were low among those with high age, obesity, low SEP, physical inactivity and somatic ill-health at phase 1, whereas MCS scores were low among those with drinking problems. The mean PCS scores at phase 1 tended to be higher among men than women.
The mean PCS scores showed an inverse dose-response association with BMI, showing that PCS decreased with increasing BMI, whereas for MCS there was no such association (Table 2). Regression analyses showed that compared to normal weight weight-maintainers the age-adjusted differences in PCS scores between the weight groups were statistically significant for the overweight and obese women at phase 1 and phase 3 (Fig. 1). Among men the differences in PCS scores were significant for the obese at phase 1 and 3 and for the overweight weight-gainers at phase 3. Among weight-losers both women and men showed a lower PCS score than the normal weight weight-maintainers (Fig. 1). The mean MCS scores were similar in the weight groups (Table 2). However, the regression analyses showed that weight-gaining normal weight women and weight-gaining overweight men had lower MCS scores than the normal weight weight-maintainers at phase 1 (Fig. 2).
In addition to the dose—response association found for PCS, the mean scores also suggested a time trend for both PCS and MCS. However, in contrast to PCS, MCS mean scores showed a slight increase over time (Table 2). When the differences in the change of PCS mean scores were examined with repeated measures analyses, weight gain among women was associated with a greater decline, irrespective of phase 1 BMI: weight-gaining normal weight (−1.3 points), overweight (−1.3 points) and obese (−3.6 points) women showed a greater decline in PCS scores than weight-maintaining normal weight women (Table 3). Among weight-maintainers, only obese (−1.8 points) women showed a greater decline.
Adjustment for health behaviours and somatic ill-health slightly attenuated the associations, and except for the weight-gaining overweight women, the changes remained statistically significant (Table 3). There was a similar, but weaker, difference between weight-gaining overweight, weight-gaining obese, and weight-maintaining obese men. Only for the weight-gaining obese men, the decrease was statistically significant, even after adjustments. Among weight-losing women and men there were no significant changes in PCS scores.
In line with the mean scores, the analyses showed no statistically significant differences in the changes in MCS scores for weight-maintainers and weight-gainers (Table 4). Weight-losing women showed a − 0.7 points difference to the reference group, and adjustment for covariates slightly attenuated the estimate. Weight-gaining obese men showed a non-significant difference in MCS score (−2.0 points).
Discussion
Principal findings
Obese but also weight-gaining women showed worse and declining physical health functioning compared with normal weight weight-maintaining women. These findings were similar, but statistically weaker for obese men. The changes in mental health functioning, however, did not differ between the weight groups. Adjusting for health behavior and somatic ill-health showed small, but mainly statistically non-significant effects, on the findings. Weight-loss did not show a positive association with health functioning.
Comparison to previous studies
This study confirms the findings from others suggesting that physical health functioning declines faster among the obese. As expected, also weight gain was associated with a greater decline in physical health functioning. Obesity and weight gain increase musculoskeletal strain, but may also add to the internal metabolic stress and inflammation [24, 25]. Therefore, it is possible that besides obesity, weight-gain itself also contributes to the genesis of inflammation-mediated physical and mental conditions (e.g. depression, diabetes, and cardiovascular diseases) [37, 38], which might explain why weight-gaining women show a greater decline in physical health functioning than weight-maintaining women. However, no association occurred for mental health functioning. It is possible that the decline in physical, and especially mental health functioning is too slow to be observed within a decade of follow-up. To reconfirm our findings, further studies with longer and more frequent follow-ups within different cohorts are needed.
As in previous studies, the association between weight change and mental health functioning remained less clear also in our study. A meta-analysis showed an association with mental health functioning only for the morbidly obese with BMI > 40 kg/m2 [15]. In our study the morbidly obese (BMI ≥35 kg/m2) women (n = 136) and men (n = 30) were few. We however, examined the severely obese separately in sensitivity analyses. Weight-gaining and weight-losing severely obese women showed a greater decline in PCS scores than the weight-gaining and weight-losing obese with BMI 30–35 kg/m2. Among the severely obese no associations were found for MCS.
