
Abstract
Background
Obsessive-compulsive disorder (OCD) imposes significant burdens on individuals, families, and healthcare systems and the COVID-19 pandemic appears to have exacerbated OCD symptoms. Currently, there are no validated prevention programs for OCD, highlighting a critical gap in mental health services. This study aims to develop and validate the first ØCD prevention program, for at-risk adults, utilizing cognitive-behavioral therapy (CBT) and exposure response prevention (ERP) techniques.
Methods
A single-blind, randomized controlled trial comparing the ØCD prevention program to a waitlist control group will be conducted. Participants, at-risk adults (18–65 years) with subclinical OCD symptoms (OCI-R score ≥ 12), will be recruited for the study. The ØCD prevention program compresise of six online group sessions incorporating CBT and ERP techniques over three modules. The primary outcomes are OCD symptom severity (measured by the Obsessive-Compulsive Inventory- revised form; OCI-R), depression symptoms (measured by the Patient Health Questionnaire; PHQ-9), and anxiety symptoms (measured by the Generalised Anxiety Disorder 7-item; GAD-7). Secondary outcomes include OCD-related beliefs, experiential avoidance, resilience, quality of life, uncertainty intolerance, automatic thoughts, and distress. Outcome measures will be collected at baseline, at completion of the intervention, and one year later (follow-up). At follow-up, we will also analyze the OCD diagnostic incidence, using the Structured Clinical Interview for DSM-5. We will employ a multivariate analysis of variance (MANOVA) to explore whether significant differences exist between groups across dependent variables. To compare the OCD incidence levels from the pre-test to the follow-up we will use the chi-squared test.
Discusion
The present study may contribute novel data on the efficacy of OCD prevention approaches, leading to the development of an evidence-based OCD prevention program that could alleviate individual and societal burdens associated with OCD.
Trial registration
This trial was approved by the University Ethical Review Authority (937/ 28.11.2023) at Babeș-Bolyai University and is registered on clinicaltrials.gov (ID: NCT06262464).
Similar content being viewed by others


Article summary
Strengths and limitations of this study
• First study to develop and validate an OCD prevention program for at-risk adults.
• The program integrates psychological prevention techniques from evidence-based treatments.
• Moderate expected rates of participants dropout
Background
Obsessive-compulsive disorder (OCD) is one of the most debilitating mental health disorders, with considerable burden on patients, their families, and health services [19]. As a psychiatric disorder, it is characterized by the co-occurrence of recurring, intrusive obsessions that induce substantial distress, along with compulsions—ritualistic behaviors aimed at relieving the distress triggered by the obsessions but ultimately resulting in additional distress and impairment (American Psychiatric Association, 2013). The prevalence estimates vary from 0.7-3% in adults [26],Adam et al., 2011), and 0.25-0.30% in children (Sadler et al., 2017; [17].
OCD has both direct costs, such as medical costs [16, 18], as well as indirect costs, such as work absenteeism due to impaired functionality and lost opportunities for career advancement [9]. One UK study [19] found that the overall cost-of-illness of OCD rises to £5,095,759,464, with an average annual cost-of-illness of £7077 per person.
Worryingly, the COVID-19 pandemic seems to have led to an increase in the incidence of OCD. A systematic review [22] found that both people with and without diagnosed OCD before the pandemic experienced a worsening of OCD symptoms during the pandemic. One study [25] found that participants reported significantly higher OCD scores during the pandemic compared to before the pandemic, as OCD severity increased on all symptom dimensions and the most pronounced change was on the washing dimension. Another review (Cunning & Hodes, 2021) found that the COVID-19 pandemic is associated with a worsening of OCD symptoms in young people and that being in treatment seems to have a protective effect, thus underlining the importance of maintaining mental health services. While we have multiple evidence-based treatments for OCD, there are currently no validated protocols for the prevention of general OCD. This is a major shortcoming, seeing as an effective prevention program for at-risk individuals could constitute a preemptive strike against the high associated costs and burden of living that come with a diagnosis of OCD. Former prevention programs for depression and anxiety usually carried out for adolescents and young adults, have varying rates of efficacy, but are overall considered successful in reducing psychopathological symptoms incidence in time (Conley et al., 207; Werner et al., 2021).
