
Abstract
Background
Alcohol plays a complex role in society. A recent study showed that over half of Irish adults drink hazardously. Adolescents report increased levels of alcohol consumption. Previous research has inferred the influence of the parent on their adolescent. Thus, the aim of the current study was to investigate the association between adolescent alcohol consumption and their parent’s consumption pattern and attitude toward alcohol use in Southern Ireland.
Methods
A cross-sectional survey was undertaken in November 2014. This involved distributing a survey to adolescents (n = 982) in their final two years of second level education and at least one of their parents from a local electorate area in Southern Ireland. This survey included: alcohol use, self- reported height and weight, smoking status, mental health and well-being along with attitudinal questions. Chi-square tests and multivariate logistic regression were utilised.
Results
A 37 % response rate was achieved. Over one-third (34.2 %) of adolescents and 47 % of parents surveyed reported hazardous drinking. Over 90 % of parents disagreed with allowing their adolescent to get drunk and rejected the idea that getting drunk is part of having fun as an adolescent. The majority (79.5 %) of parents surveyed believed that their alcohol consumption pattern set a good example for their adolescent. Multivariate logistic regression highlights the association between adolescent hazardous alcohol consumption and hazardous drinking by the father. Furthermore either parent permitting their adolescent to drink alcohol on special occasions was associated with hazardous alcohol consumption in the adolescent.
Conclusion
The findings of this research notes a liberal attitude to alcohol and increased levels of consumption by the parent are linked to hazardous adolescent drinking behaviour. Future action plans aimed at combatting adolescent hazardous alcohol consumption should also be aimed at tackling parents’ attitudes towards and consumption of alcohol.
Similar content being viewed by others

Background
Alcohol plays a complex role in society. It represents an integral part of modern culture and is generally consumed for reasons of enjoyment and sociability [1]. It is causally related to over 60 different medical conditions and implicated in premature deaths every year [2]. The World Health Organisation (WHO) highlight that the European Union (E.U.) is the heaviest drinking region in the world [2]. Irish people consume higher levels of alcohol when compared to the E.U. average [3] with over half of Irish adults reporting hazardous drinking [4]. This is defined as “a pattern of alcohol consumption that increases the risk of harmful consequences for the user or others” [5].
Principally alcohol is the first harmful substance misused in adolescence [6–10]. Adolescents represent a unique subsection of society, vulnerable to the harms associated with alcohol use [10–12]. Excessive alcohol use among adolescents is associated with increased drug [12] sexual health [11] and mental health issues [13, 14]. It also impacts on brain development and academic performance [15]. Young European adults report being drunk more often than their counter parts world-wide. This equates to 39 % of European students reporting being drunk in the last 30 days [16]. The rate of heavy episodic drinking by adolescents in Ireland is above the European average [16, 14]. Recent research has signalled that adolescents who drink alcohol before the age of 15 are ‘four times more likely to develop alcohol dependency than those who wait until they are 21’ [17].
A number of factors influence the onset of adolescent alcohol consumption including peer pressure, societal factors and parental influences [18–20].
-
1.
Peer: Previous research has noted the influence of peers on adolescent consumption and other risky behaviours such as substance use during adolescence and early adulthood [20–24].
-
2.
Culture: Alcohol consumption has it’s foundations in ancestral European culture [18]. European adolescents drink more often and at higher levels than any of their counterparts worldwide, 57 % of European adolescents reported having a drink in the last 30 days [16, 25, 26]. The alcohol industry promotes a pro-alcohol lifestyle using social-networking systems that are extensively used by adolescents. Evidence-based harm reduction policies are not widely followed [27].
-
3.
Parent: Research has noted the impact of the parent in the formative years of an adolescent’s life. Parent alcohol consumption can be regarded by the child as acceptable behaviour to emulate [8, 28, 29]. A recent systematic review of relevant studies reports on a number of parenting strategies aimed at reducing adolescent alcohol consumption [30]. Results indicate that it is risky for parents to allow children to drink during early adolescence [17]. The risk of dependence is increased by a family history of alcohol problems [31]. It’s been reported that fathers who report heavy drinking and early onset of alcohol use is predictive of harmful alcohol use in their children [32].