In our study, among weight-losing women a weak association with a greater decline in mental health functioning occurred, whereas there was no association for physical health functioning. However, for reliable analysis of the weight-losers intended and unintended weight-loss should be distinguished. We did adjust for self-reported somatic ill-health as time variant, but for reliable examination, unintended weight-loss due to somatic health problems, such as cancer, should be ruled out. Intended weight-loss among the obese individuals would improve especially physical health functioning according to findings from a clinical trial [39]. In addition, also when examining mental health functioning, it is important to distinguish between intended and unintended weight loss, as depression as well as other mental problems might cause unintended weight-changes and thus bias the results.
Weight-loss among women and weight-gain among obese men was associated with a non-significantly greater decline in mental health functioning. Common mental disorders such as anxiety disorder and psychotic disorders such as schizophrenia are associated with weight gain, which may possibly explain the association among the weight-gaining obese men [40, 41].
Strengths and limitations
The strengths of this study include a large cohort including both women and men representing hundreds of different occupations. Three identical repeated measurements of the widely used SF-36 health functioning were available, which allowed the examination of the differences in changes over a decade of follow-up. Furthermore, several covariates were included at all three time points.
The study limitations include, firstly, that the data covered only middle-aged municipal employees. However, this growing population group is important to study because health functioning is closely related to work ability, quality of life and ageing [19,20,21]. Secondly, height and weight as well as covariates were based on self-reports. In these data self-reported BMI predicted sickness absence as accurately as did measured BMI, however [42]. Thirdly, obese (n = 84) and weight-losing (n = 115) men were few in number, which complicates reliable analyses for these groups. Fourthly, we were unable to distinguish between intended and unintended weight-loss. Many somatic diseases may cause unintended weight-loss, which might bias the results. However, we were able to adjust for a range of somatic diseases. Fifthly, the time between follow-ups was relatively long (5–7 years) with some unobserved changes in the data possibly taking place. Finally, the survey response rate was acceptable, but non-response and selection of healthy workers remains a problem. Healthy workers are likely overrepresented, which weakens the generalizability of the results [43]. The excluded participants who retired due to disability retirement had lower SF-36 scores at phase 1.
Also retirees that retired due to non-medical reasons showed lower SF-36 scores than the employed, however visually, the curves among the weight groups among the retired and the employed were similar. The interaction between these groups was statistically significant, but we considered the interaction to be of removable type [44], after examining retirees separately in sensitivity analyses and finding that female retirees at phase 2 showed a greater but similar decline in PCS and that including this group in the final analysis did not affect the final estimates or the conclusions.
Conclusions
Besides obesity also weight gain associates with worse physical, but not mental health functioning. Weight-loss showed no positive association with either physical or mental health functioning. Preventing further weight gain may be beneficial in maintaining physical health functioning and work ability particularly among already-obese employees.
Change history
17 October 2017
A correction to this article has been published.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- MET:
-
Metabolic equivalent task
- SEP:
-
Socioeconomic position
- SF-36:
-
Short Form 36 Health Survey
- WHO:
-
World Health Organization
References
Borodulin K, Vartiainen E, Peltonen M, Jousilahti P, Juolevi A, Laatikainen T, et al. Fourty-five-year trends in cardiovascular risk factors in Finland. Eur J Pub Health. 2014;25:539–46.
Organisation for Economic Co-operation and Development. OECD: Obestiy Update 2014. http://www.oecd.org/els/health-systems/obesity-update.htm. Accessed 10 Aug 2016.
Rokholm B, Baker J, Sørensen T. The levelling off of the obesity epidemic since the year 1999--a review of evidence and perspectives. Obes Rev. 2010;11:835–46.
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–81.
GBD 2013 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. 2015;6736:1990–2013.
Kodama S, Horikawa C, Fujihara K, Yoshizawa S, Yachi Y, Tanaka S, et al. Quantitative relationship between body weight gain in adulthood and incident type 2 diabetes: a meta-analysis. Obes Rev. 2014;15:202–14.
Roos E, Laaksonen M, Rahkonen O, Lahelma E, Lallukka T. Weight change and sickness absence-a prospective study among middle-aged employees. Eur J Pub Health. 2015;25:263–7.
The Global BMI Mortality Collaboration. Body-mass index and all-cause mortality: individual- participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388:776–86.
Pan A, Kawachi I, Luo N, Manson JE, Willett WC, Hu FB, et al. Changes in body weight and health-related quality of life: 2 cohorts of US women. Am J Epidemiol. 2014;180:254–62.