The development and validation of an intervention protocol for the prevention of OCD among at-risk adults, as presented in the ØCD prevention program, are thus paramount. By advancing OCD preventive approaches, this study offers hope for mitigating the long-term consequences of OCD and reducing the associated costs and burden on individuals and society.
Specific contents of the ØCD prevention protocol
The program involves six sessions and includes established components of CBT [4] and ERP [11], namely: (1) psychoeducation and encouragement to reduce, change, or eliminate anxiety-reducing rituals (1 session), (2) cognitive restructuring by challenging dysfunctional beliefs (2 sessions), (3) behavioral changes by prolonged, imaginal and real-life exposure to distress-provoking stimuli (2 sessions), (4) addressing ways and skills to reduce relevant risk factors (i.e. fear of COVID-19) and to develop resilience factors (i.e. resilience levels, coping skills) and summary and recapitulation (1 session). The six sessions of the 2 weeks program correspond to three treatment modules (3 hours/module). An overview of the content covered in each stage is provided in Table 1.
Aim of the present study
The main objective of the proposed study is to develop and assess the efficacy of the ØCD prevention program in preventing OCD symptoms and reducing associated symptoms versus a waitlist control group. In this single-blind, superior randomized controlled trial, we will evaluate the efficacy of the ØCD prevention program compared with a waitlist. If, as we hypothesize, the ØCD prevention program demonstrates superiority compared to a control group, it has the potential to increase the variety of evidence-based intervention options for adults at risk of developing OCD.
We hypothesize that the ØCD prevention program will be superior to a control group in the reduction of OCD symptoms as measured by the Obsessional Compulsive Inventory – revised form (OCI-R; [10]), depressive symptoms (Patient Health Questionnaire-9,PHQ-9; [20]), and anxiety symptoms (Generalized Anxiety Disorder-7,GAD-7; [29]). The intervention also covers the cognitive component of OCD, so we expect a reduction in obsessive beliefs (The Obsessive Beliefs Questionnaire,OBQ-44; [24]) and automatic thoughts (Automatic Thoughts Questionnaire,ATQ; Steven & Phillip, 1980). We also expect a reduction in experiential avoidance levels (The Brief Experiential Avoidance Questionnaire; EAQ; Gamez et al., 2014), intolerance of uncertainty (Intolerance of Uncertainty Scale: IUS; [5]), and general distress (General Health Questionnaire-12,GHQ; [15]). As for protective factors, we expect an increase in resilience (Resilience Scale for Adults,RSA; [13]) and quality of life (WHO Quality of Life - BREF,WHOQOL-BREF; [28]).
Methods
Study design and ethical aspects
We will conduct a single-blind (blinded outcome assessors), randomized (1:1), controlled, parallel-group, superiority trial comparing the ØCD prevention program with a control group (waitlist) for adults at risk of OCD. The study is registered on clinicaltrials.gov (ID: NCT06262464). All quality and safety aspects will be regularly monitored by an external party: the University Ethical Review Board, and by the financing authority of the project (National Authority for Scientific Research). The study has been approved by the University Ethical Review Authority (937/28.11.2023). Potential protocol modifications will be described in detail on clinicaltrials.gov. We used the SPIRIT reporting guidelines [6].
Participants will be asked to provide informed consent before baseline assessment. They will receive detailed information about the study and their right to withdraw from the study without the obligation to give reasons. We do not expect major relevant risks for participants during the study, or after the study is completed. The time burden for the participants will be a reasonable amount. The data collection and storage will be conducted according to GDPR legislation, and all personal data will be securely stored on the University’s encrypted servers, following the set data management guidelines.
Sample size
G*Power was used for the sample size calculation and, following an effect size of d=0.3 with a n alpha level of α = 0.05 and power of 0.95, a sample size of 175 was suggested. Based on this power analysis and expected drop-out rates, we aim for 200 participants (100 per treatment arm). The Consolidated Standards of Reporting Trials flow chart of the trial is shown in Figure 1.

CONSORT flow diagram
Recruitment
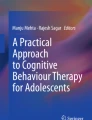
Participants are recruited online, using social media platforms to promote the study. By clicking the enrolment link, participants read the study information section and the informed consent form, which can be signed digitally, by agreeing to the terms and the conditions of the study. Participants are queried about the criteria for inclusion and exclusion, following which eligible individuals are selected through randomization. The planned flow of participants can be consulted in Figure 2.