However, the most recent review on the subject of parent child relationship highlighted a lack of nation specific research of this culturally specific phenomenon [33]. Furthermore, a lack of European research was noted. Thus, the aim of this current research is to investigate the relationship between parental attitude and consumption of alcohol and adolescent alcohol consumption in Southern Ireland.
Methods
Survey design
A cross-sectional survey was undertaken. This involved distributing a questionnaire to a sample of second-level students in the Kanturk-Mallow local electorate area (Southern Ireland). The survey was carried out during the academic year 2014–15.
Sampling
The sample consisted of students in their final 2 years of second level education from a local electorate area in Southern Ireland, which has an estimated general population of 28,404 and a total secondary school population of 2119 across 6 year groups. According to the 2011 national census this area has a breadth of socioeconomic classes and incomes [34]. All eight secondary schools in the locality were included yielding a sample population of 982 students in their penultimate and final year.
These 982 students were asked to bring an envelope home to their parents containing a consent form and two parent surveys. Parents completed their survey and returned it in the sealed envelope provided. The consent forms were separated from the parent questionnaires on collection. This consent form outlined the aim of the study, the nature of the survey and provided detail on who was organising the research. Furthermore, it highlighted the voluntary nature of the research and an individual’s right to discontinue at any point. The front page of the survey included information on the aim, the nature of participation, who the researchers were and the benefits of completing the questionnaire. Parents consented both for themselves and their child. The child also signed the consent form in the presence of their parent or guardian. Students were surveyed in class. Prior to completion students were again advised of the aim of the study and the voluntary nature of participation. The surveys were confidential; each parent and pupil had a corresponding identification number on their survey to link results. The final page of both parent and pupil questionnaires provided information on individuals and organisations to contact in case of distress or upset as a result of taking the survey. Data collection occurred over a 2 week period during November 2014.
Measurement
Topics in both parent and pupil surveys included alcohol use, self-reported height and weight, smoking status, mental health and well-being. The study utilised previously validated questions. Consumption questions were attained from the Alcohol Use Disorders Identification Test for Consumption (AUDIT-C) [35]. AUDIT-C takes the first three questions of the AUDIT questionnaire which focus on frequency and volume of alcohol consumption. The guidelines on low-risk alcohol consumption are lower in adolescents than those for parents, reflecting their increased vulnerability to alcohol-related harm. Based on previous national and international research, hazardous drinkers were defined as an AUDIT-C score of 5 or more amongst parents [4] and 4 or more amongst adolescents [35]. Parental attitude to alcohol questions were included in the parent survey [36, 37]. Questions on adverse consequences described in CLAN were utilised in the adolescent survey [38]. Personal wellbeing was measured using the Personal Wellbeing Index (PWI) in both adolescents [39] and parents [40]. Parental attitude questions were taken from Smyth et al. and Research New Zealand papers [36, 37]. Second-hand effect, smoking and body mass index questions were taken from the Survey of Lifestyle, Attitudes and Nutrition in Ireland (SLAN) [41] and the College Lifestyle Attitudinal National (CLAN) Survey [38]. Body mass index (BMI) was estimated from self-reported height and weight [42].
Statistical analysis
IBM Statistical Package for Social Science (SPSS) Statistics 20 was used for statistical analysis. AUDIT-C scores were calculated according to instrument guidelines [43, 44]. Analysis included descriptive, frequency and binary logistic regression analysis. Parental attitude questions were measured on a 5-point Likert scale. To increase statistical power, strongly disagree, disagree and neutral were combined as were strongly agree and agree. Hazardous alcohol consumption of the adolescent, as described using the AUDIT-C, was the dependent variable. A stepwise multivariate logistic regression was undertaken to investigate the association between parent consumption, behaviour and demographics and adolescent alcohol consumption. The first model investigated the association between adolescent alcohol consumption and parental sociodemographic factors. The second model included parental attitude. The final model included consumption, attitude and socio-demographic information.