Laxy M, Holle R, Döring A, Peters A, Hunger M. The longitudinal association between weight change and health-related quality of life: The KORA S4/F4 cohort study. Int J Public Health. 2014;59:279–88.
León-Muñoz LM, Guallar-Castillón P, Banegas JR, Gutiérrez-Fisac JL, López-García E, Jiménez FJ, et al. Changes in body weight and health-related quality-of-life in the older adult population. Int J Obes. 2005;29:1385–91.
Verkleij SPJ, Adriaanse MC, Wendel-Vos GCW, Schuit AJ. Longitudinal relation between weight change and quality of life in a community-based population: a prospective cohort study. Eur J Pub Health. 2013;23:285–90.
Fine JT, G a C, Coakley EH, Moseley G, Manson JE, Willett WC, et al. A prospective study of weight change and health-related quality of life in women. JAMA. 1999;282:2136–42.
Döring N, de Munter J, Rasmussen F. The associations between overweight, weight change and health related quality of life: Longitudinal data from the Stockholm Public Health Cohort 2002–2010. Prev Med. 2015;75:12–7.
Ul-Haq Z, Mackay DF, Fenwick E, Pell JP. Meta-analysis of the association between body mass index and health-related quality of life among adults, assessed by the SF-36. Obesity. 2013;21:322–7.
Fontaine KR, Barofsky I. Obesity and health-related quality of life. Obes Rev. 2001;2:173–82.
de Hollander EL, Picavet HSJ, Milder IE, Verschuren WMM, Bemelmans WJE, de Groot LCPGM. The impact of long-term body mass index patterns on health-related quality of life: the Doetinchem Cohort Study. Am J Epidemiol. 2013;178:804–12.
Cameron AJ, Magliano DJ, Dunstan DW, Zimmet PZ, Hesketh K, Peeters A, et al. A bi-directional relationship between obesity and health-related quality of life: evidence from the longitudinal AusDiab study. Int J Obes. 2012;36:295–303.
Christensen K, Doblhammer G, Roland R, James WV. Ageing populations: the challenges ahead. Lancet. 2009;374:1196–208.
Ware JE, Gandek B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J Clin Epidemiol. 1998;51:903–12.
Hemingway H, Stafford M, Stansfeld S, Shipley M, Marmot M. Is the SF-36 a valid measure of change in population health? Results from the Whitehall II study. BMJ. 1997;315:1273–9.
Backholer K, Wong E, Freak-Poli R, Walls HL, Peeters A. Increasing body weight and risk of limitations in activities of daily living: a systematic review and meta-analysis. Obes Rev. 2012;13:456–68.
Dowd JB, Zajacova a. Long-term obesity and physical functioning in older Americans. Int J Obes. Nat Publ Group. 2014;39:502–7.
Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444:860–7.
Fogarty AW, Glancy C, Jones S, Lewis S a, Mckeever TM, Britton JR. A prospective study of weight change and systemic inflammation. Am J Clin Nutr. 2008;87:30.35.
Laaksonen E, Lallukka T, Lahelma E, Ferrie JE, Rahkonen O, Head J, et al. Economic difficulties and physical functioning in Finnish and British employees: contribution of social and behavioural factors. Eur J Pub Health. 2011;21:456–62.
Robinson SM, Jameson KA, Syddall HE, Dennison EM, Cooper C, Sayer AA, et al. Clustering of lifestyle risk factors and poor physical function in older adults: The Hertfordshire Cohort Study. J Am Geriatr Soc. 2013;16:1684–91.
Lahti J, Sabia S, Singh-Manoux A, Kivimäki M, Tatsuse T, Yamada M, et al. Leisure time physical activity and subsequent physical and mental health functioning among midlife Finnish, British and Japanese employees: a follow-up study in three occupational cohorts. BMJ Open. 2016;6
Laaksonen M, Aittomäki A, Lallukka T, Rahkonen O, Saastamoinen P, Silventoinen K, et al. Register-based study among employees showed small nonparticipation bias in health surveys and check-ups. J Clin Epidemiol. 2008;61:900–6.
Lahelma E, Aittomäki A, Laaksonen M, Lallukka T, Martikainen P, Piha K, et al. Cohort profile: the Helsinki Health Study. Int J Epidemiol. 2013;42:722–30.