Planned flow of participants. Note: ATQ-Automatic Thoughts Questionnaire; BEAQ-Brief Experiential Avoidance Questionnaire; CSQ-8- Client Satisfaction Questionnaire-8; GAD-7-Generalized Anxiety Disorder-7; GHQ-12-General Health Questionnaire-12; IUS-Intolerance of Uncertainty Scale; OBQ-44-Obsessive Beliefs Questionnaire-44; ØCD - OCD prevention program; OCI-R-Obsessional Compulsive Inventory – Revised; PHQ-9-Patient Health Questionnaire-9; RSA-Resilience Scale for Adults; WHOQOL-BREF-WHO Quality of Life – BREF
Therapists are from the clinical psychology master's program. We recruited four terminal year students following an introductory meeting on the purpose of the study and the procedures involved. The expected time expenditure for the therapists will be 9 hours per week. Before implementation, all therapists will have participated in a training supported by the study coordinator.
Inclusion and exclusion criteria
Participants are included if they are of legal age (above 18). We include participants who have an OCI-R [10] score at or above the cut-off point on the OCD subscale (≥ 12). Exclusion criteria are as follows: (1) clinically diagnosed OCD, (2) current psychiatric/psychotherapeutic treatment, (3) a personality disorder diagnosis, and (4) suicidal ideation.
Procedure and randomization
Inclusion and exclusion criteria are verified based on the screening form completed by the participants. Eligible participants are randomly allocated to one of the two conditions in a 1:1 ratio. Randomization is conducted by a member of the research team, using the online tool, randomizer.org. The allocation sequence is generated through a computer-generated random sequence for the two study conditions. The following study personnel will remain blind to group allocation until the final data analyses are completed: principal investigator, data managers, and outcome assessors.
Outcome measures
For participants, the baseline assessment will take place after randomization and include a set of validated questionnaires.
Primary outcome measures
Obsessional Compulsive Inventory - Revised (OCI-R; [10])
OCI-R is a self-report questionnaire of 18 items, and it measures OCD symptoms across six subscales: washing, checking, neutralising, obsessing, ordering, and hoarding. OCI-R was used in the initial screening of eligible participants, where the OCD subscale (which excludes the hoarding component) was used to determine participants who are at risk of developing OCD symptoms (cut off point (≥ 12). For the present study, the reduction in OCI-R OCD subscale assessment is the primary outcomes.
Patient Health Questionnaire-9 (PHQ-9; [20])
PHQ-9 is one of the most widely used measures of depression and it is based on the diagnostic criteria for major depressive disorder in the Diagnostic and Statistical Manual (DSM-IV; APA, 1994). Scores vary from 0 to 27, where a greater score indicates more severe depressive symptoms.
Generalized Anxiety Disorder-7 (GAD-7; [29])
GAD-7 measures symptoms of anxiety, based on the generalized anxiety disorder criteria in DSM-IV; APA, 1994). Respondents evaluate the level of their symptoms over the last two weeks and a cut-off score greater than 10 indicates further evaluation is recommended.
Secondary outcome measures
Obsessive Beliefs Questionnaire (OBQ-44; [24])
OBQ-44 is a self-report scale that measures belief domains linked to OCD. The three subscales are (1) responsibility/threat estimation, (2) perfectionism/certainty, and (3) importance/control of thoughts. Answers are rated on a 7-point scale (1 = “disagree very much” to 7 = “agree very much”).
Automatic Thoughts Questionnaire (ATQ; Hollon & Kendall, 1980)
The Romanian version of ATQ [23] is a 15-item measure that evaluates self-reported negative thoughts. The questionnaire was developed to measure the most frequent negative thoughts and negative self-evaluations, typically associated with depression. Answers are rated on a 5-point scale (1 = “not at all” to 5 = “all the time”) and the total score ranges from 15 to 75.
Brief Experiential Avoidance Questionnaire (BEAQ; Gamez et al., 2014)
The BEAQ is a 15-item self-reports questionnaire that measures experiential avoidance. Items are rated on a 6-point Likert scale (1 = “strongly disagree” to 6 = “strongly agree”). Item 6 is a reversed item, and scores range from 15 to 90 points. Higher scores reflect higher experiential avoidance.