Results
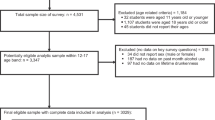
Three hundred and sixty students completed the questionnaire yielding a response rate of 37 % based on the number of students registered to those particular school years in the local-electorate area. Five hundred and forty-two corresponding questionnaires were retrieved from the participating students’ parents. Pupil and parent data were linked using a matching unique identification number.
Adolescent
The median age of adolescents was 17 years. 55.8 % were female. Over one-third of adolescents reported being hazardous drinkers (34.2 %), more males (39.6 %; 95 % CI 31.9–47.3 %)) than females (29.9 %; 95 % CI 23.5–36.2 %)). 68.2 % of these hazardous drinking adolescents were under the age of 18. These results are shown in Table 1.
Parent
More mothers (55.8 %) took part in the survey than fathers (44.2 %). Forty-seven percent of all parents surveyed were hazardous drinkers. The median age was 50 years for fathers and 48 years for mothers. Fathers were more likely to be hazardous drinkers (50 %) compared to mothers (46.8 %). These results are shown in Table 2.
Parent attitude
Over 90 % of parents disagreed with allowing their adolescent to get drunk. However, almost one-fifth of parents said they would not be worried if their adolescent consumed four pints of alcohol once a month. A large number of parents (42.8 %) agreed with permitting their adolescent to drink on special occasions and almost 18.2 % believed it would be okay for another parent to provide alcohol to their adolescent under supervision.
When fathers’ attitude toward alcohol was investigated further in univariate analysis it was found that if an adolescent is a hazardous drinker, their father is more likely to agree that it’s ‘Okay for their adolescent to get drunk sometimes’ (14.8 % vs. 2.8 %). Similarly, fathers of hazardous drinking adolescents were more likely to agree that ‘Getting drunk is part of having fun as an adolescent’ (13.5 % vs. 3.9 %) or that ‘It’s okay for pupils to drink on special occasions’ (65.2 % vs 29.8 %), when compared to adolescents that do not drink hazardously. Furthermore, if the adolescent is a hazardous drinker their father is more likely to ‘Allow another parent to supply their adolescent with alcohol’ (32.6 % vs. 9 %). These results are shown in Table 3.
The mother of an adolescent reporting hazardous drinking is more likely to agree that “it’s okay for their adolescent to get drunk sometimes” (5.9 % vs. 1.4 %) or that “getting drunk is part of having fun as an adolescent” (9.2 % vs. 2.8 %). Furthermore, 47.5 % of mothers of hazardous drinking teenagers agreed that adolescents should not drink at all compared to 63.3 % of mothers with non-hazardous drinking teenagers. Mothers who felt it was ok for their child to drink on special occasions were more likely to have hazardous consuming teenagers (62.5 %). These mothers were more likely to agree with introducing alcohol in the home (39 %) and not be concerned if there adolescent “drank four pints once a month” (27.4 %). These results are shown in Table 3.
Multivariate analysis
A stepwise multivariate logistic regression was undertaken to investigate the association between parent consumption, behaviour and demographics on adolescent alcohol consumption. Two hundred twenty-one individuals are included in the final, fully adjusted model. The fully adjusted model reports that adolescents whose fathers reported hazardous alcohol consumption were almost three times as likely to report hazardous alcohol consumption themselves (O.R = 2.90, 95 % CI: 1.32–6.35). Parental attitude toward drinking on special occasions was also positively associated with adolescent hazardous alcohol consumption. The father permitting drinking on special occasions results in adolescents being over four times more likely to report hazardous alcohol consumption (O.R = 4.60, 95 % CI: 1.19–11.18). This is over three times more likely if mothers report the same attitude (O.R = 3.79 95 % CI: 1.31–10.94). These results are shown in Table 4.