Samsa G, Edelman D, Rothman ML, Williams GR, Lipscomb J, Matchar D. Determining clinically important differences in health status measures: a general approach with illustration to the Health Utilities Index Mark II. PharmacoEconomics. 1999;15:141–55.
Lahelma E, Martikainen P, Rahkonen O, Roos E, Saastamoinen P. Occupational class inequalities across key domains of health: Results from the Helsinki Health Study. Eur J Pub Health. 2005;15:504–10.
Kujala UM, Kaprio J, Sarna S, Koskenvuo M. Relationship of leisure-time physical activity and mortality: the Finnish twin cohort. J Am Med Assoc. 1998;279:440–4.
Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET in- tensities. Med Sci Sports Exerc. 2000;32:S498–504.
Lahti J, Lallukka T, Lahelma E, Rahkonen O. Leisure-time physical activity and psychotropic medication: A prospective cohort study. Prev Med. 2013;57:173–7.
Ewing JA. Detecting alcoholism. The CAGE questionnaire. JAMA J. Am. Med. Assoc. 1984;252:1905–7.
Stuart MJ, Baune BT. Depression and type 2 diabetes: inflammatory mechanisms of a psychoneuroendocrine co-morbidity. Neurosci Biobehav Rev Elsevier Ltd. 2012;36:658–76.
Hamer M, Batty GD, Kivimaki M. Risk of future depression in people who are obese but metabolically healthy: the English longitudinal study of ageing. Mol Psychiatry. 2012;17:940–5.
Warkentin LM, Majumdar SR, Johnson JA, Agborsangaya CB, Rueda-Clausen CF, Sharma AM, et al. Weight loss required by the severely obese to achieve clinically important differences in health-related quality of life: two-year prospective cohort study. BMC Med. 2014;12:175.
Manu P, Dima L, Shulman M, Vancampfort D, De Hert M, Correll CU. Weight gain and obesity in schizophrenia: Epidemiology, pathobiology, and management. Acta Psychiatr Scand. 2015;132:97–108.
Faith MS, Butryn M, Wadden TA, Fabricatore A, Nguyen AM, Heymsfield SB. Evidence for prospective associations among depression and obesity in population-based studies. Obes Rev. 2011;12:438–53.
Korpela K, Roos E, Lallukka T, Rahkonen O, Lahelma E, Laaksonen M. Different measures of body weight as predictors of sickness absence. Scand J Public Health. 2013;41:25–31.
Li C, Sung F. A review of the healthy worker effect in occupational epidemiology. Occup Med. 1999;49:225–9.
Breslow N, Day N. Statistical methods in cancer research. Volume I - The analysis of case-control studies: IARC Sci Publ; 1980.
Acknowledgements
We thank the City of Helsinki, Finland and all the participating employees.
Funding
The Study was funded by the Academy of Finland (grant #1294514), the Ministry of Education and Culture, the Finnish Work Environment Fund (grant #112231), the Juho Vainio Foudation and the University of Helsinki. AS was supported by Finska Läkaresällskapet. JL was supported by the Academy of Finland (Grant #1294566). TL was supported by the Academy of Finland (grant #287488 and #294096). EL was supported by the Academy of Finland (grant # 1257362). MM was supported by the Finnish Work Environment Fund (grant #115182) and the Juho Vainio Foundation.
Availability of data and materials
The questionnaire data are available on request. Permission can be applied from the Helsinki Health Study by contacting data management of the Helsinki Health Study (kttl-hhs@helsinki.fi). All the members of the Helsinki Health Study research team have permission to use the data.
Author information
Authors and Affiliations
Contributions
AS, JL and MM performed statistical analyses, whereas authors AS, JL, TL, OR, EL and MM contributed to designing the study, interpreting results and drafting the manuscript. All authors critically reviewed the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethics committees of the Department of Public Health, the University of Helsinki and the health authorities of the City of Helsinki approved the Helsinki Health Study protocol. The ethical approval applies to the current study. The participants gave written informed consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional information
The original version of this article has been revised to correct parameters for the data in the tables.
A correction to this article is available online at https://doi.org/10.1186/s12889-017-4828-0.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Svärd, A., Lahti, J., Roos, E. et al. Obesity, change of body mass index and subsequent physical and mental health functioning: a 12-year follow-up study among ageing employees. BMC Public Health 17, 744 (2017). https://doi.org/10.1186/s12889-017-4768-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-017-4768-8