Intolerance of Uncertainty Scale (IUS; [5])
The IUS is a 27-item measure that evaluates how individuals relate to uncertainty. It contains items such as “Uncertainty makes me uneasy, anxious, or stressed”, “A small unforeseen event can spoil everything, even with the best of planning” and “When I am uncertain, I can’t go forward”. Answers are rated on a 5 points scale (1 = “not at all characteristics” to 5 = “entirely characteristic”)
General Health Questionnaire-12 (GHQ-12; [15])
The GHQ-12 consists of 12 items, each assessing the severity of a mental issue over the past few weeks. Answers are rated on a 4-point Likert scale, from 0 to 3. A total score of 36 can be generated, by rating the positive items from 0 (always) to 3 (never) and the negative ones from 3 (always) to 0 (never), so that a higher score indicate worse health.
Resilience Scale for Adults (RSA; [13])
The RSA is a 43-item measure with five factors: personal competence, social competence, family cohesion, social support, and personal organization. Answers are rated on a 5-point Likert scale from 1 = “not at all” to 5 = “a lot”).
WHO Quality of Life - BREF (WHOQOL-BREF; [28])
WHOQOL-BREF is one of the most widely used assessments of quality of life. In the current study, we will use the global item of the instrument (How would you rate your quality of life), answered on a 5-point Likert scale.
Post-intervention assessment will take place immediately after the intervention is completed and will include the same measures, as well as the Client Satisfaction Questionnaire-8 (CSQ-8; [21]). The assessments will be completed online, using the Qualtrics platform. We will also perform one follow-up assessment six months later, using the same measures and the Structured Clinical Interview for DSM-5 to compare the OCD diagnostic incidence.
Statistical analyses
Data analysis
Demographic and clinical data will be reported as means and SDs for continuous parametric data, medians, and ranges for non-parametric data, and frequencies and percentages for categorical data. Only two authors will have access to the final trial dataset. To illustrate participant flow, we will report results in a CONSORT diagram. Data analysis will be conducted using SPSS for Windows version 25. Given the anticipated dropout rate, mixed models will be employed as the most suitable statistical method. This approach is well-suited for analyzing repeated measures, accounting for the dependency between observations and handling missing data effectively. Mixed models will be adjusted for baseline values of the repeated measures. Descriptive statistics will be generated to summarize the means and proportions of baseline clinical and demographic variables across treatment conditions, allowing for the assessment of potential imbalances. Fixed effects in the model will include time, treatment, and their interaction. In cases of missing data, these variables will also be included as fixed effects. The significance of the time*treatment interaction p-values for various outcome measures will be assessed using the Benjamini–Hochberg procedure (two-sided p < 0.05). Time will be treated categorically, with the first post-baseline measurement serving as the reference category. To address the correlation among repeated measurements, a first-order autoregressive (AR (1)) structure will be imposed on the residuals. Furthermore, the interaction effect between time and group will be explored by analyzing estimated marginal means at different time points. We anticipate a significant interaction effect between time and group, signifying differential changes in scores over time between the two treatment conditions. Specifically, we expect a more pronounced decline in scores over time in the prevention group compared to the control group. To assess the statistical significance of improvements in the treatment conditions, a least significant difference test will be conducted with estimated marginal means to compare changes between groups. Linear mixed models are expected to reveal a statistically significant decline in the prevention condition from pretest to post-test, with no significant differences between post-test and follow-up measures. To facilitate comparisons with other studies, Cohen’s d statistic will be calculated to determine within-group effect sizes. In cases where the proportion of missing data exceeds 10%, maximum likelihood imputations will be performed based on demographics and pretreatment scores. Additionally, the proportions of dropouts and diagnostic incidence (from pre-test to follow-up) in the two treatment groups will be compared using the chi-square test.