Discussion
Previous research highlights the role of the parent in terms of their attitude towards gender roles, sexual behaviour and substance use [45]. Hazardous drinking by the father was closely related to hazardous drinking by the adolescent, supporting recent research findings [19]. It is noteworthy that no such effect is observed with the drinking pattern of the mother. However, mothers’ attitudes towards alcohol is associated with adolescent consumption. Introducing alcohol at home on special occasions may be causing increased levels of consumption amongst adolescents [46]. A more authoritative parenting style may have a protective effect as previously suggested [47]. As previously highlighted, a joint parenting approach is important when confronting the issue of adolescent alcohol consumption [48]. A recent Irish study found similar attitudes amongst parents, however no link with adolescent drinking patterns was investigated [36]. Internationally, Bellis et al. found that adolescents who attained alcohol from parents experienced less alcohol-related harm, this study found that mothers introducing alcohol in a controlled home environment to have a protective effect [49]. Although these results are noted in the current research, policy reviews have noted the negative impact of this behaviour [50]. A larger sampling frame is required to investigate this curious finding.
Policy recommendations
The findings advocate the need for further public policy. In tackling alcohol consumption a variety of policy measures are required. Previous research has noted the importance of a minimum age for consumption. Exposure to alcohol in adolescence has detrimental effects on brain development and intellectual capabilities while it also increases the likelihood for later alcohol dependence [51, 52]. However, the current study notes that the majority of hazardous adolescent drinkers (68.2 %) were under the legal age of consumption. Therefore there is an urgent need to enhance our understanding of how adolescents acquire alcohol alongside improving enforcement of the law regarding under age alcohol sales. Moreover, previous research has noted the importance of restricting alcohol advertising and marketing which is aimed directly at adolescents [53–55]. The promotion of alcohol in areas such as sport, social media and music is increasingly prevalent [55]. Well-established evidence shows alcohol marketing increases the likelihood that adolescents will start to drink or will drink more if they are already using alcohol [54]. The evidence surrounding minimum unit pricing highlights its protective effects [56]. In addition, introduction of a parent programme to equip parents with the development of a culture of nurturing behaviours, establishing boundaries, and parental monitoring has shown promising results [48].
Strengths and weaknesses
This study had a number of strengths and weaknesses. The strengths of this study were that an electorate area in Southern Ireland was sampled and this is unlikely to differ significantly from the general population. Furthermore, every student in the final two years of second level education within the electorate area were invited to participate. The proportions of male and female participants was broadly similar to national figures where males represent 48 % of the population compared to 52 % of females [57]. In addition, age demographics were similar to national statistics [57]. Finally, the proportion of numbers who participated in the research across the penultimate and final years were broadly similar to national levels [57]. Moreover, our findings regarding parental and adolescent hazardous drinking levels were similar to recent national research [1, 58]. Both parent and adolescent surveys utilised previously validated questions from international studies. This study included two parent questionnaires so that both the influence of the mother and the father could be recorded.
However, a low response rate (37 %) was attained. Selection bias cannot be ruled out as no information on those who chose not to complete the survey is available. Furthermore, response rates for parents are unavailable due to the fact that population size information is unavailable. In addition, due to low response numbers particular characteristics could not be investigated due to infrequency of reporting i.e. single mothers, education status etc. It is possible that the survey may have produced socially desirable responses, certain results such as BMI were different from similar previous studies [41, 59–61]. However the results of participants were confidential. Finally, as parent and adolescent alcohol consumption were measured simultaneously, reverse causation cannot be dismissed [62].
Conclusion
Over one-third of adolescents were hazardous drinkers, and, of these, the majority were under the legal age of consumption. In particular, the influencing nature of both the father and the mother in terms of behaviour and attitude is noteworthy. In future, we recommend that any action plan to tackle adolescent drinking behaviours should also be aimed at tackling parent’s attitudes towards and consumption of alcohol. This research notes that the majority of hazardous adolescent drinkers (68.2 %) were under the legal age of consumption, hence an enhanced understanding of how adolescents acquire alcohol alongside improved enforcement of the law regarding under age adolescents buying alcohol is required. Furthermore, nation specific longitudinal research is required to investigate the impact of parental alcohol consumption, attitude and parenting style on adolescent alcohol consumption.
Abbreviations
- AUDIT-C:
-
Alcohol use disorders identification test for consumption
- BMI:
-
Body mass index
- CLAN:
-
College lifestyle attitudinal national (Survey)
- EU:
-
European Union
- PWI:
-
Personal wellbeing index
- SLAN:
-
Survey of lifestyle, attitudes and nutrition (in Ireland)
- SPSS:
-
Statistical package for social science
- WHO:
-
World Health Organization
References
Mongan D, Hope A, Nelson M. In: Board HR, editor. Social consequences of harmful use of alcohol in Ireland, HRB Overview Series 9. Dublin: Health Research Board; 2009. p. 11–51. http://www.hrb.ie/uploads/tx_hrbpublications/HRBOverview_9.pdf.
World Health Organization. Global status report on alcohol and health. 2014th ed. Switzerland: World Health Organization; 2014. http://www.who.int/substance_abuse/publications/global_alcohol_report/msb_gsr_2014_1.pdf?ua = 1.
Mäkelä P, Gmel G, Grittner U, Kuendig H, Kuntsche S, Bloomfield K, Room R. Drinking patterns and their gender differences in Europe. Alcohol Alcohol. 2006;41 suppl 1:i8–18.
Long J, Mongan D. Alcohol consumption in Ireland 2013: analysis of a national alcohol diary survey. Dublin: Health Research Board; 2014. http://www.drugsandalcohol.ie/22138.
World Health Organisation. Lexicon of Alcohol and Drug Terms. Geneva: World Health Organisation; 1994.
Monshouwer K, Smit F, de Zwart WM, Spruit I, van Ameijden EJ. Progress from a first drink to first intoxication: Age of onset, time-windows and risk factors in a Dutch national sample of secondary school students. J Subst Use. 2003;8(3):155–63.
Fischer JA, Najman JM, Plotnikova M, Clavarino AM. Quality of life, age of onset of alcohol use and alcohol use disorders in adolescence and young adulthood: Findings from an Australian birth cohort. Drug Alcohol Rev. 2015;34(4):388–96.
Loke AY, Mak Y-W. Family Process and Peer Influences on Substance Use by Adolescents. Int J Environ Res Public Health. 2013;10(9):3868–85.
Wadolowski M, Hutchinson D, Bruno R, Aiken A, Clare P, Slade T, Najman J, Kypri K, McBride N, Mattick RP. Early Adolescent Alcohol Use: Are Sipping and Drinking Distinct? Alcohol Clin Exp Res. 2015;39(9):1805–13.
Kandel D, Yamaguchi K. From beer to crack: developmental patterns of drug involvement. Am J Public Health. 1993;83(6):851–5.
Sneed CD, Tan HP, Meyer JC. The Influence of Parental Communication and Perception of Peers on Adolescent Sexual Behavior. J Health Commun. 2015;20(8):888–92.
Palmer D, O’Reilly G. Young people, alcohol and drugs. Dublin: Juvenile Mental Health Matters; 2008. http://www.drugs.ie/resourcesfiles/research/2008/2768-2964.pdf.
McCambridge J, McAlaney J, Rowe R. Adult consequences of late adolescent alcohol consumption: a systematic review of cohort studies. PLoS Med. 2011;8(2):e1000413.