Discussion
According to the most recent clinical advances guide for OCD [12], a greater effort needs to be made at multiple levels (e.g., education, treatment services development, and screening of ‘at-risk’ individuals) to implement effective strategies for prevention, early diagnosis, and intervention. To the best of our knowledge, we will develop the first evidence-based cognitive-behavioral prevention program for OCD for at-risk individuals. The study will provide novel data about the efficacy of OCD preventive strategies. Implementing the prevention program in normal healthcare would significantly enhance the availability of effective prevention programs to persons at risk of developing OCD. The potential benefits of such a prevention program extend beyond individual participants to encompass broader societal and research impacts. By intervening early to prevent the onset of OCD symptoms, the program could alleviate strain on mental health services, reduce healthcare costs, and improve overall well-being. Moreover, the research generated from implementing and evaluating this innovative prevention approach could inform future interventions and contribute to advancing our understanding of OCD prevention.
Trial status
Inclusion started in March 2024 and is expected to end in October 2024. At the time of submission, 121 participants had been randomized. Data analysis and reporting of results will begin when all data from the primary endpoint has been collected.
Availability of data and materials
Data will be made available upon reasonable request from the corresponding author.
Abbreviations
- OCD:
-
Obsessive Compulsive Disorder
- CBT:
-
Cognitive Behavioral Therapy
- ERP:
-
Exposure and Response Prevention
References
Adam Y, Meinlschmidt G, Gloster AT, Lieb R. Obsessive–compulsive disorder in the community: 12-month prevalence, comorbidity and impairment. Soc Psychiatry Psychiatr Epidemiol. 2012;47:339–49.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Bream V, Challacombe F, Palmer A, Salkovskis P. Cognitive behaviour therapy for obsessive-compulsive disorder. Oxford University Press; 2017.
Buhr K, Dugas MJ. The intolerance of uncertainty scale: Psychometric properties of the English version. Behav Res Ther. 2002;40(8):931–45.
Chan A-W, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin J, Dickersin K, Hróbjartsson A, Schulz KF, Parulekar WR, Krleža-Jerić K, Laupacis A, Moher D. SPIRIT 2013 Explanation and Elaboration: Guidance for protocols of clinical trials. BMJ. 2013;346: e7586.
Conley CS, Shapiro JB, Kirsch AC, Durlak JA. A meta-analysis of indicated mental health prevention programs for at-risk higher education students. J Couns Psychol. 2017;64(2):121.
Cunning C, Hodes M. The COVID-19 pandemic and obsessive–compulsive disorder in young people: Systematic review. Clin Child Psychol Psychiatry. 2022;27(1):18–34.
El-slamon, M. A. E. F. A., Al-Moteri, M., Plummer, V., Alkarani, A. S., & Ahmed, M. G. (2022, February). Coping strategies and burden dimensions of family caregivers for people diagnosed with obsessive–compulsive disorder. In Healthcare (Vol. 10, No. 3, p. 451). MDPI.
Foa EB, Huppert JD, Leiberg S, Langner R, Kichic R, Hajcak G, Salkovskis PM. The Obsessive-Compulsive Inventory: development and validation of a short version. Psychol Assess. 2002;14(4):485.
Foa, E. B., Yadin, E., & Lichner, T. K. (2012). Exposure and response (ritual) prevention for obsessive-compulsive disorder: Therapist guide. Oxford University Press.
Fineberg NA, Van Ameringen M, Drummond L, Hollander E, Stein DJ, Geller D, Walitza S, Pallanti S, Pellegrini L, Zohar J. How to manage obsessive-compulsive disorder (OCD) under COVID-19: A clinician’s guide from the International College of Obsessive-Compulsive Spectrum Disorders (ICOCS) and the Obsessive-Compulsive and Related Disorders Research Network (OCRN) of the European College of Neuropsychopharmacology. Compr Psychiatry. 2020;100: 152174.
Friborg O, Hjemdal O, Rosenvinge JH, Martinussen M. A new rating scale for adult resilience: what are the central protective resources behind healthy adjustment? Int J Methods Psychiatr Res. 2003;12:65–76.
Gámez W, Chmielewski M, Kotov R, Ruggero C, Suzuki N, Watson D. The brief experiential avoidance questionnaire: development and initial validation. Psychol Assess. 2014;26(1):35.
Goldberg, P. (1972). The detection of psychiatric illness by questionnaire. Maudsley monograph.