Kerr RA. Adolescent males in secondary school in Ireland: alcohol use and depressed mood. Ir J Appl Soc Stud. 2013;13(1). Available at: http://arrow.dit.ie/ijass/vol13/iss1/3
Clark DB, Thatcher DL, Tapert SF. Alcohol, psychological dysregulation, and adolescent brain development. Alcohol Clin Exp Res. 2008;32(3):375–85.
Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, Kokkevi A, Kraus L: The 2011 ESPAD Report. Substance Use Among Students in 36 European Countries. In. The Swedish Council for Information on Alcohol and Other Drugs (CAN). http://www.espad.org/uploads/espad_reports/2011/the_2011_espad_report_full_2012_10_29.pdf: The Swedish Council for Information on Alcohol and other Drugs (CAN). The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Council of Europe, Co-operation Group to Combat Drug Abuse and Illicit Trafficking in Drugs (Pompidou Group); 2012.
The Irish Society for the Prevention of Cruelty to Children. If they’re getting loaded why can’t I? In. Dublin: National Children's Consultation Report; 2010. http://www.ispcc.ie/file/7/0_0/If+they%27re+getting+loaded+why+can%27t+I.pdf
Antoñanzas F, Rodríguez-Ibeas R, Barco E, Ramírez M, Pinillos M. Alcohol consumption in the EU: health economics and policy issues under a permanent debate. Eur J Health Econ. 2008;9(1):1–6.
Hung C-C, Chang H-Y, Luh D-L, Wu C-C, Yen L-L. Do parents play different roles in drinking behaviours of male and female adolescents? A longitudinal follow-up study. BMJ Open. 2015;5(4):e007179.
Studer J, Baggio S, Deline S, N’Goran AA, Henchoz Y, Mohler-Kuo M, Daeppen J-B, Gmel G. Peer pressure and alcohol use in young men: a mediation analysis of drinking motives. Int J Drug Policy. 2014;25:700–8.
Brown BB. The extent and effects of peer pressure among high school students: A retrospective analysis. J Youth Adolesc. 1982;11(2):121–33.
Iwamoto DK, Smiler AP. Alcohol makes you macho and helps you make friends: the role of masculine norms and peer pressure in adolescent boys’ and girls’ alcohol use. Subst Use Misuse. 2013;48(5):371–8.
Windle M, Spear LP, Fuligni AJ, Angold A, Brown JD, Pine D, Smith GT, Giedd J, Dahl RE. Transitions into underage and problem drinking: developmental processes and mechanisms between 10 and 15 years of age. Pediatrics. 2008;121(Supplement 4):S273–89.
Anacker AM, Loftis JM, Ryabinin AE. Alcohol intake in prairie voles is influenced by the drinking level of a peer. Alcohol Clin Exp Res. 2011;35(10):1884–90.
Eaton DK, Kann L, Kinchen S, Shanklin S, Flint KH, Hawkins J, Harris WA, Lowry R, McManus T, Chyen D. Youth risk behavior surveillance-United States, 2011. Morb Mortal Wkly Rep Surveill Summ. 2012;61(4):1–162.
White VM, Bariola E. Australian Secondary School Students’ Use of Tobacco, Alcohol, and Over-the-counter and Illicit Substances in 2011. Report prepared for: National Drug Strategy, Centre for Behavioural Research in Cancer, The Cancer Council Victoria; 2012.
Hope A. ‘Lead Us Not into Temptation’: Adolescence and Alcohol Policy in Europe. Alcohol Alcohol. 2013;49:126–7.
Shek DT. Family environment and adolescent psychological well-being, school adjustment, and problem behavior: A pioneer study in a Chinese context. J Genet Psychol. 1997;158(1):113–28.
Parker JS, Benson MJ. Parent-adolescent relations and adolescent functioning: Self-esteem, substance abuse, and delinquency. Adolescence. 2004;39(155):519–30.
Ryan SM, Jorm AF, Lubman DI. Parenting factors associated with reduced adolescent alcohol use: a systematic review of longitudinal studies. Aust N Z J Psychiatry. 2010;44(9):774–83.
Shortt AL, Hutchinson DM, Chapman R, Toumbourou JW. Family, school, peer and individual influences on early adolescent alcohol use: first-year impact of the Resilient Families programme. Drug Alcohol Rev. 2007;26(6):625–34.
Seljamo S, Aromaa M, Koivusilta L, Rautava P, Sourander A, Helenius H, Sillanpää M. Alcohol use in families: a 15‐year prospective follow‐up study. Addiction. 2006;101(7):984–92.
Visser L, de Winter AF, Reijneveld SA. The parent–child relationship and adolescent alcohol use: a systematic review of longitudinal studies. BMC Public Health. 2012;12(1):886.
Census 2011 Results: Area Profile for County Cork [http://census.cso.ie/areaprofiles/PDF/CTY/cork.pdf]
Rumpf H-J, Wohlert T, Freyer-Adam J, Grothues J, Bischof G. Screening questionnaires for problem drinking in adolescents: performance of AUDIT, AUDIT-C, CRAFFT and POSIT. Eur Addict Res. 2012;19(3):121–7.
Smyth BP, Darker CD, Donnelly-Swift E, Barry JM, Allwright SP. A telephone survey of parental attitudes and behaviours regarding teenage drinking. BMC Public Health. 2010;10(1):297.
Palmer S, Kalafatelis E. Parental attitudes and behaviours towards teen drinking: Survey of parents of 12–17 year olds - Final Report. Research New Zealand; 2008. Available from: http://www.hpa.org.nz/sites/default/files/imported/field_research_publication_file/ParentalAttitudes.pdf
Hope A, Dring C, Dring J. College lifestyle and attitudinal national (CLAN) survey. Dublin: The Health of Irish Students, Health Service Executive; 2005.
Tomyn AJ, Cummins RA. The subjective wellbeing of high-school students: Validating the personal wellbeing index—school children. Soc Indic Res. 2011;101(3):405–18.
The International Wellbeing Group: Personal Wellbeing Index – Adult. In., 5th edn. Melbourne. http://www.acqol.com.au/iwbg/wellbeing-index/: Australian Centre on Quality of Life, Deakin University; 2013.
Harrington J, Perry I, Lutomski J, Morgan K, McGee H, Shelley E, Watson D, Barry M. SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland. Dietary habits of the Irish population. Dublin: Department of Health and Children; 2008. Available from: http://epubs.rcsi.ie/cgi/viewcontent.cgi?article=1005&context=psycholrep
Crawford D, Campbell K. Lay definitions of ideal weight and overweight. Int J Obes Relat Metab Disord. 1999;23(7):738–45.
Kelly TM, Donovan JE, Chung T, Bukstein OG, Cornelius JR. Brief screens for detecting alcohol use disorder among 18–20 year old young adults in emergency departments: Comparing AUDIT-C, CRAFFT, RAPS4-QF, FAST, RUFT-Cut, and DSM-IV 2-Item Scale. Addict Behav. 2009;34(8):668–74.
Dawson DA, Grant BF, Stinson FS, Zhou Y. Effectiveness of the derived alcohol use disorders identification test (AUDIT‐C) In screening for alcohol use disorders and risk drinking in the US general population. Alcohol Clin Exp Res. 2005;29(5):844–54.
Carlson MJ. Family structure, father involvement, and adolescent behavioral outcomes. J Marriage Fam. 2006;68(1):137–54.
Long Foley K, Altman D, Wolfson M. Adults’ approval and adolescents’ alcohol use. J Adolesc Health. 2004;35(4):345. e317-345. e326.
Calafat A, Garcia F, Juan M, Becoña E, Fernández-Hermida JR. Which parenting style is more protective against adolescent substance use? Evidence within the European context. Drug Alcohol Depend. 2014;138:185–92.
Foxcroft DR, Tsertsvadze A. Universal multi-component prevention programs for alcohol misuse in young people. Cochrane Database Syst Rev. 2011;9:CD009307.