Heslin, M., Gellatly, J., Pedley, R., Knopp-Hoffer, J., Hardy, G., Arundel, C., ... & Byford, S. (2022). Out of pocket expenses in obsessive compulsive disorder. Journal of Mental Health, 31(5), 607-612.
Heyman I, Fombonne E, Simmons H, Ford T, Meltzer H, Goodman R. Prevalence of obsessive–compulsive disorder in the British nationwide survey of child mental health. Br J Psychiatry. 2001;179(4):324–9.
Jo C. Cost-of-illness studies: concepts, scopes, and methods. Clin Mol Hepatol. 2014;20(4):327.
Kochar N, Ip S, Vardanega V, Sireau NT, Fineberg NA. A cost-of-illness analysis of the economic burden of obsessive-compulsive disorder in the United Kingdom. Compr Psychiatry. 2023;127: 152422.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13.
Larsen DL, Attkisson CC, Hargreaves WA, Nguyen TD. Assessment of client/patient satisfaction: development of a general scale. Eval Program Plann. 1979;2(3):197–207.
Linde ES, Varga TV, Clotworthy A. Obsessive-compulsive disorder during the COVID-19 pandemic—a systematic review. Front Psych. 2022;13: 806872.
Moldovan, R. (2007). Chestionarul gandurilor automate [Automatic thoughts questionnaire]. Sistem de evaluare clinica [Clinical Evaluation System]. Cluj-Napoca: RTS Publishing.
Moulding R, Anglim J, Nedeljkovic M, Doron G, Kyrios M, Ayalon A. The Obsessive Beliefs Questionnaire (OBQ): Examination in nonclinical samples and development of a short version. Assessment. 2011;18(3):357–74.
Otte J, Schicktanz N, Bentz D. Impact of the COVID-19 pandemic on obsessive-compulsive symptoms in the Swiss general population. Front Psychol. 2023;14:1071205.
Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15(1):53–63.
Sadler, K., Vizard, T., Ford, T., Goodman, A., Goodman, R., & McManus, S. (2018). Mental health of children and young people in England, 2017: trends and characteristics.
Skevington SM, Lotfy M, O’Connell KA. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13:299–310.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7.
Steven D, H., & Philip C, K. Automatic Thoughts Questionnaire. Psychological Assessment: A Journal of Consulting and Clinical Psychology.
Werner-Seidler, A., Spanos, S., Calear, A. L., Perry, Y., Torok, M., O'Dea, B., ... & Newby, J. M. (2021). School-based depression and anxiety prevention programs: An updated systematic review and meta-analysis. Clinical Psychology Review, 89, 102079.
Whitehead AL, Julious SA, Cooper CL, et al. Estimating the sample size for a pilot randomized trial to minimize the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016;25:1057–73.
Acknowledgements
None
Funding
This work is supported by a grant from the Romanian National Authority for Scientific Research, CNCS–UEFISCDI [grant number PN-III-P1-1.1-PD-2021-0750].
Author information
Authors and Affiliations
Contributions
RAIC: conceptualization, methodology, formal analysis, investigation, data curation, writing - original draft, writing - review & editing. EPD: methodology, formal analysis, investigation, data curation, writing – original draft. OAD: conceptualization, writing - review & editing, supervision, project administration.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors assert that all procedures contributing to this study comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study has been approved by the University Ethical Review Authority (937/28.11.2023). Potential protocol modifications will be described in detail on clinicaltrials.gov (ID: NCT06262464). Any modification will be informed on Clinicaltrials.gov.
Regarding participants’ consent, participants will be informed about the basics of the study and the potential benefits. Informed consent of the participants will be obtained after the nature of the procedures has been fully explained. Only those who provide the consent will be included in the study. They will also be reminded that they can withdraw their consent at any point to terminate their participation and that anonymity and confidentiality are ensured. Regarding the potential risks of the study, no risks are expected. Nevertheless, in case of adverse events (e.g. relevant clinical symptoms) individualized assistance will be offered. If necessary, specialized services will be provided.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cardoș, R.A.I., Dumitru, E.P. & David, O.A. ØCD: protocol for the development and evaluation of a cognitive-behavioral prevention program for obsessive-compulsive disorder. BMC Psychiatry 24, 348 (2024). https://doi.org/10.1186/s12888-024-05791-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05791-3