Bellis MA, Phillips-Howard PA, Hughes K, Hughes S, Cook PA, Morleo M, Hannon K, Smallthwaite L, Jones L. Teenage drinking, alcohol availability and pricing: a cross-sectional study of risk and protective factors for alcohol-related harms in school children. BMC Public Health. 2009;9(1):1.
Pedersen W. Parents as alcohol pushers? Tidsskr Nor Laegeforen. 1990;110(14):1834–7.
Zeigler DW, Wang CC, Yoast RA, Dickinson BD, McCaffree MA, Robinowitz CB, Sterling ML. The neurocognitive effects of alcohol on adolescents and college students. Prev Med. 2005;40(1):23–32.
Komro KA, Maldonado‐Molina MM, Tobler AL, Bonds JR, Muller KE. Effects of home access and availability of alcohol on young adolescents’ alcohol use. Addiction. 2007;102(10):1597–608.
Winpenny EM, Marteau TM, Nolte E. Exposure of children and adolescents to alcohol marketing on social media websites. Alcohol Alcohol. 2014;49(2):154–9.
Anderson P, De Bruijn A, Angus K, Gordon R, Hastings G. Impact of alcohol advertising and media exposure on adolescent alcohol use: a systematic review of longitudinal studies. Alcohol Alcohol. 2009;44:229–43.
Fox KA, Kelly C, Molcho M. Alcohol Marketing and Young People’s Drinking Behaviour in Ireland. 2015.
Brennan A, Meng Y, Holmes J, Hill-McManus D, Meier PS. Potential benefits of minimum unit pricing for alcohol versus a ban on below cost selling in England 2014: modelling study. BMJ. 2014;349:g5452.
Annual Statistical Reports: 2014/2015 [http://www.education.ie/en/Publications/Statistics/Statistical-Reports/]
Callaghan M, Gavin A, Keane E, Nic Gabhainn S, Molcho M, Kelly C. The Irish health behaviour in school-aged children (HBSC) study 2014. 2015.
Cagney H. The X-HALE Awards: stubbing out youth smoking in Ireland. Lancet Oncol. 2013;14(8):693.
Garnett C, Crane D, West R, Michie S, Brown J, Winstock A. Normative misperceptions about alcohol use in the general population of drinkers: A cross-sectional survey. Addict Behav. 2014;42:203–6.
Hattori A, Sturm R. The obesity epidemic and changes in self‐report biases in BMI. Obesity. 2013;21(4):856–60.
Otten R, Van Der Zwaluw CS, Van Der Vorst H, Engels RC. Partner effects and bidirectional parent-child effects in family alcohol use. Eur Addict Res. 2008;14(2):106–12.
Acknowledgements
Not applicable.
Availability of data and materials
The dataset supporting the conclusions of this article is not available. This is due to the sensitive nature of the data and the potentially identifiable nature of individual responses.
Authors’ contributions
EM – Formed research question, drafted manuscript, conducted analysis of data and formatting of research article. IO’S – Formed research question, drafted manuscript, conducted analysis of data and formatting of research article. DO’D – Provided guidance and feedback on research question, data collection and manuscript. AH – Provided guidance on research question, outlined detailed feedback on drafts. MPD – Supervised project, provided guidance on research question, outlined detailed feedback on drafts. All authors have read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval was granted by the Clinical Research Ethics Committee for Cork Teaching Hospitals. This approval recognised each co-author as a co-investigator and sanctioned each data collection site. Parents consented both for themselves and for their adolescent to participate in the research study. In addition, adolescents signed their consent form in the presence of their parent/guardian to participate in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Murphy, E., O’Sullivan, I., O’Donovan, D. et al. The association between parental attitudes and alcohol consumption and adolescent alcohol consumption in Southern Ireland: a cross-sectional study. BMC Public Health 16, 821 (2016). https://doi.org/10.1186/s12889-016-3504-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-016-3504-0